Treatment of Patients with Low Back Pain: A Comparison of Physical Therapy and Chiropractic Manipulation


Abstract
1. Introduction
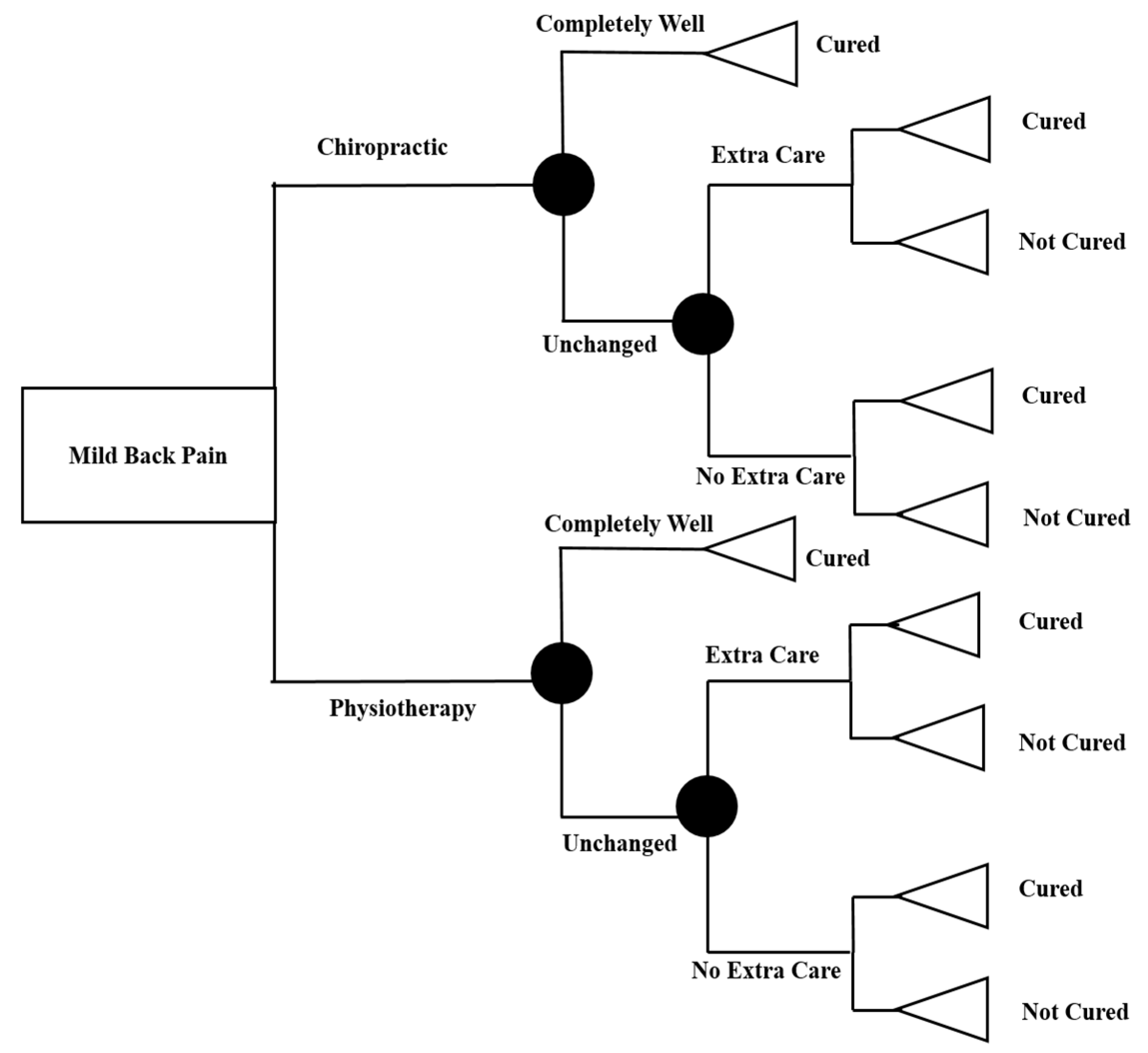
2. Materials and Methods
2.1. Sample of Study
2.2. Costs of Treatments
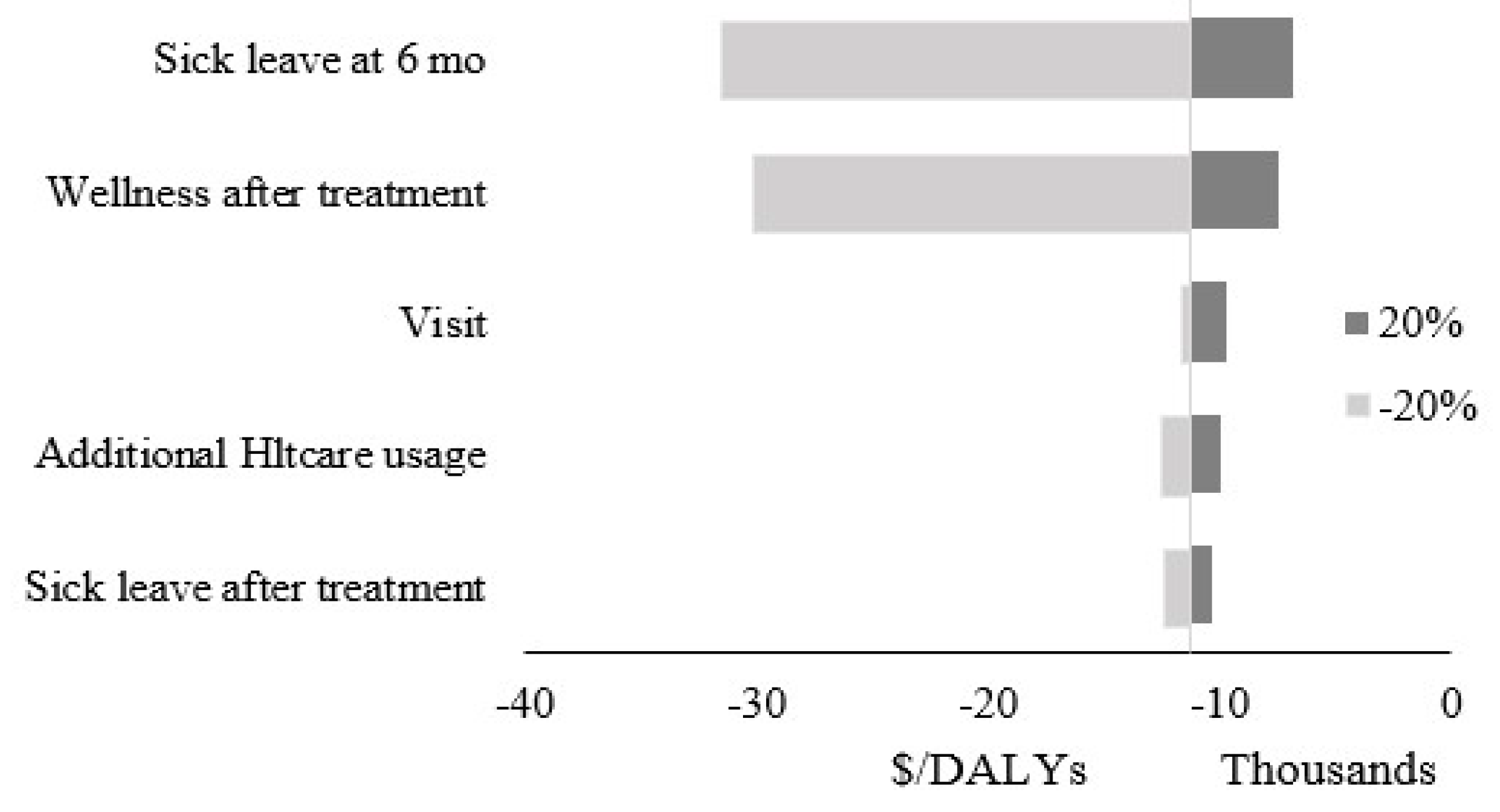
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P.; Hartvigsen, J.; Cherkin, D.; Foster, N.E.; et al. Low back pain: A call for action. Lancet 2018, 391, 2384–2388. [Google Scholar] [CrossRef]
- Assendelft, W.J.; Morton, S.C.; Emily, I.Y.; Suttorp, M.J.; Shekelle, P.G. Spinal manipulative therapy for low-back pain. Cochrane Database Syst. Rev. 2004. [Google Scholar] [CrossRef]
- Skargren, E.I.; Öberg, B.E.; Carlsson, P.G.; Gade, M. Cost and effectiveness analysis of chiropractic and physiotherapy treatment for low back and neck pain: Six-month follow-up. Spine 1997, 22, 2167–2177. [Google Scholar] [CrossRef] [PubMed]
- Malmivaara, A.; Häkkinen, U.; Aro, T.; Heinrichs, M.L.; Koskenniemi, L.; Kuosma, E.; Lappi, S.; Paloheimo, R.; Servo, C.; Vaaranen, V.; et al. The treatment of acute low back pain—bed rest, exercises, or ordinary activity? N. Engl. J. Med. 1995, 332, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Gore, M.; Sadosky, A.; Stacey, B.R.; Tai, K.; Leslie, D. The burden of chronic low back pain: Clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine 2012, 37, E668–E677. [Google Scholar] [CrossRef]
- Rogerson, M.D.; Gatchel, R.J.; Bierner, S.M. A cost utility analysis of interdisciplinary early intervention versus treatment as usual for high-risk acute low back pain patients. Pain Pract. 2010, 10, 382–395. [Google Scholar] [CrossRef]
- Balagué, F.; Mannion, A.F.; Pellisé, F.; Cedraschi, C. Non-specific low back pain. Lancet 2012, 379, 482–491. [Google Scholar] [CrossRef]
