

Overcoming EGFR Resistance in Metastatic Colorectal Cancer Using Vitamin C: A Review



Department of Internal Medicine, Division of Hematology/Oncology, Naef Khaled Basile Cancer Institute—NKBCI, American University of Beirut Medical Center, Beirut 1107 2020, Lebanon
*
Author to whom correspondence should be addressed.
Biomedicines 2023, 11(3), 678; https://doi.org/10.3390/biomedicines11030678
Submission received: 2 December 2022
/
Revised: 21 December 2022
/
Accepted: 28 December 2022
/
Published: 23 February 2023
(This article belongs to the Special Issue Tumor Microenvironment and Cancer Therapy)
Abstract
:Targeted monoclonal antibody therapy against Epidermal Growth Factor Receptor (EGFR) is a leading treatment modality against metastatic colorectal cancer (mCRC). However, with the emergence of KRAS and BRAF mutations, resistance was inevitable. Cells harboring these mutations overexpress Glucose Transporter 1 (GLUT1) and sodium-dependent vitamin C transporter 2 (SVCT2), which enables intracellular vitamin C transport, leading to reactive oxygen species generation and finally cell death. Therefore, high dose vitamin C is proposed to overcome this resistance. A comprehensive search strategy was adopted using Pubmed and MEDLINE databases (up to 11 August 2022). There are not enough randomized clinical trials to support its use in the clinical management of mCRC, except for a subgroup analysis from a phase III study. High dose vitamin C shows a promising role in overcoming EGFR resistance in mCRC with wild KRAS mutation with resistance to anti-epidermal growth factor inhibitors and in patients with KRAS and BRAF mutations.
Keywords:
vitamin C; ascorbic acid; colorectal cancer; EGFR Resistance; KRAS mutation; BRAF mutation1. Introduction
Colorectal cancer (CRC), one of the most common malignant neoplasms, is the third leading cause of death among all malignancies. Depending on the type of cancer, gender and location, it is ranked 2nd to 4th in terms of incidence in the world [1]. Many efforts have been made with the aim of finding the optimal treatment plan to improve the prognosis of CRC. Specifically, in RAS, BRAF wild and MSS tumors, cytotoxic/cytostatic chemotherapy (5-FU), Vascular Endothelial Growth Factor Inhibitor (VEGF), and Multi-Kinase targeted agents, in addition to targeted monoclonal antibodies (against Epidermal Growth Factor Receptor (EGFR), have been widely used as the leading treatment modality against metastatic CRC (mCRC) [2,3]. Indeed, EGFR targeted therapy was found to increase overall survival by 10–20% in colorectal cancer [4]. However, resistance to this therapy was inevitable with the emergence of KRAS and BRAF mutations, driven by intrinsic and extrinsic mechanisms affecting both cellular pathways and tumor microenvironment, respectively.
Numerous studies have been conducted with the aim to overcome this resistance and improve the prognosis. One of the proposed investigational therapies is high dose vitamin C (intravenous route). Vitamin C, or ascorbic acid, is a water-soluble vitamin essential for humans, though they lack the ability to synthesize it and rely on its intake from diet [5,6]. Its main biologic function revolves around its ability to provide reducing equivalents, and therefore is a cofactor in several reactions that require reduction of iron or copper metalloenzymes. Due to its redox potential and involvement in several cellular processes, vitamin C is being investigated in clinical trials as a treatment modality for several types of cancers. In particular, cells harboring KRAS and BRAF mutations overexpress Glucose Transporter 1 (GLUT1) and sodium-dependent vitamin C transporter 2 (SVCT2), which leads to increased intracellular vitamin C transport, resulting in reactive oxygen species (ROS) generation and finally cell death. Therefore, high dose vitamin C is proposed to overcome resistance to EGFR targeted therapy in BRAF/KRAS mutated CRC. Furthermore, vitamin C exerts its anti-neoplastic effect via different mechanisms; it interferes with anaerobic glycolysis, which is the main metabolic pathway in cancer cells, and also hinders angiogenesis [7,8].
The aim of this review is to summarize the data available on the therapeutic use of high dose vitamin C in metastatic CRC (mCRC), in addition to expanding on its potential use in overcoming anti-EGFR resistance.
2. Methods and Search Strategy
A comprehensive search strategy was adopted using Pubmed and MEDLINE databases (up to 11 August 2022). The MeSH terms used for the search included “Vitamin C”, “Colorectal Neoplasm”, “KRAS mutation”, “EGFR resistance”, and “Ascorbic Acid”. We screened the abstracts to identify relevant articles, and we included basic science studies, clinical trials, and reviews on the topic. In addition, we screened the bibliography of the selected articles to identify important studies that could have been missed in the search. The included studies’ abstracts were checked for their relevance to the research question, and the eligible articles were extensively assessed for inclusion in this work. Additional papers were obtained for the bibliographies of the included studies. A thorough evaluation was conducted on the studies that have been chosen regarding their relation to the topic, results, and outcome.
3. Findings
3.1. Mechanisms of EGFR Resistance in mCRC
Although mCRC is associated with a very poor prognosis, almost half of the patients newly diagnosed with CRC first present in the metastatic phase. Combination chemotherapy has been regarded as the cornerstone for mCRC management [9]. Furthermore, anti-EGFR monoclonal antibodies (mAbs), such as Cetuximab, have proven to be an effective clinical therapy for mCRC patients with wild type KRAS tumors, and prolonged survival for 10–20% of patients [4]. One particular trial (CRYSTAL), revealed that the application of cetuximab and FOLFIRI can increase overall survival (OS) by 8.2 months and reduce the risk of progression by 15% in patients with KRAS wild type mCRC compared to FOLFIRI alone [10]. However, its clinical application is still limited due to high rates of drug resistance, such that treatment benefit has been shown to last only 8–10 months.
Numerous therapeutic strategies have been conducted and investigated to overcome the resistance to anti-EGFR mAbs. However, we must first understand the two mechanisms of resistance.
