1. Introduction
The symmetrical chamber dilation, increased myocardial mass and relative bradycardia observed in athletes’ heart [
1] are easily distinguished from the typical morphological and functional features of severe hypertrophic cardiomyopathy (HCM). The differentiation between benign athletic cardiac remodeling and mild phenotypic HCM may, however, be a more difficult task [
2,
3]. Furthermore, the prevalence of HCM is high in the general population, and it will obviously be present in some individuals performing sports. ECG changes may not be conclusive [
4], and conventional echocardiography and cardiac magnetic resonance imaging (CMR) have important shortcomings [
5]. Genetic tests have similar limitations, as 40% of HCM patients do not carry known pathogenic mutations [
6], and the identification of genetic mutations of uncertain significance imposes further uncertainty on the well-being of an athlete and their immediate family.
Myocardial alterations in typical HCM, including myocardial disarray and fibrosis, induce heterogeneity in ventricular contractions not observed in healthy athletes [
7]. Strain echocardiography has been reported to be promising in the differentiation between typical phenotypic HCM and athletes’ hearts [
7,
8,
9], but has not been evaluated in the discrimination of mild HCM from athletic cardiac remodeling. CMR studies have reported high intracellular volumes in the physiological hypertrophy of athletes’ hearts [
10], and conversely high extracellular volumes (ECVs) in patients with HCM [
11]. However, no head-to-head comparisons between athletes and mutation-positive HCM with a mild phenotype using the native T1-time on the same magnet have been performed previously.
We aimed to describe mutation-positive HCM with a mild phenotype and athletes’ hearts using strain echocardiography and CMR indices in order to evaluate their role in the differentiation between the two entities.
2. Materials and Methods
2.1. Study Population
Study participants were recruited between April 2016 and June 2017 in a cross-sectional study. We informed high-level cycling and cross-country skiing teams and other endurance athletes in Oslo about the planned study. Healthy volunteering athletes were encouraged to contact our study group to be considered for inclusion, as previously described [
12]. A selection of clinical data, two-dimensional (2D) echocardiographic measurements and conventional CMR indices from these healthy volunteering athletes have been previously published by Lie et al. in a comparison with athletes with ventricular arrhythmias [
12].
Athletes disclosed their exercise history from school age to present in a structured interview. Exercise was reported as the type of activity/sport, graded at perceived intensity levels 1–3 (light, moderate, vigorous), and the duration was reported as hours per week, months per year, and years. The intensity of the reported activities was rated according to the Compendium of Physical Activities and quantified as metabolic equivalents (METs) [
13]. Exercise dose, expressed as MET-hours, was estimated by means of the multiplication of exercise intensity and exercise duration [
14]. Only mutation-positive, otherwise healthy, sedentary HCM patients with mild phenotypes and a maximal wall thickness of 12–16 mm were included for comparison. These patients were identified by a cascade genetic screening program of 144 HCM probands. Genetic testing was performed as previously described [
15]. Only patients with pathogenic or likely pathogenic mutations were included (myosin binding protein C 3 (
MYBPC3, n = 13), beta-myosin heavy chain 7 (
MYH7, n = 4), troponin I (
TNNI3, n = 2) and troponin T (
TNNT2, n = 1)).
Subjects with more than moderate valvular disease, left ventricular (LV) outflow track obstruction, atrial fibrillation, hypertension, coronary artery disease, diabetes mellitus, a pacemaker/implantable cardioverter defibrillator or reported use of performance-enhancing drugs were excluded. The study was approved by the Regional Committee for Medical Research in Norway (approval number 2015/1593). Written informed consent was obtained from all study participants.
2.2. Echocardiography
All subjects underwent transthoracic echocardiographic examinations using the Vivid 95 ultrasound system (GE Vingmed Ultrasound AS, Horten, Norway). Data were analyzed with EchoPAC version 201 software (GE Vingmed Ultrasound AS, Horten, Norway). Echocardiographic parameters were assessed in agreement with the expert consensus document on multi-modality imaging approaches to athletes’ hearts [
16]. Maximal wall thickness was assessed by means of 2D echocardiography. Full-volume three-dimensional (3D) LV acquisitions were obtained in the left decubital position during a complete breath-hold for six heart cycles, achieving frame rates of >35 frames per second. Three-dimensional LV volumes, mass and ejection fraction (EF) were estimated during post-processing with the LVQ-tool (GE Healthcare). The left atrial volume was calculated using the biplane area–length method.
