Using Deep Dive Methodology to Investigate an Increased Incidence of Hospital-Acquired Avoidable Category 2 and 3 Pressure Ulcers


 and
and
Abstract
:1. Introduction
1.1. Local Context
1.2. External Factors
1.3. Aims
- Undertake a ‘Deep Dive’ into the case notes of patients who developed a hospital-acquired avoidable pressure ulcer (category 2 and 3) during the period, October 2017 to March 2018.
- Explore whether there were any specific factors or variables that may account for or explain the increase in patients developing grade 2 and 3 pressure ulcers during this period.
- Make recommendations both in the short and long term to prevent this situation from occurring in the future.
2. Materials and Methods
2.1. Participants
2.2. Procedure
- an investigation of something gone awry, not understood or where independent assurance is lacking;
- something more than usual performance management, audit, assurance;
- a limited exercise producing understanding, conclusions and actions.
2.2.1. Stage 1: Assurances
2.2.2. Stage 2: Identification and Selection of Cases
2.2.3. Stage 3: Individual Case Review
2.2.4. Ethical Considerations
2.2.5. Data Analysis
3. Results
3.1. Admission and Patient Journey
3.2. Time in A&E
3.3. Development of a Pressure Ulcer
Types of Injury
4. Discussion
5. Conclusions/Recommendations
5.1. Improvements to Date
- Redesign of A&E documentation to focus on preventative measures where operational pressures delay opportunity to perform a full risk assessment/body map, etc. The admission documentation now has an ‘Immediate Interventions’ section, guiding staff to work on the assumption of risk for all patients nursed on trolleys.
- Review of emergency portal access to heel offloading devices, beds and dynamic mattresses to ensure that they have adequate supply to meet increases in demand.
- AMU are currently undertaking a trial involving Acute Medical Rapid Assessment (AMRA) involving staff from AMU working with colleagues in A&E with the view to speed up the assessment process and reduce the number of hours in A&E, moves and admissions.
- Tissue Viability training and support provided on key themes and as part of the yearly statutory and mandatory training within the emergency portals.
- Dissemination of the key themes emerging from the RCA’s of avoidable pressure ulcers during this period—Trust-wide via the ‘Wound Wednesdays’ and TV ‘Tips on Tuesday’ Staff education sessions.
- Established a Pressure Ulcer Strategy Group that is multidisciplinary comprising representation from ambulance service, portering, nursing assistants, tissues viability, quality, medicine, AMU, allied health professionals, all in-reach services, Commissioners, NHS England and R&D. The purpose of the group will be to review and develop a targeted pressure ulcer prevention strategy for our admission portals.
5.2. Short Term
- Review A&E nursing assessment for the risk of pressure ulcer development and implementation of a relevant and targeted action plan (skin bundle/comfort rounds)/access to heel offloading devices/access to beds and dynamic mattresses in the department (review current SOP).
- Reinforce the importance of early intervention and the utilization of all pressure-relieving equipment available, especially with A&E and other emergency portals so that the chain of event identified in this evaluation can be broken.
