
Kinematic and Electrophysiological Characteristics of Pedal Operation by Elderly Drivers during Emergency Braking

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
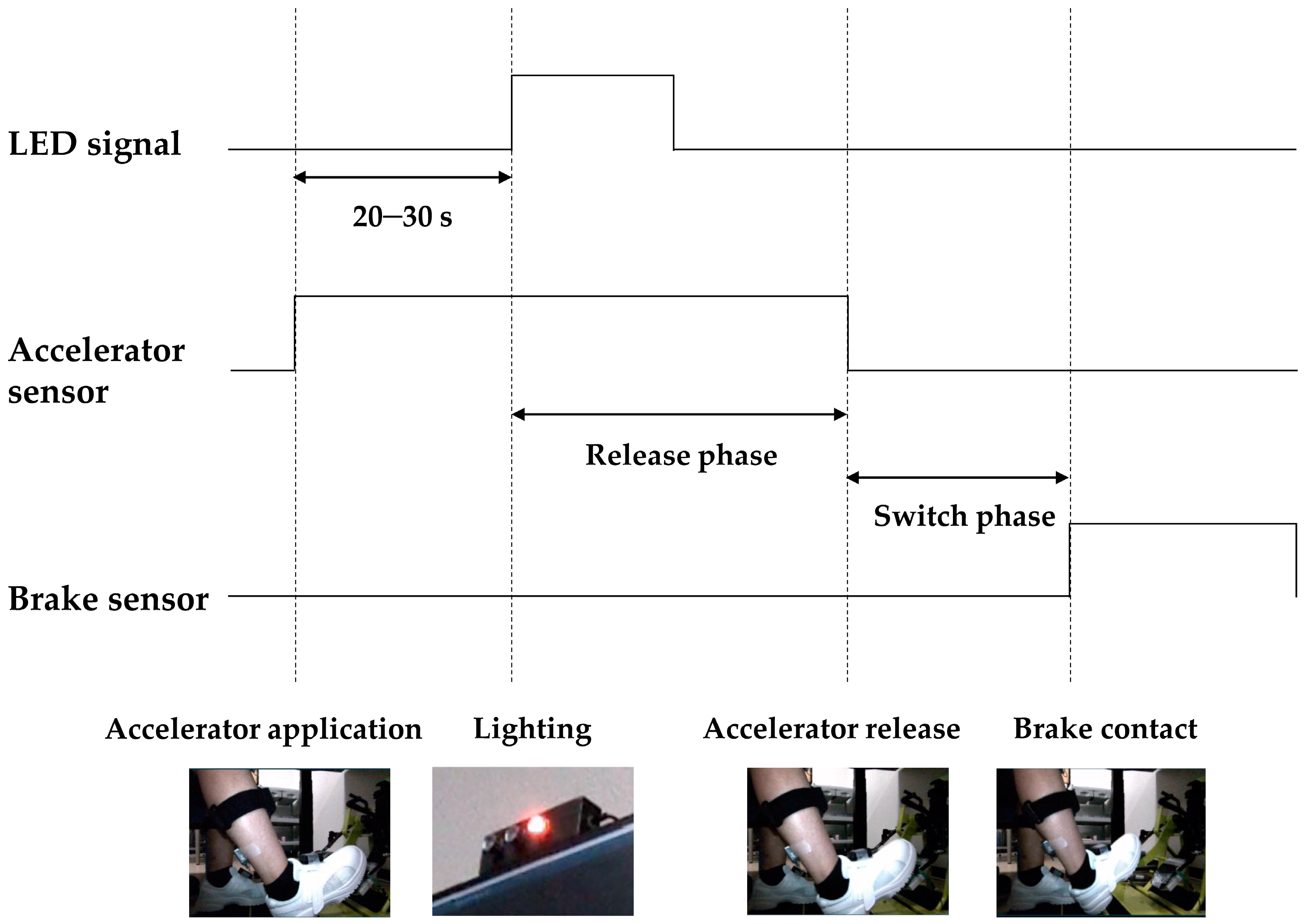
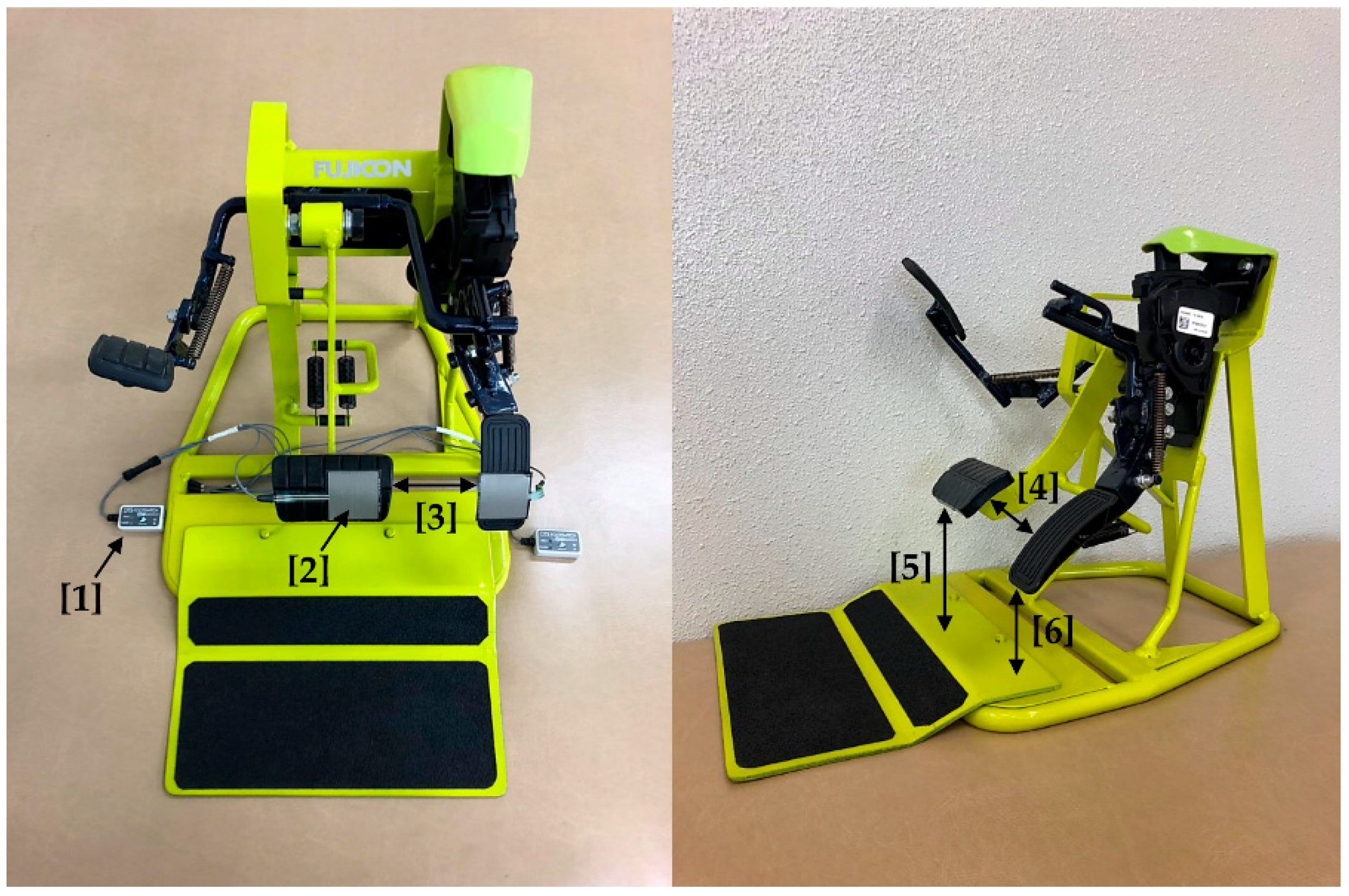
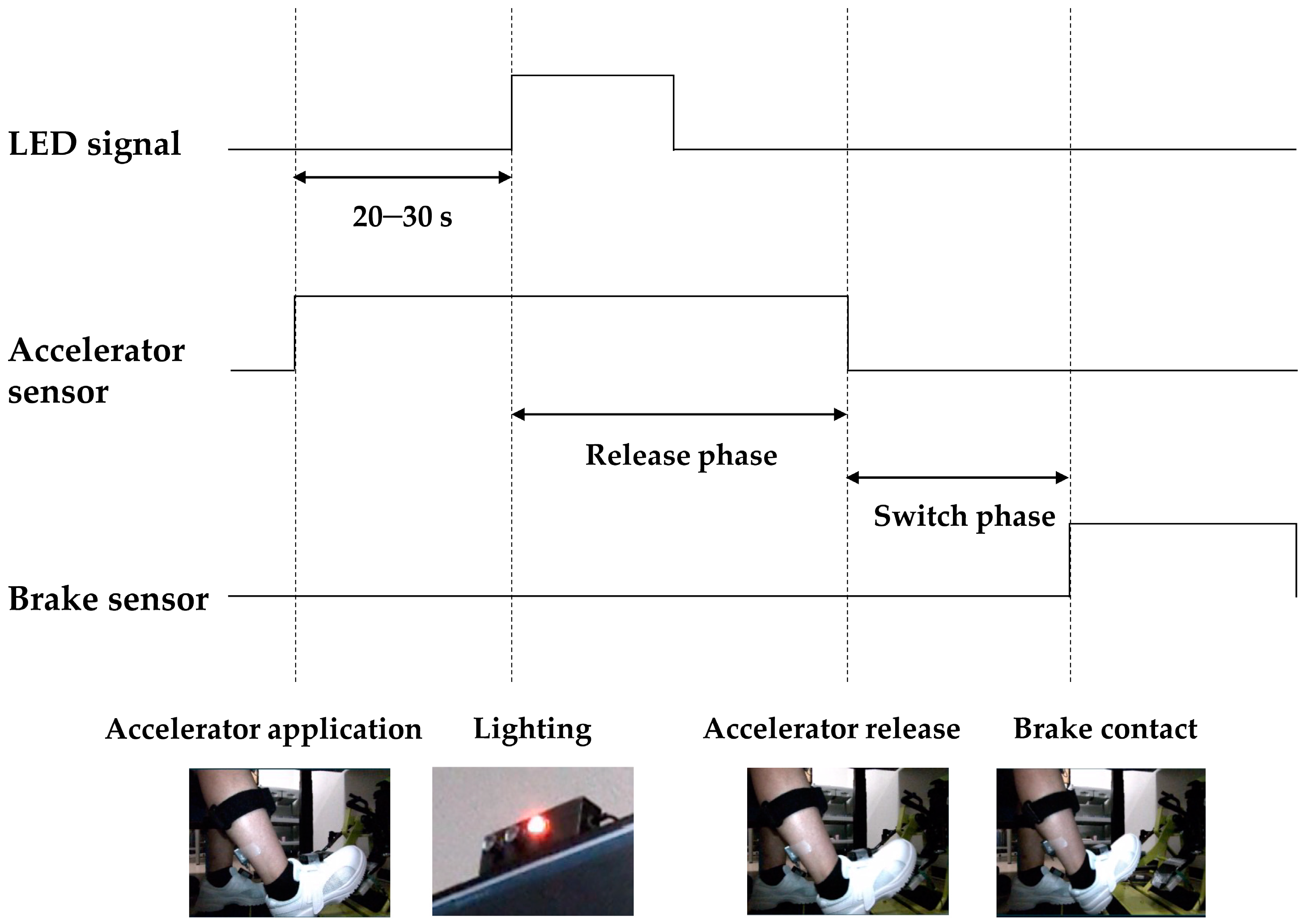
2.2. Experimental Setup and Protocol
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
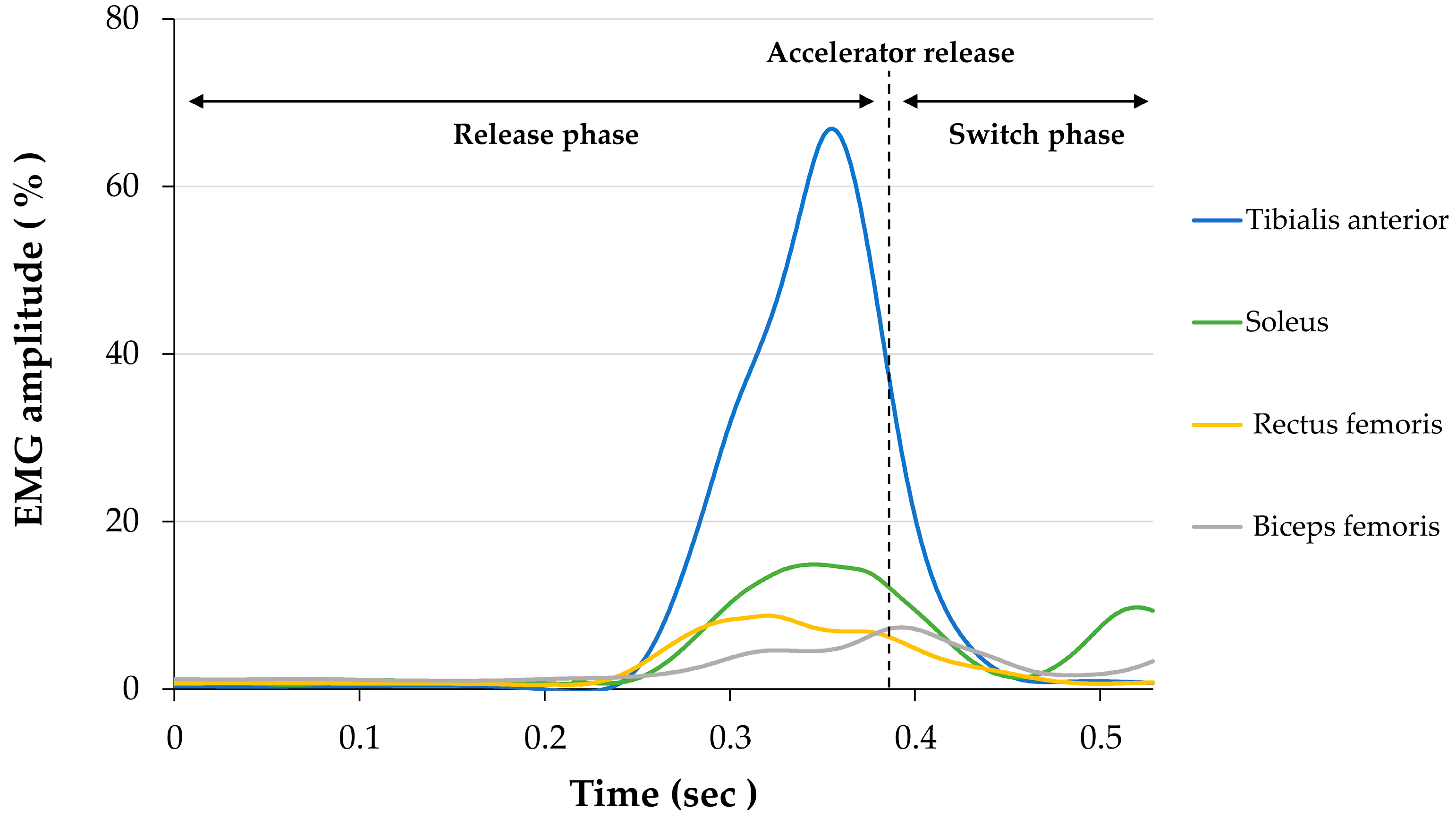
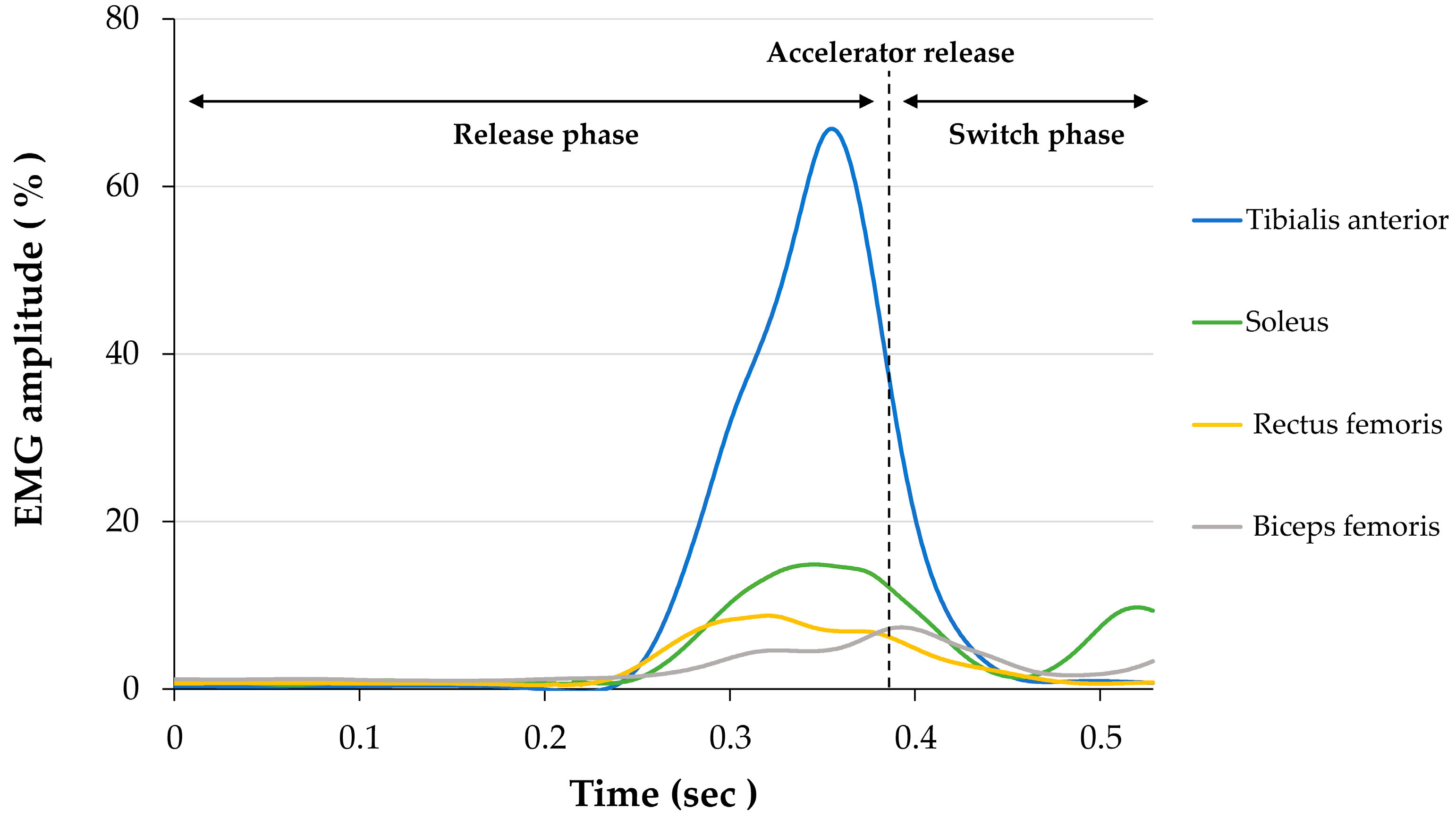
3.1. Electromyographic Activity
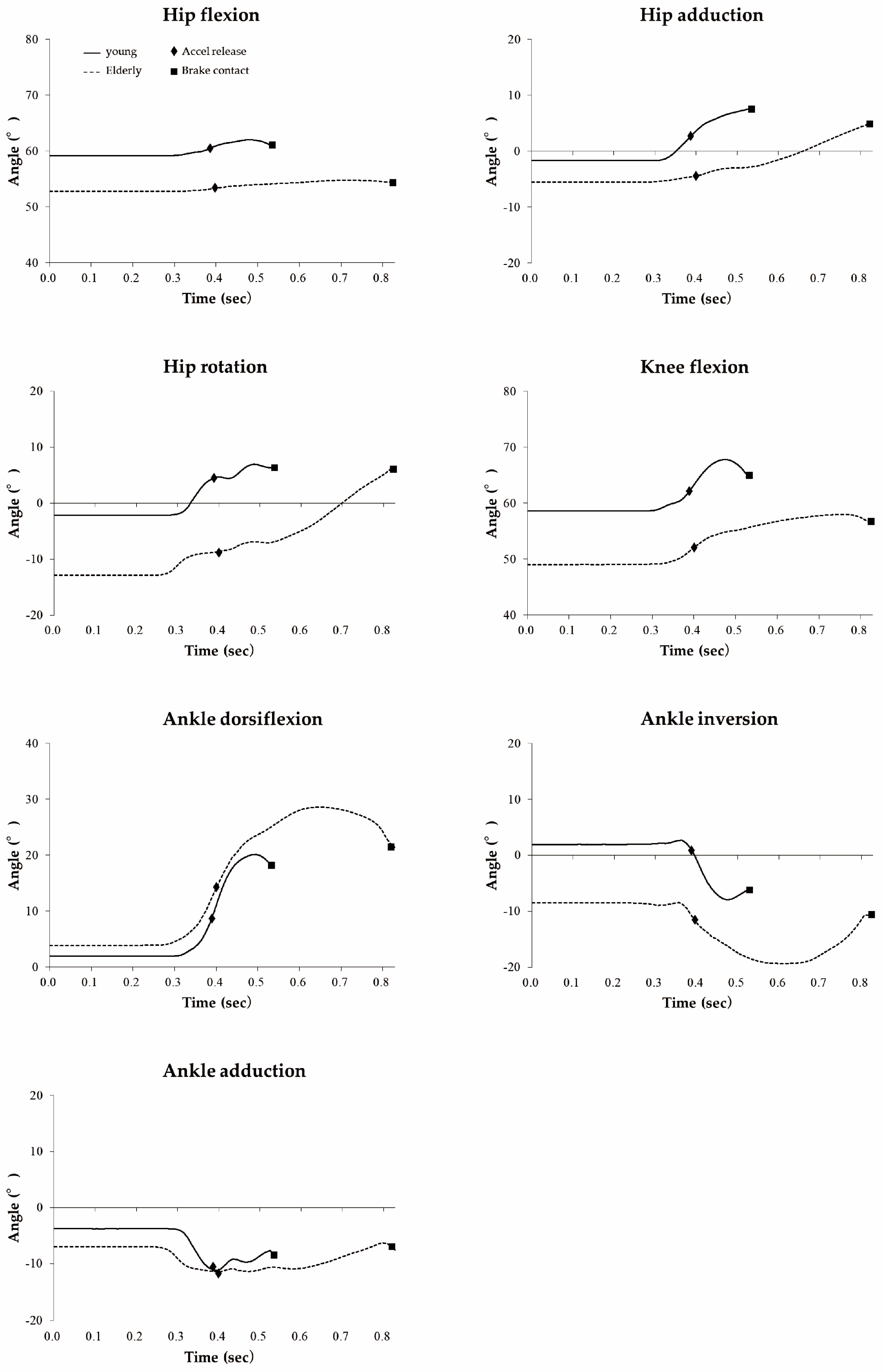
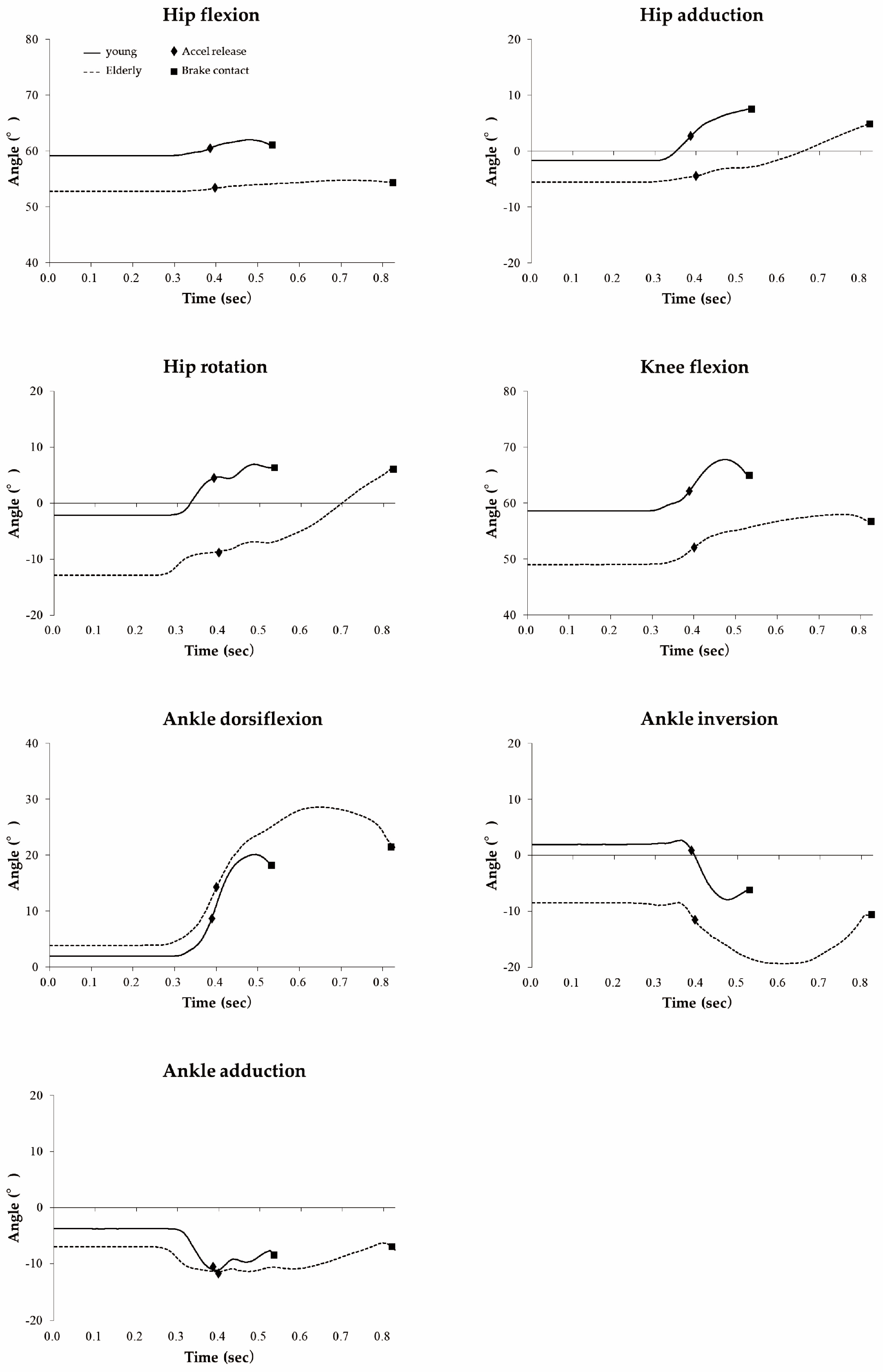
3.2. Kinematics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Police Agency. Available online: https://www.npa.go.jp/publications/statistics/koutsuu/jiko/R1shibou_bunseki.pdf (accessed on 27 April 2021).
- Wang, C.; Kosinski, C.J.; Schwartzberg, J.G.; Shanklin, A.V.; American Medical Association. Physician’s Guide to Assessing and Counseling Older Drivers (No. DOT-HS-809-647); American Medical Association: Chicago, IL, USA, 2003. [Google Scholar]
- Freund, B.; Colgrove, L.A.; Petrakos, D.; McLeod, R. In My Car the Brake Is on the Right: Pedal Errors Among Older Drivers. Accid. Anal. Prev. 2008, 40, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Lindle, R.S.; Metter, E.J.; Lynch, N.A.; Fleg, J.L.; Fozard, J.L.; Tobin, J.; Roy, T.A.; Hurley, B.F. Age and Gender Comparisons of Muscle Strength in 654 Women and Men Aged 20–93 yr. J. Appl. Physiol. 1997, 83, 1581–1587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thelen, D.G.; Schultz, A.B.; Alexander, N.B.; Ashton-Miller, J.A. Effects of Age on Rapid Ankle Torque Development. