
TFEB Rearranged Renal Cell Carcinoma: Pathological and Molecular Characterization of 10 Cases, with Novel Clinical Implications: A Single Center 10-Year Experience

Abstract
:1. Introduction
2. Material and Methods
2.1. Patients and Samples
2.2. Immunohistochemistry
2.3. Fluorescence In Situ Hybridization (FISH)
3. Results
3.1. Clinicopathologic Findings
3.2. Microscopic Features
3.2.1. Architecture
3.2.2. Cytomorphological Features
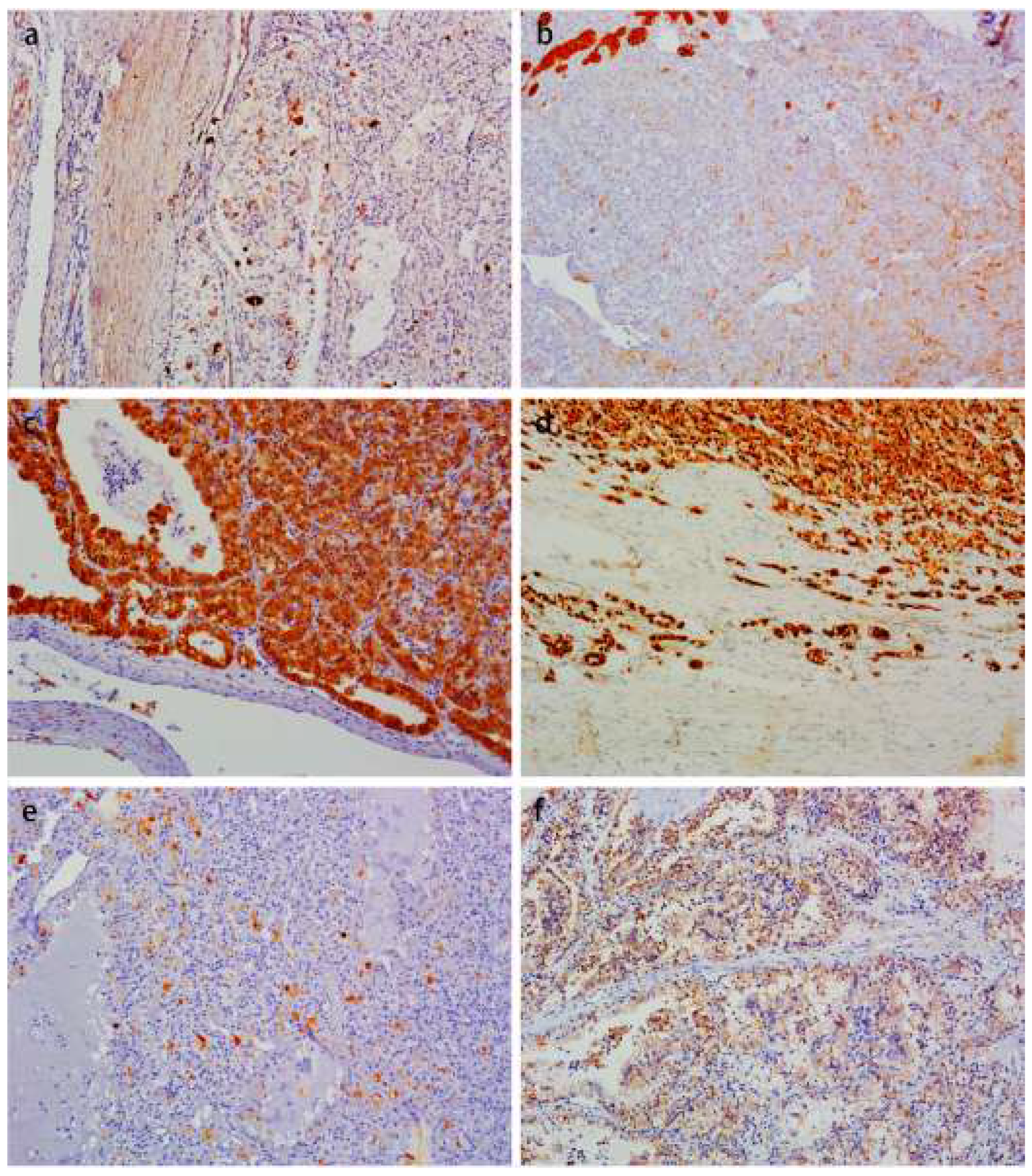
3.3. Immunohistochemistry Findings
3.4. FISH Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Malouf, G.G.; Su, X.; Yao, H.; Gao, J.; Xiong, L.; He, Q.; Compérat, E.; Couturier, J.; Molinié, V.; Escudier, B.; et al. Next-generation sequencing of translocation renal cell carcinoma reveals novel RNA splicing partners and frequent mutations of chromatin-remodeling genes. Clin. Cancer Res. 2014, 20, 4129–4140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durinck, S.; Stawiski, E.W.; Pavía-Jiménez, A.; Modrusan, Z.; Kapur, P.; Jaiswal, B.S.; Zhang, N.; Toffessi-Tcheuyap, V.; Nguyen, T.T.; Pahuja, K.B.; et al. Spectrum of diverse genomic alterations define non-clear cell renal carcinoma subtypes. Nat. Genet. 2015, 47, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Linehan, W.M.; Ricketts, C.J. The Cancer Genome Atlas of renal cell carcinoma: Findings and clinical implications. Nat. Rev. Urol. 2019, 16, 539–552. [Google Scholar] [CrossRef] [PubMed]
- Xia, Q.Y.; Wang, X.T.; Fang, R.; Wang, Z.; Zhao, M.; Chen, H.; Chen, N.; Teng, X.D.; Wang, X.; Wei, X.; et al. Clinicopathologic and Molecular Analysis of the TFEB Fusion Variant Reveals New Members of TFEB Translocation Renal Cell Carcinomas (RCCs): Expanding the Genomic Spectrum. Am. J. Surg. Pathol. 2020, 44, 477–489. [Google Scholar] [CrossRef]
- Caliò, A.; Harada, S.; Brunelli, M.; Pedron, S.; Segala, D.; Portillo, S.C.; Magi-Galluzzi, C.; Netto, G.J.; Mackinnon, A.C.; Martignoni, G. TFEB rearranged renal cell carcinoma. A clinicopathologic and molecular study of 13 cases. Tumors harboring MALAT1-TFEB, ACTB-TFEB, and the novel NEAT1-TFEB translocations constantly express PDL1. Mod. Pathol. 2021, 34, 842–850. [Google Scholar] [CrossRef]
- Moch, H.; Amin, M.B.; Berney, D.M.; Compérat, E.M.; Gill, A.J.; Hartmann, A.; Menon, S.; Raspollini, M.R.; Rubin, M.A.; Srigley, J.R.; et al. The 2022 World Health Organization Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2022, 82, 458–468. [Google Scholar] [CrossRef]
- Argani, P.; Hawkins, A.; Griffin, C.A.; Goldstein, J.D.; Haas, M.; Beckwith, J.B.; Mankinen, C.B.; Perlman, E.J. A distinctive pediatric renal neoplasm characterized by epithelioid morphology, basement membrane production, focal HMB45 immunoreactivity, and t (6;11) (p21.1; q12) chromosome translocation. Am. J. Pathol. 2001, 158, 2089–2096. [Google Scholar] [CrossRef] [Green Version]
