Pain and Pain Medication among Older People with Intellectual Disabilities in Comparison with the General Population



Abstract
1. Introduction
2. Materials and Methods
2.1. Registers
2.2. Study Cohorts
2.3. Pain
2.4. Pain Medication
2.5. Ethics Approval
2.6. Statistics
3. Results
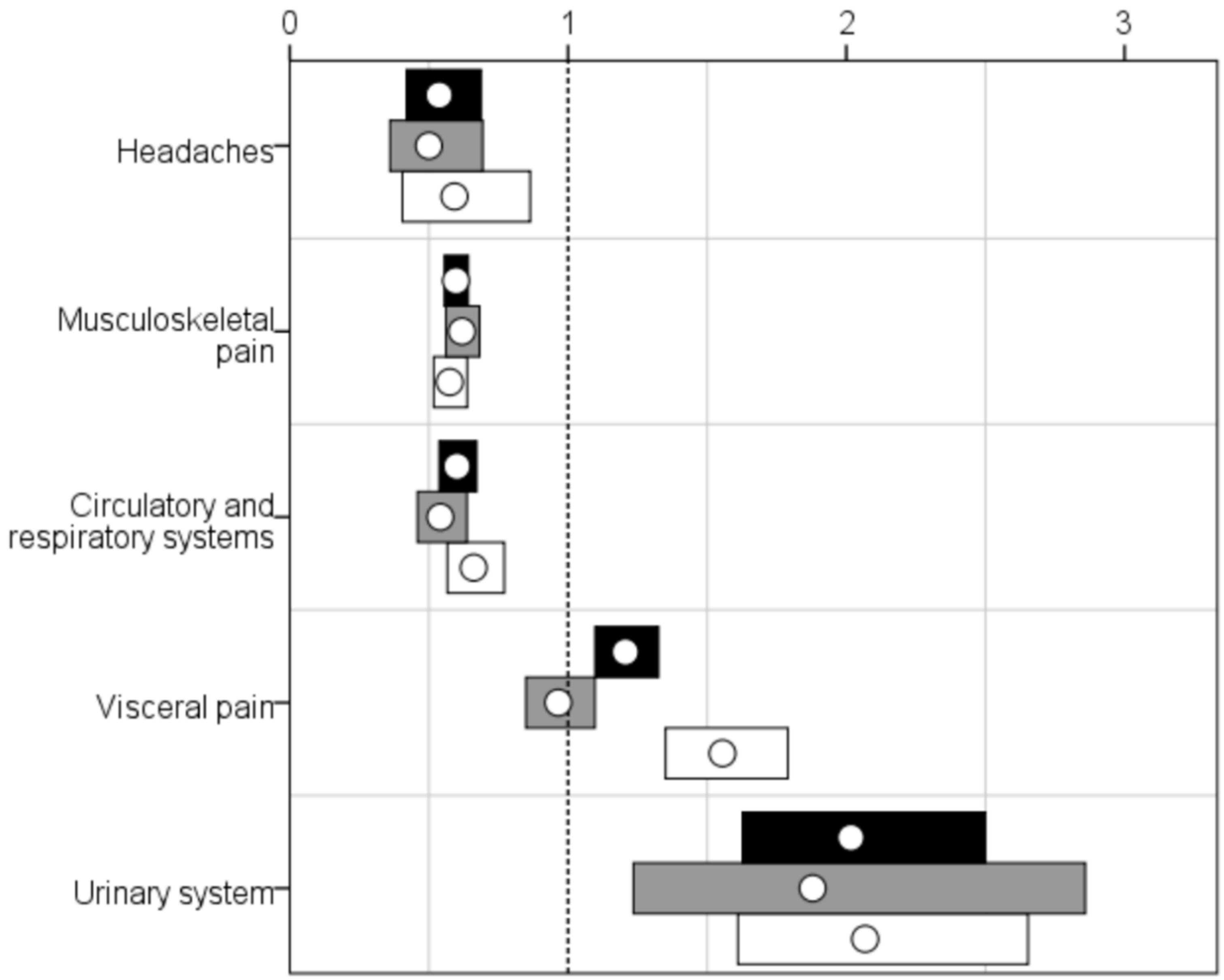
3.1. Pain
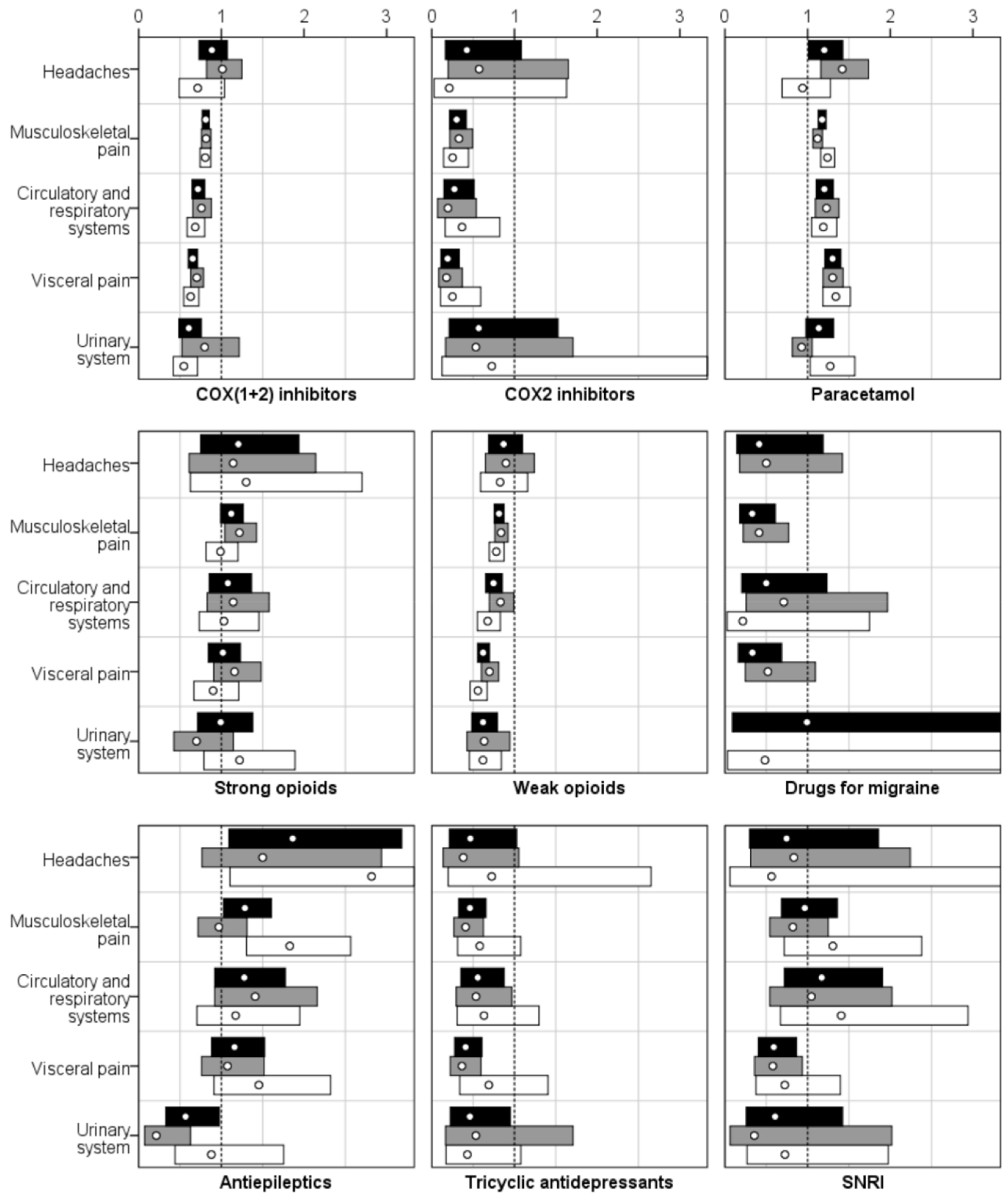
3.2. Pain Medication
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- IASP Task Force on Taxonomy. Classification of chronic pain. In Part III: Pain Terms, a Current List with Definitions and Notes on Usage; Merskey, H., Bogduk, N., Eds.; IASP Press: Seattle, WA, USA, 1994. [Google Scholar]
- International Association for the Study of Pain. IASP Terminology. Available online: https://www.iasp-pain.org/terminology (accessed on 10 April 2018).
