
Reference Intervals for Non-Fasting CVD Lipids and Inflammation Markers in Pregnant Indigenous Australian Women

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
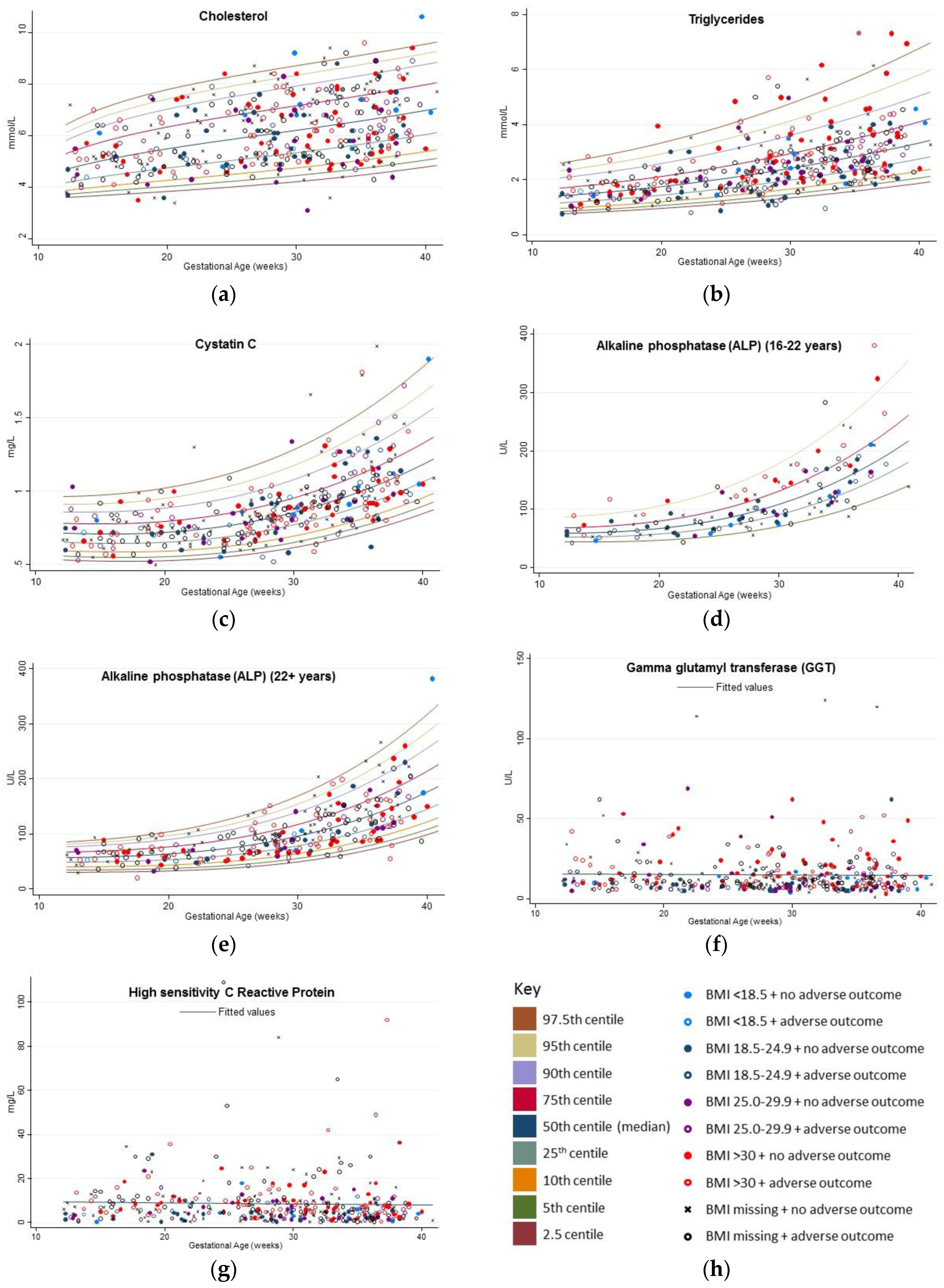
3. Results
Variation in Reference Intervals for Gestational Age
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Available online: http://www.who.int/mediacentre/factsheets/fs310/en/ (accessed on 2 August 2017).
