
Effects of Prenatal Tobacco and Wood-Fuel Smoke Exposure on Birth Weight in Sri Lanka

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Data Analyis
3. Results
3.1. Characteristics of Participants
3.2. Relationship between Maternal Parameters and Birth Weight
3.3. Exposure Response
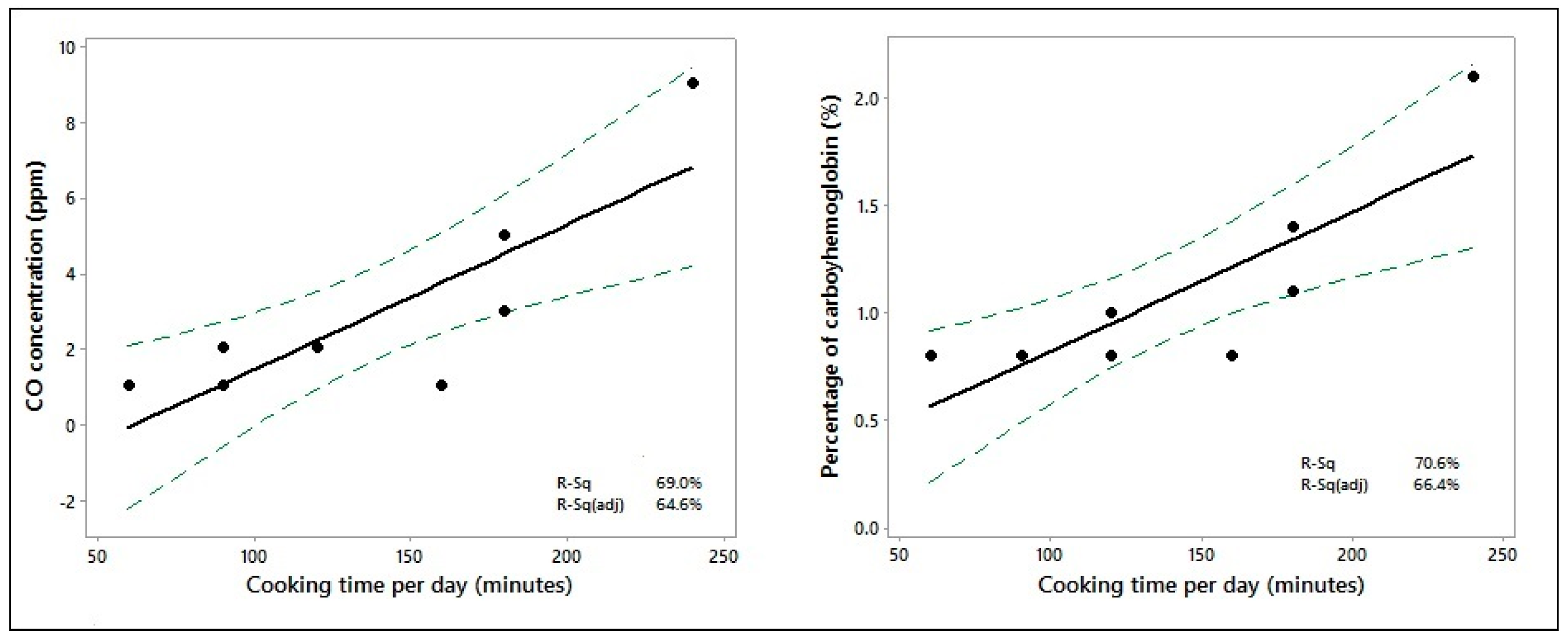
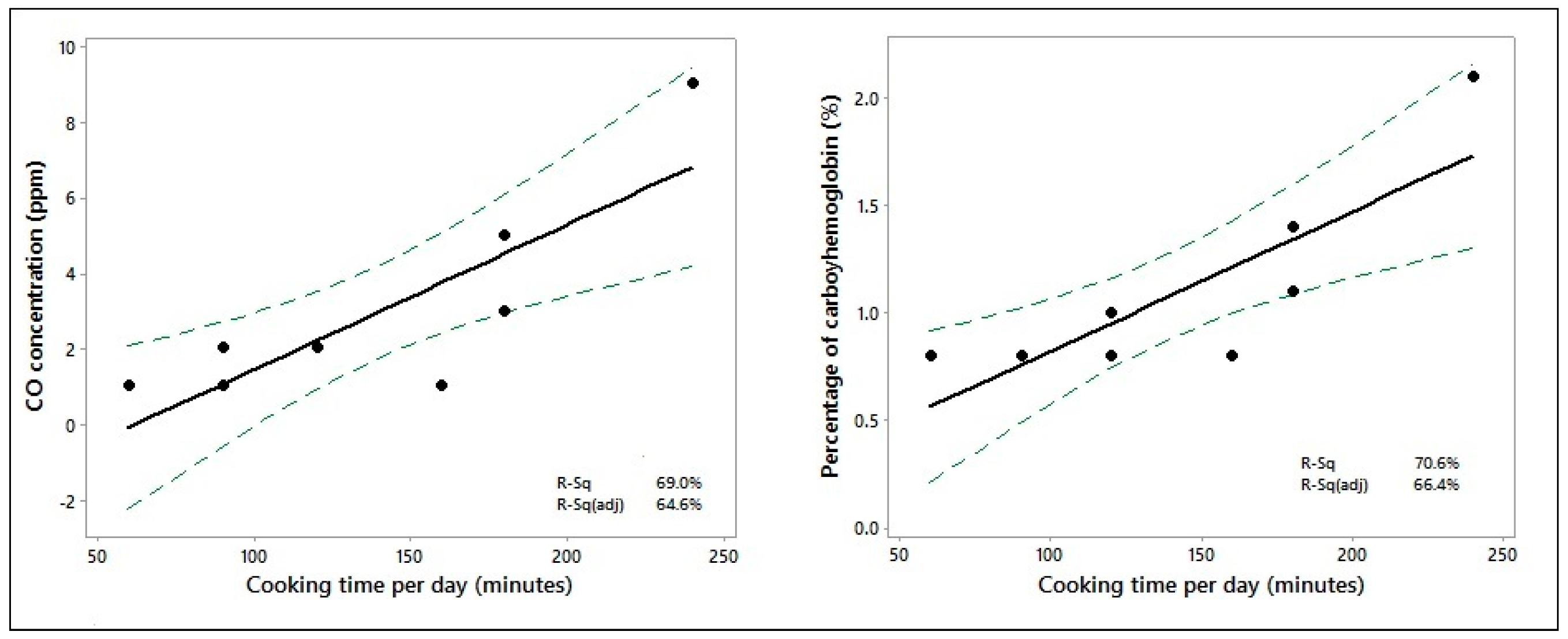
3.4. Time Spent Cooking and CO and COHb Measurements
4. Discussion
Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ministry of Health. Annual Health Bulletin; Ministry of Health, Nutrition and Indigenous Medicine, Medical Statistics Unit: Colombo, Sri Lanka, 2014.
- World Health Organization and United Nations Children’s Fund. Low Birth Weight; Country, Regional and Global Estimates. Available online: https://www.unicef.org/publications/files/low_birthweight_from_EY.pdf (accessed on 10 April 2017).