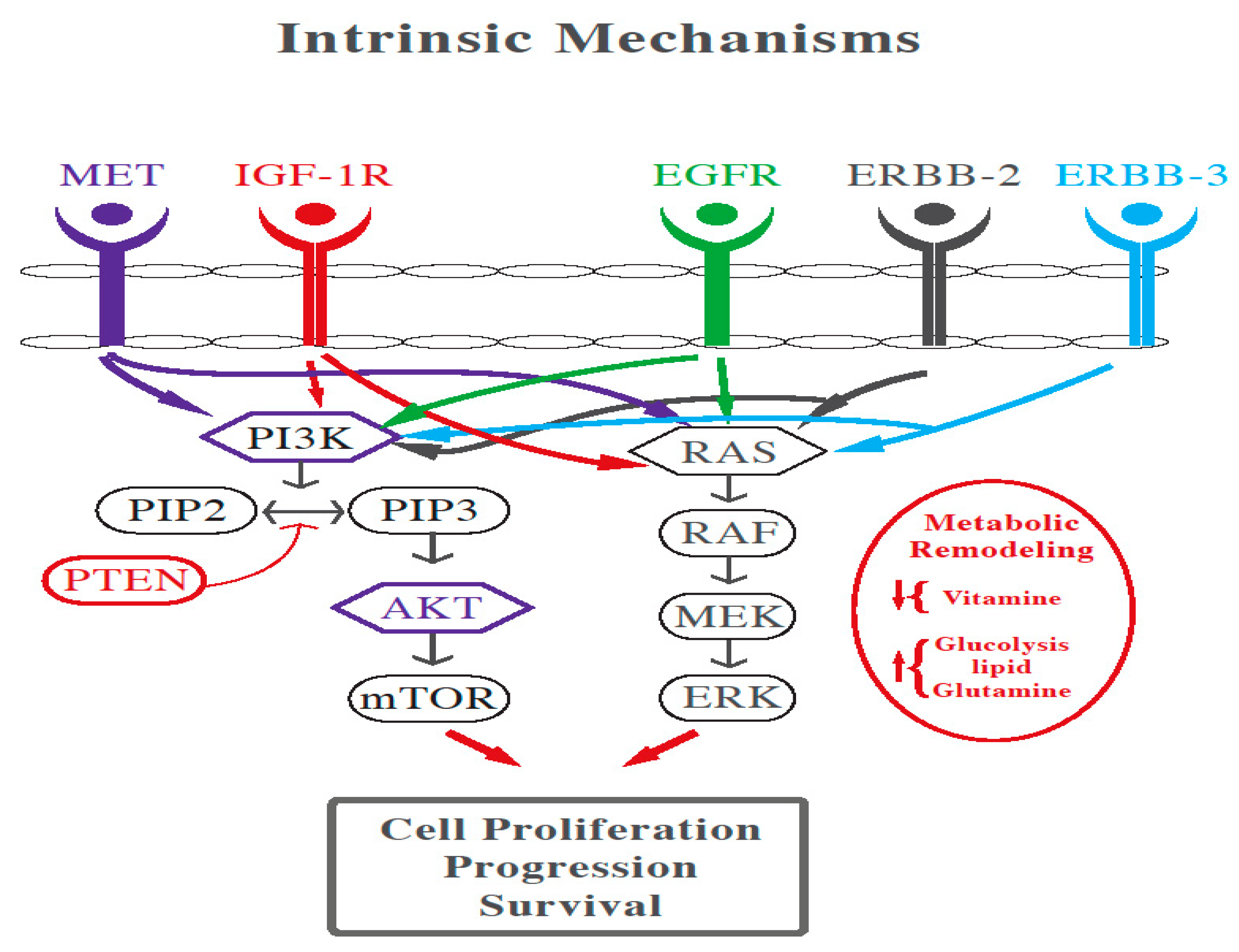
Intrinsic mechanisms include the activation of RAS/RAF/MEK/ERK and PI3K/AKT/mTOR cascades through genomic alterations and protein phosphorylation (as shown in Figure 1). Furthermore, compensatory feedback loop signaling of EGFR is stimulated by ERBB2/MET amplification and abnormal IGF-1R activation. In addition, epithelial-to-mesenchymal transition, glycolysis, lipid synthesis, fatty acid oxidation, and vitamin deficiency are also contributors to resistance [11].
On the other hand, the tumor microenvironment also plays a role in conferring extrinsic resistance to anti-EGFR therapy. This can include dysfunction of natural killer (NK) cells and macrophages that decrease the anti-EGFR antibody-dependent cellular cytotoxicity, and decreased density of effector T-cells and increased PD-L1 expression which assist cancer survival. Other factors leading to drug resistance are cancer-associated fibroblasts secreting mitogenic growth factors that activate RAS or MET pathways, in addition to abnormal angiogenesis [11].
Another aspect leading to acquired resistance in mCRC is caused by the emergence of a heterogeneous resistant population of surviving clones (i.e., persister cells, drug-sensitive RAS/BRAF wild type cells which were not eliminated by anti-EGFR targeted therapies) characterized by a drug tolerant state instigated by prolonged drug exposure, relying on different mechanisms, either genetic or non-genetic [12].
3.2. The Role of High Dose Vitamin C in Cancer
3.2.1. Vitamin C Bioavailability and Requirements
Oral vitamin C produces tissue and plasma concentrations that the body tightly controls [13,14]. Normally, total body content of vitamin C ranges from 300 mg (at near scurvy) to about 2 g [14,15]. Plasma concentration of vitamin C is tightly controlled, and generally does not surpass 100 μM. Roughly, at moderate intakes of 30–180 mg/day, 70–90% of vitamin C is absorbed [15]. However, at doses above 1 g/day, absorption decreases by less than 50% and absorbed ascorbic acid is excreted in the urine [14,16]. However, when vitamin C is administered by IV route, it bypasses the gastrointestinal regulation and attains a dose-dependent plasma concentration. Nonetheless, its half-life is less than 2 h [17].
3.2.2. High Dose Vitamin C in Cancer Clinical Trials
In 1979, Cameron, Pauling et al., showcased that patients with terminal cancer treated with high pharmacological doses of vitamin C (10 g/day by IV infusion for about 10 days and orally thereafter) had significantly prolonged survival rates and improved quality of life compared to matched controls that did not receive vitamin C [18]. In a randomized double-blinded placebo control study conducted at Mayo Clinic, high dose oral vitamin C did not replicate this favorable response in advanced cancer [19,20]. One possible explanation is that oral vitamin C does not achieve the required plasma concentration to exert an anti-cancer effect, unlike IV. Indeed, orally administered vitamin C achieves maximum plasma concentrations of no more than 220 μmol/L of blood, while high-dose IV vitamin C generates plasma concentrations up into the millimolar range (≥15 mmol/L), leading to different outcomes [16,21,22]. Yeom et al., evaluated the quality of life of 39 terminal cancer patients who received high dose vitamin C (10 g twice by IV and 4 g oral daily intake for a week). Patients reported significant improvement on the functional scale in terms of physical, role, emotional, and cognitive function, in addition to significant lower scores for fatigue, nausea/vomiting, pain, and loss of appetite [23]. Similar results were also found in other trials where high dose vitamin C was found to ameliorate quality of life for patients with terminal cancer on palliative care [24,25,26,27].
