
Patient Blood Management in Liver Transplant—A Concise Review
 , ,
, ,
Abstract
:1. Introduction
2. Coagulopathy in Liver Disease
3. The Importance of Limiting Transfusion in Liver Transplants (Table 1)
3.1. Fresh Frozen Plasma
3.2. Platelets
3.3. Red Blood Cells (RBC)

{kind=link}
{kind=link}
{kind=link}
| Blood Product | Complications | References |
|---|---|---|
| Plasma-Containing Blood Components (platelets, FFP) | Graft loss Reduced post-transplant survival TACO (with increased portal hypertension and bleeding) TRALI | [33,34,35] |
| Platelets | Most associated with increased morbidity and mortality, TRALI | [43,44,45,46,47] |
| RBC | Artery thrombosis Early surgical reintervention after ORL Reoperation for hemorrhage Graft loss Postoperative infections Prolonged length of stay Decreased one-year survival TACO (with increased portal hypertension and bleeding) AKI | [48,49,50,51,52] |
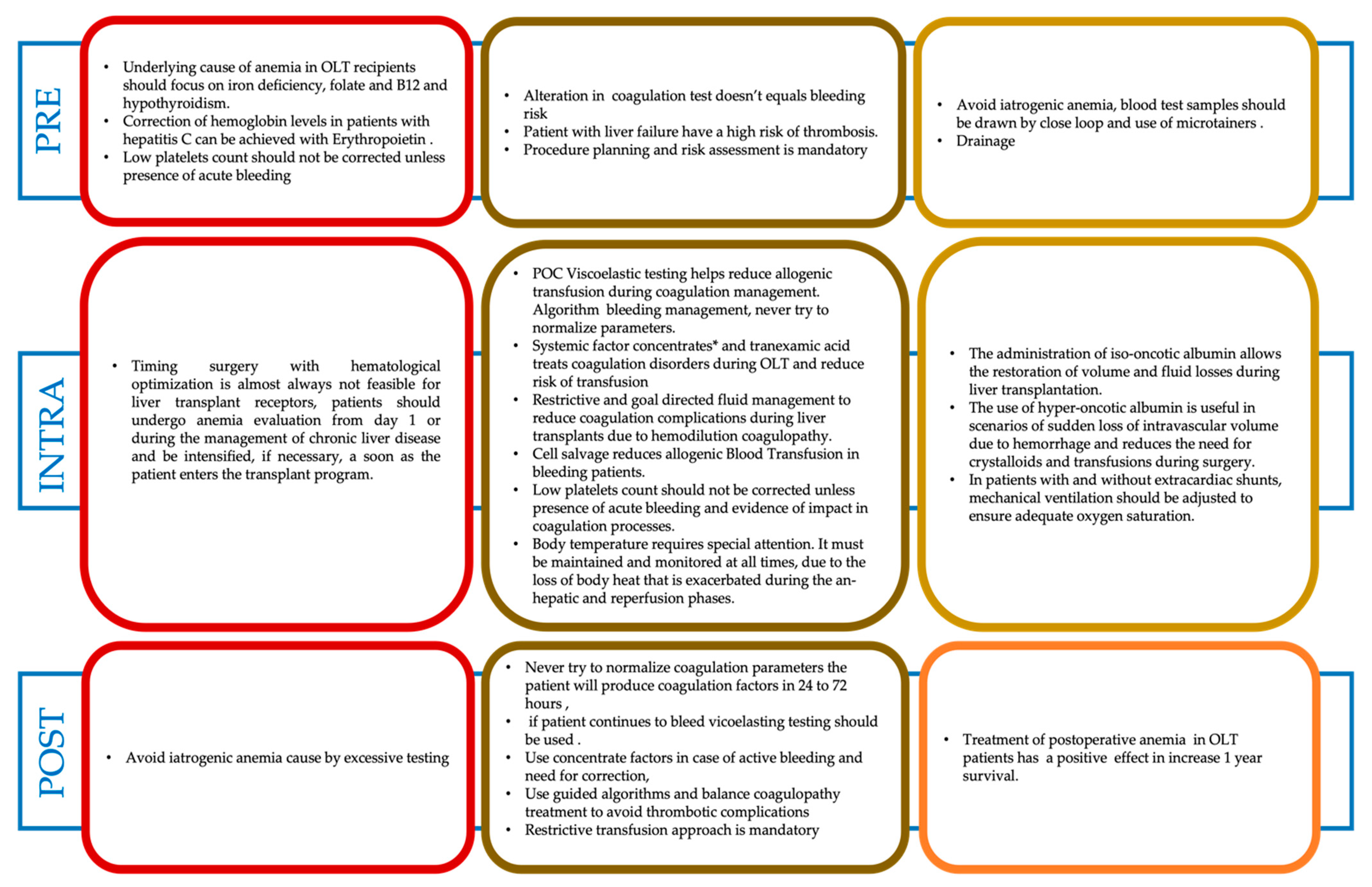
3.4. The Three-Pillar Matrix of PBM in Liver Transplantation (Figure 1)
3.4.1. Anemia and Thrombocytopenia Management

3.4.2. Bleeding and Coagulation Management
3.5. Coagulation Issues during Liver Transplantation
3.5.1. Pre-Anhepatic Phase
3.5.2. Anhepatic Phase
3.5.3. Post Reperfusion Phase
3.5.4. Postoperative Phase
3.6. Viscoelastic Testing for Coagulation Management in Liver Transplant
4. Hemostatic Drugs
4.1. Antifibrinolytics
4.2. Fibrinogen Concentrates
4.3. Prothrombin Complex Concentrate
4.4. Thrombopoietin Receptors Agonist (TPO)
5. Pediatric Considerations
6. Blood Conservation Technics in Liver Transplantation
7. Patient Blood Management Consideration for Acute Liver Failure
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rana, A.; Petrowsky, H.; Hong, J.C.; Agopian, V.G.; Kaldas, F.M.; Farmer, D.; Yersiz, H.; Hiatt, J.R.; Busuttil, R.W. Blood transfusion requirement during liver transplantation is an important risk factor for mortality. J. Am. Coll. Surg. 2013, 216, 902–907. [Google Scholar] [CrossRef]
- McCluskey, S.A.; Karkouti, K.; Wijeysundera, D.N.; Kakizawa, K.; Ghannam, M.; Hamdy, A.; Grant, D.; Levy, G. Derivation of a risk index for the prediction of massive blood transfusion in liver transplantation. Liver Transpl. 2006, 12, 1584–1593. [Google Scholar] [CrossRef]
- Massicotte, L.; Lenis, S.; Thibeault, L.; Sassine, M.P.; Seal, R.F.; Roy, A. Effect of low central venous pressure and phlebotomy on blood product transfusion requirements during liver transplantations. Liver Transpl. 2006, 12, 117–123. [Google Scholar] [CrossRef]
- Cleland, S.; Corredor, C.; Ye, J.J.; Srinivas, C.; McCluskey, S.A. Massive haemorrhage in liver transplantation: Consequences, prediction and management. World J. Transplant. 2016, 6, 291e305. [Google Scholar] [CrossRef]
- Holt, S.; Donaldson, H.; Hazlehurst, G.; Varghese, Z.; Contreras, M.; Kingdon, E.; Sweny, P.; Burns, A. Acute transplant rejection induced by blood transfusion reaction to the Kidd blood group system. Nephrol. Dial. Transplant. 2004, 19, 2403–2406. [Google Scholar] [CrossRef] [Green Version]
- Han, S.; Kwon, J.H.; Jung, S.H.; Seo, J.Y.; Jo, Y.J.; Jang, J.S.; Yeon, S.M.; Jung, S.H.; Ko, J.S.; Gwak, M.S.; et al. Perioperative Fresh Red Blood Cell Transfusion May Negatively Affect Recipient Survival After Liver Transplantation. Ann. Surg. 2018, 267, 346–351. [Google Scholar] [CrossRef]
- Görlinger, K.; Saner, F.H. Prophylactic Plasma and Platelet Transfusion in the Critically Ill Patient: Just Useless and Expensive or even Harmful? BMC Anesthesiol. 2015, 15, 86. [Google Scholar] [CrossRef] [Green Version]
- Steinbicker, A.U.; Wittenmeier, E.; Goobie, S.M. Pediatric Non-Red Cell Blood Product Transfusion Practices: What’s the Evidence to Guide Transfusion of the ‘Yellow’ Blood Products? Curr. Opin. Anaesthesiol. 2020, 33, 259–267. [Google Scholar] [CrossRef]
- Shander, A.; Hardy, J.F.; Ozawa, S.; Farmer, S.L.; Hofmann, A.; Frank, S.M.; Kor, D.J.; Faraoni, D.; Freedman, J. A Global Definition of Patient Blood Management. Anesth Analg. 2022, 135, 476–488. [Google Scholar] [CrossRef]
- Isbister, J. The three-pillar matrix of patient blood management. ISBT Sci. Series 2015, 10, 286–294. [Google Scholar] [CrossRef]
- Hofmann, A.; Friedman, D.; Farmer, S. Western Australian Patient Blood Management Project 2008–2012: Analysis, Strategy, Implementation and Financial Projections; Western Australia Department of Health: Perth, Australia, 2007; pp. 1–154. [Google Scholar]
- Hofmann, A.; Farmer, S.; Shander, A. Five drivers shifting the paradigm from product-focused transfusion practice to patient blood management. Oncologist 2011, 16 (Suppl. 3), 3–11. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The Urgent Need to Implement Patient Blood Management: Policy Brief; World Health Organization: Geneva, Switzerland, 2021; ISBN 9789240035744. Available online: https://apps.who.int/iris/handle/10665/346655 (accessed on 12 March 2023).
- Parker, A.; Karvellas, C.J. Coagulation Defects in the Cirrhotic Patient Undergoing Liver Transplantation. Transplantation 2018, 102, 1453–1458. [Google Scholar] [CrossRef]