- Wisborg, K.; Henriksen, T.B.; Hedegaard, M.; Secher, N.J. Smoking during pregnancy and preterm birth. Br. J. Obstet. Gynaecol. 1996, 103, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Suzuki, K.; Tanaka, T.; Kohama, M.; Yamagata, Z. Okinawa Child Health Study Group. Association between maternal smoking during pregnancy and low birth weight: Effects by maternal age. PLoS ONE 2016, 11, e0146241. [Google Scholar] [CrossRef]
- Shah, T.; Sullivan, K.; Carter, J. Sudden infant death syndrome and reported maternal smoking during pregnancy. Am. J. Public Health 2006, 96, 1757–1759. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.L.; Lehti, V.; Lampi, K.M.; Helenius, H.; Suominen, A.; Gissler, M.; Brown, A.S.; Sourander, A. Smoking during pregnancy and risk of autism spectrum disorder in a Finnish national birth cohort. Paediatr. Perinat. Epidemiol. 2013, 27, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Longo, L.D. The biological effects of carbon monoxide on the pregnant woman, fetus, and newborn infant. Am. J. Obstet. Gynecol. 1977, 129, 69–103. [Google Scholar] [CrossRef]
- Seidman, D.; Mashiach, S. Involuntary smoking and pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 1991, 41, 105–116. [Google Scholar] [CrossRef]
- Smith, K.R. Biofuels, Air Pollution, and Health: A Global Review, 1st ed.; Plenum Press: New York, NY, USA, 1987; pp. 369–373. ISBN 978-1-4613-0891-1. [Google Scholar]
- Boy, E.; Bruce, N.; Delgado, H. Birth weight and exposure to kitchen wood smoke during pregnancy in rural Guatemala. Environ. Health Perspect. 2002, 110, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.R.; Samet, J.M.; Romieu, I.; Bruce, N. Indoor air pollution in developing countries and acute lower respiratory infections in children. Thorax 2000, 55, 518–532. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, M.; Kammen, D.M. Quantifying the effects of exposure to indoor air pollution from biomass combustion on acute respiratory infections in developing countries. Environ. Health Perspect. 2001, 109, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Bruce, N.; Perez-Padilla, R.; Albalak, R. Indoor air pollution in developing countries: A major environmental and public health challenge. Bull. World Health Organ. 2000, 78, 1078–1092. [Google Scholar] [PubMed]
- Pathirathna, M.L.; Sekijima, K.; Sadakata, M.; Fujiwara, N.; Muramatsu, Y.; Wimalasiri, K.M. Impact of Second Trimester Maternal Dietary Intake on Gestational Weight Gain and Neonatal Birth Weight. Nutrients 2017, 9, 627. [Google Scholar] [CrossRef] [PubMed]
- piCO+TM Smokerlyzer® Operating Manual. Available online: https://www.bedfont.com/file.php?f=ZmlsZSMjNzE0 (accessed on 18 December 2016).
- Yucra, S.; Tapia, V.; Steenland, K.; Naeher, L.P.; Gonzales, G.F. Maternal exposure to biomass smoke and carbon monoxide in relation to adverse pregnancy outcome in two high altitude cities of Peru. Environ. Res. 2014, 130, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141–1143. [Google Scholar] [CrossRef] [PubMed]