- Argani, P. MiT family translocation renal cell carcinoma. Semin. Diagn. Pathol. 2015, 32, 103–113. [Google Scholar] [CrossRef]
- Wyvekens, N.; Rechsteiner, M.; Fritz, C.; Wagner, U.; Tchinda, J.; Wenzel, C.; Kuithan, F.; Horn, L.C.; Moch, H. Histological and molecular characterization of TFEB-rearranged renal cell carcinomas. Virchows Arch. 2019, 474, 625–631. [Google Scholar] [CrossRef]
- Caliò, A.; Brunelli, M.; Segala, D.; Pedron, S.; Tardanico, R.; Remo, A.; Gobbo, S.; Meneghelli, E.; Doglioni, C.; Hes, O.; et al. t (6;11) renal cell carcinoma: A study of seven cases including two with aggressive behavior, and utility of CD68 (PG-M1) in the differential diagnosis with pure epithelioid PEComa/epithelioid angiomyolipoma. Mod. Pathol. 2018, 31, 474–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, Q.Y.; Wang, X.T.; Zhan, X.M.; Tan, X.; Chen, H.; Liu, Y.; Shi, S.S.; Wang, X.; Wei, X.; Ye, S.B.; et al. Xp11 translocation renal cell carcinomas (RCCs) with RBM10-TFE3 gene fusion demonstrating melanotic features and overlapping morphology with t (6;11) RCC: Interest and diagnostic pitfall in detecting a paracentric inversion of TFE3. Am. J. Surg. Pathol. 2017, 41, 663–676. [Google Scholar] [CrossRef] [PubMed]
- Zattara-Cannoni, H.; Daniel, L.; Roll, P.; Coulange, C.; Vagner-Capodano, A.M. Molecular cytogenetics of t(X;1) (p11.2;q21) with complex rearrangements in a renal cell carcinoma. Cancer Genet. Cytogenet. 2000, 123, 61–64. [Google Scholar] [CrossRef]
- Mancini, M.; Righetto, M.; Baggio, G. Gender-Related Approach to Kidney Cancer Management: Moving Forward. Int. J. Mol. Sci. 2020, 21, 3378. [Google Scholar] [CrossRef] [PubMed]
- Argani, P.; Reuter, V.E.; Zhang, L.; Sung, Y.S.; Ning, Y.; Epstein, J.I.; Netto, G.J.; Antonescu, C.R. TFEB-amplified Renal Cell Carcinomas: An Aggressive Molecular Subset Demonstrating Variable Melanocytic Marker Expression and Morphologic Heterogeneity. Am. J. Surg. Pathol. 2016, 40, 1484–1495. [Google Scholar] [CrossRef]
- Argani, P.; Yonescu, R.; Morsberger, L.; Morris, K.; Netto, G.J.; Smith, N.; Gonzalez, N.; Illei, P.B.; Ladanyi, M.; Griffin, C.A. Molecular confirmation of t (6;11) (p21; q12) renal cell carcinoma in archival paraffin-embedded material using a break-apart TFEB FISH assay expands its clinicopathologic spectrum. Am. J. Surg. Pathol. 2012, 36, 1516–1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, S.R.; Eble, J.N.; Palanisamy, N. Sclerosing TFEB-rearrangement renal cell carcinoma: A recurring histologic pattern. Hum. Pathol. 2017, 62, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Trpkov, K.; Hes, O.; Williamson, S.R.; Adeniran, A.J.; Agaimy, A.; Alaghehbandan, R.; Amin, M.B.; Argani, P.; Chen, Y.B.; Cheng, L.; et al. New developments in existing WHO entities and evolving molecular concepts: The Genitourinary Pathology Society (GUPS) update on renal neoplasia. Mod. Pathol. 2021, 34, 1392–1424. [Google Scholar] [CrossRef]