- Mrzljak, A.; Franusic, L.; Pavicic-Saric, J.; Kelava, T.; Jurekovic, Z.; Kocman, B.; Mikulic, D.; Budimir-Bekan, I.; Knotek, M. Pre- and intraoperative Predictors of Acute Kidney Injury after Liver Transplantation. World J. Clin. Cases 2020, 8, 4034–4042. [Google Scholar] [CrossRef]
- Lisman, T.; Adelmeijer, J.; de Groot, P.G.; Janssen, H.L.; Leebeek, F.W. No evidence for an intrinsic platelet defect in patients with liver cirrhosis studies under flow conditions. J. Thromb. Haemost. 2006, 4, 2070–2072. [Google Scholar] [CrossRef]
- Tripodi, A.; Primignani, M.; Chantarangkul, V.; Clerici, M.; Dell’Era, A.; Fabris, F.; Salerno, F.; Mannucci, P.M. Thrombin generation in patients with cirrhosis: The role of platelets. Hepatology 2006, 44, 440–445. [Google Scholar] [CrossRef]
- Blanchard, R.A.; Furie, B.C.; Jorgensen, M.; Kruger, S.F.; Furie, B. Acquired vitamin K-dependent carboxylation deficiency in liver disease. N. Engl. J. Med. 1981, 305, 242–248. [Google Scholar] [CrossRef]
- Martinez, J.; MacDonald, K.A.; Palascak, J.E. The role of sialic acid in the dysfibrinogenemia associated with liver disease: Distribution of sialic acid on the constituent chains. Blood 1983, 61, 1196–1202. [Google Scholar] [CrossRef] [Green Version]
- Hughes, R.D.; Lane, D.A.; Ireland, H.; Langley, P.G.; Gimson, A.E.; Williams, R. Fibrinogen derivatives and platelet activation products in acute and chronic liver disease. Clin. Sci. 1985, 68, 701–707. [Google Scholar] [CrossRef] [Green Version]
- McMurry, H.S.; Jou, J.; Shatzel, J. The Hemostatic and Thrombotic Complications of Liver Disease. Eur. J. Haematol. 2021, 107, 383–392. [Google Scholar] [CrossRef]
- Gunetilleke, B.; Welikala, N.D.; Görlinger, K. Viscoelastic Haemostatic Test Based Management of Coagulopathy in Liver Transplantation for Cirrhosis. Sri Lanka J. Haematol. 2021, 13, 1–9. [Google Scholar]
- Lisman, T.; Leebeek, F.W.; Mosnier, L.O.; Bouma, B.N.; Meijers, J.C.; Janssen, H.L.; Nieuwenhuis, H.K.; De Groot, P.G. Thrombin-activatable fibrinolysis inhibitor deficiency in cirrhosis is not associated with increased plasma fibrinolysis. Gastroenterology 2001, 121, 131–139. [Google Scholar] [CrossRef]
- Pihusch, R.; Rank, A.; Gohring, P.; Pihusch, M.; Hiller, E.; Beuers, U. Platelet function rather than plasmatic coagulation explains hypercoagulable state in cholestatic liver disease. J. Hepatol. 2002, 37, 548–555. [Google Scholar] [CrossRef]
- Ben-Ari, Z.; Panagou, M.; Patch, D.; Bates, S.; Osman, E.; Pasi, J.; Burroughs, A. hypercoagulability in patients with primary biliary cirrhosis and primary sclerosing cholangitis evaluated by thrombelastography. J. Hepatol. 1997, 26, 554–559. [Google Scholar] [CrossRef]
- Lisman, T.; Porte, R.J. Rebalanced hemostasis in patients with liver disease: Evidence and clinical consequences. Blood 2010, 116, 878–885. [Google Scholar] [CrossRef] [Green Version]
- Lisman, T.; Bongers, T.N.; Adelmeijer, J.; Janssen, H.L.; de Maat, M.P.; de Groot, P.G.; Leebeek, F.W. Elevated levels of von Willebrand factor in cirrhosis support platelet adhesion despite reduced functional capacity. Hepatology 2006, 44, 53–61. [Google Scholar] [CrossRef]
- Mannucci, P.M.; Canciani, M.T.; Forza, I.; Lussana, F.; Lattuada, A.; Rossi, E. Changes in health and disease of the metalloprotease that cleaves von Willebrand factor. Blood 2001, 98, 2730–2735. [Google Scholar] [CrossRef]
- Stravitz, R.T.; Fontana, R.J.; Meinzer, C.; Durkalski-Mauldin, V.; Hanje, A.J.; Olson, J.; Koch, D.; Hamid, B.; Schilsky, M.L.; McGuire, B.; et al. ALF Study Group. Coagulopathy, Bleeding Events and Outcome According to Rotational Thromboelastometry in Patients with Acute Liver Injury/Failure. Hepatology 2021, 72, 937–949. [Google Scholar] [CrossRef]
- Colucci, M.; Binetti, B.M.; Branca, M.G.; Clerici, C.; Morelli, A.; Semeraro, N.; Gresele, P. Deficiency of thrombin activatable fibrinolysis inhibitor in cirrhosis is associated with increased plasma fibrinolysis. Hepatology 2003, 38, 230–237. [Google Scholar] [CrossRef]
- Müller, M.C.; Straat, M.; Meijers, J.C.; Klinkspoor, J.H.; de Jonge, E.; Arbous, M.S.; Schultz, M.J.; Vroom, M.B.; Juffermans, N.P. Fresh frozen plasma transfusion fails to influence the hemostatic balance in critically ill patients with a coagulopathy. J. Thromb. Haemost. 2015, 13, 989–997. [Google Scholar] [CrossRef]
- Wolberg, A.S.; Meng, Z.H.; Monroe, D.M., III; Hoffman, M. A systematic evaluation of the effect of temperature on coagulation enzyme activity and platelet function. J. Trauma. 2004, 56, 1221–1228. [Google Scholar] [CrossRef]
- Mohanty, A.; Kapuria, D.; Canakis, A.; Lin, H.; Amat, M.J.; Rangel Paniz, G.; Placone, N.T.; Thomasson, R.; Roy, H.; Chak, E.; et al. Fresh Frozen Plasma Transfusion in Acute Variceal Haemorrhage: Results from a Multicentre Cohort Study. Liver Int. 2021, 41, 1901–1908. [Google Scholar] [CrossRef]
- Hartmann, M.; Walde, C.; Dirkmann, D.; Saner, F.H. Safety of Coagulation Factor Concentrates guided by ROTEM-Analyses in Liver Transplantation: Results from 372 Procedures. BMC Anesthesiol. 2019, 19, 97. [Google Scholar] [CrossRef] [PubMed]