In addition, several clinical trials were conducted to test the safety of high dose vitamin C as monotherapy or in combination with other chemotherapeutic agents, as well as to determine the maximal tolerable dose that could be used in phase II and III trials. For instance, Wang et al., administered vitamin C with FOLFOX or FOLFIRI with or without bevacizumab to patients with colorectal or gastric cancer. The study reported no drug limiting toxicity and showed decreased hematological and gastrointestinal toxicities compared to other trials employing the same chemotherapy regimens for these two cancers [28,29,30,31,32]. Monti et al., administered vitamin C to 14 stage IV patients with pancreatic cancer receiving gemcitabine and erlotinib. In this study, eight patients had a decrease in the tumor size, seven had a stable disease and two had disease progression, although progression free survival and overall survival were comparable to those on gemcitabine/erlotinib alone [33]. In two other studies also on pancreatic cancer, vitamin C was found to decrease the rate of severe toxicity in patients receiving gemcitabine 500 mg/m, irinotecan 80 mg/m, leucovorin 300 mg, 5-fluorouracil (5-FU) 400 mg/m, and gemcitabine monotherapy [34,35]. Additional studies investigating the efficacy of vitamin C in advanced cancers did not show objective tumor response [26,27]. With respect to toxicity, mild side effects were recorded in some trials, mainly due to the osmotic load of the vitamin C infusion, and were reversible with adequate hydration [26,33], and one study reported kidney stone formation and hypokalemia as possibly related to vitamin C [36]. More severe side effects in these trials were related to the administration of chemotherapy. Furthermore, caution should be made in patients with G6PD deficiency, as high dose vitamin C can induce hemolysis, and patients should be screened before administration of IV vitamin C [37]. Results from several studies demonstrated that the optimal dose of IV vitamin C that could be adopted in phase II trials was 1.5 g/kg or 70 to 80 g/m2 [32].
3.2.3. Role of Vitamin C in KRAS and BRAF Mutated Colorectal Cancer
RAS mutations are present in around 40% of mCRC, while BRAF mutations account for 10% [38]. Both mutations have been used as predictors of resistance to EGFR targeting drugs. In fact, testing for these mutations on tissue specimen of mCRC patients before the initiation of anti-EGFR therapy has become mandatory, particularly since resistance may be present originally or even may develop during the treatment in initially wild type patients; a phenomenon known as acquired (or secondary) resistance [39]. In order to identify these mutations, tissue and liquid biopsy method can be used as an analytical technique to detect tumor-derived biomarkers in body fluids such as circulating tumor DNA (ctDNA) [40]. Indeed, the detection of ctDNA released by cancer cells provides valuable information in relation to the prognosis and prediction of therapeutic resistance or sensitivity. Undeniably, improving detection of KRAS/BRAF mutations at different time points, enhancing correlation between its levels and survival and monitoring its response to therapy.
Furthermore, KRAS and BRAF mutations correlate with GLUT1 overexpression by cancer cells and excessive dependence on aerobic glycolysis as an energy source [41]. Aerobic glycolysis, also known as the Warburg effect, is a hallmark of cancer, in which glucose is converted to lactate despite the availability of oxygen. This is because pyruvate, the end product of glycolysis, is diverted from the mitochondria as a result of transcriptional activation of pyruvate dehydrogenase kinase 1, which in turn inactivates pyruvate dehydrogenase. As a result, the conversion of pyruvate to acetyl-CoA is hindered, and pyruvate is diverted into the cytosol where it is converted to lactate [42]. Although the shift from oxidative phosphorylation to aerobic glycolysis may seem to generate less energy per mol of glucose, the latter process is around 10 to 100 times faster and thus generates more ATP per unit time compared to oxidative phosphorylation [43,44]. Even though aerobic glycolysis is not exclusive to cancer cells and occurs in normal rapidly growing cells [45,46], its activation is enhanced and sustained in cancer cells because of activation of oncogenes and loss of tumor suppressor genes [43]. In addition, aerobic glycolysis sustains the production of metabolic intermediates (carbon moieties) for the synthesis of cellular components of the growing tumor [15], producing reducing equivalents when these intermediates are shunted into the pentose phosphate pathway (PPP) and reducing the production of reactive oxygen species (ROS), which enhances cellular proliferation [14]. Finally, the accumulation of lactic acid renders the tumor microenvironment more acidic, which in turn drives genetic instability, favors tumor invasion, cell motility, epithelial-to-mesenchymal transition, metastasis, resistance to apoptosis, immune evasion, and enhances angiogenesis [13,14].