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1996, 51, M226–M232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGehee, D.V.; Roe, C.A.; Ng Boyle, L.N.; Wu, Y.; Ebe, K.; Foley, J.; Angell, L. The Wagging Foot of Uncertainty: Data Collection and Reduction Methods for Examining Foot Pedal Behavior in Naturalistic Driving. SAE Int. J. Trans. Saf. 2016, 4, 289–294. [Google Scholar] [CrossRef]
- Cantin, V.; Blouin, J.; Simoneau, M.; Teasdale, N. Driving in a Simulator and Lower Limb Movement Variability in Elderly Persons: Can We Infer Something About Pedal Errors. Adv. Transp. Stud. 2004, 39–46. [Google Scholar]
- Lodha, N.; Moon, H.; Kim, C.; Onushko, T.; Christou, E.A. Motor Output Variability Impairs Driving Ability in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1676–1681. [Google Scholar] [CrossRef] [Green Version]
- Bucsuhazy, K.; Svozilova, V.; Semela, M.; Stana, I.; Gruberova, O. Analysis of Driver Reaction during Braking and Avoidance Maneuver. IOP Conf. Ser. Mater. Sci. Eng. 2019, 603, 042085. [Google Scholar] [CrossRef]
- Jammes, Y.; Behr, M.; Weber, J.P.; Berdah, S. Consequences of Simulated Car Driving at Constant High Speed on the Sensorimotor Control of Leg Muscles and the Braking Response. Clin. Physiol. Funct. Imaging 2017, 37, 767–775. [Google Scholar] [CrossRef]
- Gao, Z.; Li, C.; Hu, H.; Zhao, H.; Chen, C.; Yu, H. Experimal Study of Young Male Drivers’ Responses to Vehicle Collision Using EMG of Lower Extremity. Bio-Med. Mater. Eng. 2015, 26, S563–S573. [Google Scholar] [CrossRef] [Green Version]
- Nishimoto, T.; Nagai, K. Influence of Aging on Lower Extremity Electromyogram under Crash Stopping. Trans. Jpn. Soc. Mech. Eng. Ser. C 2012, 78, 2962–2971. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Lavoie, B.A.; Devanne, H.; Capaday, C. Differential Control of Reciprocal Inhibition during Walking Versus Postural and Voluntary Motor Tasks in Humans. J. Neurophysiol. 1997, 78, 429–438. [Google Scholar] [CrossRef]