- Mitrophanov, A.Y.; Rosendaal, F.R.; Reifman, J. Computational analysis of the effects of reduced temperature on thrombin generation: The contributions of hypothermia to coagulopathy. Anesth. Analg. 2013, 117, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Vitin, A.; Muczynski, K.; Bakthavatsalam, R.; Martay, K.; Dembo, G.; Metzner, J. Treatment of severe lactic acidosis during the pre-anhepatic stage of liver transplant surgery with intraoperative hemodialysis. J. Clin. Anesth. 2010, 22, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Abuelkasem, E.; Hasan, S.; Mazzeffi, M.A.; Planinsic, R.M.; Sakai, T.; Tanaka, K.A. Reduced Requirement for Prothrombin Complex Concentrate for the Restoration of Thrombin Generation in Plasma From Liver Transplant Recipients. Anesth. Analg. 2017, 125, 609–615. [Google Scholar] [CrossRef]
- Dötsch, T.M.; Dirkmann, D.; Bezinover, D.; Hartmann, M.; Treckmann, J.W.; Paul, A.; Saner, F.H. Assessment of Standard Laboratory Tests and Rotational Thromboelastometry for the Prediction of Postoperative Bleeding in Liver Transplantation. Br. J. Anaesth. 2017, 119, 402–410. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, P.; Agarwal, A.; Jha, A.; Rodricks, S.; Malik, T.; Makki, K.; Singhal, A.; Vij, V. Utility of prothrombin complex concentrate as first-line treatment modality of coagulopathy in patients undergoing liver transplantation: A propensity score-matched study. Clin. Transplant. 2018, 32, e13435. [Google Scholar] [CrossRef]
- Zamper, R.P.C.; Amorim, T.C.; Queiroz, V.N.F.; Lira, J.D.O.; Costa, L.G.V.; Takaoka, F.; Juffermans, N.P.; Neto, A.S. Association between Viscoelastic Tests-guided Therapy with Synthetic Factor Concentrates and Allogenic Blood Transfusion in Liver Transplantation: A before-after Study. BMC Anesthesiol. 2018, 18, 198. [Google Scholar] [CrossRef]
- Katsanoulas, K.; Georgopoulou, E.; Markopoulos, I.; Katsika, E. Thromboelastometry-Based Algorithm and Transfusion Management During Orthotopic Liver Transplantations. Eur. J. Anaesthesiol. 2021, 38, 444–446. [Google Scholar] [CrossRef]
- Rodríguez-Laiz, G.P.; Melgar-Requena, P.; Alcázar-López, C.F.; Franco-Campello, M.; Villodre-Tudela, C.; Pascual-Bartolomé, S.; Bellot-García, P.; Rodríguez-Soler, M.; Miralles-Maciá, C.F.; Más-Serrano, P.; et al. Fast-Track Liver Transplantation: Six-year Prospective Cohort Study with an Enhanced Recovery After Surgery (ERAS) Protocol. World J. Surg. 2021, 45, 1262–1271. [Google Scholar] [CrossRef]
- Pereboom, I.T.; de Boer, M.T.; Haagsma, E.B.; Hendriks, H.G.; Lisman, T.; Porte, R.J. Platelet Transfusion during Liver Transplantation is Associated with Increased Postoperative Mortality due to Acute Lung Injury. Anesth. Analg. 2009, 108, 1083–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, J.L.; Hisamuddin, S.H.; O’Sullivan, A.; Chan, G.; McCormick, P.A. Thrombocytopenia, Platelet Transfusion, and Outcome Following Liver Transplantation. Clin. Appl. Thromb. Hemost. 2016, 22, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Zhao, K.M.; Luo, L.H.; Yu, Y.; Zhu, S.M. Perioperative Single-Donor Platelet Apheresis and Red Blood Cell Transfusion Impact on 90-Day and overall Survival in Living Donor Liver Transplantation. Chin. Med. J. 2018, 131, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Schenk, B.; Lindner, A.K.; Treichl, B.; Bachler, M.; Hermann, M.; Larsen, O.H.; Fenger-Eriksen, C.; Wally, D.; Tauber, H.; Velik-Salchner, C.; et al. Fibrinogen supplementation ex vivo increases clot firmness comparable to platelet transfusion in thrombocytopenia. Br. J. Anaesth. 2016, 117, 576–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripodi, A.; Primignani, M.; Chantarangkul, V.; Lemma, L.; Jovani, M.; Rebulla, P.; Mannucci, P.M. Global hemostasis tests in patients with cirrhosis before and after prophylactic platelet transfusion. Liver Int. 2013, 33, 362–367. [Google Scholar] [CrossRef]
- Hudcova, J.; Qasmi, S.T.; Ruthazer, R.; Waqas, A.; Haider, S.B.; Schumann, R. Early Allograft Dysfunction Following Liver Transplant: Impact of Obesity, Diabetes, and Red Blood Cell Transfusion. Transplant. Proc. 2021, 53, 119–123. [Google Scholar] [CrossRef]
- Gjærde, L.K.; Sørensen, A.L.T.; von Stemann, J.H.; Fischer-Nielsen, A.; Hansen, M.B.; Sengeløv, H.; Ostrowski, S.R. Platelet and Red Blood Cell Transfusions and Risk of Acute Graft-versus-Host Disease after Myeloablative Allogeneic Hematopoietic Cell Transplantation. Transplant. Cell. Ther. 2021, 27, 866.e1–866.e9. [Google Scholar] [CrossRef]
- Hosoba, S.; Waller, E.K.; Shenvi, N.; Graiser, M.; Easley, K.A.; Al-Kadhimi, Z.; Andoh, A.; Antun, A.G.; Barclay, S.; Josephson, C.D.; et al. Peritransplantation Red Blood Cell Transfusion Is Associated with Increased Risk of Graft-versus-Host Disease after Allogeneic Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2018, 24, 973–982. [Google Scholar] [CrossRef] [Green Version]
