Mechanisms of Negative Fetal Outcome in Frontal Vehicle Collisions Involving Unbelted Pregnant Drivers

Abstract
:1. Introduction
2. Materials and Methods
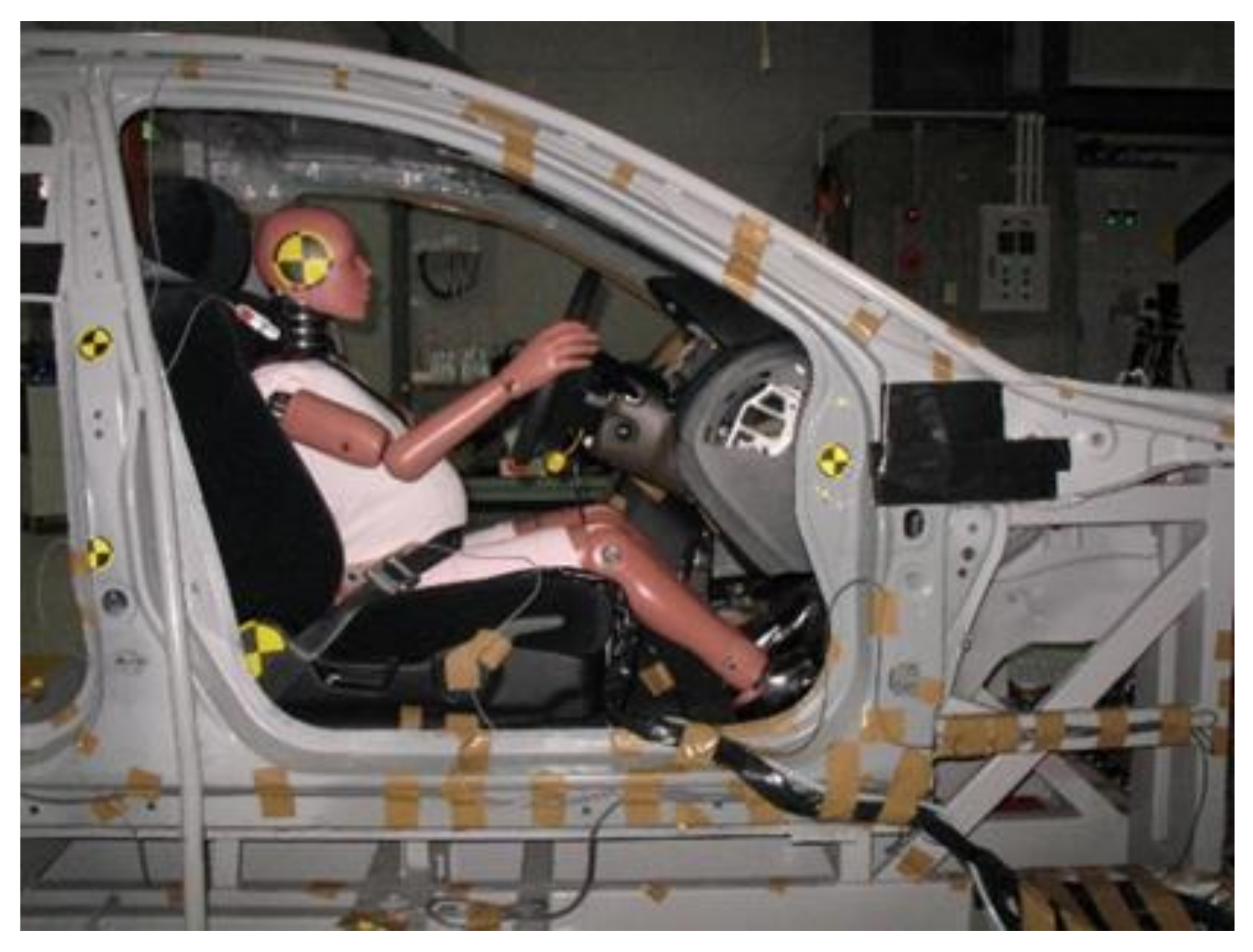
2.1. Dummy
2.2. Seating Position of the Dummy
2.3. Test Setup
2.4. Measurements