- Kido, A.; Tanaka, N.; Stein, R.B. Spinal Excitation and Inhibition Decrease as Humans Age. Can. J. Physiol. Pharmacol. 2004, 82, 238–248. [Google Scholar] [CrossRef]
- Shinohara, K.; Kimura, T. The Characteristics of Foot Position and Movement for Operating the Automotive Pedal and the Experience of Pedal Misapplications. Traffic. Sci. 2018, 49, 33–40. (In Japanese) [Google Scholar]
- Behr, M.; Poumarat, G.; Serre, T.; Arnoux, P.J.; Thollon, L.; Brunet, C. Posture and Muscular Behaviour in Emergency Braking: An Experimental Approach. Accid. Anal. Prev. 2010, 42, 797–801. [Google Scholar] [CrossRef]
- Sakuma, N.; Ura, C.; Miyamae, F.; Inagaki, H.; Ito, K.; Niikawa, H.; Awata, S. Distribution of Mini-Mental State Examination scores among urban community-dwelling older adults in Japan. Int. J. Geriatr. Psychiatry 2017, 32, 718–725. [Google Scholar] [CrossRef]
- Fujita, K.; Kobayashi, Y.; Hitosugi, M. Temporal Changes in Electromyographic Activity and Gait Ability During Extended Walking in Individuals Post-Stroke: A Pilot Study. Healthcare 2021, 9, 444. [Google Scholar] [CrossRef]
- Fujita, K.; Kobayashi, Y.; Miaki, H.; Hori, H.; Tsushima, Y.; Sakai, R.; Nomura, T.; Ogawa, T.; Kinoshita, H.; Nishida, T.; et al. Pedaling Improves Gait Ability of Hemiparetic Patients with Stiff-Knee Gait: Fall Prevention During Gait. J. Stroke Cerebrovasc. Dis. 2020, 29, 105035. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Miaki, H.; Hori, H.; Kobayashi, Y.; Nakagawa, T. How Effective Is Physical Therapy for Gait Muscle Activity in Hemiparetic Patients Who Receive Botulinum Toxin Injections? Eur. J. Phys. Rehabil. Med. 2019, 55, 8–18. [Google Scholar] [CrossRef]