- Benson, A.B.; Burton, J.R., Jr.; Austin, G.L.; Biggins, S.W.; Zimmerman, M.A.; Kam, I.; Mandell, S.; Silliman, C.C.; Rosen, H.; Moss, M. Differential effects of plasma and red blood cell transfusions on acute lung injury and infection risk following liver transplantation. Liver Transpl. 2011, 17, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Ramos, E.; Dalmau, A.; Sabate, A.; Lama, C.; Llado, L.; Figueras, J.; Jaurrieta, E. Intraoperative red blood cell transfusion in liver transplantation: Influence on patient outcome, prediction of requirements, and measures to reduce them. Liver Transpl. 2003, 9, 1320–1327. [Google Scholar] [CrossRef]
- Gkamprela, E.; Deutsch, M.; Pectasides, D. Iron deficiency anemia in chronic liver disease: Etiopathogenesis, diagnosis and treatment. Ann. Gastroenterol. 2017, 30, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Cariani, E.; Pelizzari, A.M.; Rodella, A.; Gargiulo, F.; Imberti, L.; Manca, N.; Rossi, G. Immune-mediated hepatitis-associated aplastic Anemia caused by the emergence of a mutant hepatitis B virus undetectable by standard assays. J. Hepatol. 2007, 46, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.P.; Younossi, Z.M. Managing the hematologic side effects of antiviral therapy for chronic hepatitis C: Anemia, neutropenia, and thrombocytopenia. Cleve. Clin. J. Med. 2004, 71 (Suppl. 3), S17–S21. [Google Scholar] [CrossRef] [PubMed]
- Reau, N.; Hadziyannis, S.J.; Messinger, D.; Fried, M.W.; Jensen, D.M. Early predictors of Anemia in patients with hepatitis C genotype 1 treated with peginterferon alfa-2a (40KD) plus ribavirin. Am. J. Gastroenterol. 2008, 103, 1981–1988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ioannou, G.N.; Dominitz, J.A.; Weiss, N.S.; Heagerty, P.J.; Kowdley, K.V. The effect of alcohol consumption on the prevalence of iron overload, iron deficiency, and iron deficiency anemia. Gastroenterology 2004, 126, 1293–1301. [Google Scholar] [CrossRef]
- Lichtenegger, P.; Schiefer, J.; Graf, A.; Berlakovich, G.; Faybik, P.; Baron, D.M.; Baron-Stefaniak, J. The association of preoperativepreoperative anaemia with survival after orthotopic liver transplantation. Anaesthesia 2020, 75, 472–478. [Google Scholar] [CrossRef]
- Viguera, L.; Blasi, A.; Reverter, E.; Arjona, B.; Caballero, M.; Chocron, I.; García-López, J.A.; Gutierrez, R.; Martin, M.J.; Pérez-Peña, J.; et al. Baseline Haemoglobin and Thromboelastometry are Predictive of Red Blood Cell Requirements and One-Year Mortality in Liver Transplantation. Transfus. Apher. Sci. 2021, 60, 103259. [Google Scholar] [CrossRef]
- Berger, T.; Reisler, I.; Shochat, T.; Raanani, P.; Nesher, E.; Mor, E.; Gafter-Gvili, A.; Shlomai, A. Post-Liver Transplantation Anemia and Its Correlation with Mortality and Graft Failure. Dig. Dis. Sci. 2020, 65, 3040–3051. [Google Scholar] [CrossRef]
- Spivak, J.L. Cancer-related Anemia: Its causes and characteristics. Semin. Oncol. 1994, 21, 3–8. [Google Scholar]
- Görlinger, K.; Pérez-Ferrer, A.; Dirkmann, D.; Saner, F.; Maegele, M.; Calatayud, Á.A.P.; Kim, T.Y. The role of evidence-based algorithms for rotational thromboelastometry-guided bleeding management. Korean J. Anesthesiol. 2019, 72, 297–322. [Google Scholar] [CrossRef] [Green Version]
- Bezinover, D.; Dirkmann, D.; Findlay, J.; Guta, C.; Hartmann, M.; Nicolau-Raducu, R.; Mukhtar, A.M.; Moguilevitch, M.; Pivalizza, E.; Rosenfeld, D.; et al. Perioperative Coagulation Management in Liver Transplant Recipients. Transplantation 2018, 102, 578–592. [Google Scholar] [CrossRef] [PubMed]
- Biancofiore, G.; Blasi, A.; De Boer, M.T.; Franchini, M.; Hartmann, M.; Lisman, T.; Liumbruno, G.M.; Porte, R.J.; Saner, F.; Senzolo, M.; et al. Perioperative Hemostatic Management in the Cirrhotic Patient: A Position Paper on behalf of the Liver Intensive Care Group of Europe (LICAGE). Minerva Anestesiol. 2019, 85, 782–798. [Google Scholar] [CrossRef]
- Yoon, U.; Bartoszko, J.; Bezinover, D.; Biancofiore, G. ERAS4OLT.org Working Group. Intraoperative Transfusion Management, Antifibrinolytic Therapy, Coagulation Monitoring and the Impact on Short-term Outcomes after Liver Transplantation—A Systematic Review of the Literature and Expert Panel Recommendations. Clin. Transplant. 2022, 6, e14637. [Google Scholar] [CrossRef]
- Warnaar, N.; Lisman, T.; Porte, R.J. The two tales of coagulation in liver transplantation. Curr. Opin. Organ. Transplant. 2008, 13, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Shimauchi, T.; Yamaura, K.; Higashi, M.; Abe, K.; Yoshizumi, T.; Hoka, S. Fibrinolysis in living donor liver transplantation recipients evaluated using thromboelastometry: Impact on mortality. Transplant. Proc. 2017, 49, 2117–2121. [Google Scholar] [CrossRef]
- Poon, K.S.; Chen, C.C.; Thorat, A.; Chiang, Y.Y.; Jeng, L.B.; Yang, H.R.; Chen, T.H.; Yeh, C.C.; Chen, K.B. Fibrinolysis after reperfusion of liver graft. Acta Anaesthesiol. Taiwan 2015, 53, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Yassen, K.; Refaat, E.; Helal, S.; Metwally, A.; Youssef, S.; Gorlinger, K. Perioperative heparinase rotational thromboelastometry monitoring during and after adult living related liver transplantation. Eur. J. Anaesthesiol. 2018, 35 (Suppl. 56), 286. [Google Scholar]
- Vetrovec, G.; Stravitz, R.T. Bleeding in Patients with Cirrhosis Undergoing Invasive Cardiovascular Procedures: Do We Overestimate Risk? Circulation 2020, 141, 1279–1281. [Google Scholar] [CrossRef]