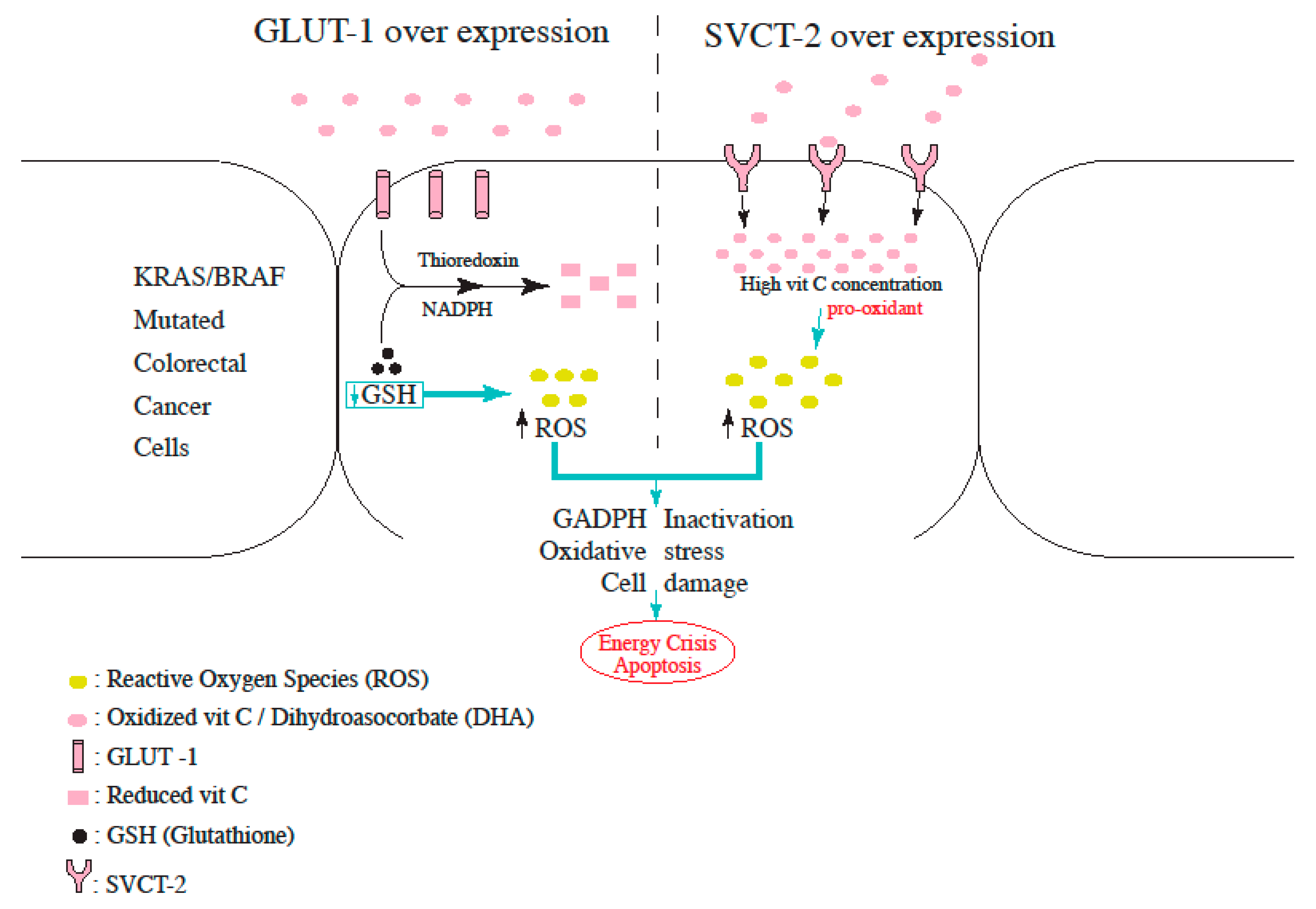
Therefore, targeting this rewired glucose metabolism can be an effective therapeutic option for KRAS and BRAF-mutant CRC. GLUT1 and GLUT3 transport the oxidized form of vitamin C, dehydroascorbate (DHA) into the cells, where it is reduced back to vitamin C at the expense of glutathione (GSH), thioredoxin, and NADPH. In their study, Yun et al., demonstrated that DHA transport was increased in KRAS and BRAF-mutant cells, and this was mediated by GLUT1 overexpression. The rapid uptake of DHA and its intra-cellular reduction to vitamin C depletes the reserves of glutathione, leading to ROS accumulation and GADPH inactivation (as shown in Figure 2). The end result is an energy crisis and apoptosis in KRAS and BRAF mutated cells, which is not observed in wild-type CRC cells [42]. Aguilera et al., also demonstrated the vitamin C induced disruption of the Warburg metabolism in KRAS mutant CRC cells. Intracellular vitamin C causes detachment of RAS from the plasma membrane, thereby blocking the phosphorylation of PKM2 (pyruvate kinase M2), leading to downregulation of GLUT-1 expression [43,44].
In a study conducted by Jung et al., L-ascorbic acid induced cell death when partnered with cetuximab. This was mainly demonstrated in human colon cancer cells with a mutant KRAS gene, influenced by sodium-dependent vitamin C transporter 2 (SVCT-2) with administration of daily doses of 10 g of L-ascorbic acid for 6 h. Specifically, the knockdown of endogenous SVCT-2 induced resistance to L-ascorbic acid treatment in SVCT-2-positive cells, whereas ectopic expression of SVCT-2 induced sensitivity to L-ascorbic acid treatment in human CRCs that do not express SVCT-2 [45]. In addition, differences in SVCT-2 expression revealed a clear correlation with sensitivities to cetuximab and L-ascorbic acid (as shown in Figure 2). Particularly, recent studies that showed flow of L-ascorbic acid into the cell via SVCT-2 but not SVCT-1 support these findings. Taken together, these outcomes suggest that SVCT-2 expression may enable bypassing resistance to cetuximab in human colon cancer patients with a mutant KRAS by L-ascorbic acid.
Another approach to overcoming secondary resistance to EGFR blockade is targeting cellular proliferation axes with a variety of drugs. At first, MAPK signaling pathway was assessed; particularly over the past 30 years, research has proven that it plays a crucial role in initiating a wide range of cellular responses (proliferation, migration, differentiation, and apoptosis) by converting extracellular stimuli [46]. However, since no significant changes were noted when evaluating the MAPK signaling pathway upon the addition of cetuximab, focus was shifted towards changes in the RAF-MEK-ERK pathway after L-ascorbic acid exposure. Remarkably, decreased phospho-MEK, phospho-ERK, phospho-BRAF, and phospho-CRAF were noted when both drugs were used in the treatment [45], all of which are known to be key molecules for EGFR resistance in mutant KRAS human CRC cells expressing SVCT-2.
CRAF has been known to bind to ASK-1, suppressing its pro-apoptotic activity. According to their study, Jung et al., revealed that activation of ASK-1 and p38 pathway was induced by L-ascorbic acid and cetuximab in SVCT-2 expressing cells [47]. These findings suggest that SVCT-2-dependent reactive oxygen species production induces the activation of the ASK-1 p38 pathway, modulating cellular apoptosis. Changes in these signaling molecules were observed only in the tissues from the mutant KRAS and SVCT-2-positive human colon cancer cell line SW620 but not in tissues from the mutant KRAS and SVCT-2-negative cell line HCT116.
While long-term and larger studies are still lacking, available data supports the notion that L-ascorbic acid overcomes resistance to cetuximab by initiating the ASK-1-mediated apoptosis pathway through the blockade of the MAPK signaling pathway.