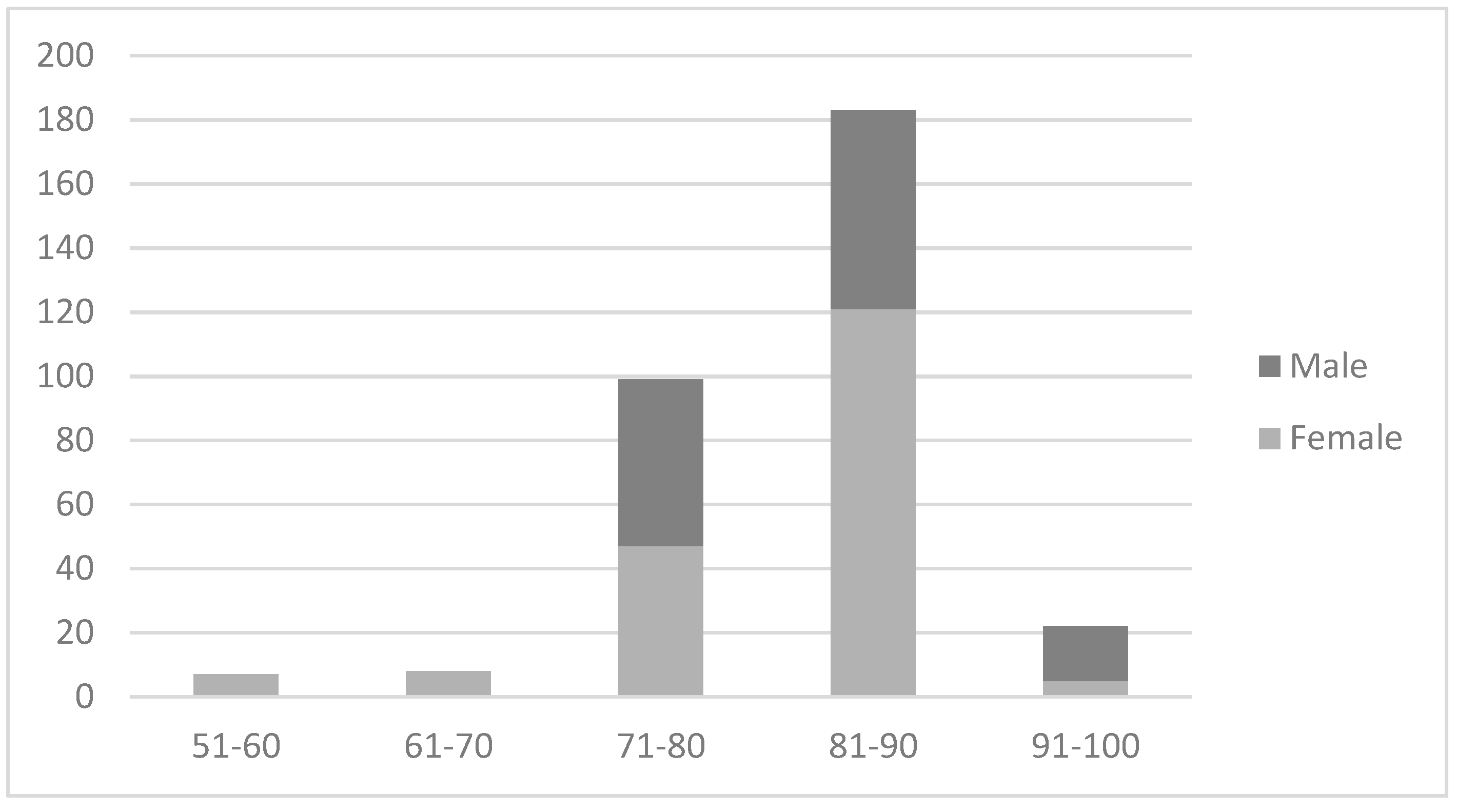
- Raise awareness of the specific factors that appear to predispose particular groups of individuals, particularly those who are frail, over the age of 80–90 years, who spend an extended length of time in A&E and experience multiple moves.
- Review the process in A&E for supporting older people, especially those diagnosed with ‘frailty’, ensuring preventative action taken, shortest possible stay and quick transfer from A&E with minimal moves (maximum 1) to their final destination of care.
5.3. Long Term
- Conduct a more formal piece of research, using a larger representative dataset, incorporating a wider number of variables such as staffing, so that comparisons between those who developed a pressure sore during this period and those who did not can be undertaken to inform a predictive model.
- Develop a research protocol and seek the necessary Health Research Authority approval to access the relevant data sets within UHNM and the necessary authorization and permissions to conduct the investigation within the organization.
- Utilize more advanced parametric statistical tests (such as regression analysis) to develop a predictive model of those factors that may contribute to the development of a pressure ulcer during times of escalation and reduced capacity within the organization.