- Mpaili, E.; Tsilimigras, D.I.; Moris, D.; Sigala, F.; Frank, S.M.; Hartmann, J.; Pawlik, T.M. Utility of Viscoelastic Coagulation Testing in Liver Surgery: A Systematic Review. HPB 2021, 23, 331–343. [Google Scholar] [CrossRef]
- Schaden, E.; Saner, F.H.; Goerlinger, K. Coagulation Pattern in Critical Liver Dysfunction. Curr. Opin. Crit. Care 2013, 19, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, M.; Lorenz, B.; Brenner, T.; Saner, F.H. Elevated Pre- and Postoperative ROTEM™ Clot Lysis Indices Indicate Reduced Clot Retraction and Increased Mortality in Patients Undergoing Liver Transplantation. Biomedicines 2022, 10, 1975. [Google Scholar] [CrossRef] [PubMed]
- Fayed, N.; Mourad, W.; Yassen, K.; Görlinger, K. Preoperative Thromboelastometry as a Predictor of Transfusion Requirements during Adult Living Donor Liver Transplantation. Transfus. Med. Hemother. 2015, 42, 99–108. [Google Scholar] [CrossRef] [Green Version]
- Hashir, A.; Singh, S.A.; Krishnan, G.; Subramanian, R.; Gupta, S. Correlation of Early ROTEM Parameters with Conventional Coagulation Tests in Patients with Chronic Liver Disease undergoing Liver Transplant. Indian J. Anaesth. 2019, 63, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Carrier, F.M.; Denault, A.Y.; Nozza, A.; Rioux-Massé, B.; Roy, A.; Massicotte, L. Association between intraoperative Rotational Thromboelastometry or Conventional Coagulation Tests and Bleeding in Liver Transplantation: An observational exploratory Study. Anaesth. Crit. Care Pain Med. 2020, 39, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.K.; Moon, Y.J.; Song, I.K.; Kang, E.J.; Shin, W.J.; Hwang, G.S. A Look into Hemostatic Characteristics during Pediatric Liver Transplantation using the Thromboelastometry (ROTEM®) Test. Liver Transpl. 2022, 28, 1628–1639. [Google Scholar] [CrossRef] [PubMed]
- Al Moosawi, M.; Trudeau, J.; Smith, T.; Lefebvre, A.; Shih, A.W. ROTEM in the Setting of Liver Transplant Surgery Reduces Frozen Plasma Transfusion. Transfus. Apher. Sci. 2021, 60, 103125. [Google Scholar] [CrossRef]
- Sabate, A.; Dalmau, A.; Koo, M.; Aparicio, I.; Costa, M.; Contreras, L. Coagulopathy management in liver transplantation. Transplant. Proc. 2012, 44, 1523–1525. [Google Scholar] [CrossRef]
- Görlinger, K.; Sakai, T.; Dirkmann, D.; Planinsic, R.M.; Saner, F.H. Bleeding related to liver transplant. In Management of Bleeding Patients; Teruya, J., Ed.; Springer: Basel, Switzerland, 2016; pp. 263–280. [Google Scholar]
- Pandey, C.K.; Singh, A.; Kajal, K.; Dhankhar, M.; Tandon, M.; Pandey, V.K.; Karna, S.T. Intraoperative blood loss in orthotopic liver transplantation: The predictive factors. World J. Gastrointest. Surg. 2015, 7, 86–93. [Google Scholar] [CrossRef]
- Görlinger, K. Coagulation management during liver transplantation. Hamostaseologie 2006, 26 (Suppl. 1), S64–S76. [Google Scholar] [CrossRef] [Green Version]
- Schofield, N.; Sugavanam, A.; Thompson, K.; Mallett, S.V. No increase in blood transfusions during liver transplantation since the withdrawal of aprotinin. Liver Transpl. 2014, 20, 584–590. [Google Scholar] [CrossRef]
- Dirkmann, D.; Gorlinger, K.; Peters, J. Assessment of early thromboelastometric variables from extrinsically activated assays with and without aprotinin for rapid detection of fibrinolysis. Anesth. Analg 2014, 119, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Song, S.H.; Kim, G.S.; Ko, J.S.; Gwak, M.S.; Lee, S.K. Evaluation of “flat-line” thromboelastography after reperfusion during liver transplantation. Transplant. Proc. 2015, 47, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Abuelkasem, E.; Lu, S.; Tanaka, K.; Planinsic, R.; Sakai, T. Comparison between thrombelastography and thromboelastometry in hyperfibrinolysis detection during adult liver transplantation. Br. J. Anaesth. 2016, 116, 507–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katori, N.; Tanaka, K.A.; Szlam, F.; Levy, J.H. The effects of platelet count on clot retraction and tissue plasminogen activator-induced fibrinolysis on thrombelastography. Anesth. Analg. 2005, 100, 1781–1785. [Google Scholar] [CrossRef]
- Sabate, A.; Blasi, A.; Costa, M.; Reyes, R.; Beltran, J.; Torres, F. Assessment of rotational thromboelastometry for the prediction of red blood cell requirements in orthotopic liver transplantation. Minerva Anestesiol. 2018, 84, 447–454. [Google Scholar] [CrossRef]
- Hincker, A.; Feit, J.; Sladen, R.N.; Wagener, G. Rotational thromboelastometry predicts thromboembolic complications after major noncardiac surgery. Crit. Care 2014, 18, 549. [Google Scholar] [CrossRef]
- Rossetto, V.; Spiezia, L.; Senzolo, M.; Rodriguez-Castro, K.I.; Maggiolo, S.; Simioni, P. Whole blood rotation thromboelastometry (ROTEM®) profiles in subjects with non-neoplastic portal vein thrombosis. Thromb. Res. 2013, 132, e131–e134. [Google Scholar] [CrossRef]
- Zanetto, A.; Senzolo, M.; Vitale, A.; Cillo, U.; Radu, C.; Sartorello, F.; Spiezia, L.; Campello, E.; Rodriguez-Castro, K.; Ferrarese, A.; et al. Thromboelastometry hypercoagulable profiles and portal vein thrombosis in cirrhotic patients with hepatocellular carcinoma. Dig. Liver Dis. 2017, 49, 440–445. [Google Scholar] [CrossRef]