Although not enough clinical evidence favors the use of high dose vitamin C in KRAS or BRAF mutated CRC, data from a phase III clinical trial revealed promising results. A total of 442 patients were assigned to receive either chemotherapy (control group) or chemotherapy plus high-dose IV vitamin C 1.5 g/kg/day on day 1–3 (experimental group) and were followed up for 24.5 months [48]. PFS, ORR, and OS were similar between the control and experimental group. At first, results revealed that chemotherapy alone yielded a superior PFS when compared to chemotherapy plus high dose vitamin C. However, the prespecified subgroup analysis of patients with RAS mutation showed improved PFS in the experimental group only in patients with mCRC and KRAS mutation (9.2 vs. 7.8 months, HR 0.67; 95% CI, 0.50–0.91; p = 0.01). Finally, treatment related adverse effect of grade 3 or higher occurred in 33.5% of the patients in the experimental group, as compared with 30.3% in the control group [48]. Table 1 showcases the results of various trials using vitamin C as treatment.
4. Conclusions
Despite the lack of robust supportive trials, high dose vitamin C shows a promising role in overcoming EGFR resistance in mCRC with wild KRAS mutation with resistance to anti-epidermal growth factor inhibitors and in patients with KRAS and BRAF mutations; specifically with mutant cells overexpressing GLUT1 and SVCT2, both of which enable intracellular vitamin C transport, leading to reactive oxygen species generation and finally cell death.
Furthermore, while this experiment measured vitamin C efficiency, additional larger prospective trials are required to consolidate this finding and gain more insight on anti-EGFR resistance mechanisms; to investigate, for instance, development of effective therapies, with promising second-generation antibodies and combinations with MET signaling pathway, or MEK inhibitors and pan-ERBB.
Author Contributions
Conceptualization, A.S., A.M., L.C. and S.T.; methodology, A.S., A.M., L.C. and S.T.; validation, A.S., A.M., L.C. and S.T.; formal analysis, A.S., A.M., L.C. and S.T.; investigation, A.S., A.M., L.C. and S.T.; data curation A.S., A.M. and L.C.; writing—original draft preparation A.M and L.C.; writing—review and editing A.M., L.C.; supervision A.S. and S.T.; project administration A.S.; All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Przybyłowicz, K.E. A Review of Colorectal Cancer in Terms of Epidemiology, Risk Factors, Development, Symptoms and Diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef]
- Biller, L.H.; Schrag, D. Diagnosis and Treatment of Metastatic Colorectal Cancer: A Review. JAMA 2021, 325, 669–685. [Google Scholar] [CrossRef]
- Böttger, F.; Vallés-Martí, A.; Cahn, L.; Jimenez, C.R. High-dose intravenous vitamin C, a promising multi-targeting agent in the treatment of cancer. J. Exp. Clin. Cancer Res. CR 2021, 40, 343. [Google Scholar] [CrossRef]
- Yuan, M.; Wang, Z.; Lv, W.; Pan, H. The Role of Anti-EGFR Monoclonal Antibody in mCRC Maintenance Therapy. Front. Mol. Biosci. 2022, 9, 870395. [Google Scholar] [CrossRef]
- Padayatty, S.J.; Levine, M. Vitamin C: The known and the unknown and Goldilocks. Oral Dis. 2016, 22, 463–493. [Google Scholar] [CrossRef]
- Ngo, B.; Van Riper, J.M.; Cantley, L.C. Targeting cancer vulnerabilities with high-dose vitamin C. Nat. Rev. Cancer 2019, 19, 271–282. [Google Scholar] [CrossRef]
- El Halabi, I.; Bejjany, R.; Nasr, R.; Mukherji, D.; Temraz, S.; Nassar, F.J.; El Darsa, H.; Shamseddine, A. Ascorbic Acid in Colon Cancer: From the Basic to the Clinical Applications. Int. J. Mol. Sci. 2018, 19, 2752. [Google Scholar] [CrossRef]
- Dachs, G.U.; Gandhi, J.; Wohlrab, C.; Carr, A.C.; Morrin, H.R.; Pullar, J.M.; Bayer, S.B.; Eglinton, T.W.; Robinson, B.A.; Vissers, M.C.M. Vitamin C Administration by Intravenous Infusion Increases Tumor Ascorbate Content in Patients With Colon Cancer: A Clinical Intervention Study. Front. Oncol. 2021, 10, 600715. [Google Scholar] [CrossRef]
- Arrington, A.K.; Heinrich, E.L.; Lee, W.; Duldulao, M.; Patel, S.; Sanchez, J.; Garcia-Aguilar, J.; Kim, J. Prognostic and Predictive Roles of KRAS Mutation in Colorectal Cancer. Int. J. Mol. Sci. 2012, 13, 12153–12168. [Google Scholar] [CrossRef]
- Zhou, J.; Ji, Q.; Li, Q. Resistance to anti-EGFR therapies in metastatic colorectal cancer: Underlying mechanisms and reversal strategies. J. Exp. Clin. Cancer Res. 2021, 40, 328. [Google Scholar] [CrossRef]
- Lorenzato, A.; Magrì, A.; Matafora, V.; Audrito, V.; Arcella, P.; Lazzari, L.; Montone, M.; Lamba, S.; Deaglio, S.; Siena, S.; et al. Vitamin C Restricts the Emergence of Acquired Resistance to EGFR-Targeted Therapies in Colorectal Cancer. Cancers 2020, 12, 685. [Google Scholar] [CrossRef]
- Frei, B.; England, L.; Ames, B.N. Ascorbate is an outstanding antioxidant in human blood plasma. Proc. Natl. Acad. Sci. USA 1989, 86, 6377–6381. [Google Scholar] [CrossRef]