- Chow, J.W.; Yablon, S.A.; Stokic, D.S. Coactivation of Ankle Muscles During Stance Phase of Gait in Patients with Lower Limb Hypertonia After Acquired Brain Injury. Clin. Neurophysiol. 2012, 123, 1599–1605. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 11, 155–159. [Google Scholar] [CrossRef]
- Green, M. “How Long Does It Take to Stop?” Methodological Analysis of Driver Perception-Brake Times. Transp. Hum. Factors 2000, 2, 195–216. [Google Scholar] [CrossRef]
- Toft, E.; Sinkjaer, T.; Andreassen, S.; Larsen, K.N.U.D. Mechanical and Electromyographic Responses to Stretch of the Human Ankle Extensors. J. Neurophysiol. 1991, 65, 1402–1410. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Mazzocchio, R.; Scarpini, C. Changes in Ia Reciprocal Inhibition from the Peroneal Nerve to the Soleus α-Motoneurons with Different Static Body Positions in Man. Neurosci. Lett. 1988, 84, 283–286. [Google Scholar] [CrossRef]
- Earles, D.; Vardaxis, V.; Koceja, D. Regulation of Motor Output between Young and Elderly Subjects. Clin. Neurophysiol. 2001, 112, 1273–1279. [Google Scholar] [CrossRef]
- Schünke, M.; Schulte, E.; Schumacher, U.; Voll, M.; Wesker, K.; LernAtlas der Anatomie, P. Allgemeine Anatomie und Bewegunssystem; Georg Thieme Verlag: Stuttgart, Germany, 2014. [Google Scholar]
- Johnson, M.; Polgar, J.; Weightman, D. Data on the Distribution of Fiber Types in Thirty-Six Human Muscles: An Autopsy Study. J. Neurol. Sci. 1973, 18, 111–129. [Google Scholar] [CrossRef]