- Tretiakova, M.S. Eosinophilic solid and cystic renal cell carcinoma mimicking epithelioid angiomyolipoma: Series of 4 primary tumors and 2 metastases. Hum. Pathol. 2018, 80, 65–75. [Google Scholar] [CrossRef]
- Lobo, J.; Rechsteiner, M.; Helmchen, B.M.; Rupp, N.J.; Weber, A.; Moch, H. Eosinophilic solid and cystic renal cell carcinoma and renal cell carcinomas with TFEB alterations: A comparative study. Histopathology 2022, 81, 32–43. [Google Scholar] [CrossRef]
- Simonaggio, A.; Ambrosetti, D.; Verkarre, V.; Auvray, M.; Oudard, S.; Vano, Y.A. MiTF/TFE Translocation Renal Cell Carcinomas: From Clinical Entities to Molecular Insights. Int. J. Mol. Sci. 2022, 23, 7649. [Google Scholar] [CrossRef]
- Argani, P. Translocation carcinomas of the kidney. Genes Chromosomes Cancer 2022, 61, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Peckova, K.; Vanecek, T.; Martinek, P.; Spagnolo, D.; Kuroda, N.; Brunelli, M.; Vranic, S.; Djuricic, S.; Rotterova, P.; Daum, O.; et al. Aggressive and nonaggressive translocation t (6;11) renal cell carcinoma: Comparative study of 6 cases and review of the literature. Ann. Diagn. Pathol. 2014, 18, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.E.; Illei, P.B.; Allaf, M.; Gonzalez, N.; Morris, K.; Hicks, J.; DeMarzo, A.; Reuter, V.E.; Amin, M.B.; Epstein, J.I.; et al. t (6;11) renal cell carcinoma (RCC): Expanded immunohistochemical profile emphasizing novel RCC markers and report of 10 new genetically confirmed cases. Am. J. Surg. Pathol. 2014, 38, 604–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dizman, N.; Philip, E.J.; Pal, S.K. Genomic profiling in renal cell carcinoma. Nat. Rev. Nephrol. 2020, 16, 435–451. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Motzer, R.J. Systemic Therapy for Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2017, 376, 354–366. [Google Scholar] [CrossRef]
- Walter, B.; Gil, S.; Naizhen, X.; Kruhlak, M.J.; Linehan, W.M.; Srinivasan, R.; Merino, M.J. Determination of the Expression of PD-L1 in the Morphologic Spectrum of Renal Cell Carcinoma. J. Cancer 2020, 11, 3596–3603. [Google Scholar] [CrossRef]