- Jacob, R.A.; Sotoudeh, G. Vitamin C function and status in chronic disease. Nutr. Clin. Care Off. Publ. Tufts Univ. 2002, 5, 66–74. [Google Scholar] [CrossRef]
- German Nutrition Society. New Reference Values for Vitamin C Intake. Ann. Nutr. Metab. 2015, 67, 13–20. [Google Scholar] [CrossRef]
- Padayatty, S.J.; Sun, H.; Wang, Y.; Riordan, H.D.; Hewitt, S.M.; Katz, A.; Wesley, R.A.; Levine, M. Vitamin C pharmacokinetics: Implications for oral and intravenous use. Ann. Intern. Med. 2004, 140, 533–537. [Google Scholar] [CrossRef]
- Cameron, E.; Pauling, L. Supplemental ascorbate in the supportive treatment of cancer: Prolongation of survival times in terminal human cancer. Proc. Natl. Acad. Sci. USA 1976, 73, 3685–3689. [Google Scholar] [CrossRef]
- Creagan, E.T.; Moertel, C.G.; O’Fallon, J.R.; Schutt, A.J.; O’Connell, M.J.; Rubin, J.; Frytak, S. Failure of high-dose vitamin C (ascorbic acid) therapy to benefit patients with advanced cancer. A controlled trial. N. Engl. J. Med. 1979, 301, 687–690. [Google Scholar] [CrossRef]
- Moertel, C.G.; Fleming, T.R.; Creagan, E.T.; Rubin, J.; O’Connell, M.J.; Ames, M.M. High-dose vitamin C versus placebo in the treatment of patients with advanced cancer who have had no prior chemotherapy. A randomized double-blind comparison. N. Engl. J. Med. 1985, 312, 137–141. [Google Scholar] [CrossRef]
- Hoffer, L.J.; Levine, M.; Assouline, S.; Melnychuk, D.; Padayatty, S.J.; Rosadiuk, K.; Rousseau, C.; Robitaille, L.; Miller, W.H., Jr. Phase I clinical trial of i.v. ascorbic acid in advanced malignancy. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2008, 19, 1969–1974. [Google Scholar] [CrossRef]
- Stephenson, C.M.; Levin, R.D.; Spector, T.; Lis, C.G. Phase I clinical trial to evaluate the safety, tolerability, and pharmacokinetics of high-dose intravenous ascorbic acid in patients with advanced cancer. Cancer Chemother. Pharmacol. 2013, 72, 139–146. [Google Scholar] [CrossRef]
- Yeom, C.H.; Jung, G.C.; Song, K.J. Changes of terminal cancer patients’ health-related quality of life after high dose vitamin C administration. J. Korean Med. Sci. 2007, 22, 7–11. [Google Scholar] [CrossRef]
- Mansoor, F.; Kumar, S.; Rai, P.; Anees, F.; Kaur, N.; Devi, A.; Kumar, B.; Memon, M.K.; Khan, S. Impact of Intravenous Vitamin C Administration in Reducing Severity of Symptoms in Breast Cancer Patients During Treatment. Cureus 2021, 13, e14867. [Google Scholar] [CrossRef]
- Günes-Bayir, A.; Kiziltan, H.S. Palliative Vitamin C Application in Patients with Radiotherapy-Resistant Bone Metastases: A Retrospective Study. Nutr. Cancer 2015, 67, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Vollbracht, C.; Schneider, B.; Leendert, V.; Weiss, G.; Auerbach, L.; Beuth, J. Intravenous vitamin C administration improves quality of life in breast cancer patients during chemo-/radiotherapy and aftercare: Results of a retrospective, multicentre, epidemiological cohort study in Germany. In Vivo 2011, 25, 983–990. [Google Scholar]
- Wang, F.; He, M.-M.; Wang, Z.-X.; Li, S.; Jin, Y.; Ren, C.; Shi, S.-M.; Bi, B.-T.; Chen, S.-Z.; Lv, Z.-D. Phase I study of high-dose ascorbic acid with mFOLFOX6 or FOLFIRI in patients with metastatic colorectal cancer or gastric cancer. BMC Cancer 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Monti, D.A.; Mitchell, E.; Bazzan, A.J.; Littman, S.; Zabrecky, G.; Yeo, C.J.; Pillai, M.V.; Newberg, A.B.; Deshmukh, S.; Levine, M. Phase I Evaluation of Intravenous Ascorbic Acid in Combination with Gemcitabine and Erlotinib in Patients with Metastatic Pancreatic Cancer. PLoS ONE 2012, 7, e29794. [Google Scholar] [CrossRef]
- Bruckner, H.; Hirschfeld, A.; Gurell, D.; Lee, K. Broad safety impact of high-dose ascorbic acid and induction chemotherapy for high-risk pancreatic cancer. J. Clin. Oncol. 2017, 35, e15711. [Google Scholar] [CrossRef]
- Welsh, J.L.; Wagner, B.A.; Van’t Erve, T.J.; Zehr, P.S.; Berg, D.J.; Halfdanarson, T.R.; Yee, N.S.; Bodeker, K.L.; Du, J.; Roberts, L.J., 2nd; et al. Pharmacological ascorbate with gemcitabine for the control of metastatic and node-positive pancreatic cancer (PACMAN): Results from a phase I clinical trial. Cancer Chemother. Pharmacol. 2013, 71, 765–775. [Google Scholar] [CrossRef]
- Riordan, H.D.; Casciari, J.J.; González, M.J.; Riordan, N.H.; Miranda-Massari, J.R.; Taylor, P.; Jackson, J.A. A pilot clinical study of continuous intravenous ascorbate in terminal cancer patients. Puerto Rico Health Sci. J. 2005, 24, 269–276. [Google Scholar]
- Cho, S.; Chae, J.S.; Shin, H.; Shin, Y.; Song, H.; Kim, Y.; Yoo, B.C.; Roh, K.; Cho, S.; Kil, E.J.; et al. Hormetic dose response to (L)-ascorbic acid as an anti-cancer drug in colorectal cancer cell lines according to SVCT-2 expression. Sci. Rep. 2018, 8, 11372. [Google Scholar] [CrossRef]