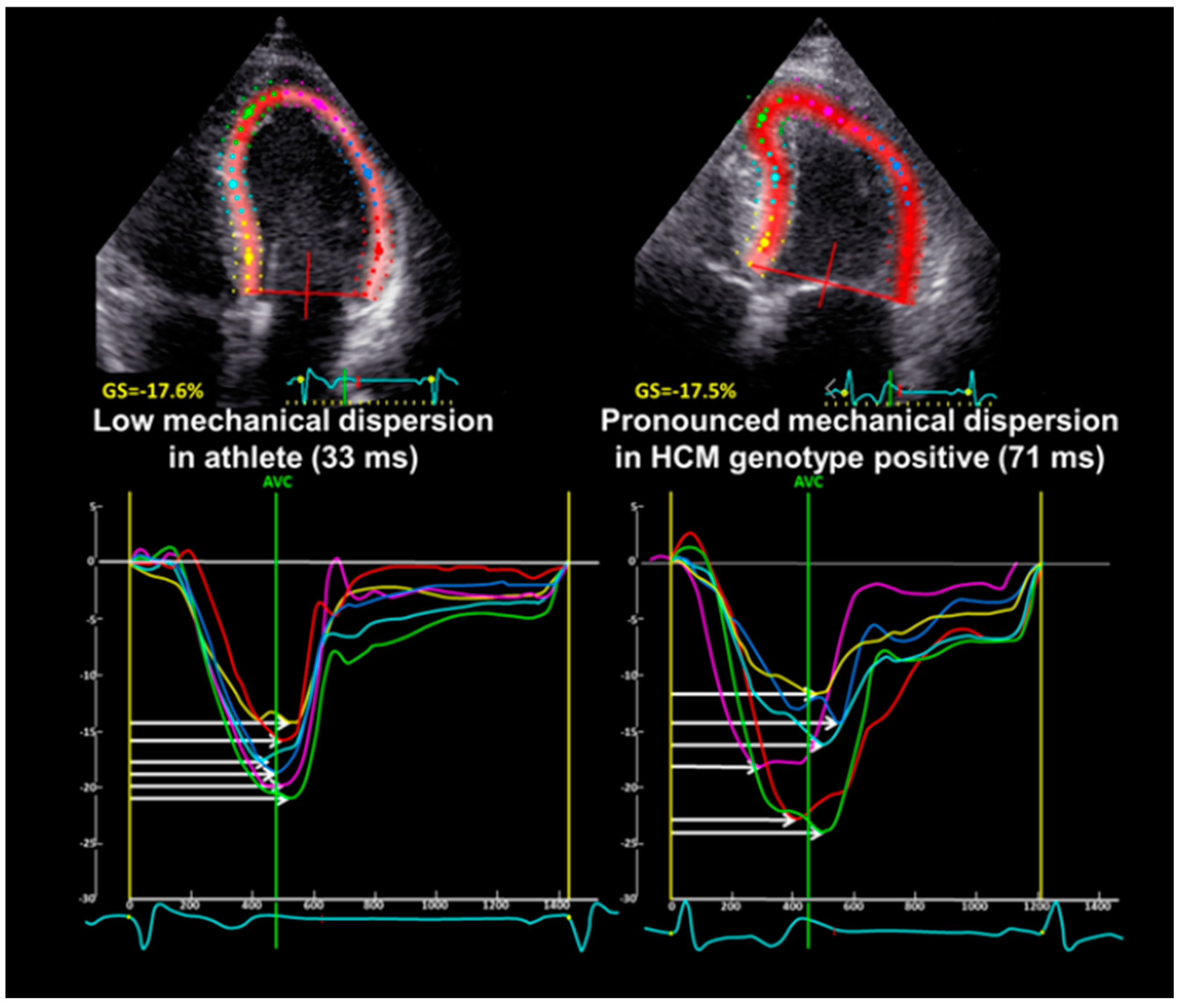
The LV global longitudinal strain (GLS) was derived from speckle tracking analyses on 2D gray scale image loops with >50 frames per second from the three apical views, and was expressed as the average peak systolic strain in a 16 segment LV model [
17]. LV mechanical dispersion was defined as the standard deviation of time from Q/R on the surface ECG to the peak negative strain in 16 LV segments [
18] (
Figure 1).