- Blasi, A.; Molina, V.; Sanchez-Cabus, S.; Balust, J.; Garcia-Valdecasas, J.C.; Taura, P. Prediction of thromboembolic complications after liver resection for cholangiocarcinoma: Is there a place for thromboelastometry? Blood Coagul. Fibrinolysis 2018, 29, 61–66. [Google Scholar] [CrossRef]
- Kamel, Y.; Hassanin, A.; Ahmed, A.R.; Gad, E.; Afifi, M.; Khalil, M.; Görlinger, K.; Yassen, K. Perioperative thromboelastometry for adult living donor liver transplant recipients with a tendency to hypercoagulability: A prospective observational cohort study. Transfus. Med. Hemother. 2018, 45, 404–412. [Google Scholar] [CrossRef]
- Hawkins, R.B.; Raymond, S.L.; Hartjes, T.; Efron, P.A.; Larson, S.D.; Andreoni, K.A.; Thomas, E.M. Review: The Perioperative Use of Thromboelastography for Liver Transplant Patients. Transplant. Proc. 2018, 50, 3552–3558. [Google Scholar] [CrossRef] [PubMed]
- Boylan, J.F.; Klinck, J.R.; Sandler, A.N.; Arellano, R.; Greig, P.D.; Nierenberg, H.; Roger, S.L.; Glynn, M.F. Tranexamic acid reduces blood loss, transfusion requirements, and coagulation factor use in primary orthotopic liver transplantation. Anesthesiology 1996, 85, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Dalmau, A.; Sabaté, A.; Acosta, F.; Garcia-Huete, L.; Koo, M.; Sansano, T.; Rafecas, A.; Figueras, J.; Jaurrieta, E.; Parrilla, P. Tranexamic acid reduces red cell transfusion better than epsilon-aminocaproic acid or placebo in liver transplantation. Anesth. Analg. 2000, 91, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, P.; Bechstein, W.O.; Lefbre, B.; Blumhardt, G.; Slama, K. Effect of aprotinin on intraoperative bleeding and fibrinolysis in liver transplantation. Lancet 1989, 2, 924–925. [Google Scholar] [CrossRef] [PubMed]
- Lentschener, C.; Roche, K.; Ozier, Y. A review of aprotinin in orthotopic liver transplantation: Can its harmful effects offset its beneficial effects? Anesth. Analg. 2005, 100, 1248–1255. [Google Scholar] [CrossRef]
- Dalmau, A.; Sabaté, A.; Koo, M.; Bartolomé, C.; Rafecas, A.; Figueras, J.; Jaurrieta, E. The prophylactic use of tranexamic acid and aprotinin in orthotopic liver transplantation: A comparative study. Liver Transpl. 2004, 10, 279–284. [Google Scholar] [CrossRef]
- Molenaar, I.Q.; Warnaar, N.; Groen, H.; TenVergert, E.M.; Slooff, M.J.H.; Porte, R.J. Efficacy and safety of antifibrinolytic drugs in liver transplantation: A systematic review and meta-analysis. Am. J. Transplant. 2007, 7, 185–194. [Google Scholar] [CrossRef]
- Badenoch, A.; Sharma, A.; Gower, S.; Selzner, M.; Srinivas, C.; Wąsowicz, M.; McCluskey, S.A. The effectiveness and safety of tranexamic acid in orthotopic liver transplantation clinical practice: A propensity score matched cohort study. Transplantation 2017, 101, 1658–1665. [Google Scholar] [CrossRef]
- HALT-IT Trial Collaborators. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): An international randomised, double-blind, placebo-controlled trial. Lancet 2020, 395, 1927–1936. [Google Scholar] [CrossRef]
- Stolt, H.; Shams Hakimi, C.; Singh, S.; Jeppsson, A.; Karlsson, M. A comparison of the in vitro effects of three Fibrinogen Concentrates on clot strength in blood samples from cardiac surgery patients. Acta Anaesthesiol. Scand. 2021, 65, 1439–1446. [Google Scholar] [CrossRef]
- Colin-Bracamontes, I.; Pérez-Calatayud, Á.A.; Carrillo-Esper, R.; Rodríguez-Ayala, E.; Padilla-Molina, M.; Posadas-Nava, A.; Olvera-Vázquez, S.; Hernández-Salgado, L. Observational Safety Study of Clottafact® Fibrinogen Concentrate: Real-World Data in Mexico. Clin. Drug Investig. 2020, 40, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zermatten, M.G.; Fraga, M.; Moradpour, D.; Bertaggia Calderara, D.; Aliotta, A.; Stirnimann, G.; De Gottardi, A.; Alberio, L. Hemostatic Alterations in Patients With Cirrhosis: From Primary Hemostasis to Fibrinolysis. Hepatology 2020, 71, 2135–2148. [Google Scholar] [CrossRef]
- Hensley, N.B.; Mazzeffi, M.A. Pro-Con Debate: Fibrinogen Concentrate or Cryoprecipitate for Treatment of Acquired Hypofibrinogenemia in Cardiac Surgical Patients. Anesth. Analg. 2021, 133, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Neisser-Svae, A.; Hegener, O.; Görlinger, K. Differences in the Biochemical Composition of Three Plasma Derived Human Fibrinogen Concentrates. Thromb. Res. 2021, 205, 44–46. [Google Scholar] [CrossRef] [PubMed]
- Groeneveld, D.J.; Adelmeijer, J.; Hugenholtz, G.C.G.; Arins, R.A.S.; Porte, R.J.; Lisman, T. Ex vivo addition of fibrinogen concentrate improves the fibrin network structure in plasma samples taken during liver transplantation. J. Thromb. Haemost. 2015, 13, 2192–2201. [Google Scholar] [CrossRef] [PubMed]