- Pope, D.P.; Mishra, V.; Thompson, L.; Siddiqui, A.R.; Rehfuess, E.A.; Weber, M.; Bruce, N.G. Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol. Rev. 2010, 32, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.R.; Gold, E.B.; Yang, X.; Lee, K.; Brown, K.H.; Bhutta, Z.A. Prenatal exposure to wood fuel smoke and low birth weight. Environ. Health Perspect. 2008, 116, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Gomez, C.; Berlin, I.; Marquis, P.; Delcroix, M. Expired air carbon monoxide concentration in mothers and their spouses above 5 ppm is associated with decreased fetal growth. Prev. Med. 2005, 40, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.M.; Bruce, N.; Eskenazi, B.; Diaz, A.; Pope, D.; Smith, K.R. Impact of reduced maternal exposures to wood smoke from an introduced chimney stove on newborn birth weight in rural Guatemala. Environ. Health Perspect. 2011, 119, 1489–1494. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | All (n = 76) | Exposed to Second Hand Tobacco Smoke | Wood Fuel Smoke Exposure | |||
|---|---|---|---|---|---|---|
| Exposed (n = 73) | Not Exposed a n = 3 | |||||
| Yes (n = 26, 34.2%) | No (n = 50, 65.8%) | In a Kitchen with a Chimney (n = 64, 87.7%) | In a Kitchen without a Chimney (n = 9, 12.3%) | |||
| Age (years) † | 29.3 ± 5.7 | 27.8 ± 6.4 | 30.0 ± 5.3 | 29.7 ± 5.7 | 26.8 ± 5.3 | 27.3 ± 6.5 |
| Pre-pregnancy BMI (kg/m2) † | 22.7 ± 4.3 | 22.3 ± 4.5 | 22.9 ± 4.2 | 22.8 ± 4.3 | 22.7 ± 4.6 | 20.0 ± 2.3 |
| Education level, n (%) | ||||||
| Up to primary | 9 (12.0%) | 4 (16.0%) | 5 (10.0%) | 8 (12.7%) | 1 (11.1%) | - |
| Secondary/higher | 66 (88.0%) | 21 (84.0%) | 45 (90.0%) | 55 (87.3%) | 8 (88.9%) | 3 (100.0%) |
| Monthly household income, n (%) | ||||||
| Up to 14,000 LKR | 15 (20.0%) | 4 (16.0%) | 11 (22.0%) | 12 (19.0%) | 3 (33.3%) | - |
| 14,000 to 32,000 LKR | 51 (68.0%) | 18 (72.0%) | 33 (66.0%) | 43 (68.2%) | 6 (66.7%) | 2 (66.7%) |
| ≥32,000 LKR | 9 (12.0%) | 3 (12.0%) | 6 (12.0%) | 8 (12.7%) | - | 1 (33.3%) |
| Residential area, n (%) | ||||||
| Urban | 7 (9.3%) | 3 (12.0%) | 4 (8.0%) | 7 (11.1%) | - | - |
| Sub-urban | 35(46.7%) | 11 (44.0%) | 24 (48.0%) | 30 (47.6%) | 4 (44.4%) | 1 (33.3%) |
| Rural | 33 (44.0%) | 11 (44.0%) | 22 (44.0%) | 26 (41.3%) | 5 (55.6%) | 2 (66.7%) |
| Parity, n (%) | ||||||
| Primiparous | 23 (30.3%) | 7 (26.9%) | 16 (32.0%) | 15 (23.4%) | 5 (55.6%) | 3 (100.0%) |
| Multiparous | 53 (69.7%) | 19 (73.1%) | 34 (68.0%) | 49 (76.6%) | 4 (44.4%) | - |
| Previous history of LBW, n (%) | ||||||
| Yes | 14 (18.4%) | 6 (23.1%) | 8 (16.0%) | 12 (18.8%) | 2 (22.2%) | - |
| No | 62 (81.6%) | 20 (76.9%) | 42 (84.0%) | 52 (81.2%) | 7 (77.8%) | 3 (100.0%) |
| History of miscarriage and/or abortion, n (%) | ||||||
| Yes | 20 (26.3%) | 6 (23.1%) | 14 (28.0%) | 18 (28.1%) | 2 (22.2%) | - |