- Nilwik, R.; Snijders, T.; Leenders, M.; Groen, B.B.; van Kranenburg, J.; Verdijk, L.B.; van Loon, L.J. The Decline in Skeletal Muscle Mass with Aging Is Mainly Attributed to a Reduction in Type II Muscle Fiber Size. Exp. Gerontol. 2013, 48, 492–498. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Young (n = 11) | Elderly (n = 10) | p | ||
|---|---|---|---|---|
| Age | (Years) | 26.3 ± 5.4 | 78.4 ± 4.0 | <0.001 |
| Sex | (Female/Male) | 6/5 | 5/5 | NS |
| Height | (cm) | 164.7 ± 8.8 | 157.6 ± 6.5 | NS |
| Weight | (kg) | 55.4 ± 9.1 | 56.0 ± 6.5 | NS |
| Shoe size | (cm) | 24.5 ± 1.2 | 24.6 ± 1.1 | NS |
| Driving self-confidence | 4 (4.5) | 0 (1.5) | 0.033 | |
| MMSE | 30 (0) | 28 (2.5) | 0.002 | |
| Pedal error history | (Yes/No) | 2/9 | 1/9 | NS |
| Fall history | (Yes/No) | 0/11 | 1/9 | NS |
| Young (n = 11) | Elderly (n = 10) | p | ES | |
|---|---|---|---|---|
| Reaction time (s) | ||||
| Entire phase | 0.650 ± 0.047 | 0.762 ± 0.059 | <0.001 | 2.104 |
| Release phase | 0.450 ± 0.038 | 0.473 ± 0.064 | NS | 0.430 |
| Switch phase | 0.199 ± 0.031 | 0.289 ± 0.088 | 0.014 | 1.386 |
| Muscle activity onset (s) | ||||
| Tibialis anterior | 0.290 ± 0.050 | 0.320 ± 0.072 | NS | 0.473 |
| Soleus | 0.332 ± 0.047 | 0.339 ± 0.076 | NS | 0.108 |
| Rectus femoris | 0.316 ± 0.046 | 0.472 ± 0.156 | 0.015 | 1.387 |
| Biceps femoris | 0.365 ± 0.036 | 0.409 ± 0.068 | NS | 0.823 |
| Time difference between TA and Sol | 0.042 ± 0.028 | 0.019 ± 0.011 | 0.033 | 1.052 |
| Young (n = 11) | Elderly (n = 10) | p | ES | ||
|---|---|---|---|---|---|
| Amplitude (%) | |||||
| Tibialis anterior | A a | 2.3 ± 2.4 | 3.5 ± 1.9 | NS | 0.535 |
| R p | 52.6 ± 16.6 | 72.7 ± 20.2 | 0.028 | 1.096 | |
| S p | 54.0 ± 21.7 | 75.9 ± 29.3 | NS | 0.854 | |