- Sabate, A.; Gutierrez, R.; Beltran, J.; Mellado, P.; Blasi, A.; Acosta, F.; Costa, M.; Reyes, R.; Torres, F. Impact of preemptive fiFibrinogenoncentrate on transfusion requirements in liver transplantation: A multicenter, randomized, double-blind, placebo- controlled trial. Am. J. Transplant. 2016, 16, 2421–2429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stange, B.J.; Glanemann, M.; Nuessler, N.C.; Settmacher, U.; Steinmüller, T.; Neuhaus, P. Hepatic artery thrombosis after adult liver transplantation. Liver Transpl. 2003, 9, 612–620. [Google Scholar] [CrossRef]
- Bekker, J.; Ploem, S.; de Jong, K.P. Early hepatic artery thrombosis after liver transplantation: A systematic review of the incidence, outcome and risk factors. Am. J. Transplant. 2009, 9, 746–757. [Google Scholar] [CrossRef]
- Gunsar, F.; Rolando, N.; Pastacaldi, S.; Patch, D.; Raimondo, M.L.; Davidson, B.; Rolles, K.; Burroughs, A.K. Late hepatic artery thrombosis after orthotopic liver transplantation. Liver Transpl. 2003, 9, 605–611. [Google Scholar] [CrossRef]
- Kirchner, C.; Dirkmann, D.; Treckmann, J.W.; Paul, A.; Hartmann, M.; Saner, F.H.; Görlinger, K. Coagulation management with factor concentrates in liver transplantation: A single-center experience: Factor concentrates in liver transplant. Transfusion 2014, 54, 2760–2768. [Google Scholar] [CrossRef]
- Goldstein, J.N.; Refaai, M.A.; Milling TJJr Lewis, B.; Goldberg-Alberts, R.; Hug, B.A.; Sarode, R. Four-factor prothrombin complex concentrate versus plasma for rapid vitamin K antagonist reversal in patients needing urgent surgical or invasive interventions: A phase 3b, open-label, non-inferiority, randomized trial. Lancet 2015, 385, 2077–2087. [Google Scholar] [CrossRef] [PubMed]
- Refaai, M.A.; Goldstein, J.N.; Lee, M.L.; Durn, B.L.; Milling, T.J.; Sarode, R. Increased risk of volume overload with plasma compared with four-factor prothrombin complex concentrate for urgent vitamin K antagonist reversal. Transfusion 2015, 55, 2722–2729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, D.A.; O’Brien, F.J.; Hutton, R.A.; Tuddenham, E.G.; Summerfield, J.A.; Sherlock, S. The Effect of liver disease on factors V, VIII and protein C. Br. J. Haematol. 1985, 61, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, R.; Kienast, J.; Otto, U.; Egger, K.; Kiehl, M.; Schreiter, D.; Kwasny, H.; Haertel, S.; Barthels, M. Efficacy and safety of a prothrombin complex concentrate with two virus-inactivation steps in patients with severe liver damage. Eur. J. Gastroenterol. Hepatol. 2003, 15, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Lodge, J.P.; Jonas, S.; Jones, R.M.; Olausson, M.; Mir-Pallardo, J.; Soefelt, S.; Garcia-Valdecasas, J.C.; McAlister, V.; Mirza, D.F. Efficacy and safety of repeated perioperative doses of recombinant factor VIIa in liver transplantation. Liver Transpl. 2005, 11, 973–979. [Google Scholar] [CrossRef]
- Terrault, N.; Chen, Y.C.; Izumi, N.; Kayali, Z.; Mitrut, P.; Tak, W.Y.; Allen, L.F.; Hassanein, T. Avatrombopag Before Procedures Reduces Need for Platelet Transfusion in Patients With Chronic Liver Disease and Thrombocytopenia. Gastroenterology 2018, 155, 705–718. [Google Scholar] [CrossRef] [Green Version]
- Peck-Radosavljevic, M.; Simon, K.; Iacobellis, A.; Hassanein, T.; Kayali, Z.; Tran, A.; Makara, M.; Ben Ari, Z.; Braun, M.; Mitrut, P.; et al. Lusutrombopag for the treatment of thrombocytopenia in patients with chronic liver disease undergoing invasive procedures (L-Plus 2). Hepatology 2019, 70, 1336–1348. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Ferrer, A.; García-Erce, J.A.; Muñóz, M. Medicina Transfusional Patient Blood Management. Edicion 2. El Paciente Pediátrico; Editorial Panamericana: Madrid, Spain, 2018; pp. 161–172. [Google Scholar]
- Squires, R.H.; Ng, V.; Romero, R.; Ekong, U.; Hardikar, W.; Emre, S.; Mazariegos, G.V. Evaluation of the pediatric patient for liver transplantation: 2014 practice guideline by the American Association for the Study of Liver Diseases, American Society of Transplantation and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Hepatology 2014, 60, 362–398. [Google Scholar] [CrossRef]
- Kozek-Langenecker, S.A.; Ahmed, A.B.; Afshari, A.; Albaladejo, P.; Aldecoa, C.; Barauskas, G.; De Robertis, E.; Faraoni, D.; Filipescu, D.C.; Dietmar, F.; et al. Management of severe perioperative bleeding: Guidelines from the european society of anaesthesiology. Eur. J. Anaesthesiol. 2017, 34, 332–395. [Google Scholar] [CrossRef] [Green Version]
- Yudkowitz, F.S.; Chietero, M. Anesthesic issues in pediatric liver transplantation. Pediatric. Transplant. 2005, 9, 1399–3046. [Google Scholar] [CrossRef]
- Hass, T.; Mauch, J.; Weis, M.; Schmugge, M. Management of dilutional coagulophaty during pediatric major surgery. Transfus. Med. Hemotheraphy 2012, 39, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faroni, D.; Goobie, S.M. New insights about the use of tranexamic acid in children undergoing cardiac surgery: From pharmacokinetics to pharmacodynamic. Anesth. Analg. 2013, 117, 760–762. [Google Scholar] [CrossRef] [PubMed]