| No | 56 (73.7%) | 20 (76.9%) | 36 (72.0%) | 46 (71.9%) | 7 (77.8%) | 3 (100.0%) |
| Gestational age, weeks b,† | 39.1 ± 1.4 | 38.5 ± 1.8 | 39.2 ± 1.1 | 39.1 ± 1.2 | 38.2 ± 2.4 | 39.0 ± 1.1 |
| Birth weight, n (%) | ||||||
| <2500 g | 13 (17.1%) | 5 (19.2%) | 8 (16.0%) | 10 (15.6%) | 2 (22.2%) | 1 (33.3%) |
| ≥2500 g | 63 (82.9%) | 21 (80.8%) | 42 (84.0%) | 54 (84.4%) | 7 (77.8%) | 2 (66.7%) |
| Hemoglobin levels at booking visit (g/dL) † (n = 70) | 11.5 ± 1.3 | 11.4 ± 1.3 | 11.5 ± 1.2 | 11.5 ± 1.2 | 10.8 ± 1.8 | 11.6 ± 0.4 |
| Anemic at booking visit c, n (%) | 19 (27.1%) | 5 (22.7%) | 14 (29.2%) | 17 (28.3%) | 2 (28.6%) | - |
| Non-anemic at booking visit d, n (%) | 51 (72.9%) | 17 (77.3%) | 34 (70.8%) | 43 (71.7%) | 5 (71.4%) | 3 (100.0%) |
| Hemoglobin levels at third trimester (g/dL) † (n = 52) | 10.9 ± 1.1 | 10.9 ± 1.1 | 10.9 ± 1.1 | 11.0 ± 1.0 | 10.1 ± 1.4 | No data |
| Anemic at third trimester c, n (%) | 25 (48.1%) | 8 (47.1%) | 17 (48.6%) | 20 (44.4%) | 5 (71.4%) | No data |
| Non-anemic at third trimester d, n (%) | 27 (51.9%) | 9 (52.9%) | 18 (51.4%) | 25 (55.6%) | 2 (28.6%) | No data |
| Term | Coefficient | 95% CI | t-Value | p-Value |
|---|---|---|---|---|
| Constant | −2239 | −5558–−1080 | −1.35 | 0.183 |
| Continuous variables | ||||
| Pre-pregnancy BMI | 11.6 | −14.0–−37.2 | 0.91 | 0.368 |
| Gestational age at delivery | 107.3 | 28.3–186.4 | 2.71 | 0.009 ** |
| Categorical variables | ||||
| Area of residence (urban)-reference level | ||||
| Area of residence (sub-urban) | −50 | −436–−335 | −0.26 | 0.795 |
| Area of residence (rural) | 241 | −145–−627 | 1.25 | 0.217 |
| Monthly household income (up to 14,000 LKR)-reference level | ||||
| Monthly household income (14,000-32,000 LKR) | 204 | −75–−483 | 1.46 | 0.148 |
| Monthly household income (32,000 LKR) | 520 | 115–926 | 2.56 | 0.013 ** |
| Previous history of LBW (yes)-reference level | ||||
| Previous history of LBW (no) | 311 | 24–597 | 2.17 | 0.034 ** |
| Parity (primiparous)-reference level | ||||
| Parity (multiparous) | 258 | 6–510 | 2.05 | 0.045 ** |
| n | CO Conc. (ppm) | p-Value | COHb (%) | p-Value | Cooking Time (min) | p-Value | GA (Weeks) | p-Value | Birth Weight (g) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Second-hand tobacco smoke exposure | Yes | All a | 26 | 1.885 (0.178) | 0.104 a,h 0.205 b,e 0.099 c,d 0.102 c,f 0.633 d,f | 0.969 (0.049) | 0.445 a,h 0.099 b,e 0.109 c,d 0.109 c,f 0.798 d,f | 108 (14) | 0.054 a,h 0.666 b,e 0.721 c,d 0.721 c,f 0.488 d,f | 38.5 (0.4) | 0.078 a,h 0.045 b,e,** 0.523 c,d 0.523 c,f 0.367 d,f | 2865 (107) | 0.408 a,h 0.046 b,e,** 0.857 c,d 0.028 c,f,** 0.381 d,f | |
| Daily | All b | 16 | 2.063 (0.232) | 1.025 (0.073) | 113 (21) | 38.0 (0.5) | 2703 (135) | |||||||
| With kitchen chimney c | 13 | 2.231 (0.257) | 1.061 (0.086) | 111(25) | 38.4 (0.4) | 2722 (135) | ||||||||
| Without kitchen chimney d | 3 | 1.330 (0.333) | 0.867 (0.067) | 123 (20) | 36.6 (2.3) | 2617 (497) | ||||||||