2.3. Cardiac Magnetic Resonance Imaging
CMR was performed on a single 3 Tesla unit (Philips Ingenia, Philips Healthcare, Best, The Netherlands). Cine sequences of standardized long-axis projections and multiple short-axis projections covering both ventricles were performed (
Figure 2). LV and right ventricular (RV) volumes were calculated semiautomatically by experienced radiologists using the freely available software Segment v2.2 R6405 [
19]. After intravenous injection of the contrast medium, late gadolinium enhancement (LGE) was assessed in the steady state and qualitatively recorded as being present or absent. Native T1 time was recorded as the mean septal value. The ECV was calculated as the ratio between myocardial and blood relaxivity change after contrast medium injection, multiplied by the blood ECV (1—hematocrit) and expressed as a percentage of the total myocardium. Hematocrit values were obtained immediately prior to investigation.
2.4. Statistics
Values were presented as mean ± standard deviations, frequencies with percentages, and medians with the interquartile range (IQR) and were compared using Student’s t-test, χ2, Fischer’s exact test or the Mann–Whitney U test as appropriate (SPSS statistics 27.0, SPSS Inc., Chicago, IL, USA), The discriminatory ability of imaging markers from strain echocardiography and CMR were assessed using receiver operator characteristics (ROC) curves and expressed by the area under the curve (AUC) with a 95% confidence interval (CI). The coordinates from the ROC curves closest to the upper left corner defined the optimal cut-off values. Two-sided p-values < 0.05 were considered statistically significant.
3. Results
3.1. Clinical Characteristics
We included 20 healthy, sedentary mutation-positive HCM subjects with a mild phenotype (15% female, age 51 ± 12 years) identified by means of cascade genetic screening of a population of 144 family members (
Table 1). Thirty healthy competitive endurance elite and elite master athletes were used as a control group and included for comparison [
12]. These athletes (7% female, age 41 ± 9 years) had an accumulated life-time exercise dose of 94 (IQR 64–154) thousand MET-hours. The represented sports were cycling (63%), cross-country skiing (27%), rowing (3%) and triathlon (3%). The athletes were younger and had a lower body surface area (
Table 1).
3.2. Cardiac Imaging
The maximal wall thickness was 10 ± 2 mm in athletes and 13 ± 1 mm in mild phenotypic HCM, as measured by 2D echocardiography (
p < 0.001).
Table 1 shows that athletes and mutation positive HCM subjects had a similar LV mass and LV EF, but the LV volumes established by 3D echocardiography were greater in athletes (
p < 0.001). Furthermore, the RV function assessed by means of 2D fractional area change (FAC) was better in mutation-positive HCM subjects (
p = 0.001). The left atrium was similarly enlarged in mild HCM subjects and athletes. Other indices of diastolic function (E/A ratio, e’ and E/e’ ratio) were normal in both groups, although the values of these diastolic variables were higher in athletes (
Table 1). Speckle tracking echocardiography showed that the athletes and the mutation-positive HCM subjects had similar, normal GLS, but mechanical dispersion was more pronounced in mutation-positive HCM subjects (
p = 0.001).
CMR was completed in 19 (86%) mild phenotypic HCM subjects and 29 (97%) healthy athletes. Higher LVEF and RVEF were found in mild HCM subjects, while athletes had greater LV and RV volumes. LGE was more prevalent in mild phenotypic HCM than in healthy athletes. Athletes had a lower native T1 time and a lower ECV (
Table 1).