- Rosellini, M.; Marchetti, A.; Mollica, V.; Rizzo, A.; Santoni, M.; Massari, F. Prognostic and predictive biomarkers for immunotherapy in advanced renal cell carcinoma. Nat. Rev. Urol. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Lacquaniti, A.; Altavilla, G.; Picone, A.; Donato, V.; Chirico, V.; Mondello, P.; Aloisi, C.; Marabello, G.; Loddo, S.; Buemi, A.; et al. Apelin beyond kidney failure and hyponatremia: A useful biomarker for cancer disease progression evaluation. Clin. Exp. Med. 2015, 15, 97–105. [Google Scholar] [CrossRef]
- Bakouny, Z.; Sadagopan, A.; Ravi, P.; Metaferia, N.Y.; Li, J.; AbuHammad, S.; Tang, S.; Denize, T.; Garner, E.R.; Gao, X.; et al. Integrative clinical and molecular characterization of translocation renal cell carcinoma. Cell Rep. 2022, 38, 110190. [Google Scholar] [CrossRef]
- Keir, M.E.; Latchman, Y.E.; Freeman, G.J.; Sharpe, A.H. Programmed death-1 (PD-1): PD-ligand 1 interactions inhibit TCR-mediated positive selection of thymocytes. J. Immunol. 2005, 175, 7372–7379. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Location | Age/Gender | Tumor Size (mm) | Procedure | Gross | Stage | WHO/ISUP Grade | Status | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | R | 25/F | 57 | Radical | Variegated cystic solid | pT1bNxMx | G2-G3 | ANED | 25 |
| 2 | R | 26/M | 37 | Partial | Variegated cystic solid | pT1aNxMx | G2 | ANED | 24 |
| 3 | R | 24/F | 72 | Radical | Gray-yellow solid | pT2aNxMx | G2-G3 | ANED | 19 |
| 4 | L | 38/F | 160 | Radical | Gray-yellow cystic solid | pT2bNxMx | G2 | ANED | 4 |
| 5 | L | 40/M | 122 | Radical | Variegated cystic solid | pT2bN0Mx | G3-G4 | ANED | 108 |
| 6 | L | 50/F | 34 | Partial | Gray-yellow cystic solid | pT1aNxMx | G2 | ANED | 79 |
| 7 | R | 23/F | 130 | Radical | Gray-brown solid | pT3aNxMx | G2 | ANED | 45 |
| 8 | L | 33/M | 82 | Partial | Gray-yellow cystic solid | pT2aNxMx | G2 | ANED | 57 |
| 9 | R | 35/M | 110 | Radical | Gray-yellow honeycomb | pT2bNxMx | G2 | ANED | 44 |
| 10 | R | 55/F | 45 | Radical | Gray-yellow cystic solid | pT3aNxMx | G2-G3 | ANED | 43 |
| Case | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Nests | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 |
| Papillary | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Pseudopapillary | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Tubular | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Solid sheet | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Cystic | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Biphasic | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 |
| Non-neoplastic renal tubules | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Psammoma bodies | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Pseudocapsule | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Pigmentation | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Multinucleate cells | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Clear and eosinophilic cytoplasm | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Intracellular vacuolization | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 |