Author Contributions
Funding
Conflicts of Interest
References
- Lannering, C.; Bravell, M.E.; Johansson, L. Prevention of falls, malnutrition and pressure ulcers among older persons —Nursing staff’s experiences of a structured preventive care process. Health Soc. Care Community 2017, 25, 1011–1020. [Google Scholar] [PubMed]
- Downie, F.; Sandoz, H.; Gilroy, P.; Royall, D.; Davies, S.; Brett, D.; Bates, J. Avoidable pressure ulcer rates in six acute UK Trusts. Wounds UK 2014, 10, 48–53. [Google Scholar]
- Catherine, A.; Sharp, C.A.; White, R.J. Pressure ulcer risk assessment: Do we need a golden hour? J. Wound Care 2015, 24, 237. [Google Scholar]
- Stop Pressure Ulcers. Available online: www.epaup.org (accessed on 8 August 2018).
- Emergency Hospital Admissions in England: Which May Be Avoidable and How? Available online: https://www.health.org.uk/sites/health/files/Briefing_Emergency%2520admissions_web_final.pdf (accessed on 21 August 2018).
- Sherwin, J. Contemporary topics in health care: Root cause analysis. PT Motion 2011, 3, 28–31. [Google Scholar]
- NHS Improvement Pressure Ulcers: Revised Definition and Measurement. Available online: https://improvement.nhs.uk/documents/2932/NSTPP_summary__recommendations_20June2018.pdf (accessed on 14 August 2018).
- Defining Avoidable and Uvoidable Pressure Ulcers. Available online: https://pdfs.semanticscholar.org/94cd/53cecfd99c88a2d0219050a8d05187bae970.pdf (accessed on 13 December 2018).
- What is a Deep Dive? Available online: https://www.good-governance.org.uk/wp-content/uploads/2017/04/What-is-a-deep-dive.pdf (accessed on 10 August 2018).
- Serious Incident Framework, Supporting Learning to Prevent Recurrence. Available online: https://www.england.nhs.uk/wp-content/uploads/2015/04/serious-incidnt-framwrk-upd.pdf (accessed on 10 August 2018).
- Coleman, S.; Gorecki, C.; Nelson, A.E.; Cross, S.J.; Defloor, T.; Halfens, R.; Amanda Farrin, A.; Brown, J.; Schoonhoven, L.; Nixon, J. Patient risk factors for pressure ulcer development: Systematic review. Int. J. Nurs. Stud. 2013, 50, 974–1003. [Google Scholar] [CrossRef] [PubMed]
- Pressure Ulcer Prevention Manual. Available online: http://www.judy-waterlow.co.uk/downloads/WATerlow%20cover%20no%20logos.pdf (accessed on 2 April 2019).
- Frailty in Older People. Available online: https://www.rcn.org.uk/clinical-topics/older-people/frailty (accessed on 10 August 2018).
- Guidance on the Notification of Pressure Ulcers. Available online: http://nhs.stopthepressure.co.uk/path/docs/Reporting%20guidance.pdf (accessed on 13 December 2018).