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed]
- Tsang, A.; von Korff, M.; Lee, S.; Alonso, J.; Karam, E.; Angermeyer, M.C.; Borges, G.L.; Bromet, E.J.; Demytteneare, K.; de Girolamo, G.; et al. Common chronic pain conditions in developed and developing countries: Gender and age differences and comorbidity with depression-anxiety disorders. J. Pain 2008, 9, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Hooten, W.M. Chronic pain and mental health disorders: Shared neural mechanisms, epidemiology, and treatment. Mayo Clin. Proc. 2016, 91, 955–970. [Google Scholar] [CrossRef] [PubMed]
- Fillingim, R.B.; Bruehl, S.; Dworkin, R.H.; Dworkin, S.F.; Loeser, J.D.; Turk, D.C.; Widerstrom-Noga, E.; Arnold, L.; Bennett, R.; Edwards, R.R.; et al. The acttion-american pain society pain taxonomy (AAPT): An evidence-based and multidimensional approach to classifying chronic pain conditions. J. Pain 2014, 15, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S.J.; Lussier, D. Prevalence and relevance of pain in older persons. Pain Med. 2012, 13 (Suppl. 2), S23–S26. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Binnekade, T.; Eggermont, L.; Sepehry, A.A.; Patchay, S.; Schofield, P. Pain and the risk for falls in community-dwelling older adults: Systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2014, 95, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Horgas, A.L. Pain assessment in older adults. Nurs. Clin. N. Am. 2017, 52, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, J.; Larsen, D. Assessing pain in cognitively impaired older adults. Nurs. Stand. 2004, 18, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Curtiss, C.P. Challenges in pain assessment in cognitively intact and cognitively impaired older adults with cancer. Oncol. Nurs. Forum 2010, 37, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Eisenberg, E.; O’Brien, T. The individual and societal burden of chronic pain in europe: The case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Fain, K.; Alexander, G.C.; Dore, D.D.; Segal, J.B.; Zullo, A.R.; Castillo-Salgado, C. Frequency and predictors of analgesic prescribing in U.S. Nursing home residents with persistent pain. J. Am. Geriatr. Soc. 2017, 65, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Shipton, E.A.; Shipton, E.E.; Shipton, A.J. A review of the opioid epidemic: What do we do about it? Pain Ther. 2018, 7, 23–36. [Google Scholar] [CrossRef] [PubMed]
- de Knegt, N.; Lobbezoo, F.; Schuengel, C.; Evenhuis, H.M.; Scherder, E.J. Self-reporting tool on pain in people with intellectual disabilities (stop-id!): A usability study. Augment. Altern. Commun. 2016, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.; Morrison, T.G.; McGuire, B.E. Chronic pain in adults with an intellectual disability: Prevalence, impact, and health service use based on caregiver report. Pain 2011, 152, 1951–1957. [Google Scholar] [CrossRef] [PubMed]
- Turk, V.; Khattran, S.; Kerry, S.; Corney, R.; Painter, K. Reporting of health problems and pain by adults with an intellectual disability and by their carers. J. Appl. Res. Intell. Disabil. 2012, 25, 155–165. [Google Scholar] [CrossRef] [PubMed]
- de Knegt, N.; Scherder, E. Pain in adults with intellectual disabilities. Pain 2011, 152, 971–974. [Google Scholar] [CrossRef] [PubMed]