Figure 3 shows the ability of imaging markers from strain echocardiography and T1 mapping techniques to identify HCM mutation carriers from athletes in the study population evaluated via ROC analysis. These results are summarized in
Table 2. According to AUC, the native T1 time and mechanical dispersion were the two imaging markers with the most promising discriminatory ability, while GLS showed poor discriminatory ability. The ROC curves show that the native T1 time established by CMR may identify HCM mutation carriers with excellent sensitivity and good specificity (
Figure 3). The optimal discrimination value of native T1 time in this study population was >1230 ms. This cut off identified all HCM mutation carriers (100% sensitivity) with a specificity of 75%. LV mechanical dispersion > 44 ms optimally discriminated between athletes and HCM mutation carriers (AUC 0.78, 95% CI 0.65–0.91). The AUC for the combined ROC curve for native T1 time and mechanical dispersion was 0.82 (95% CI 0.70–0.95), suggesting no added discriminatory value when combining the two imaging indices from CMR and strain echocardiography with the highest AUC.
In addition to the main parameters of interest (mechanical dispersion, GLS, native T1 time and ECV), we also present ROC analysis of imaging indices that were shown to be significantly different among athletes and HCM mutation carriers in
Supplementary Table S1, although these parameters were not the primary target of investigation in this study.
4. Discussion
In the current study, mutation-positive, mild phenotypic HCM patients and competitive endurance athletes underwent evaluation via echocardiography and subsequent CMR in a comparative experimental setting. Sedentary subjects with mutation-positive mild HCM had a more pronounced mechanical dispersion, a higher native T1 time, a higher ECV and a higher prevalence of LGE, suggestive of greater disarray and fibrosis than athletes. Among the strain parameters, GLS could not differentiate mild HCM from athletes’ hearts, while mechanical dispersion showed promising discriminatory ability. The native T1 time established by CMR showed better diagnostic performance than ECV and mechanical dispersion in identifying HCM mutation carriers in a mixed population with endurance athletes.
4.1. Physiological and Pathological Myocardial Remodeling
Undiagnosed underlying heart disease is the leading cause of sudden cardiac death in athletes. In younger athletes, inherited cardiomyopathies such as HCM are the main causes of these tragic events [
20]. Traditionally, people with HCM have been advised not to participate in sports. This view has become more nuanced in recent years as data regarding athletic cardiac remodeling and the impact of physical activity in HCM are accumulating [
21,
22]. HCM and athletes’ hearts share common morphological features that might complicate the differentiation between the two clinical entities. A common scenario is when maximal wall thickness falls into the “gray zone” between the pathological hypertrophy of HCM and physiological athletic remodeling, drawing attention to a possible underlying inherited cardiomyopathy. Genetic testing may be helpful, although a large proportion of patients with HCM belong to a negative genotype, and the pathogenicity of a genetic mutation may be difficult to establish [
23]. The fact that patients with an HCM-causing genetic mutation may present with virtually any wall thickness complicates this further [
24]. New biomarkers that clarify the patient’s condition are therefore of interest. The current study focused on strain echocardiography, which is widely available, and the more advanced CMR-derived native T1 time and ECV, in a comparative study to evaluate whether these indices could demonstrate differences related to myocardial properties in high-performance endurance athletes and patients with mild HCM without classical phenotypical features or discernable comorbidities that could cause cardiac remodeling.
4.2. Imaging Myocardial Properties
Myocardial cellular disarray and fibrosis are common structural alterations in HCM [
25]. These changes may even be found in young HCM patients who are completely asymptomatic until the event of sudden cardiac death [
26]. Using imaging techniques that can accurately assess myocardial function or characterize tissue may detect the disease at an earlier stage.
Strain echocardiography offers a sensitive functional assessment of the myocardium. The rationale for using strain to evaluate early pathological remodeling is the ability to uncover subtle changes in myocardial function that are not detected by conventional echocardiographic measures. Focusing on functional measures as a surrogate for altered myocardial properties rather than tissue characteristics, strain has only moderate diagnostic performance compared to CMR to detect fibrosis [
27].
Abnormal GLS has been suggested as a diagnostic tool to distinguish HCM from athletic cardiac remodeling [
8,
9], but one previous report found no discriminatory value for GLS [
28]. Without reporting the genotype, the same report described mechanical dispersion to be promising in differentiating athletes from a population of patients with a typical HCM phenotype. In the present study, pronounced mechanical dispersion revealed LV contraction heterogeneity even in milder HCM disease, although other measures of systolic LV function were similar in the athletes. In accordance with a previous report, we found no significant differences in longitudinal function by means of GLS between athletes and patients with HCM [
28].