- National Pressure Ulcer Advisory Panel; European Pressure Ulcer Advisory Panel; Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline; Cambridge Media: Osborne Park, Australia, 2014. [Google Scholar]
- Farid, K.J.; Winkelman, C.; Rizkala, A.; Jones, K. Using temperature of pressure-related intact discolored areas of skin to detect deep tissue injury: An observational, retrospective, correlational study. Ostomy Wound Manage 2012, 58, 20–31. [Google Scholar] [PubMed]
- Jaul, E. Assessment and management of pressure ulcers in the elderly current strategies. Drugs Aging 2010, 27, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Brown-O’Hara, P. Geriatric syndromes and their implications for nursing. Nursing 2014, 25, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, J.; Cameron, J. Assessment of skin integrity in the elderly 1. Br. J. Community Nurs. 2008, 13, 26–32. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Definition of a Pressure Ulcer NHS Improvement (2018) [7] | “A pressure ulcer is localised damage to the skin and/or underlying tissue, usually over a boney prominence (or related to a medical or other device), resulting from sustained pressure (including pressure associated with shear). The damage can be present as intact skin or as an open ulcer and may be painful”. |
| Avoidable Pressure Ulcer (Wound, Ostomy and Continence Nurses Society, 2009) * [8] | “Avoidable” means that the person receiving care developed a pressure ulcer and the provider of care did not do one of the following: evaluate the person’s clinical condition and pressure ulcer risk factors; plan and implement interventions that are consistent with the persons needs and goals, and recognised standards of practice; monitor and evaluate the impact of the interventions; or revise the interventions as appropriate.” UHNM policy is that any category 3 or 4 pressure ulcer that developed within 72 h of admission would be considered a deep tissue injury present on admission. |
| Demographics/Variables | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| Count | 18 | 19 | 37 | |||
| A&E attendance | 15 | 17 | 32 | |||
| Admission body map completed | 10 | 12 | 22 | |||
| A&E trolley | 11 | 15 | 26 | |||
| - | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev |
| Age (in years) | 83.5 | 5.38 | 82.36 | 9.52 | 82.95 | 7.703 |
| Number of moves | 2.12 | 0.93 | 2.69 | 1 | 2.4 | 1 |
| Hours in A&E | 9.05 | 7.83 | 11.83 | 7.46 | 10.4 | 7.67 |
| Total hours in emergency portal | 32.3 | 63.9 | 43.2 | 56.6 | 37.9 | 59.7 |
| Timespan to Pressure Ulcer development from admission (days) | 17.1 | 21.24 | 19.68 | 18.68 | 18.43 | 19.63 |
| Time Between A&E Admission and Body Map/Skin Bundle | Number of Patients |
|---|---|
| Within four hours | 8 |
| Patients with heels offloaded | 1 |
| More than four hours | 9 |
| No skin bundle completed | 8 |
| No scanned Emergency Department (ED)notes | 9 |
| TOTAL | 35 |
| Gender | Category 2 | Category 3 | Total | |||
|---|---|---|---|---|---|---|
| Male | 9 | (47.4%) | 9 | (50%) | 18 | (48.6%) |
| Female | 10 | (52.6) | 9 | (50%) | 19 | (51.3%) |
| Total | 19 | (100%) | 18 | (100%) | 37 | (100%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horton-Jones, M.; Marsh, E.; Fumarola, S.; Wright-White, H.; McSherry, W.; Rowson, T. Using Deep Dive Methodology to Investigate an Increased Incidence of Hospital-Acquired Avoidable Category 2 and 3 Pressure Ulcers. Healthcare 2019, 7, 59. https://doi.org/10.3390/healthcare7020059
Horton-Jones M, Marsh E, Fumarola S, Wright-White H, McSherry W, Rowson T. Using Deep Dive Methodology to Investigate an Increased Incidence of Hospital-Acquired Avoidable Category 2 and 3 Pressure Ulcers. Healthcare. 2019; 7(2):59. https://doi.org/10.3390/healthcare7020059
Chicago/Turabian StyleHorton-Jones, Martyne, Emma Marsh, Sian Fumarola, Helen Wright-White, Wilfred McSherry, and Trish Rowson. 2019. "Using Deep Dive Methodology to Investigate an Increased Incidence of Hospital-Acquired Avoidable Category 2 and 3 Pressure Ulcers" Healthcare 7, no. 2: 59. https://doi.org/10.3390/healthcare7020059
APA StyleHorton-Jones, M., Marsh, E., Fumarola, S., Wright-White, H., McSherry, W., & Rowson, T. (2019). Using Deep Dive Methodology to Investigate an Increased Incidence of Hospital-Acquired Avoidable Category 2 and 3 Pressure Ulcers. Healthcare, 7(2), 59. https://doi.org/10.3390/healthcare7020059