- Boerlage, A.A.; Valkenburg, A.J.; Scherder, E.J.; Steenhof, G.; Effing, P.; Tibboel, D.; van Dijk, M. Prevalence of pain in institutionalized adults with intellectual disabilities: A cross-sectional approach. Res. Dev. Disabil. 2013, 34, 2399–2406. [Google Scholar] [CrossRef] [PubMed]
- McGuire, B.E.; Daly, P.; Smyth, F. Chronic pain in people with an intellectual disability: Under-recognised and under-treated? J. Intell. Disabil. Res. 2010, 54, 240–245. [Google Scholar] [CrossRef]
- Amor-Salamanca, A.; Menchon, J.M. Pain underreporting associated with profound intellectual disability in emergency departments. J. Intell. Disabil. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Baldridge, K.H.; Andrasik, F. Pain assessment in people with intellectual or developmental disabilities. Am. J. Nurs. 2010, 110, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Findlay, L.; Williams, A.C.; Scior, K. Exploring experiences and understandings of pain in adults with intellectual disabilities. J. Intell. Disabil. Res. 2014, 58, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Kankkunen, P.; Janis, P.; Vehvilainen-Julkunen, K. Pain assessment among non-communicating intellectually disabled people described by nursing staff. Open Nurs. J. 2010, 4, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Turk, V.; Kerry, S.; Corney, R.; Rowlands, G.; Khattran, S. Why some adults with intellectual disability consult their general practitioner more than others. J. Intell. Disabil. Res. 2010, 54, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, O.; McGuire, B.E.; Finn, D.P. The effect of pain on cognitive function: A review of clinical and preclinical research. Prog. Neurobiol. 2011, 93, 385–404. [Google Scholar] [CrossRef] [PubMed]
- Passmore, P.; Cunningham, E. Pain assessment in cognitive impairment. J. Pain Palliat. Care Pharmacother. 2014, 28, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Zis, P.; Daskalaki, A.; Bountouni, I.; Sykioti, P.; Varrassi, G.; Paladini, A. Depression and chronic pain in the elderly: Links and management challenges. Clin. Interv. Aging 2017, 12, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Snowden, M.B.; Steinman, L.E.; Bryant, L.L.; Cherrier, M.M.; Greenlund, K.J.; Leith, K.H.; Levy, C.; Logsdon, R.G.; Copeland, C.; Vogel, M.; et al. Dementia and co-occurring chronic conditions: A systematic literature review to identify what is known and where are the gaps in the evidence? Int. J. Geriatr. Psychiatry 2017, 32, 357–371. [Google Scholar] [CrossRef] [PubMed]
- Wranker, L.S.; Rennemark, M.; Berglund, J. Pain among older adults from a gender perspective: Findings from the swedish national study on aging and care (SNAC-blekinge). Scand. J. Public Health 2016, 44, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Kaye, A.D.; Baluch, A.; Scott, J.T. Pain management in the elderly population: A review. Ochsner J. 2010, 10, 179–187. [Google Scholar] [PubMed]