CMR using LGE can identify the patchy replacement fibrosis of HCM typically present in the most maximally hypertrophied segments [
5]. However, as approximately 50% of patients have no LGE, HCM cannot be ruled out based on LGE assessment [
5]. Therefore, the novel techniques of assessing diffuse myocardial fibrosis according to the native T1 time and ECV have gained more attention. In our cohort, we found more individuals with LGE indicative of replacement fibrosis in the mild HCM phenotype. A longer native T1 time and a higher ECV were consistent with different tissue characteristics in mild HCM, possibly due to more cellular disarray and cellular matrix expansion compared to athletes. This provides a plausible explanation for the more pronounced mechanical dispersion observed in the HCM group, as changes in myocardial composition have previously been linked to heterogeneous ventricular contractions in HCM [
7].
4.3. Diagnostic Considerations and Future Perspectives
As illustrated by the ROC curves, sensitivity and specificity vary among echocardiographic and CMR indices. The current study preselected athletes and mild phenotypic HCM patients under rigorous circumstances using genetic testing of known mutations as a gold standard to identify HCM in a mixed population with athletes.
ROC analysis suggests that the native T1 time has better diagnostic performance than mechanical dispersion and the ECV, and that the discriminatory ability of GLS is inadequate to separate athletes and HCM. Moreover, combined ROC analysis indicates no additional discriminatory improvement compared to a multimodality approach combining STE and CMR, but this may be due to the limited sample size. Although the discriminatory ability of strain imaging and T1 mapping techniques may be promising, the clinical cut off values or usefulness cannot be inferred from this study design. The next logical step would be an investigation evaluating the same imaging methods in a clinical setting in athletes with suspected HCM, where the discrimination properties of the discussed methods are likely to change.
This study focused on parameters from strain imaging and CMR. There were, however, indications of discriminatory ability among more conventional imaging parameters (
Supplementary Table S1). Worthy of note is that E/e’ had one of the highest AUC values in the dataset. Whether this phenomenon is related to structural variations among athletes and HCM patients beyond differences in cardiac volumes should be further investigated.
4.4. Limitations
This was a comparative experiment performed on two separate groups of individuals in whom different myocardial composition is certain. The results are not directly applicable to other populations. All comparative analysis should be interpreted in the context of the limited sample size. Despite the constraint of a limited sample size, the appearance of significant differences between the compared groups suggests the presence of important underlying diagnostic signals. These comparisons are merely hypothesis-generating for future studies. Finally, the maximal LV wall thickness is a common way of assessing hypertrophy, but the minor differences in wall thickness in our study were due to the study design and inclusion criteria.
5. Conclusions
Our study reveals that LV contraction heterogeneity in mild HCM is characterized by more pronounced mechanical dispersion as evidenced by strain echocardiography. Additionally, T1 mapping techniques by means of CMR demonstrate greater disarray and fibrosis in mild HCM patients than in athletes. These findings underscore the potential of speckle tracking echocardiography and CMR as sensitive tools for detecting myocardial alterations that can effectively differentiate between athletic cardiac remodeling and mild HCM. Our findings offer valuable insights into the mechanisms of cardiac remodeling, disclosing differences in physiological and pathological hypertrophy.
Future research should evaluate the utility of speckle tracking echocardiography and CMR in broader populations, particularly in athletes presenting with suspected HCM. The identification of these differences could possibly also be applied in novel diagnostic pathways not only for HCM, but also for other cardiomyopathies.
Author Contributions
Conceptualization, L.G.K., Ø.H.L., K.H.H. and T.E.; methodology, L.G.K., Ø.H.L., P.H.B., K.H.H. and T.E.; formal analysis, L.G.K., Ø.H.L., G.B. and E.H.; writing—original draft preparation, L.G.K., P.H.B. and T.E.; writing—review and editing, L.G.K., Ø.H.L., P.H.B., G.B., E.H., K.H.H. and T.E.; supervision, T.E. All authors have read and agreed to the published version of the manuscript.