3. Results
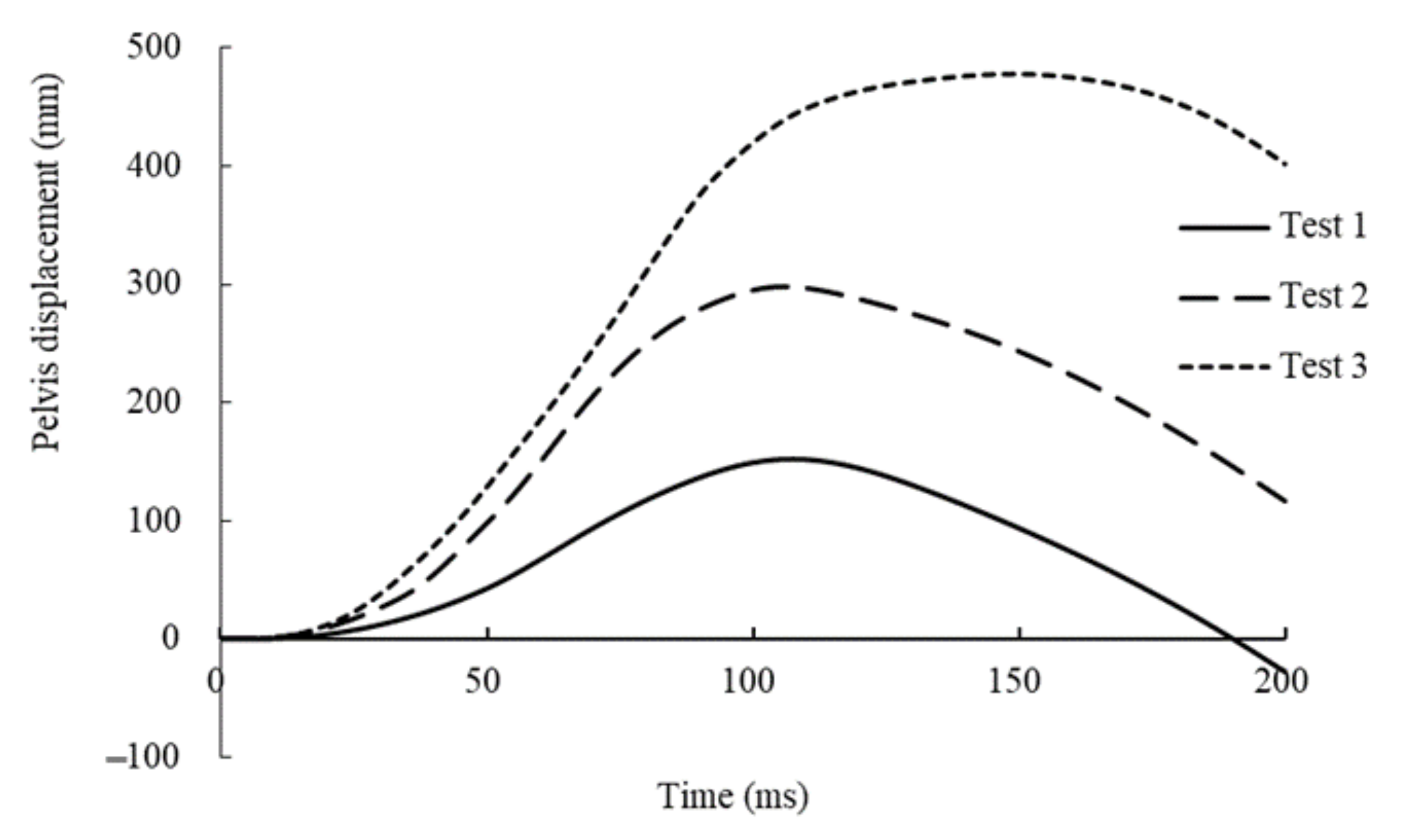
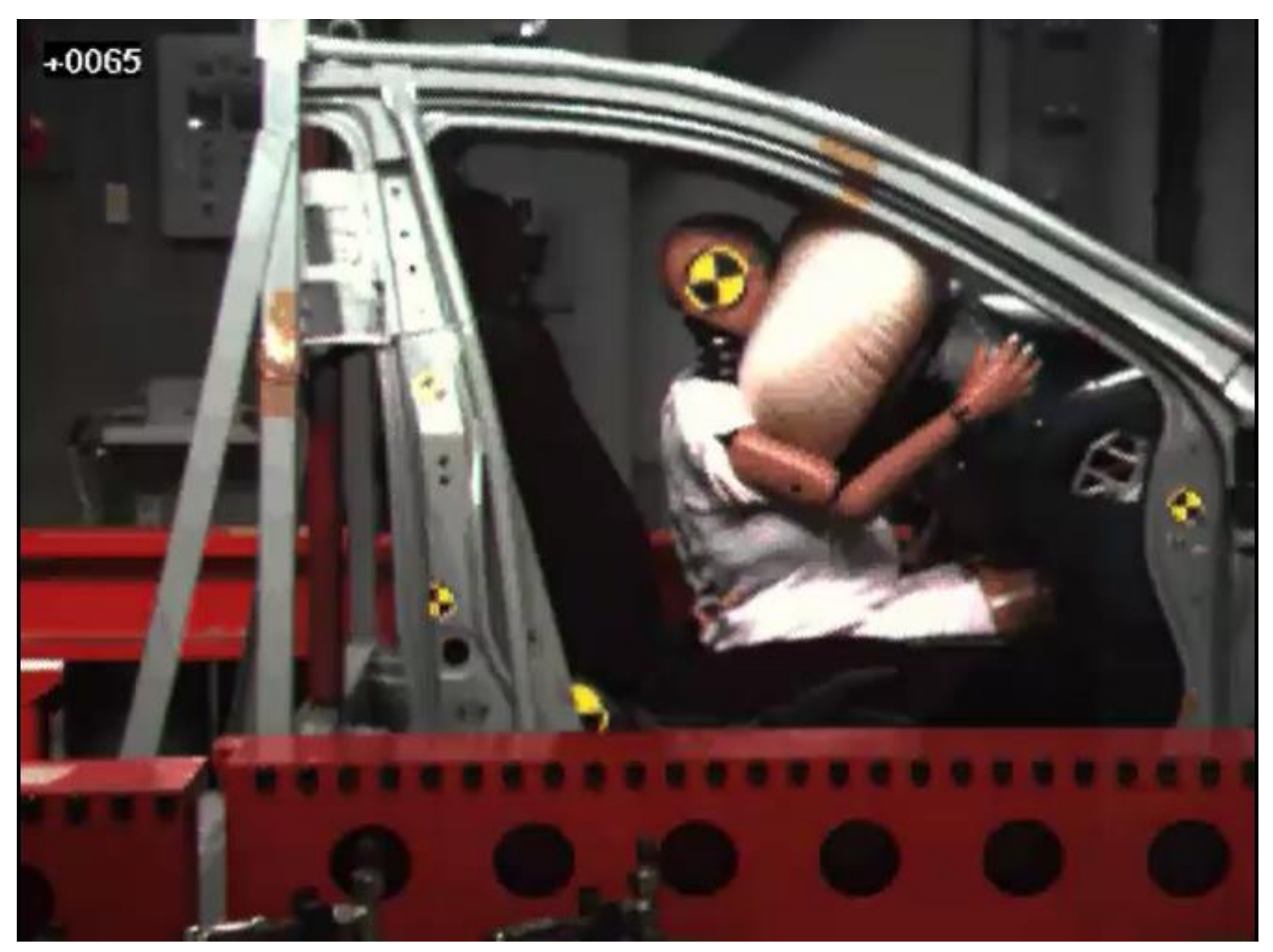
3.1. Kinematics of the Dummy
