

Evaluation of the Prognostic Impact of SP263-Evaluated PD-L1 Expression in Patients with Stage III Non-Small Cell Lung Cancer (NSLC) Treated with Radio-Chemotherapy
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Treatments
2.2. End Points and Assessments
2.3. Study Oversight
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. PFS
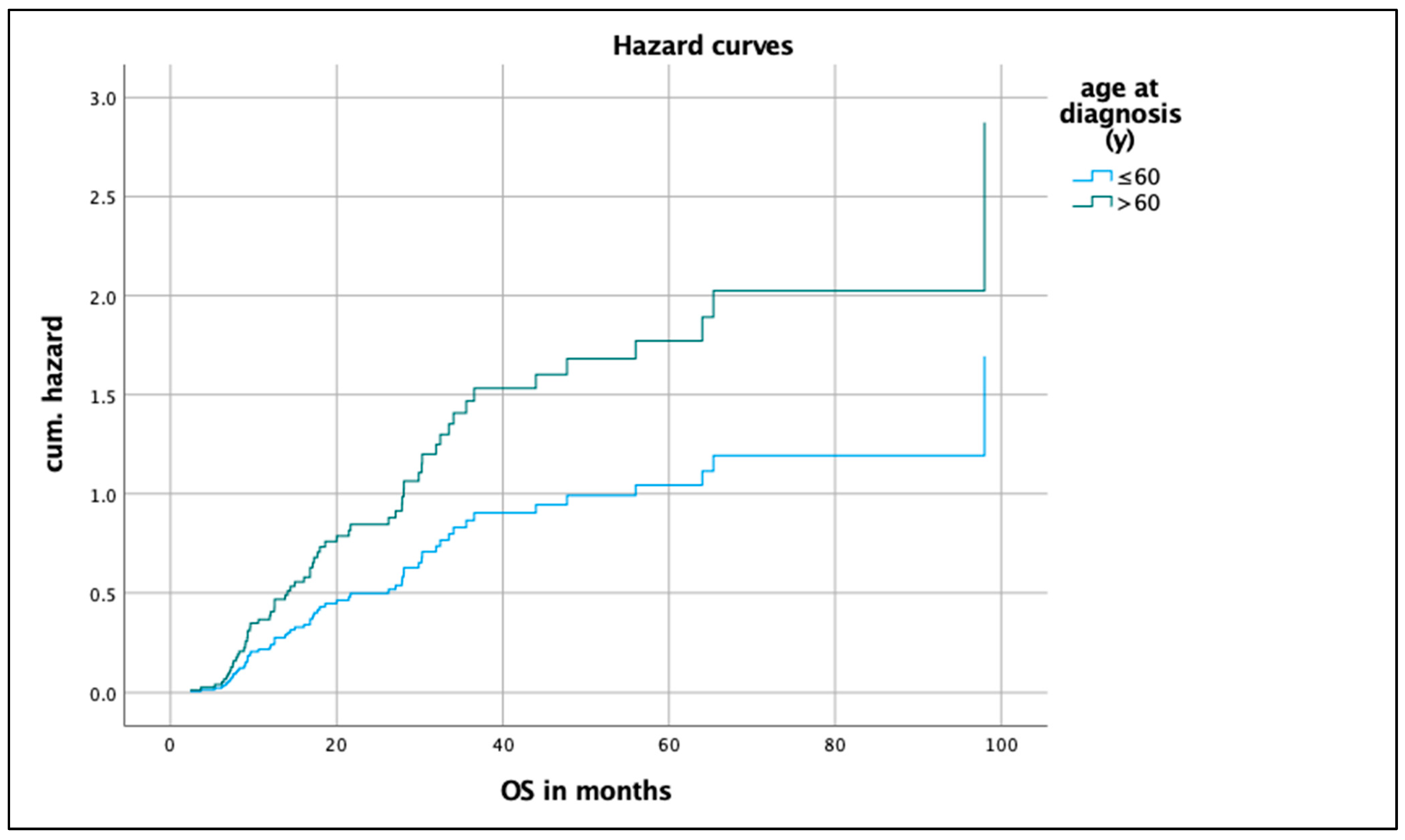
3.3. OS
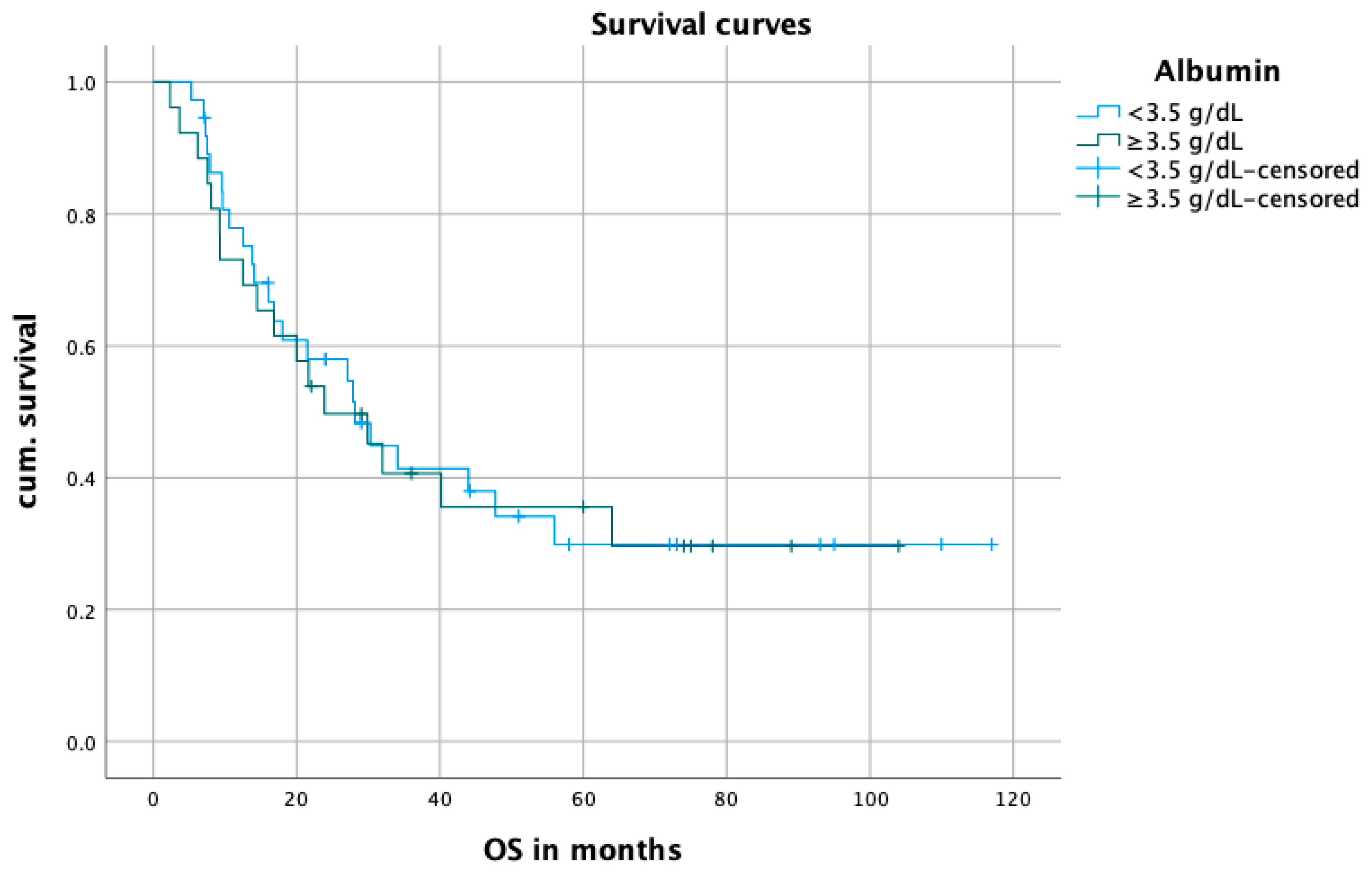
3.4. Blood Parameters
3.5. Cox-Regression
4. Discussion
4.1. Differences in Populations
4.2. Comparison of PFS and OS as a Function of PD-L1 Expression and Blood-Based Biomarkers
4.3. Strengths and Weaknesses of Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Albumin

Appendix A.2. CRP/Albumin Quotient

References
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for pd-l1–positive non–small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with pd-l1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef] [PubMed]
- Ryu, R.; Ward, K.E. Atezolizumab for the first-line treatment of non-small cell lung cancer (NSCLC): Current status and future prospects. Front. Oncol. 2018, 8, 277. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.; Attili, I.; de Marinis, F. Checkmate 9la: Broadening treatment options for patients with non-small-cell lung cancer. Lancet Oncol. 2021, 22, 157–159. [Google Scholar] [CrossRef]
- Arbour, K.C.; Riely, G.J. Systemic therapy for locally advanced and metastatic non-small cell lung cancer: A review. JAMA 2019, 322, 764–774. [Google Scholar] [CrossRef]
- Gadgeel, S.; Rodríguez-Abreu, D.; Speranza, G.; Esteban, E.; Felip, E.; Dómine, M.; Hui, R.; Hochmair, M.J.; Clingan, P.; Powell, S.F.; et al. Updated analysis from keynote-189: Pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metastatic nonsquamous non–small-cell lung cancer. J. Clin. Oncol. 2020, 38, 1505–1517. [Google Scholar] [CrossRef]
- Socinski, M.A.; Mok, T.S.; Nishio, M.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; Moro-Sibilot, D.; et al. Abstract ct216: Impower150 final analysis: Efficacy of atezolizumab (atezo) + bevacizumab (bev) and chemotherapy in first-line (1l) metastatic nonsquamous (nsq) non-small cell lung cancer (nsclc) across key subgroups. Cancer Res. 2020, 80, CT216. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Vicente, D.; Tafreshi, A.; Robinson, A.; Parra, H.S.; Mazières, J.; Hermes, B.; Cicin, I.; Medgyasszay, B.; Rodríguez-Cid, J.; et al. A randomized, placebo-controlled trial of pembrolizumab plus chemotherapy in patients with metastatic squamous nsclc: Protocol-specified final analysis of keynote-407. J. Thorac. Oncol. 2020, 15, 1657–1669. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after chemoradiotherapy in stage iii non-small-cell lung cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.G.; Vansteenkiste, J.F.; Garassino, M.C.; Hui, R.; Quantin, X.; et al. Five-year survival outcomes with durvalumab after chemoradiotherapy in unresectable stage iii nsclc: An update from the pacific trial. J. Clin. Oncol. 2021, 39. [Google Scholar] [CrossRef]
- Gennen, K.; Käsmann, L.; Taugner, J.; Eze, C.; Karin, M.; Roengvoraphoj, O.; Neumann, J.; Tufman, A.; Orth, M.; Reu, S.; et al. Prognostic value of pd-l1 expression on tumor cells combined with cd8+ til density in patients with locally advanced non-small cell lung cancer treated with concurrent chemoradiotherapy. Radiat. Oncol. 2020, 15, 5. [Google Scholar] [CrossRef]
- Tokito, T.; Azuma, K.; Kawahara, A.; Ishii, H.; Yamada, K.; Matsuo, N.; Kinoshita, T.; Mizukami, N.; Ono, H.; Kage, M.; et al. Predictive relevance of pd-l1 expression combined with cd8+ til density in stage iii non-small cell lung cancer patients receiving concurrent chemoradiotherapy. Eur. J. Cancer 2016, 55, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Tufman, A.; Neumann, J.; Manapov, F.; Sellmer, L.; Jung, A.; Kauffmann-Guerrero, D.; Kahnert, K.; Mertsch, P.; Borgmeier, A.; Semrau, S.; et al. Prognostic and predictive value of pd-l1 expression and tumour infiltrating lymphocytes (tils) in locally advanced nsclc treated with simultaneous radiochemotherapy in the randomized, multicenter, phase iii german intergroup lung trial (gilt). Lung Cancer 2021, 160, 17–27. [Google Scholar] [CrossRef]
- Vrankar, M.; Kern, I.; Stanic, K. Prognostic value of pd-l1 expression in patients with unresectable stage iii non-small cell lung cancer treated with chemoradiotherapy. Radiat. Oncol. 2020, 15, 247. [Google Scholar] [CrossRef]