- Australian Bureau of Statistics. Australian Aboriginal and Torres strait Islander Health Survey: Biomedical Results, 2012-13; Australian Bureau of Statistics, Ed.; Commonwealth of Australia: Canberra, Australia, 2014.
- Kelishadi, R.; Poursafa, P. A review on the genetic, environmental, and lifestyle aspects of the early-life origins of cardiovascular disease. Curr. Probl. Pediatr. Adolesc. Health Care 2014, 44, 54–72. [Google Scholar] [CrossRef] [PubMed]
- Juonala, M.; Magnussen, C.G.; Venn, A.; Dwyer, T.; Burns, T.L.; Davis, P.H.; Chen, W.; Srinivasan, S.R.; Daniels, S.R.; Kahonen, M.; et al. Influence of age on associations between childhood risk factors and carotid intima-media thickness in adulthood: The cardiovascular risk in young finns study, the childhood determinants of adult health study, the bogalusa heart study, and the muscatine study for the international childhood cardiovascular cohort (i3c) consortium. Circulation 2010, 122, 2514–2520. [Google Scholar] [PubMed]
- National Vascular Disease Prevention Alliance; Lalor, E.; Boyden, A.; Cadilhac, D.; Colagiur, S.; Doust, J.; Fraser, D.; Harris, M.; Huang, N.; Johnson, D.; et al. Guidelines for the Management of Absolute Cardiovascular Disease Risk; Report 0987283014; National Stroke Foundation: Melbourne, Australia, 2012. [Google Scholar]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., 3rd; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the centers for disease control and prevention and the american heart association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Schreuder, Y.J.; Hutten, B.A.; van Eijsden, M.; Jansen, E.H.; Vissers, M.N.; Twickler, M.T.; Vrijkotte, T.G. Ethnic differences in maternal total cholesterol and triglyceride levels during pregnancy: The contribution of demographics, behavioural factors and clinical characteristics. Eur. J. Clin. Nutr. 2011, 65, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Vrijkotte, T.G.; Krukziener, N.; Hutten, B.A.; Vollebregt, K.C.; van Eijsden, M.; Twickler, M.B. Maternal lipid profile during early pregnancy and pregnancy complications and outcomes: The abcd study. J. Clin. Endocrinol. Metab. 2012, 97, 3917–3925. [Google Scholar] [CrossRef] [PubMed]
- Piechota, W.; Staszewski, A. Reference ranges of lipids and apolipoproteins in pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 1992, 45, 27–35. [Google Scholar] [CrossRef]
- Ryckman, K.K.; Spracklen, C.N.; Smith, C.J.; Robinson, J.G.; Saftlas, A.F. Maternal lipid levels during pregnancy and gestational diabetes: A systematic review and meta-analysis. BJOG 2015, 122, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Mankuta, D.; Elami-Suzin, M.; Elhayani, A.; Vinker, S. Lipid profile in consecutive pregnancies. Lipids Health Dis. 2010, 9, 58. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhong, X.; Cheng, G.; Zhao, C.; Zhang, L.; Hong, Y.; Wan, Q.; He, R.; Wang, Z. Hs-crp and all-cause, cardiovascular, and cancer mortality risk: A meta-analysis. Atherosclerosis 2017, 259, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Kashanian, M.; Aghbali, F.; Mahali, N. Evaluation of the diagnostic value of the first-trimester maternal serum high-sensitivity c-reactive protein level for prediction of pre-eclampsia. J. Obstet. Gynaecol. Res. 2013, 39, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.S.; Kwon, J.Y.; Kim, M.A.; Park, Y.W.; Kim, Y.H. Maternal serum highly sensitive c-reactive protein in normal pregnancy and pre-eclampsia. Int. J. Gynaecol. Obstet. 