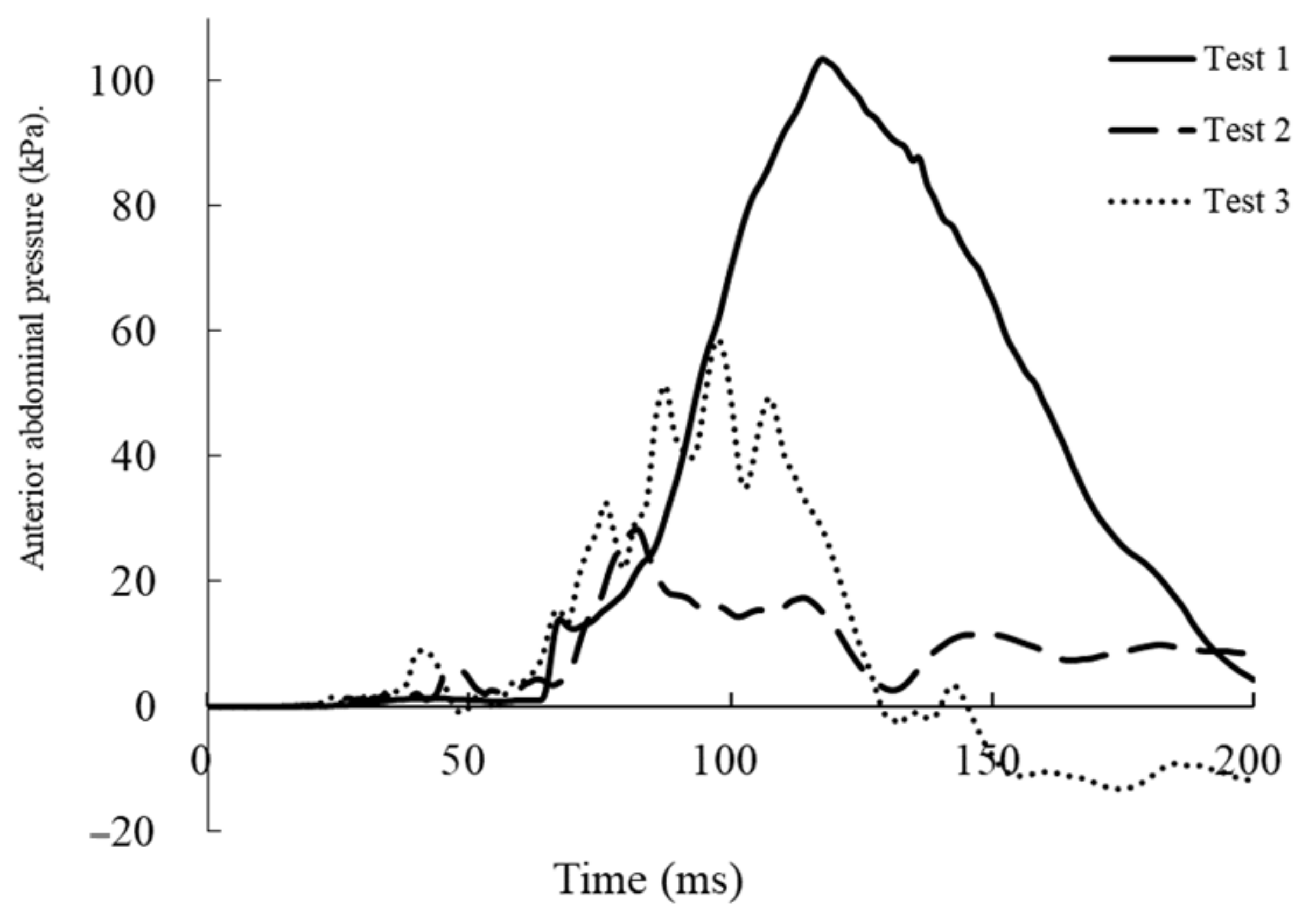
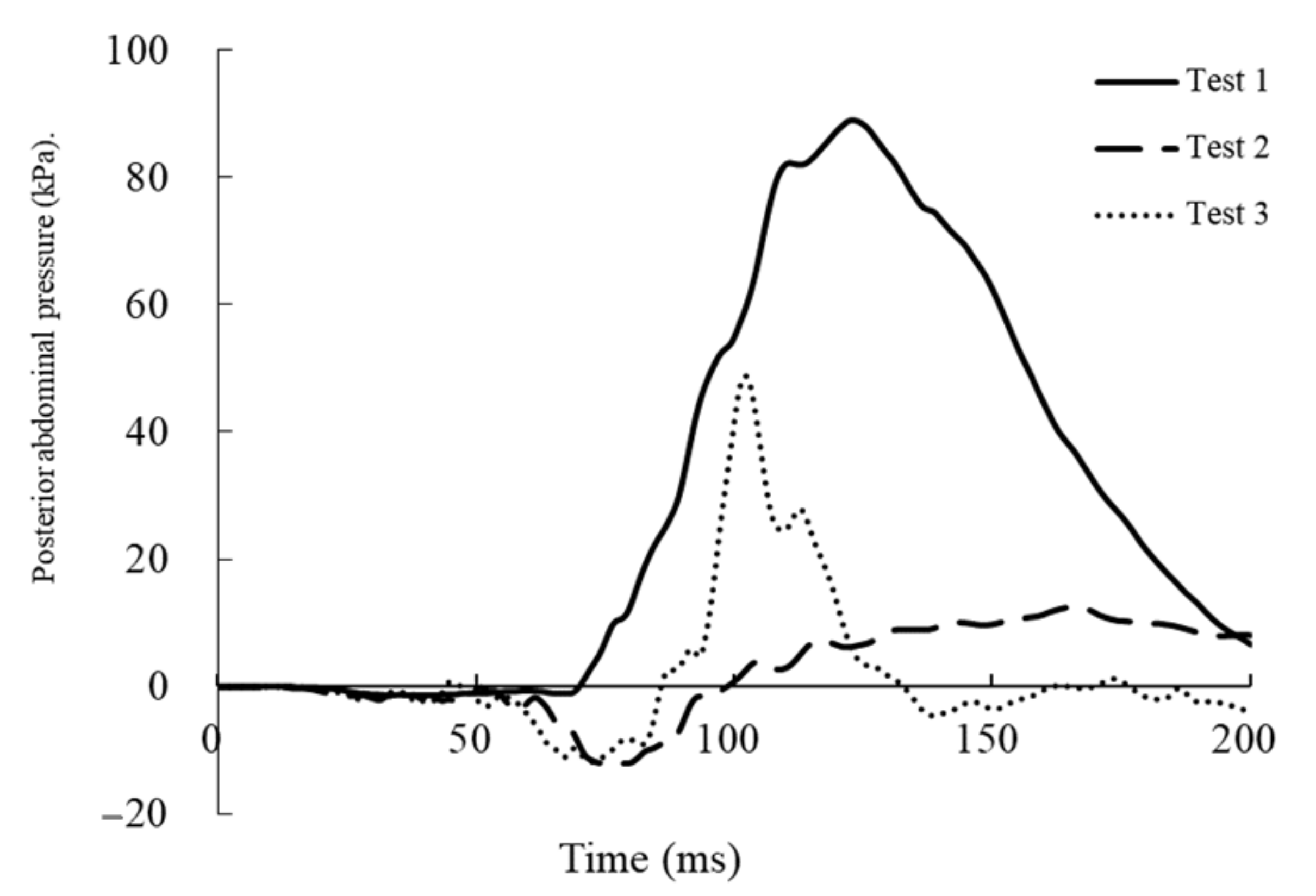
3.2. Measured Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Road Safety. 2018. Available online: https://www.who.int/publications/i/item/global-status-report-on-road-safety-2018 (accessed on 9 October 2020).