- Carey, T.S.; Garrett, J.; Jackman, A.; McLaughlin, C.; Fryer, J.; Smucker, D.R.; North Carolina Back Pain Project. The outcomes and costs of care for acute low back pain among patients seen by primary care practitioners, chiropractors, and orthopedic surgeons. N. Engl. J. Med. 1995, 333, 913–917. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Polatin, P.B.; Noe, C.; Gardea, M.; Pulliam, C.; Thompson, J. Treatment-and cost-effectiveness of early intervention for acute low-back pain patients: A one-year prospective study. J. Occup. Rehabil. 2003, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Henchoz, Y.; Pinget, C.; Wasserfallen, J.B.; Paillex, R.; de Goumoëns, P.; Norberg, M.; So, A.K.L. Cost-utility analysis of a three-month exercise programme vs usual care following multidisciplinary rehabilitation for chronic low back pain. J. Rehabil. Med. 2010, 42, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Oakley, P.A.; Cuttler, J.M.; Harrison, D.E. X-ray imaging is essential for contemporary chiropractic and manual therapy spinal rehabilitation: Radiography increases benefits and reduces risks. Dose-Response 2018, 16, 1559325818781437. [Google Scholar] [CrossRef] [PubMed]
- Lemmers, G.P.; Van Lankveld, W.; Westert, G.P.; van der Wees, P.J.; Staal, J.B. Imaging versus no imaging for low back pain: A systematic review, measuring costs, healthcare utilization and absence from work. Eur. Spine J. 2019, 28, 937–950. [Google Scholar] [CrossRef] [PubMed]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W.; et al. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- Flor, H.; Fydrich, T.; Turk, D.C. Efficacy of multidisciplinary pain treatment centers: A meta-analytic review. Pain 1992, 49, 221–230. [Google Scholar] [CrossRef]
- Fritz, J.M.; Kim, M.; Magel, J.S.; Asche, C.V. Cost-effectiveness of primary care management with or without early physical therapy for acute low back pain: Economic evaluation of a randomized clinical trial. Spine 2017, 42, 285–290. [Google Scholar] [CrossRef]
- Fritz, J.M.; Cleland, J.A.; Speckman, M.; Brennan, G.P.; Hunter, S.J. Physical therapy for acute low back pain: Associations with subsequent healthcare costs. Spine 2008, 33, 1800–1805. [Google Scholar] [CrossRef]