2007, 98, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Apekey, T.A.; Khan, H. Liver enzymes and risk of cardiovascular disease in the general population: A meta-analysis of prospective cohort studies. Atherosclerosis 2014, 236, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Bakker, S.J.; Kootstra-Ros, J.E.; Gansevoort, R.T.; Gregson, J.; Dullaart, R.P. Serum alkaline phosphatase and risk of incident cardiovascular disease: Interrelationship with high sensitivity c-reactive protein. PLoS ONE 2015, 10, e0132822. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Song, L.; Zhao, L.; Dong, P.; Lai, L.; Wang, H. Predictive value of cystatin c in people with suspected or established coronary artery disease: A meta-analysis. Atherosclerosis 2017, 263, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, K.; Lindstrom, V.; Schmidt, C.; Blirup-Jensen, S.; Grubb, A.; Wide-Swensson, D.; Strevens, H. Temporal changes of the plasma levels of cystatin c, beta-trace protein, beta2-microglobulin, urate and creatinine during pregnancy indicate continuous alterations in the renal filtration process. Scand. J. Clin. Lab. Investig. 2007, 67, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Ashman, A.M.; Collins, C.E.; Weatherall, L.; Brown, L.J.; Rollo, M.E.; Clausen, D.; Blackwell, C.C.; Pringle, K.G.; Attia, J.; Smith, R.; et al. A cohort of indigenous australian women and their children through pregnancy and beyond: The gomeroi gaaynggal study. J. Dev. Orig. Health Dis. 2016, 7, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Royston, P.; Wright, E.M. Goodness-of-fit statistics for age-specific reference intervals. Stat. Med. 2000, 19, 2943–2962. [Google Scholar] [CrossRef]
- Pathology North and NSW Government Health Pathology. Labinfo Test Directory. Available online: http://www.palms.com.au/php/labinfo/index.php (accessed on 15 June 2017).
- Koerbin, G.; Sikaris, K.A.; Jones, G.R.; Ryan, J.; Reed, M.; Tate, J. Evidence-based approach to harmonised reference intervals. Clin. Chim. Acta 2014, 432, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Langsted, A.; Freiberg, J.J.; Nordestgaard, B.G. Fasting and nonfasting lipid levels: Influence of normal food intake on lipids, lipoproteins, apolipoproteins, and cardiovascular risk prediction. Circulation 2008, 118, 2047–2056. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, Y.; Conroy, S.M.; Ollberding, N.J.; Kim, Y.; Lim, U.; Cooney, R.V.; Franke, A.A.; Wilkens, L.R.; Hernandez, B.Y.; Goodman, M.T.; et al. Ethnic differences in serum adipokine and c-reactive protein levels: The multiethnic cohort. Int. J. Obes. 2014, 38, 1416–1422. [Google Scholar] [CrossRef] [PubMed]
- Veeranna, V.; Zalawadiya, S.K.; Niraj, A.; Kumar, A.; Ference, B.; Afonso, L. Association of novel biomarkers with future cardiovascular events is influenced by ethnicity: Results from a multi-ethnic cohort. Int. J. Cardiol. 2013, 166, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, S.; Matsuzawa, Y.; Tokunaga, K.; Tarui, S. Contribution of intra-abdominal fat accumulation to the impairment of glucose and lipid metabolism in human obesity. Metabolism 1987, 36, 54–59. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 47270do009_20122013 Australian Aboriginal and Torres Strait Islander Health Survey: First Results, 2012-13—Australia; Commonwealth of Australia: Canberra, Australian, 2014.