- New, H.V.; Berryman, J.; Bolton-Maggs, P.H.; Cantwell, C.; Chalmers, E.A.; Davies, T.; Gottstein, R.; Kelleher, A.; Kumar, S.; Morley, S.L.; et al. Guidelines on transfusion for fetuses, neonates and older children. Br. J. Haematol. 2016, 175, 784–828. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.; Al, M.; Westwood, M.; Ramos, I.C.; Ryder, S.; Armstrong, N.; Misso, K.; Ross, J.; Severens, J.; Kleijnen, J. Viscoelastic point-of-care testing to assist with the diagnosis, management and monitoring of haemostasis: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2015, 19, 1–228. [Google Scholar] [CrossRef] [Green Version]
- Pinto, M.A.; Chedid, M.F.; Sekine, L.; Schmidt, A.P.; Capra, R.P.; Prediger, C.; Prediger, J.E.; Grezzana-Filho, T.J.; Kruel, C.R. Intraoperative cell salvage with autologous transfusion in liver transplantation. World J. Gastrointest. Surg. 2019, 11, 11–18. [Google Scholar] [CrossRef]
- Massicotte, L.; Thibeault, L.; Beaulieu, D.; Roy, J.D.; Roy, A. Evaluation of cell salvage autotransfusion utility during liver transplantation. HPB 2007, 9, 52–57. [Google Scholar] [CrossRef] [Green Version]
- Feltracco, P.; Michieletto, E.; Barbieri, S.; Serra, E.; Rizzi, S.; Salvaterra, F.; Cillo, U.; Ori, C. Microbiologic contamination of intraoperative blood salvaged during liver transplantation. Transplant. Proc. 2007, 39, 1889–1891. [Google Scholar] [CrossRef]
- O’Leary, J.G.; Greenberg, C.S.; Patton, H.M.; Caldwell, S.H. AGA Clinical Practice Update: Coagulation in Cirrhosis. Gastroenterology 2019, 157, 34–43.e1. [Google Scholar] [CrossRef]


| Step | Explanation | |
|---|---|---|
| 1 | Check basic conditions | Temp. > 35 °C; pH > 7.3; Cai 2+ > 1 mmol/L; Hb ≥ 7 g/dL. |
| 2 | Antifibrinolytic therapy | FIBCT > 600 s represents a flat line in FIBTEM. Pre-anhepatic hyperfibrinolysis increases mortality in OLT [62]; hyperfibrinolysis at/after reperfusion without diffuse bleeding may be self-limiting; if ML is less than 15%, consider avoidance of TXA treatment. |
| 3 | Fibrinogen dose calculation | Fibrinogen dose (g) = targeted increase in A5FIB (mm) × body weight (kg)/160. The correction factor (140–160 mm kg/g) depends on the plasma volume; 10 U Cryoprecipitate ≈2 g fibrinogen concentrate. |
| 4 | Platelet concentrate transfusion | Platelet transfusion is associated with increased mortality in liver transplantation. |
| 5 | Antithrombin (AT) substitution | Consider AT substitution in patients with an increased risk of thrombosis (e.g., primary biliary cirrhosis, Budd–Chiari syndrome, portal vein thrombosis, malignancies) and known pre-existing severe AT Deficiency. |
| 6 | Protamine | Endogenous heparin effect after liver graft reperfusion is self-limiting and does not require reversal by protamine. Consider protamine administration in severe bleeding. |
| 7 | Simultaneous interventions | Only in severe bleeding, consider a maximum of three interventions simultaneously. In moderate bleeding, consider a maximum of two interventions simultaneously. There was only one intervention simultaneously (in second or later analysis and mild to moderate bleeding). |
| Step | Explanation | |
|---|---|---|
| 1 | Check basic conditions | Temp. > 35 °C; pH > 7.3; Cai 2+ > 1 mmol/L; Hb ≥ 7 g/dL. |
| 2 | Antifibrinolytic therapy | Tranexamic Acid pediatric dose is 15 mg/kg as a single bolus. |
| 3 | Fibrinogen dose calculation | Fibrinogen dose (g) = targeted increase in A5FIB (mm) × body weight (kg)/160. The correction factor (140–160 mm kg/g) depends on the plasma volume; 10 U Cryoprecipitate ≈ 2 g fibrinogen concentrate. |
| 4 | Platelet concentrate transfusion | Platelet concentrate 5–10 mL/kg single donor or apheresis. |
| 5 | Antithrombin (AT) substitution | Consider AT substitution in patients with an increased risk of thrombosis (e.g., primary biliary cirrhosis, Budd–Chiari syndrome, portal vein thrombosis, malignancies) and known pre-existing severe AT deficiency. |
| 6 | Protamine | Consider protamine (0.3–0.5 mg/kg) in severe bleeding. |
| 7 | Simultaneous interventions | Only in severe bleeding, consider a maximum of three interventions simultaneously. Moderate bleeding, consider a maximum of two interventions simultaneously. There was only one intervention simultaneously (in second or later analysis and mild to moderate bleeding). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Calatayud, A.A.; Hofmann, A.; Pérez-Ferrer, A.; Escorza-Molina, C.; Torres-Pérez, B.; Zaccarias-Ezzat, J.R.; Sanchez-Cedillo, A.; Manuel Paez-Zayas, V.; Carrillo-Esper, R.; Görlinger, K. Patient Blood Management in Liver Transplant—A Concise Review. Biomedicines 2023, 11, 1093. https://doi.org/10.3390/biomedicines11041093
Pérez-Calatayud AA, Hofmann A, Pérez-Ferrer A, Escorza-Molina C, Torres-Pérez B, Zaccarias-Ezzat JR, Sanchez-Cedillo A, Manuel Paez-Zayas V, Carrillo-Esper R, Görlinger K. Patient Blood Management in Liver Transplant—A Concise Review. Biomedicines. 2023; 11(4):1093. https://doi.org/10.3390/biomedicines11041093
Chicago/Turabian StylePérez-Calatayud, Angel Augusto, Axel Hofmann, Antonio Pérez-Ferrer, Carla Escorza-Molina, Bettina Torres-Pérez, Jed Raful Zaccarias-Ezzat, Aczel Sanchez-Cedillo, Victor Manuel Paez-Zayas, Raul Carrillo-Esper, and Klaus Görlinger. 2023. "Patient Blood Management in Liver Transplant—A Concise Review" Biomedicines 11, no. 4: 1093. https://doi.org/10.3390/biomedicines11041093