- Globe, G.; Farabaugh, R.J.; Hawk, C.; Morris, C.E.; Baker, G.; Whalen, W.M.; Walters, S.; Kaeser, M.; Dehen, M.; Augat, T. Clinical practice guideline: Chiropractic care for low back pain. J. Manip. Physiol. Ther. 2016, 39, 1–22. [Google Scholar] [CrossRef]
- Goertz, C.M.; Long, C.R.; Hondras, M.A.; Petri, R.; Delgado, R.; Lawrence, D.J.; Owens, E.F.; Meeker, W.C. Adding chiropractic manipulative therapy to standard medical care for patients with acute low back pain: Results of a pragmatic randomized comparative effectiveness study. Spine 2013, 38, 627–634. [Google Scholar] [CrossRef]
- Hurwitz, E.L.; Morgenstern, H.; Harber, P.; Kominski, G.F.; Belin, T.R.; Yu, F.; Adams, A.H. A randomized trial of medical care with and without physical therapy and chiropractic care with and without physical modalities for patients with low back pain: 6-month follow-up outcomes from the UCLA low back pain study. Spine 2002, 27, 2193–2204. [Google Scholar] [CrossRef]
- Chou, R.; Qaseem, A.; Snow, V.; Casey, D.; Cross, J.T.; Shekelle, P.; Owens, D.K. Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann. Intern. Med. 2007, 147, 478–491. [Google Scholar] [CrossRef]
- Cherkin, D.C.; Deyo, R.A.; Battié, M.; Street, J.; Barlow, W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N. Engl. J. Med. 1998, 339, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Meade, T.W.; Dyer, S.; Browne, W.; Townsend, J.; Frank, A.O. Low back pain of mechanical origin: Randomised comparison of chiropractic and hospital outpatient treatment. BMJ 1990, 300, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Berenguera, A.; Pujol-Ribera, E.; Rodriguez-Blanco, T.; Violan, C.; Casajuana, M.; de Kort, N.; Trapero-Bertran, M. Study protocol of cost-effectiveness and cost-utility of a biopsychosocial multidisciplinary intervention in the evolution of non-specific sub-acute low back pain in the working population: Cluster randomised trial. BMC Musculoskelet. Disord. 2011, 12, 194. [Google Scholar] [CrossRef] [PubMed]