- Eshriqui, I.; Franco-Sena, A.B.; Farias, D.R.; Freitas-Vilela, A.A.; Cunha, D.B.; Barros, E.G.; Emmett, P.M.; Kac, G. Prepregnancy dietary patterns are associated with blood lipid level changes during pregnancy: A prospective cohort study in rio de janeiro, brazil. J. Acad. Nutr. Diet. 2017, 117, 1066.e1–1079.e1. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.L.; Siega-Riz, A.M.; Sotres-Alvarez, D.; Robinson, W.R.; Daniels, J.L.; Perrin, E.M.; Stuebe, A.M. Maternal dietary patterns are associated with lower levels of cardiometabolic markers during pregnancy. Paediatr. Perinat. Epidemiol. 2016, 30, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Salehi-Abargouei, A.; Maghsoudi, Z.; Shirani, F.; Azadbakht, L. Effects of dietary approaches to stop hypertension (dash)-style diet on fatal or nonfatal cardiovascular diseases–incidence: A systematic review and meta-analysis on observational prospective studies. Nutrition 2013, 29, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Esmaillzadeh, A. Vitamin d supplementation affects serum high-sensitivity c-reactive protein, insulin resistance, and biomarkers of oxidative stress in pregnant women. J. Nutr. 2013, 143, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Ranasinghe, P.; Wathurapatha, W.S.; Ishara, M.H.; Jayawardana, R.; Galappatthy, P.; Katulanda, P.; Constantine, G.R. Effects of zinc supplementation on serum lipids: A systematic review and meta-analysis. Nutr. Metab. 2015, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Rahmat, A.; Patimah, I.; Khaza’ai, H.; Abed, Y. Effect of vitamin c on inflammation and metabolic markers in hypertensive and/or diabetic obese adults: A randomized controlled trial. Drug Des. Dev. Ther. 2015, 9, 3405–3412. [Google Scholar] [CrossRef] [PubMed]
- Ashman, A.M.; Collins, C.E.; Weatherall, L.J.; Keogh, L.; Brown, L.J.; Rollo, M.E.; Smith, R.; Rae, K.M. Dietary intakes and anthropometric measures of indigenous australian women and their infants in the gomeroi gaaynggal cohort. J. Dev. Orig. Health Dis. 2016, 7, 481–497. [Google Scholar] [CrossRef] [PubMed]
- Ordovas, J.M.; Pocovi, M.; Grande, F. Plasma lipids and cholesterol esterification rate during pregnancy. Obstet. Gynecol. 1984, 63, 20–25. [Google Scholar] [PubMed]
- Forey, B.A.; Fry, J.S.; Lee, P.N.; Thornton, A.J.; Coombs, K.J. The effect of quitting smoking on hdl-cholesterol—A review based on within-subject changes. Biomark. Res. 2013, 1, 26. [Google Scholar] [CrossRef] [PubMed]
- Novakov Mikic, A.; Cabarkapa, V.; Nikolic, A.; Maric, D.; Brkic, S.; Mitic, G.; Ristic, M.; Stosic, Z. Cystatin c in pre-eclampsia. J. Matern. Fetal Neonatal Med. 2012, 25, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Vieira, M.C.; Poston, L.; Fyfe, E.; Gillett, A.; Kenny, L.C.; Roberts, C.T.; Baker, P.N.; Myers, J.E.; Walker, J.J.; McCowan, L.M.; et al. Clinical and biochemical factors associated with preeclampsia in women with obesity. Obesity 2017, 25, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Sattar, N.; Papcosta, O.; Lennon, L.; Whincup, P.H. Alkaline phosphatase, serum phosphate, and incident cardiovascular disease and total mortality in older men. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Picklesimer, A.H.; Jared, H.L.; Moss, K.; Offenbacher, S.; Beck, J.D.; Boggess, K.A. Racial differences in c-reactive protein levels during normal pregnancy. Am. J. Obstet. Gynecol. 2008, 199, 523.e1–523.e6. [Google Scholar] [CrossRef] [PubMed]