- Vitiello, P.P.; De Falco, V.; Giunta, E.F.; Ciardiello, D.; Cardone, C.; Vitale, P.; Zanaletti, N.; Borrelli, C.; Poliero, L.; Terminiello, M.; et al. Clinical Practice Use of Liquid Biopsy to Identify RAS/BRAF Mutations in Patients with Metastatic Colorectal Cancer (mCRC): A Single Institution Experience. Cancers 2019, 11, 1504. [Google Scholar] [CrossRef]
- Michela, B. Liquid Biopsy: A Family of Possible Diagnostic Tools. Diagnostics 2021, 11, 1391. [Google Scholar] [CrossRef]
- Hirahata, T.; Ul Quraish, R. Liquid Biopsy: A Distinctive Approach to the Diagnosis and Prognosis of Cancer. Cancer Inform. 2022, 21, 11769351221076062. [Google Scholar] [CrossRef]
- Vissers, M.C.M.; Gunningham, S.P.; Morrison, M.J.; Dachs, G.U.; Currie, M.J. Modulation of hypoxia-inducible factor-1 alpha in cultured primary cells by intracellular ascorbate. Free. Radic. Biol. Med. 2007, 42, 765–772. [Google Scholar] [CrossRef]
- Campbell, E.J.; Vissers, M.C.M.; Wohlrab, C.; Hicks, K.O.; Strother, R.M.; Bozonet, S.M.; Robinson, B.A.; Dachs, G.U. Pharmacokinetic and anti-cancer properties of high dose ascorbate in solid tumours of ascorbate-dependent mice. Free. Radic. Biol. Med. 2016, 99, 451–462. [Google Scholar] [CrossRef]
- Vaupel, P.; Schmidberger, H.; Mayer, A. The Warburg effect: Essential part of metabolic reprogramming and central contributor to cancer progression. Int. J. Radiat. Biol. 2019, 95, 912–919. [Google Scholar] [CrossRef]
- Vaupel, P.; Multhoff, G. Revisiting the Warburg effect: Historical dogma versus current understanding. J. Physiol. 2021, 599, 1745–1757. [Google Scholar] [CrossRef]
- Liberti, M.V.; Locasale, J.W. The Warburg Effect: How Does it Benefit Cancer Cells? Trends Biochem. Sci. 2016, 41, 211–218. [Google Scholar] [CrossRef]
- Denko, N.C. Hypoxia, HIF1 and glucose metabolism in the solid tumour. Nat. Rev. Cancer 2008, 8, 705–713. [Google Scholar] [CrossRef]
- De Grooth, H.J.; Manubulu-Choo, W.P.; Zandvliet, A.S.; Spoelstra-de Man, A.M.E.; Girbes, A.R.; Swart, E.L.; Oudemans-van Straaten, H.M. Vitamin C Pharmacokinetics in Critically Ill Patients: A Randomized Trial of Four IV Regimens. Chest 2018, 153, 1368–1377. [Google Scholar] [CrossRef]
- Gaianigo, N.; Melisi, D.; Carbone, C. EMT and Treatment Resistance in Pancreatic Cancer. Cancers 2017, 9, 122. [Google Scholar] [CrossRef]
- Yun, J.; Mullarky, E.; Lu, C.; Bosch, K.N.; Kavalier, A.; Rivera, K.; Roper, J.; Chio, I.I.C.; Giannopoulou, E.G.; Rago, C.; et al. Vitamin C selectively kills KRAS and BRAF mutant colorectal cancer cells by targeting GAPDH. Science 2015, 350, 1391–1396. [Google Scholar] [CrossRef]
- Aguilera, O.; Muñoz-Sagastibelza, M.; Torrejón, B.; Borrero-Palacios, A.; del Puerto-Nevado, L.; Martínez-Useros, J.; Rodriguez-Remirez, M.; Zazo, S.; García, E.; Fraga, M.; et al. Vitamin C uncouples the Warburg metabolic switch in KRAS mutant colon cancer. Oncotarget 2016, 7, 47954–47965. [Google Scholar] [CrossRef]
- Linardou, H.; Dahabreh, I.J.; Kanaloupiti, D.; Siannis, F.; Bafaloukos, D.; Kosmidis, P.; Papadimitriou, C.A.; Murray, S. Assessment of somatic k-RAS mutations as a mechanism associated with resistance to EGFR-targeted agents: A systematic review and meta-analysis of studies in advanced non-small-cell lung cancer and metastatic colorectal cancer. Lancet Oncol. 2008, 9, 962–972. [Google Scholar] [CrossRef]
- Jung, S.-A.; Lee, D.-H.; Moon, J.-H.; Hong, S.-W.; Shin, J.-S.; Hwang, I.Y.; Shin, Y.J.; Kim, J.H.; Gong, E.-Y.; Kim, S.-M.; et al. L-Ascorbic acid can abrogate SVCT-2-dependent cetuximab resistance mediated by mutant KRAS in human colon cancer cells. Free. Radic. Biol. Med. 2016, 95, 200–208. [Google Scholar] [CrossRef]
- Yue, J.; López, J.M. Understanding MAPK Signaling Pathways in Apoptosis. Int. J. Mol. Sci. 2020, 21, 2346. [Google Scholar] [CrossRef]
- Temraz, S.; Mukherji, D.; Shamseddine, A. Dual Inhibition of MEK and PI3K Pathway in KRAS and BRAF Mutated Colorectal Cancers. Int. J. Mol. Sci. 2015, 16, 22976–22988. [Google Scholar] [CrossRef]
- Wang, F.; Xiao, J.; Zhang, Y.; Yuan, X.; He, M.; Fang, W.; Zhang, Y.; Wang, W.; Hu, X.; Ma, Z.; et al. SO-17 A randomized, open-label, multicenter, phase III study of high-dose vitamin C plus FOLFOX +/− bevacizumab versus FOLFOX +/− bevacizumab as first-line treatment in patients with unresectable metastatic colorectal cancer. Ann. Oncol. 2022, 33, S364. [Google Scholar] [CrossRef]
- Sartore-Bianchi, A.; Pietrantonio, F.; Lonardi, S.; Mussolin, B.; Rua, F.; Crisafulli, G.; Bartolini, A.; Fenocchio, E.; Amatu, A.; Manca, P.; et al. Circulating tumor DNA to guide rechallenge with panitumumab in metastatic colorectal cancer: The phase 2 CHRONOS trial. Nat Med. 2022, 28, 1612–1618. [Google Scholar] [CrossRef]
Figure 1.
Cross talk between MAPK, PI3K, and Wnt pathway in CRC.

Figure 2.
Proposed mechanism for increased ROS production in L-Ascorbic Acid-treated cells overexpressing either GLUT-1 or SVCT-2.
Figure 2.
Proposed mechanism for increased ROS production in L-Ascorbic Acid-treated cells overexpressing either GLUT-1 or SVCT-2.

{kind=link}
{kind=link}
Table 1.