Funding
This study received funding from the South-Eastern Norway Regional Health Authority (grant #2011094) and the Research Council of Norway (grant #203489).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Regional Committee for Medical Research in Norway (approval number 2015/1593).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sharma, S.; Merghani, A.; Mont, L. Exercise and the heart: The good, the bad, and the ugly. Eur. Heart J. 2015, 36, 1445–1453. [Google Scholar] [CrossRef]
- Pelliccia, A.; Caselli, S.; Sharma, S.; Basso, C.; Bax, J.J.; Corrado, D.; D’Andrea, A.; D’Ascenzi, F.; Di Paolo, F.M.; Edvardsen, T.; et al. European Association of Preventive Cardiology (EAPC) and European Association of Cardiovascular Imaging (EACVI) joint position statement: Recommendations for the indication and interpretation of cardiovascular imaging in the evaluation of the athlete’s heart. Eur. Heart J. 2018, 39, 1949–1969. [Google Scholar] [CrossRef]
- Dejgaard, L.A.; Haland, T.F.; Lie, O.H.; Ribe, M.; Bjune, T.; Leren, I.S.; Berge, K.E.; Edvardsen, T.; Haugaa, K.H. Vigorous exercise in patients with hypertrophic cardiomyopathy. Int. J. Cardiol. 2018, 250, 157–163. [Google Scholar] [CrossRef]
- Pelliccia, A.; Di Paolo, F.M.; Quattrini, F.M.; Basso, C.; Culasso, F.; Popoli, G.; De Luca, R.; Spataro, A.; Biffi, A.; Thiene, G.; et al. Outcomes in athletes with marked ECG repolarization abnormalities. N. Engl. J. Med. 2008, 358, 152–161. [Google Scholar] [CrossRef]
- Gati, S.; Sharma, S.; Pennell, D. The Role of Cardiovascular Magnetic Resonance Imaging in the Assessment of Highly Trained Athletes. J. Am. Coll. Cardiol. Imaging 2018, 11, 247–259. [Google Scholar] [CrossRef]
- Marian, A.J.; Braunwald, E. Hypertrophic Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy. Circ. Res. 2017, 121, 749–770. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Caso, P.; Cuomo, S.; Salerno, G.; Scarafile, R.; Mita, C.; De Corato, G.; Sarubbi, B.; Scherillo, M.; Calabrò, R. Prognostic value of intra-left ventricular electromechanical asynchrony in patients with mild hypertrophic cardiomyopathy compared with power athletes. Br. J. Sports Med. 2006, 40, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Richand, V.; Lafitte, S.; Reant, P.; Serri, K.; Lafitte, M.; Brette, S.; Kerouani, A.; Chalabi, H.; Dos Santos, P.; Douard, H.; et al. An ultrasound speckle tracking (two-dimensional strain) analysis of myocardial deformation in professional soccer players compared with healthy subjects and hypertrophic cardiomyopathy. Am. J. Cardiol. 2007, 100, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Kansal, M.M.; Lester, S.J.; Surapaneni, P.; Sengupta, P.P.; Appleton, C.P.; Ommen, S.R.; Ressler, S.W.; Hurst, R.T. Usefulness of two-dimensional and speckle tracking echocardiography in “Gray Zone” left ventricular hypertrophy to differentiate professional football player’s heart from hypertrophic cardiomyopathy. Am. J. Cardiol. 2011, 108, 1322–1326. [Google Scholar] [CrossRef] [PubMed]
- McDiarmid, A.K.; Swoboda, P.P.; Erhayiem, B.; Lancaster, R.E.; Lyall, G.K.; Broadbent, D.A.; Dobson, L.E.; Musa, T.A.; Ripley, D.P.; Garg, P.; et al. Athletic Cardiac Adaptation in Males Is a Consequence of Elevated Myocyte Mass. Circ. Cardiovasc. Imaging 2016, 9, e003579. [Google Scholar] [CrossRef] [PubMed]
- Parekh, K.; Markl, M.; Deng, J.; de Freitas, R.A.; Rigsby, C.K. T1 mapping in children and young adults with hypertrophic cardiomyopathy. Int. J. Cardiovasc. Imaging 2017, 33, 109–117. [Google Scholar] [CrossRef]