| Once a week | All e | 10 | 1.600 (0.267) | 0.880 (0.041) | 101 (18) | 39.3 (0.3) | 3125 (147) | |||||||
| With kitchen chimney f | 9 | 1.556 (0.294) | 0.889 (0.045) | 102 (20) | 39.3 (0.3) | 3194 (145) | ||||||||
| Without kitchen chimney g | 1 | 2.000 | 0.800 | 90 | 38.9 | 2500 | ||||||||
| No | All h | 50 | 2.340 (0.207) | 1.015 (0.033) | 144 (12) | 39.2 (0.1) | 2972 (71) | |||||||
| Wood-fuel smoke exposure | With kitchen chimney | All i | 64 | 2.078 (0.129) | 0.379 i,l 0.476 j,k 0.323 j,l 0.244 j,m 0.111 k,m 0.262 k,n 0.158 m,n | 0.989 (0.026) | 0.614 i,l 0.991 j,k 0.638 j,l 0.086 j,m 0.071 k,m 0.359 k,n 0.190 m,n | 130 (10) | 0.717 i,l 0.104 j,k 0.236 j,l 0.741 j,m 0.235 k,m 0.688 k,n 0.281 m,n | 39.1 (0.2) | 0.301 i,l 0.103 j,k 0.498 j,l 0.434 j,m 0.610 k,m 0.102 k,n 0.409 m,n | 2968 (65) | 0.268 i,l 0.559 j,k 0.426 j,l 0.441 j,m 0.342 k,m 0.554 k,n 0.538 m,n | |
| Exposed to second-hand tobacco smoke j | 22 | 1.955 (0.203) | 0.991 (0.057) | 107 (17) | 38.8 (0.3) | 2915 (109) | ||||||||
| Not exposed to second-hand tobacco smoke k | 42 | 2.143 (0.165) | 0.988 (0.264) | 142 (13) | 38.2 (0.2) | 2995 (81) | ||||||||
| Without kitchen chimney | All l | 9 | 2.899 (0.873) | 1.067 (0.146) | 138 (19) | 38.2 (0.8) | 2739 (184) | |||||||
| Exposed to second-hand tobacco smoke m | 4 | 1.500 (0.289) | 0.850 (0.050) | 115 (17) | 37.2 (1.7) | 2588 (353) | ||||||||
| Not exposed to second-hand tobacco smoke n | 5 | 4.000 (1.410) | 1.240 (0.242) | 156 (31) | 38.9 (0.3) | 2860 (197) | ||||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pathirathna, M.L.; Abeywickrama, H.M.; Sekijima, K.; Sadakata, M.; Fujiwara, N.; Muramatsu, Y.; Wimalasiri, K.M.S.; Jayawardene, U.; De Silva, D.; Dematawewa, C.M.B. Effects of Prenatal Tobacco and Wood-Fuel Smoke Exposure on Birth Weight in Sri Lanka. Healthcare 2017, 5, 64. https://doi.org/10.3390/healthcare5040064
Pathirathna ML, Abeywickrama HM, Sekijima K, Sadakata M, Fujiwara N, Muramatsu Y, Wimalasiri KMS, Jayawardene U, De Silva D, Dematawewa CMB. Effects of Prenatal Tobacco and Wood-Fuel Smoke Exposure on Birth Weight in Sri Lanka. Healthcare. 2017; 5(4):64. https://doi.org/10.3390/healthcare5040064
Chicago/Turabian StylePathirathna, Malshani L., Hansani M. Abeywickrama, Kayoko Sekijima, Mieko Sadakata, Naoshi Fujiwara, Yoshiyuki Muramatsu, Kuruppu M. S. Wimalasiri, Upali Jayawardene, Darshana De Silva, and Chandraratne M. B. Dematawewa. 2017. "Effects of Prenatal Tobacco and Wood-Fuel Smoke Exposure on Birth Weight in Sri Lanka" Healthcare 5, no. 4: 64. https://doi.org/10.3390/healthcare5040064
APA StylePathirathna, M. L., Abeywickrama, H. M., Sekijima, K., Sadakata, M., Fujiwara, N., Muramatsu, Y., Wimalasiri, K. M. S., Jayawardene, U., De Silva, D., & Dematawewa, C. M. B. (2017). Effects of Prenatal Tobacco and Wood-Fuel Smoke Exposure on Birth Weight in Sri Lanka. Healthcare, 5(4), 64. https://doi.org/10.3390/healthcare5040064