- Jones, M.R.; Ehrhardt, K.P.; Ripoll, J.G.; Sharma, B.; Padnos, I.W.; Kaye, R.J.; Kaye, A.D. Pain in the elderly. Curr. Pain Headache Rep. 2016, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Coppus, A. People with intellectual disability: What do we know about adulthood and life expectancy? Dev. Disabil. Res. Rev. 2013, 18, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.; Kettl, P. Aging with mental retardation: Increasing population of older adults with mr require health interventions and prevention strategies. Geriatrics 2005, 60, 26–29. [Google Scholar] [PubMed]
- Axmon, A.; Sandberg, M.; Ahlström, G.; Midlöv, P. Prescription of potentially inappropriate medications among older people with intellectual disability: A register study. BMC Pharmacol. Toxicol. 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Wettermark, B.; Hammar, N.; Fored, C.M.; Leimanis, A.; Otterblad Olausson, P.; Bergman, U.; Persson, I.; Sundström, A.; Westerholm, B.; Rosén, M. The new swedish prescribed drug register—Opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol. Drug Saf. 2007, 16, 726–735. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for Atc Classification and Ddd Assignment 2018; WHO: Oslo, Norway, 2017. [Google Scholar]
- Pergolizzi, J.; Boger, R.H.; Budd, K.; Dahan, A.; Erdine, S.; Hans, G.; Kress, H.G.; Langford, R.; Likar, R.; Raffa, R.B.; et al. Opioids and the management of chronic severe pain in the elderly: Consensus statement of an international expert panel with focus on the six clinically most often used world health organization step III opioids (buprenorphine, fentanyl, hydromorphone, methadone, morphine, oxycodone). Pain Pract. 2008, 8, 287–313. [Google Scholar] [PubMed]
- Driscoll, M.; Kerns, R.D. Integrated, team-based chronic pain management: Bridges from theory and research to high quality patient care. Adv. Exp. Med. Biol. 2016, 904, 131–147. [Google Scholar] [PubMed]
- Palomba, S.; Di Cello, A.; Riccio, E.; Manguso, F.; La Sala, G.B. Ovarian function and gastrointestinal motor activity. Min. Endocrinol. 2011, 36, 295–310. [Google Scholar]
- Heitkemper, M.M.; Chang, L. Do fluctuations in ovarian hormones affect gastrointestinal symptoms in women with irritable bowel syndrome? Gend. Med. 2009, 6 (Suppl. 2), 152–167. [Google Scholar] [CrossRef] [PubMed]
- Wicksell, R.K.; Ahlqvist, J.; Bring, A.; Melin, L.; Olsson, G.L. Can exposure and acceptance strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (wad)? A randomized controlled trial. Cogn. Behav. Ther. 2008, 37, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Casey, M.; Smart, K.; Segurado, R.; Hearty, C.; Gopal, H.; Lowry, D.; Flanagan, D.; McCracken, L.; Doody, C. Exercise combined with acceptance and commitment therapy (exact) compared to a supervised exercise programme for adults with chronic pain: Study protocol for a randomised controlled trial. Trials 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Polatin, P.; Bevers, K.; Gatchel, R.J. Pharmacological treatment of depression in geriatric chronic pain patients: A biopsychosocial approach integrating functional restoration. Expert Rev. Clin. Pharmacol. 2017, 10, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Peklar, J.; Kos, M.; O’Dwyer, M.; McCarron, M.; McCallion, P.; Kenny, R.A.; Henman, M.C. Medication and supplement use in older people with and without intellectual disability: An observational, cross-sectional study. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Trescot, A.M.; Helm, S.; Hansen, H.; Benyamin, R.; Glaser, S.E.; Adlaka, R.; Patel, S.; Manchikanti, L. Opioids in the management of chronic non-cancer pain: An update of american society of the interventional pain physicians’ (ASIPP) guidelines. Pain Physician 2008, 11, S5–S62. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Type of Pain | gPop | Intellectual Disabilities (ID) | ||||