| Rhabdoid | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hemorrhagic necrotic fibrosis | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Infiltrated the perirenal or renal sinus adipose | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| Thick-walled vessels | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Case | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| CK20 | + | + | - | - | + | + | - | + | + | + |
| Melan-A | ++ | ++ | ++ | +++ | ++ | +++ | ++ | +++ | +++ | ‘++ |
| CK7 | - | - | - | - | - | - | - | - | - | - |
| CD10 | ++ | + | - | + | + | - | - | - | - | - |
| Vimentin | ++ | ++ | ++ | +++ | ++ | ++ | +++ | +++ | +++ | +++ |
| CAIX | - | - | - | - | n. a. | - | - | - | - | - |
| CD117 | - | - | - | - | n. a. | n. a. | n. a. | - | - | - |
| EMA | n. a. | - | - | n. a. | n. a. | - | - | - | - | - |
| CK8/18 | n. a. | n. a. | n. a. | n. a. | n. a. | - | - | - | + | + |
| PAX8 | n. a. | n. a. | n. a. | n. a. | + | - | ++ | +++ | ++ | ++ |
| TFE3 | - | ++ | ++ | - | ++ | ++ | ++ | - | - | - |
| P504s | + | ++ | n. a. | n. a. | n. a. | n. a. | n. a. | + | - | + |
| SDHB | ++ | ++ | ++ | ++ | n. a. | n. a. | +++ | +++ | +++ | +++ |
| TFEB | +++ | +++ | ++ | ++ | ++ | ++ | ++ | ++ | +++ | +++ |
| HMB45 | ++ | ++ | + | ++ | ++ | + | ++ | - | ++ | + |
| AE1/AE3 | ++ | ++ | + | + | + | - | + | n. a. | n. a. | + |
| FH | ++ | n. a. | ++ | n. a. | n. a. | n. a. | n. a. | n. a. | n. a. | n. a. |
| PD-L1 | ++ | +++ | ++ | +++ | ++ | +++ | ++ | ++ | ++ | ++ |
| SMA | n. a. | n. a. | n. a. | n. a. | - | - | - | n. a. | n. a. | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, A.-X.; Tian, T.; Liu, L.-B.; Yang, F.; He, H.-Y.; Zhou, L.-Q. TFEB Rearranged Renal Cell Carcinoma: Pathological and Molecular Characterization of 10 Cases, with Novel Clinical Implications: A Single Center 10-Year Experience. Biomedicines 2023, 11, 245. https://doi.org/10.3390/biomedicines11020245
Wang A-X, Tian T, Liu L-B, Yang F, He H-Y, Zhou L-Q. TFEB Rearranged Renal Cell Carcinoma: Pathological and Molecular Characterization of 10 Cases, with Novel Clinical Implications: A Single Center 10-Year Experience. Biomedicines. 2023; 11(2):245. https://doi.org/10.3390/biomedicines11020245
Chicago/Turabian StyleWang, Ai-Xiang, Tai Tian, Li-Bo Liu, Feng Yang, Hui-Ying He, and Li-Qun Zhou. 2023. "TFEB Rearranged Renal Cell Carcinoma: Pathological and Molecular Characterization of 10 Cases, with Novel Clinical Implications: A Single Center 10-Year Experience" Biomedicines 11, no. 2: 245. https://doi.org/10.3390/biomedicines11020245