Results of various trials using vitamin C as treatment.
| Study | Design and Population | Aim | Intervention | Results | Notes |
|---|---|---|---|---|---|
| Wang (2019) NCT02969681 [25] | -Phase I open label single center dose escalation speed expansion -30 mCRC and 6 mGC | Determine maximum tolerated dose of AA w/mFOLFOX or FOLFIRI +/− bevacizumab | Part 1 (dose escalation): AA (0.4, 0.6, 0.8, 1, 1.2 and 1.5 g/kg) on days 1 to 3 of FOLFOX or FOLFIRI every 14 d. Part 2 (dose expansion): AA given 1.5 g/kg or MTD on days 1 to 3. Tx duration: 12 cycles or progression or side effects. | No DLT in part 1 or part 2 and MTD not reached → 1.5 g/kg chosen as RP2D. Disease control rate 95.5%. No difference in efficacy between wt and m KRAS/BRAF CRC. Median PFS of the entire cohort 8.8 m. | The current study showed markedly decreased all-grade and grade ≥ 3 bone marrow and gastrointestinal toxic effects compared with previous trials investigating the same chemotherapeutic regimens in mCRC or mGC. |
| Monti 2012 [26] | -Phase I open label dose escalation -A total of 14 stage IV pancreatic cancer patients receiving gemcitabine and erlotinib (not previously treated) | Primary: safety Secondary: response to tx | First cohort received 50 g IV AA per infusion, second cohort received 75 g/infusion, and third cohort received 100 g/infusion. A cycle consisted of three infusions per week performed on separate days, for 8 weeks. | A total of 9 patients completed the study. Side effects: mild headache and nausea from osmotic load that resolve; 8 serious adverse events recorded but related to gemcitabine/disease progression; 8 patients had dec in tumor size, 7 patients had stable disease, and 2 progressed. | Med PFS 89 days and med OS 182 d (comparable to gem/erlo alone). |
| Bruckner 2017 (abstract) [27] | -Phase II trial, open label -A total of 26 patients with advanced pancreatic cancer | High dose AA (75–100 g) 1–2 x/week with GFLIP Q2w until progression. | Decreased rate of severe toxicity. | ||
| Welsh (2013) [28] | -Phase I single institution, prospective, open label -A total of 9 patients with stage IV pancreatic cancer receiving gemcitabine | Safety and tolerability of AA with gemcitabine | Twice weekly (50–125 g) IV AA and concurrent gemcitabine until DLT or progression. Target peak AA level > 350 mg/dl. | A total of 6/9 patients maintained/improved PS. PFS 26 +/− 7 weeks and OS 12 m. Adverse events related to AA were rare and included diarrhea and dry mouth. Adverse events were less severe when compared to published data for gemcitabine alone. | |
| Stephenson [20] | -Phase I, single center, non-comparative dose escalation -A total of 17 patients with advanced cancers not responsive to standard tx | Safety and tolerability of pharmacokinetics of high dose IV AA as monotherapy in advanced tumors | A total of 5 cohorts of 3 patients receiving dose escalation (30 g/m2 and inc by 20) until MTD | No objective tumor response. Side effects were mild and possibly related to treatment. Some patients had improved qol score at 3 and 4 weeks. | Dose of 70 to 80 g/m2 appears to be optimal for future studies. |
| Hoffer (2008) [19] | -Phase I, single center, dose escalating. -A total of 24 patients with advanced cancers, pretreated. They did not receive chemo with AA. | Document the safety and clinical consequences of i.v. ascorbic acid administrated in a dose sufficient to sustain plasma ascorbic acid concentrations >10 mmol/l for several hours | Cohorts receiving fixed doses of 0.4, 0.6, 0.9, and 1.5 g/kg for 4 weeks cycle | Mild clinical toxicity occurred, all consistent with the SE attending the rapid infusion of any high-osmolarity solution. Preventable by encouraging patients to drink fluids. No objective tumor response, but 2 patients in the 0.6 group had stable disease. AA could be promising when combined with cytotoxic agents. | 1.5 g/kg (infused > 90–120 min 3 x/w) was adopted as the recommend dose for future phase II trials |
| Riordan [29] | -Pilot study -24 late stage terminal cancer patients | Clinical safety of high dose AA | Continuous infusions of 150 to 710 mg/kg/day for up to eight weeks | Most SE were mild and 2 were grade 3 possibly related to AA: kidney stone and hypoK. One patient had stable disease and continued the treatment for 48 weeks. AA is relatively safe, provided the patient does not have a history of kidney stone. | |
| Sartore-Bianchi (2022) [49] | -Open-label, single-arm phase 2 clinical trial -A total of 52 patients with tissue-RAS WT tumors after a previous treatment with anti-EGFR-based regimens underwent an interventional ctDNA-based screening. | Exploiting blood-based identification of RAS/BRAF/EGFR mutations levels to tailor a chemotherapy-free anti-EGFR rechallenge with panitumumab | A total of 36 patients were molecularly eligible for panitumumab rechallenge. Of these, 27 received the drug as per trial protocol, 6 did not meet clinical inclusion criteria, and 3 were treated otherwise as per physician choice | Of 27 enrolled patients, 8 (30%) achieved partial response and 17 (63%) disease control, including 2 unconfirmed responses. These clinical results favorably compare with standard third-line treatments and show that interventional liquid biopsies can be effectively and safely exploited in a timely manner to guide anti-EGFR rechallenge therapy with panitumumab in patients with mCRC. | |
| Wang (2022) [48] | -Randomized, open labeled, multicenter phase II -A total of 442 histologically confirmed mCRC patients with normal glucose-6-phosphate dehydrogenase status and no prior treatment for metastatic disease | Compare the efficacy and safety of high-dose vitamin C plus FOLFOX +/− bevacizumab versus FOLFOX +/− bevacizumab as first-line treatment in patients with metastatic colorectal cancer (mCRC) | A total of 442 patients were randomized into a control (FOLFOX +/− bevacizumab) and an experimental (high-dose vitamin C (1.5 g/kg/d, intravenously for 3 h from D1 to D3) plus FOLFOX +/− bevacizumab) group | In prespecified subgroup analyses, patients with RAS mutation had significantly longer Progression Free Survival (median PFS, 9.2 vs. 7.8 months; HR, 0.67; 95% CI, 0.50–0.91; p = 0.01) with vitamin C added to chemotherapy than with chemotherapy only. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Machmouchi, A.; Chehade, L.; Temraz, S.; Shamseddine, A. Overcoming EGFR Resistance in Metastatic Colorectal Cancer Using Vitamin C: A Review. Biomedicines 2023, 11, 678. https://doi.org/10.3390/biomedicines11030678
AMA Style
Machmouchi A, Chehade L, Temraz S, Shamseddine A. Overcoming EGFR Resistance in Metastatic Colorectal Cancer Using Vitamin C: A Review. Biomedicines. 2023; 11(3):678. https://doi.org/10.3390/biomedicines11030678
Chicago/Turabian StyleMachmouchi, Ahmad, Laudy Chehade, Sally Temraz, and Ali Shamseddine. 2023. "Overcoming EGFR Resistance in Metastatic Colorectal Cancer Using Vitamin C: A Review" Biomedicines 11, no. 3: 678. https://doi.org/10.3390/biomedicines11030678
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.