|---|---|---|---|---|---|---|
| Women | Men | Total | Women | Men | Total | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Headaches | 106 (2.9) | 71 (1.6) | 177 (2.2) | 53 (1.5) | 42 (1.0) | 95 (1.2) |
| Musculoskeletal pain | 868 (24.1) | 835 (19.3) | 1703 (21.5) | 537 (14.9) | 480 (11.1) | 1017 (12.8) |
| Pain related to the circulatory and respiratory systems | 381 (10.6) | 380 (8.8) | 761 (9.6) | 206 (5.7) | 251 (5.8) | 457 (5.8) |
| Visceral pain | 422 (11.7) | 292 (6.7) | 714 (9.0) | 407 (11.3) | 454 (10.5) | 861 (10.8) |
| Pain related to the urinary system | 33 (0.9) | 89 (2.1) | 122 (1.5) | 62 (1.7) | 184 (4.3) | 246 (3.1) |
| Type of Medication | gPop | ID | ||||
|---|---|---|---|---|---|---|
| Women | Men | Total | Women | Men | Total | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Headaches | ||||||
| COX(1+2) inhibitors | 75 (71) | 45 (63) | 120 (68) | 38 (72) | 19 (45) | 57 (60) |
| COX2 inhibitors | 14 (13) | 8 (11) | 22 (12) | 4 (8) | 1 (2) | 5 (5) |
| Paracetamol | 62 (58) | 45 (63) | 107 (60) | 44 (83) | 25 (60) | 69 (73) |
| Strong opioids | 21 (20) | 13 (18) | 34 (19) | 12 (23) | 10 (24) | 22 (23) |
| Weak opioids | 58 (55) | 45 (63) | 103 (58) | 26 (49) | 22 (52) | 48 (51) |
| Drugs for migraine | 16 (15) | 2 (3) | 18 (10) | 4 (8) | 0 (0) | 4 (4) |
| Antiepileptics | 16 (15) | 6 (8) | 22 (12) | 12 (23) | 10 (24) | 22 (23) |
| Tricyclic antidepressants | 21 (20) | 7 (10) | 28 (16) | 4 (8) | 3 (7) | 7 (7) |
| SNRI (Serotonin-norepinephrine reuptake inhibitor) | 12 (11) | 3 (4) | 15 (8) | 5 (9) | 1 (2) | 6 (6) |
| Musculoskeletal Pain | ||||||
| COX(1+2) inhibitors | 694 (80) | 637 (76) | 1331 (78) | 350 (65) | 295 (61) | 645 (63) |
| COX2 inhibitors | 128 (15) | 90 (11) | 218 (13) | 26 (5) | 13 (3) | 39 (4) |
| Paracetamol | 664 (76) | 536 (64) | 1200 (70) | 460 (86) | 382 (80) | 842 (83) |
| Strong opioids | 248 (29) | 211 (25) | 459 (27) | 187 (35) | 120 (25) | 307 (30) |
| Weak opioids | 548 (63) | 482 (58) | 1030 (60) | 284 (53) | 216 (45) | 500 (49) |
| Drugs for migraine | 47 (5) | 14 (2) | 61 (4) | 12 (2) | 0 (0) | 12 (1) |
| Antiepileptics | 100 (12) | 59 (7) | 159 (9) | 60 (11) | 62 (13) | 122 (12) |
| Tricyclic antidepressants | 99 (11) | 39 (5) | 138 (8) | 25 (5) | 13 (3) | 38 (4) |
| SNRI | 61 (7) | 24 (3) | 85 (5) | 31 (6) | 18 (4) | 49 (5) |
| Pain Related to the Circulatory and Respiratory Systems | ||||||
| COX(1+2) inhibitors | 263 (69) | 250 (66) | 513 (67) | 108 (52) | 113 (45) | 221 (48) |
| COX2 inhibitors | 38 (10) | 29 (8) | 67 (9) | 4 (2) | 7 (3) | 11 (2) |
| Paracetamol | 229 (60) | 210 (55) | 439 (58) | 152 (74) | 165 (66) | 317 (69) |
| Strong opioids | 76 (20) | 66 (17) | 142 (19) | 47 (23) | 45 (18) | 92 (20) |
| Weak opioids | 207 (54) | 186 (49) | 393 (52) | 93 (45) | 83 (33) | 176 (39) |
| Drugs for migraine | 13 (3) | 7 (2) | 20 (3) | 5 (2) | 1 (0) | 6 (1) |