| S m | 4.9 ± 4.7 | 6.7 ± 5.4 | NS | 0.356 | |
| Soleus | A a | 2.2 ± 1.3 | 3.2 ± 1.5 | NS | 0.686 |
| R p | 12.7 ± 5.7 | 28.0 ± 11.3 | 0.003 | 1.727 | |
| S p | 28.4 ± 15.0 | 55.0 ± 23.6 | 0.009 | 1.341 | |
| S m | 3.0 ± 1.7 | 11.5 ± 5.6 | 0.001 | 2.086 | |
| Rectus femoris | A a | 2.3 ± 2.8 | 3.3 ± 1.5 | NS | 0.416 |
| R p | 11.6 ± 5.9 | 10.0 ± 7.3 | NS | 0.252 | |
| S p | 12.0 ± 5.3 | 13.0 ± 8.7 | NS | 0.132 | |
| S m | 3.4 ± 2.0 | 3.1 ± 1.2 | NS | 0.134 | |
| Biceps femoris | A a | 1.7 ± 1.9 | 1.5 ± 0.7 | NS | 0.138 |
| R p | 3.5 ± 2.8 | 6.4 ± 5.7 | NS | 0.661 | |
| S p | 5.5 ± 3.9 | 9.6 ± 5.9 | NS | 0.820 | |
| S m | 2.3 ± 2.0 | 2.8 ± 2.1 | NS | 0.254 | |
| Co-activation duration (%) | |||||
| TA―Sol | R | 75.8 ± 12.4 | 86.1 ± 6.5 | 0.038 | 1.025 |
| S | 78.9 ± 13.6 | 89.6 ± 13.5 | NS | 0.785 | |
| RF―BF | R | 61.3 ± 23.3 | 35.5 ± 23.7 | 0.028 | 1.097 |
| S | 73.0 ± 22.4 | 49.3 ± 24.7 | 0.041 | 1.009 |
| Young (n = 11) | Elderly (n = 10) | p | ES | ||
|---|---|---|---|---|---|
| Hip flexion | A | 49.2 ± 12.7 | 56.3 ± 10.3 | NS | 0.620 |
| R | 49.7 ± 12.3 | 56.8 ± 10.8 | NS | 0.611 | |
| S p | 53.5 ± 11.7 | 59.4 ± 11.0 | NS | 0.524 | |
| B | 52.8 ± 11.7 | 58.2 ± 11.5 | NS | 0.460 | |
| Hip adduction | A | −2.4 ± 1.7 | −3.4 ± 3.3 | NS | 0.395 |
| R | −0.1 ± 2.3 | −2.2 ± 3.8 | NS | 0.654 | |
| S p | 7.0 ± 3.6 | 5.1 ± 2.3 | NS | 0.627 | |
| B | 6.8 ± 3.6 | 4.9 ± 2.2 | NS | 0.651 | |
| Hip internal rotation | A | −5.8 ± 8.6 | 1.6 ± 5.2 | 0.037 | 1.030 |
| R | −4.1 ± 9.2 | 3.3 ± 5.0 | NS | 0.941 | |
| S p | 3.9 ± 9.3 | 15.6 ± 9.0 | 0.012 | 1.274 | |
| B | 1.2 ± 8.6 | 13.7 ± 9.0 | 0.007 | 1.383 | |
| Knee flexion | A | 61.7 ± 10.4 | 48.3 ± 9.5 | 0.018 | 1.194 |