- Klinich, K.D.; Schneider, L.W.; Moore, J.L.; Pearlman, M.D. Investigations of crash involving pregnant occupants. In Annual Proceedings/Association for the Advancement of Automotive Medicine; Final Report No. UMTRI 99-29; University of Michigan, Transportation Research Institute: Arbor, MI, USA, 2000. [Google Scholar]
- Kvarnstrand, L.; Milsom, I.; Lekander, T.; Druid, H.; Jacobsson, B.O. Maternal fatalities, fetal and neonatal deaths related to motor vehicle crashes during pregnancy: A national population-based study. Acta Obstet. Gynecol. Scand. 2008, 87, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M. Pregnant women should wear seat belts. BMJ 1995, 311, 1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klinich, K.D.; Flannagan, C.A.; Rupp, J.D.; Sochor, M.; Schneider, L.W.; Pearlman, M.D. Fetal outcome in motor-vehicle crashes: Effects of crash characteristics and maternal restraint. Am. J. Obstet. Gynecol. 2008, 198, 450.e1–450.e9. [Google Scholar] [CrossRef] [PubMed]
- ACOG Educational Bulletin. Obstetric aspects of trauma management. Number 251, September 1998 (replaces Number 151, January 1991, and Number 161, November 1991). American College of Obstetricians and Gynecologists. Int. J. Gynaecol. Obstet. 1991, 64, 87–94. [Google Scholar]
- Motozawa, Y.; Hitosugi, M.; Abe, T.; Tokudome, S. Effects of seat belts worn by pregnant drivers during low-impact collisions. Am. J. Obstet. Gynecol. 2010, 203, 62.e1–62.e8. [Google Scholar] [CrossRef] [PubMed]
- Motozawa, Y.; Hitosugi, M.; Abe, T.; Tokudome, S. Analysis of the kinematics of pregnant drivers during low-speed frontal vehicle collisions. Int. J. Crashworthiness 2010, 15, 235–239. [Google Scholar] [CrossRef]
- Acar, B.S.; Edwards, A.M.; Aldah, M. Correct use of three-point seatbelt by pregnant occupants. Safety 2018, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Daud, S.; Zahid, A.Z.M.; Abdullah, B.; Mohamad, M. Knowledge and practice of seat belt use among pregnant women. J. South Asian Feder. Obs. Gynae 2018, 10, 297–301. [Google Scholar] [CrossRef]
- Ichikawa, M.; Nakahara, S.; Okubo, T.; Wakai, S. Car seatbelt use during pregnancy in Japan: Determinants and policy implications. Inj. Prev. 2003, 9, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Jamjute, P.; Eedarapalli, P.; Jain, S. Awareness of correct use of a seatbelt among pregnant women and health professionals: A multicentric survey. J. Obstet. Gynaecol. 2005, 25, 550–553. [Google Scholar] [CrossRef]
- Zhao, Y.; Ratingen, M.; Yao, C.; Brill, G.; Goldner, S.; Huang, R. Enhancement and evaluation of a small female Hybrid III pregnant dummy. In Proceedings of the International IRCOBI Conference, Madrid, Spain, 20–22 September 2006. [Google Scholar]
- Klinich, K.D.; Schneider, L.W.; Rupp, J.; Eby, B.; Pearlman, M. Challenges in frontal crash protection of pregnant drivers based on anthropometric considerations. SAE Trans. 1999, 108, 1136–1158. [Google Scholar]
- Rupp, J.D.; Klinich, K.D.; Moss, S.; Zhou, J.; Pearlman, M.D.; Schneider, L.W. Development and testing of a prototype pregnant abdomen for the small-female Hybrid III ATD. Stapp Car Crash J. 2001, 45, 61–78. [Google Scholar] [PubMed]
- Motozawa, Y.; Hitosugi, M.; Tokudome, S. Analysis of seating position and anthropometric parameters of pregnant Japanese drivers. Traffic Inj. Prev. 2008, 9, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Hitosugi, M.; Kido, M.; Maegawa, M.; Nagai, T.; Tokudome, S.; Motozawa, Y. The benefits of seatbelt use in pregnant women drivers. Forensic Sci. Int. 2007, 169, 274–275. [Google Scholar] [CrossRef] [PubMed]
- Eppinger, R.; Sun, E.; Bandak, F.; Haffner, B.; Khaewpong, N.; Maltese, M.; Kuppa, S.; Nguyen, T.; Takhounts, E.; Tannous, R.; et al. Development of Improved Injury Criteria for the Assessment of Advanced Automotive Restraint System-II; NHTSA: Washington, DC, USA, 1999. Available online: https://www.nhtsa.gov/sites/nhtsa.dot.gov/files/rev_criteria.pdf (accessed on 15 November 2020).