| Antiepileptics | 42 (11) | 31 (8) | 73 (10) | 32 (16) | 24 (10) | 56 (12) |
| Tricyclic antidepressants | 45 (12) | 24 (6) | 69 (9) | 13 (6) | 10 (4) | 23 (5) |
| SNRI | 23 (6) | 14 (4) | 37 (5) | 13 (6) | 13 (5) | 26 (6) |
| Visceral Pain | ||||||
| COX(1+2) inhibitors | 314 (74) | 182 (62) | 496 (69) | 213 (52) | 178 (39) | 391 (45) |
| COX2 inhibitors | 47 (11) | 18 (6) | 65 (9) | 8 (2) | 7 (2) | 15 (2) |
| Paracetamol | 254 (60) | 154 (53) | 408 (57) | 319 (78) | 321 (71) | 640 (74) |
| Strong opioids | 93 (22) | 60 (21) | 153 (21) | 104 (26) | 84 (19) | 188 (22) |
| Weak opioids | 177 (42) | 99 (34) | 276 (39) | 129 (32) | 95 (21) | 224 (26) |
| Drugs for migraine | 20 (5) | 5 (2) | 25 (4) | 10 (2) | 0 (0) | 10 (1) |
| Antiepileptics | 55 (13) | 23 (8) | 78 (11) | 57 (14) | 52 (11) | 109 (13) |
| Tricyclic antidepressants | 57 (14) | 14 (5) | 71 (10) | 20 (5) | 15 (3) | 35 (4) |
| SNRI | 43 (10) | 16 (5) | 59 (8) | 24 (6) | 18 (4) | 42 (5) |
| Pain Related to the Urinary System | ||||||
| COX(1+2) inhibitors | 18 (55) | 54 (61) | 72 (59) | 27 (44) | 61 (33) | 88 (36) |
| COX2 inhibitors | 5 (15) | 2 (2) | 7 (6) | 5 (8) | 3 (2) | 8 (3) |
| Paracetamol | 31 (94) | 49 (55) | 80 (66) | 54 (87) | 129 (70) | 183 (74) |
| Strong opioids | 16 (48) | 21 (24) | 37 (30) | 21 (34) | 53 (29) | 74 (30) |
| Weak opioids | 17 (52) | 37 (42) | 54 (44) | 22 (35) | 42 (23) | 64 (26) |
| Drugs for migraine | 0 (0) | 1 (1) | 1 (1) | 1 (2) | 1 (1) | 2 (1) |
| Antiepileptics | 10 (30) | 11 (12) | 21 (17) | 4 (6) | 20 (11) | 24 (10) |
| Tricyclic antidepressants | 5 (15) | 9 (10) | 14 (11) | 5 (8) | 8 (4) | 13 (5) |
| SNRI | 3 (9) | 6 (7) | 9 (7) | 2 (3) | 9 (5) | 11 (4) |
| Type of Pain | No Epilepsy | No Depression | |
|---|---|---|---|
| Antiepileptics | Tricyclic Antidepressants | SNRI | |
| Headaches | 1.16 (0.56–2.40) | 0.52 (0.22–1.22) | 0.40 (0.09–1.76) |
| Musculoskeletal pain | 0.90 (0.68–1.20) | 0.44 (0.30–0.66) | 0.80 (0.50–1.26) |
| Pain related to the circulatory and respiratory systems | 0.92 (0.62–1.38) | 0.44 (0.25–0.77) | 0.99 (0.46–2.11) |
| Visceral pain | 0.81 (0.58–1.13) | 0.34 (0.22–0.53) | 0.63 (0.37–1.05) |
| Pain related to the urinary system | 0.37 (0.18–0.75) | 0.47 (0.21–1.04) | 0.70 (0.20–2.43) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Axmon, A.; Ahlström, G.; Westergren, H. Pain and Pain Medication among Older People with Intellectual Disabilities in Comparison with the General Population. Healthcare 2018, 6, 67. https://doi.org/10.3390/healthcare6020067
Axmon A, Ahlström G, Westergren H. Pain and Pain Medication among Older People with Intellectual Disabilities in Comparison with the General Population. Healthcare. 2018; 6(2):67. https://doi.org/10.3390/healthcare6020067
Chicago/Turabian StyleAxmon, Anna, Gerd Ahlström, and Hans Westergren. 2018. "Pain and Pain Medication among Older People with Intellectual Disabilities in Comparison with the General Population" Healthcare 6, no. 2: 67. https://doi.org/10.3390/healthcare6020067
APA StyleAxmon, A., Ahlström, G., & Westergren, H. (2018). Pain and Pain Medication among Older People with Intellectual Disabilities in Comparison with the General Population. Healthcare, 6(2), 67. https://doi.org/10.3390/healthcare6020067