| R | 63.9 ± 9.7 | 51.0 ± 12.3 | 0.020 | 1.171 | |
| S p | 72.6 ± 8.3 | 58.7 ± 12.6 | 0.010 | 1.311 | |
| B | 70.0 ± 8.7 | 55.0 ± 13.2 | 0.009 | 1.348 | |
| Ankle dorsiflexion | A | 5.9 ± 9.4 | 0.8 ± 5.4 | NS | 0.661 |
| R | 12.6 ± 5.8 | 8.6 ± 6.1 | NS | 0.669 | |
| S p | 27.4 ± 5.5 | 26.2 ± 4.6 | NS | 0.234 | |
| B | 22.6 ± 5.8 | 17.8 ± 6.4 | NS | 0.786 | |
| Ankle inversion | A | 0.8 ± 7.1 | 0.7 ± 6.5 | NS | 0.026 |
| R | 0.2 ± 7.5 | −1.5 ± 6.0 | NS | 0.242 | |
| S p | 6.6 ± 9.3 | 6.6 ± 8.4 | NS | 0.003 | |
| B | 4.5 ± 8.7 | 5.2 ± 7.9 | NS | 0.087 | |
| Ankle adduction | A | −0.9 ± 3.8 | −7.7 ± 3.9 | 0.001 | 1.743 |
| R | −3.0 ± 4.2 | −9.1 ± 4.1 | 0.005 | 1.471 | |
| S p | 3.7 ± 4.3 | −1.5 ± 6.1 | 0.044 | 0.990 | |
| B | 3.0 ± 4.2 | −2.4 ± 6.0 | 0.033 | 1.056 |
| Young (n = 11) | Elderly (n = 10) | p | ES | ||
|---|---|---|---|---|---|
| Hip flexion | R | 28.8 ± 19.4 | 23.6 ± 13.3 | NS | 0.308 |
| S | 48.4 ± 16.7 | 37.9 ± 19.7 | NS | 0.577 | |
| Hip extension | R | 8.2 ± 4.7 | 10.0 ± 15.1 | NS | 0.166 |
| S | 24.8 ± 10.1 | 29.0 ± 11.2 | NS | 0.393 | |
| Hip adduction | R | 46.9 ± 26.5 | 24.7 ± 14.9 | 0.039 | 1.021 |
| S | 69.2 ± 24.1 | 48.9 ± 12.8 | 0.036 | 1.037 | |
| Hip abduction | R | 3.0 ± 2.8 | 1.8 ± 0.8 | NS | 0.542 |
| S | 0.5 ± 14.6 | 9.9 ± 14.2 | NS | 0.656 | |
| Hip internal rotation | R | 47.5 ± 30.6 | 52.7 ± 22.1 | NS | 0.195 |
| S | 111.2 ± 52.9 | 138.5 ± 64.1 | NS | 0.467 | |
| Hip external rotation | R | 17.4 ± 13.1 | 26.3 ± 16.9 | NS | 0.596 |
| S | 63.2 ± 45.7 | 102.8 ± 49.4 | NS | 0.834 | |
| Knee flexion | R | 76.4 ± 39.0 | 75.9 ± 32.2 | NS | 0.015 |
| S | 110.8 ± 25.6 | 108.5 ± 34.2 | NS | 0.078 | |
| Knee extension | R | 8.9 ± 9.8 | 16.3 ± 13.9 | NS | 0.621 |