- Legal Information Institute. Federal Motor Vehicle Safety Standard-208; occupant crash protection: Code of Federal Regulations, 49CFR571.208S15.3.6. Legal Inf. Insutitute 2003, 49, 768–859. [Google Scholar]
- Laituri, T.R.; Prasad, P.; Sullivan, K.; Frankstein, M.; Thomas, R.S. Derivation and evaluation of a provisional, age-dependent, AIS3+ thoracic risk curve for belted adults in frontal impacts. SAE Tech. Paper 2005. [Google Scholar] [CrossRef]
- United Nations. Regulation No. 137; Uniform Provisions Concerning the Approval of Vehicles with Regard to the Protection of the Occupants in the Event of a Frontal Collision, United Nations Regulation. 2016. Available online: http://www.unece.org.net4all.ch/fileadmin/DAM/trans/doc/2009/wp29grsp/ELSA-7-04e.pdf (accessed on 15 November 2020).
- Jidousyagijutsukai Inpakutobaiomekanikusubumon Iinnkai. Koutsujiko de Hito ha Donoyounisite Kegasurunoka? Kougakugijutsusya to Iryoujujisya no Tameno Inpakutobaiomekanikusu. (How Can People Get Injured in Road Accidents? Impact Biomechanics for Engineering Technicians and Healthcare Professionals); JSAE: Tokyo, Japan, 2006; p. 66. [Google Scholar]
- Klinich, K.D.; Schneider, L.W.; Moore, J.L.; Pearlman, M.D. Injuries to pregnant occupants in automotive crashes. In Annual Proceedings/Association for the Advancement of Automotive Medicine. Annu. Proc. Assoc. Adv. Automot. Med. 1998, 42, 57–91. [Google Scholar]
- Weiss, H.B.; Songer, T.J.; Fabio, A. Fetal deaths related to maternal injury. JAMA 2001, 286, 1863–1868. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test | Impact Speed (km/h) | Neck Injury Criteria | Chest Deflection | Abdominal Pressure | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Right | Left | Anterior | Posterior | ||||||||
| Value | (Time) | Value | (Time) | Value | (Time) | Value | (Time) | Value | (Time) | ||
| Test 1 | 13 | 0.12 | (102 ms) | 1.9 mm | (160 ms) | 2.7 mm | (148 ms) | 103.3 kPa | (118 ms) | 88.9 kPa | (123 ms) |
| Test 2 | 26 | 0.36 | (100 ms) | 37.9 mm | (119 ms) | 38.5 mm | (120 ms) | 28.3 kPa | (82 ms) | 12.5 kPa | (165 ms) |
| Test 3 | 40 | 0.61 | (80 ms) | >40.9 mm | (98 ms) | >40.9 mm | (99 ms) | 58.6 kPa | (98 ms) | 48.7 kPa | (102 ms) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeda, A.; Motozawa, Y.; Takaso, M.; Nakamura, M.; Hattori, S.; Hitosugi, M. Mechanisms of Negative Fetal Outcome in Frontal Vehicle Collisions Involving Unbelted Pregnant Drivers. Healthcare 2021, 9, 25. https://doi.org/10.3390/healthcare9010025
Takeda A, Motozawa Y, Takaso M, Nakamura M, Hattori S, Hitosugi M. Mechanisms of Negative Fetal Outcome in Frontal Vehicle Collisions Involving Unbelted Pregnant Drivers. Healthcare. 2021; 9(1):25. https://doi.org/10.3390/healthcare9010025
Chicago/Turabian StyleTakeda, Arisa, Yasuki Motozawa, Marin Takaso, Mami Nakamura, Shinobu Hattori, and Masahito Hitosugi. 2021. "Mechanisms of Negative Fetal Outcome in Frontal Vehicle Collisions Involving Unbelted Pregnant Drivers" Healthcare 9, no. 1: 25. https://doi.org/10.3390/healthcare9010025