- Khodakarami, N.; Dirani, K.; Rezaei, F. Employee engagement: Finding a generally accepted measurement scale. Ind. Commer. Train. 2018, 50, 305–311. [Google Scholar] [CrossRef]
- Khodakarami, N.; Dirani, K. Drivers of employee engagement: Differences by work area and gender. Ind. Commer. Train. 2020, 52. [Google Scholar] [CrossRef]
- Liang, M.; Komaroff, A.L. Roentgenograms in primary care patients with acute low back pain. Arch. Intern. Med. 1982, 142 Pt 6, 1108–1112. [Google Scholar] [CrossRef]
- Whedon, J.M.; Song, Y.; Davis, M.A. Trends in the use and cost of chiropractic spinal manipulation under Medicare Part, B. Spine J. 2013, 13, 1449–1454. [Google Scholar] [CrossRef]
- Synnott, A.; O’Keeffe, M.; Bunzli, S.; Dankaerts, W.; O’Sullivan, P.; O’Sullivan, K. Physiotherapists may stigmatise or feel unprepared to treat people with low back pain and psychosocial factors that influence recovery: A systematic review. J. Physiother. 2015, 61, 68–76. [Google Scholar] [CrossRef]
- Rubinstein, S.M. Adverse events following chiropractic care for subjects with neck or low-back pain: Do the benefits outweigh the risks? J. Manip. Physiol. Ther. 2008, 31, 461–464. [Google Scholar] [CrossRef]
- Pollycove, M. Radiobiological basis of low-dose irradiation in prevention and therapy of cancer. Dose-Response 2007, 5, 26–38. [Google Scholar] [CrossRef]
- Hays, R.D.; Spritzer, K.L.; Sherbourne, C.D.; Ryan, G.W.; Coulter, I.D. Group and individual-level change on health-related quality of life in chiropractic patients with chronic low back or neck pain. Spine 2019, 44, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Khodakarami, N. PIT8 Cost-Effectiveness Analysis of Physical Therapy Against Chiropractic for Patients with Acute Low Back Pain in the US. Value Health 2019, 22, S212–S213. [Google Scholar] [CrossRef]
- Khodakarami, N. The Impact of Sex Education on Sexual Activity, Pregnancy, and Abortion. arXiv 2019, arXiv:1903.08307. [Google Scholar]