| S | 86.9 ± 29.6 | 84.0 ± 21.9 | NS | 0.109 | |
| Ankle dorsiflexion | R | 184.6 ± 88.3 | 179.4 ± 59.6 | NS | 0.068 |
| S | 235.9 ± 68.4 | 226.6 ± 51.8 | NS | 0.152 | |
| Ankle plantarflexion | R | 2.8 ± 1.9 | 6.4 ± 7.7 | NS | 0.644 |
| S | 203.3 ± 75.3 | 220.5 ± 51.3 | NS | 0.265 | |
| Ankle inversion | R | 28.7 ± 28.1 | 22.6 ± 18.0 | NS | 0.256 |
| S | 137.0 ± 47.2 | 151.3 ± 40.4 | NS | 0.323 | |
| Ankle eversion | R | 60.8 ± 50.3 | 79.1 ± 40.2 | NS | 0.401 |
| S | 150.1 ± 69.0 | 167.1 ± 67.4 | NS | 0.249 | |
| Ankle adduction | R | 16.3 ± 12.3 | 30.3 ± 19.5 | NS | 0.865 |
| S | 118.1 ± 40.0 | 140.1 ± 71.4 | NS | 0.385 | |
| Ankle abduction | R | 53.0 ± 39.2 | 54.9 ± 27.4 | NS | 0.057 |
| S | 80.6 ± 45.0 | 114.4 ± 52.7 | NS | 0.692 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujita, K.; Kobayashi, Y.; Sato, M.; Hori, H.; Sakai, R.; Ogawa, T.; Sugano, T.; Kawabata, K.; Hitosugi, M. Kinematic and Electrophysiological Characteristics of Pedal Operation by Elderly Drivers during Emergency Braking. Healthcare 2021, 9, 852. https://doi.org/10.3390/healthcare9070852
Fujita K, Kobayashi Y, Sato M, Hori H, Sakai R, Ogawa T, Sugano T, Kawabata K, Hitosugi M. Kinematic and Electrophysiological Characteristics of Pedal Operation by Elderly Drivers during Emergency Braking. Healthcare. 2021; 9(7):852. https://doi.org/10.3390/healthcare9070852
Chicago/Turabian StyleFujita, Kazuki, Yasutaka Kobayashi, Mamiko Sato, Hideaki Hori, Ryo Sakai, Tomoki Ogawa, Tomonari Sugano, Kaori Kawabata, and Masahito Hitosugi. 2021. "Kinematic and Electrophysiological Characteristics of Pedal Operation by Elderly Drivers during Emergency Braking" Healthcare 9, no. 7: 852. https://doi.org/10.3390/healthcare9070852