- Lie, Ø.H.; Klaboe, L.G.; Dejgaard, L.A.; Skjølsvik, E.T.; Grimsmo, J.; Bosse, G.; Hopp, E.; Edvardsen, T.; Haugaa, K.H. Cardiac Phenotypes and Markers of Adverse Outcome in Elite Athletes With Ventricular Arrhythmias. J. Am. Coll. Cardiol. Imaging 2021, 14, 148–158. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Wasfy, M.M.; Baggish, A.L. Exercise Dose in Clinical Practice. Circulation 2016, 133, 2297–2313. [Google Scholar] [CrossRef]
- Haland, T.F.; Almaas, V.M.; Hasselberg, N.E.; Saberniak, J.; Leren, I.S.; Hopp, E.; Edvardsen, T.; Haugaa, K.H. Strain echocardiography is related to fibrosis and ventricular arrhythmias in hypertrophic cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 613–621. [Google Scholar] [CrossRef]
- Galderisi, M.; Cardim, N.; D’Andrea, A.; Bruder, O.; Cosyns, B.; Davin, L.; Donal, E.; Edvardsen, T.; Freitas, A.; Habib, G.; et al. The multi-modality cardiac imaging approach to the Athlete’s heart: An expert consensus of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 353–353r. [Google Scholar] [CrossRef]
- Edvardsen, T.; Haugaa, K.H. Imaging assessment of ventricular mechanics. Heart 2011, 97, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Haugaa, K.H.; Grenne, B.L.; Eek, C.H.; Ersbøll, M.; Valeur, N.; Svendsen, J.H.; Florian, A.; Sjøli, B.; Brunvand, H.; Køber, L.; et al. Strain echocardiography improves risk prediction of ventricular arrhythmias after myocardial infarction. J. Am. Coll. Cardiol. Imaging 2013, 6, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Heiberg, E.; Sjögren, J.; Ugander, M.; Carlsson, M.; Engblom, H.; Arheden, H. Design and validation of Segment—Freely available software for cardiovascular image analysis. BMC Med. Imaging 2010, 10, 1. [Google Scholar] [CrossRef]
- Semsarian, C.; Sweeting, J.; Ackerman, M.J. Sudden cardiac death in athletes. BMJ 2015, 350, h1218. [Google Scholar] [CrossRef]
- Mascia, G.; Olivotto, I.; Brugada, J.; Arbelo, E.; Di Donna, P.; Della Bona, R.; Canepa, M.; Porto, I. Sport practice in hypertrophic cardiomyopathy: Running to stand still? Int. J. Cardiol. 2021, 345, 77–82. [Google Scholar] [CrossRef]
- Pelliccia, A.; Day, S.; Olivotto, I. Leisure-time and competitive sport participation: A changing paradigm for HCM patients. Eur. J. Prev. Cardiol. 2023, 30, 488–495. [Google Scholar] [CrossRef] [PubMed]
- El Hadi, H.; Freund, A.; Desch, S.; Thiele, H.; Majunke, N. Hypertrophic, Dilated, and Arrhythmogenic Cardiomyopathy: Where Are We? Biomedicines 2023, 11, 524. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Ommen, S.R.; Semsarian, C.; Spirito, P.; Olivotto, I.; Maron, M.S. Hypertrophic Cardiomyopathy: Present and Future, with Translation into Contemporary Cardiovascular Medicine. J. Am. Coll. Cardiol. 2014, 64, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Chandra, N.; Bastiaenen, R.; Papadakis, M.; Sharma, S. Sudden Cardiac Death in Young Athletes. J. Am. Coll. Cardiol. 2013, 61, 1027–1040. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Shirani, J.; Poliac, L.C.; Mathenge, R.; Roberts, W.C.; Mueller, F.O. Sudden death in young competitive athletes. Clinical, demographic, and pathological profiles. JAMA 1996, 276, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Karamitsos, T.D.; Arvanitaki, A.; Karvounis, H.; Neubauer, S.; Ferreira, V.M. Myocardial Tissue Characterization and Fibrosis by Imaging. J. Am. Coll. Cardiol. Imaging 2020, 13, 1221–1234. [Google Scholar] [CrossRef]
- Schnell, F.; Matelot, D.; Daudin, M.; Kervio, G.; Mabo, P.; Carré, F.; Donal, E. Mechanical Dispersion by Strain Echocardiography: A Novel Tool to Diagnose Hypertrophic Cardiomyopathy in Athletes. J. Am. Soc. Echocardiogr. 2017, 30, 251–261. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}
{kind=link}
{kind=link}