- Parkinson, L.; Sibbritt, D.; Bolton, P.; van Rotterdam, J.; Villadsen, I. Well-being outcomes of chiropractic intervention for lower back pain: A systematic review. Clin. Rheumatol. 2013, 32, 167–180. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Treatment Strategies 1 | Ch | PT |
|---|---|---|
| Subjects | 55% | 45% |
| Mean age (SD) | 41.4 (11.6) | 40.5 (11.9) |
| Percent Women | 60% | 65% |
| Smokers | 36% | 31% |
| History of LBP | 72% | 70% |
| Previously treated for LBP | 24% | 35% |
| Duration of sick leave before treatment | ||
| ≤1wk | 61% | 58% |
| 1–4 wk | 37% | 33% |
| Current episode of LBP | ||
| ≤6 wk | 55% | 48% |
| Using pain medication | 20% | 26% |
| Sick leave | ||
| After treatment | 40% | 43% |
| At 6 mo | 48% | 46% |
| No of treatment sessions of Ch or Pt0-6 months | 4.9 | 6.4 |
| Treatment Strategies 1 | 1995 $ | 2018 $ | ||
|---|---|---|---|---|
| Ch 1 | PT 1 | Ch | PT | |
| Treatment | 28.01 | 49.99 | 56.94 | 101.62 |
| Imaging | 67.26 | - | 136.73 | - |
| Visit | 114 | 134 | 231.74 | 272.39 |
| Drug (Copay) | 10 | 10 | 20.33 | 20.33 |
| Ch1 | PT1 | Diff | |
|---|---|---|---|
| Costs | $410.89 | $459.45 | $48.56 |
| DALY | 0.01562 | 0.01132 | (0.0043) |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khodakarami, N. Treatment of Patients with Low Back Pain: A Comparison of Physical Therapy and Chiropractic Manipulation. Healthcare 2020, 8, 44. https://doi.org/10.3390/healthcare8010044
Khodakarami N. Treatment of Patients with Low Back Pain: A Comparison of Physical Therapy and Chiropractic Manipulation. Healthcare. 2020; 8(1):44. https://doi.org/10.3390/healthcare8010044
Chicago/Turabian StyleKhodakarami, Nima. 2020. "Treatment of Patients with Low Back Pain: A Comparison of Physical Therapy and Chiropractic Manipulation" Healthcare 8, no. 1: 44. https://doi.org/10.3390/healthcare8010044
APA StyleKhodakarami, N. (2020). Treatment of Patients with Low Back Pain: A Comparison of Physical Therapy and Chiropractic Manipulation. Healthcare, 8(1), 44. https://doi.org/10.3390/healthcare8010044