- Ertas, I.E.; Kahyaoglu, S.; Yilmaz, B.; Ozel, M.; Sut, N.; Guven, M.A.; Danisman, N. Association of maternal serum high sensitive c-reactive protein level with body mass index and severity of pre-eclampsia at third trimester. J. Obstet. Gynaecol. Res. 2010, 36, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, M.; Heidari-Bakavoli, A.R.; Shoeibi, S.; Mirhafez, S.R.; Moohebati, M.; Esmaily, H.; Ghazavi, H.; Saberi Karimian, M.; Parizadeh, S.M.; Mohammadi, M.; et al. Association of serum hs-crp levels with the presence of obesity, diabetes mellitus, and other cardiovascular risk factors. J. Clin. Lab. Anal. 2016, 30, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Sharma, U.; Pal, D.; Prasad, R. Alkaline phosphatase: An overview. Indian J. Clin. Biochem. 2014, 29, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.; Palm, M.; Hansson, L.O.; Axelsson, O. Reference values for clinical chemistry tests during normal pregnancy. BJOG 2008, 115, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Borghi, E.; de Onis, M.; Garza, C.; Van den Broeck, J.; Frongillo, E.A.; Grummer-Strawn, L.; Van Buuren, S.; Pan, H.; Molinari, L.; Martorell, R.; et al. Construction of the world health organization child growth standards: Selection of methods for attained growth curves. Stat. Med. 2006, 25, 247–265. [Google Scholar] [CrossRef] [PubMed]
- Pottel, H.; Vrydags, N.; Mahieu, B.; Vandewynckele, E.; Croes, K.; Martens, F. Establishing age/sex related serum creatinine reference intervals from hospital laboratory data based on different statistical methods. Clin. Chim. Acta 2008, 396, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Van Eijsden, M.; van der Wal, M.F.; Hornstra, G.; Bonsel, G.J. Can whole-blood samples be stored over 24 hours without compromising stability of c-reactive protein, retinol, ferritin, folic acid, and fatty acids in epidemiologic research? Clin. Chem. 2005, 51, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Cuhadar, S.; Atay, A.; Koseoglu, M.; Dirican, A.; Hur, A. Stability studies of common biochemical analytes in serum separator tubes with or without gel barrier subjected to various storage conditions. Biochem. Med. 2012, 22, 202–214. [Google Scholar] [CrossRef]


{kind=link}
| Demographic & Health Characteristic | Number of Pregnancies with Data (n = 206) | Mean (SD 1) | Median (IQR 2) |
|---|---|---|---|
| Age (at time of consent) (years) | (206) | 25.5 (6.1) | 24.3 (21.0–29.0) |
| Self-reported pre-pregnancy weight (kg) | (124) | 79.1 (23.9) | 76.5 (60.5–92.1) |
| BMI 3 based on pre-pregnancy weight (kg·m−2) | (114) | 30.0 (8.4) | 28.8 (22.9–36.6) |
| n | (%) | ||
| BMI: underweight (<18.5) | 7 | (6.1%) | |
| BMI: normal (18.5–24.99) | 31 | (27.2%) | |
| BMI: overweight (25–29.99) | 24 | (21.1%) | |
| BMI: obese (30 or higher) | 52 | (45.6%) | |
| Reported smoking during pregnancy | (185) | 63 | (34.1%) |
| Self-reported diabetes status at consent 4 | (117) | 7 | (6.1%) |
| (type 1) | - | 3 | (2.6%) |
| (type 2) | - | 4 | (3.4%) |
| Developed gestational diabetes in prior pregnancy | (180) | 18 | (8.7%) |
| Self-reported hypertensive at consent 4 | (116) | 6 | (5.2%) |
| (don’t know/unsure) | - | 4 | (3.5%) |
| Developed gestational hypertension in prior pregnancy | (185) | 11 | (5.3%) |
| Developed preeclampsia in prior pregnancy | (184) | 14 | (6.8%) |
| Self-reported IHD 4,5 status at consent | (113) | 0 | (0%) |
| (don’t know/unsure) | - | 3 | (2.7%) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schumacher, T.L.; Oldmeadow, C.; Clausen, D.; Weatherall, L.; Keogh, L.; Pringle, K.G.; Rae, K.M. Reference Intervals for Non-Fasting CVD Lipids and Inflammation Markers in Pregnant Indigenous Australian Women. Healthcare 2017, 5, 72. https://doi.org/10.3390/healthcare5040072
Schumacher TL, Oldmeadow C, Clausen D, Weatherall L, Keogh L, Pringle KG, Rae KM. Reference Intervals for Non-Fasting CVD Lipids and Inflammation Markers in Pregnant Indigenous Australian Women. Healthcare. 2017; 5(4):72. https://doi.org/10.3390/healthcare5040072
Chicago/Turabian StyleSchumacher, Tracy L., Christopher Oldmeadow, Don Clausen, Loretta Weatherall, Lyniece Keogh, Kirsty G. Pringle, and Kym M. Rae. 2017. "Reference Intervals for Non-Fasting CVD Lipids and Inflammation Markers in Pregnant Indigenous Australian Women" Healthcare 5, no. 4: 72. https://doi.org/10.3390/healthcare5040072