- Yang, J.-R.; Xu, J.-Y.; Chen, G.-C.; Yu, N.; Yang, J.; Zeng, D.-X.; Gu, M.-J.; Li, D.-P.; Zhang, Y.-S.; Qin, L.-Q. Post-diagnostic c-reactive protein and albumin predict survival in chinese patients with non-small cell lung cancer: A prospective cohort study. Sci. Rep. 2019, 9, 8143. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Boyle, T.A.; Zhou, C.; Rimm, D.L.; Hirsch, F.R. Pd-l1 expression in lung cancer. J. Thorac. Oncol. 2016, 11, 964–975. [Google Scholar] [CrossRef] [PubMed]
- Brody, R.; Zhang, Y.; Ballas, M.; Siddiqui, M.K.; Gupta, P.; Barker, C.; Midha, A.; Walker, J. Pd-l1 expression in advanced nsclc: Insights into risk stratification and treatment selection from a systematic literature review. Lung Cancer 2017, 112, 200–215. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Fu, Y.-Y.; Yue, Q.-N.; Wu, Q.; Tang, Y.; Wang, W.-Y.; Wang, Y.-S.; Jiang, L.-L. Distribution of pd-l1 expression and its relationship with clinicopathological variables: An audit from 1071 cases of surgically resected non-small cell lung cancer. Int. J. Clin. Exp. Pathol. 2019, 12, 774–786. [Google Scholar] [PubMed]
- Griesinger, F.; Eberhardt, W.; Nusch, A.; Reiser, M.; Zahn, M.O.; Maintz, C.; Bernhardt, C.; Losem, C.; Stenzinger, A.; Heukamp, L.C.; et al. Biomarker testing in non-small cell lung cancer in routine care: Analysis of the first 3,717 patients in the german prospective, observational, nation-wide crisp registry (aio-trk-0315). Lung Cancer 2021, 152, 174–184. [Google Scholar] [CrossRef]
- Alifano, M.; Falcoz, P.E.; Seegers, V.; Roche, N.; Schussler, O.; Younes, M.; Antonacci, F.; Forgez, P.; Dechartres, A.; Massard, G.; et al. Preresection serum c-reactive protein measurement and survival among patients with resectable non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2011, 142, 1161–1167. [Google Scholar] [CrossRef]
- Miyazaki, T.; Yamasaki, N.; Tsuchiya, T.; Matsumoto, K.; Kunizaki, M.; Kamohara, R.; Hatachi, G.; Doi, R.; Obata, T.; Nagayasu, T. Ratio of c-reactive protein to albumin is a prognostic factor for operable non-small-cell lung cancer in elderly patients. Surg. Today 2017, 47, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Han, H.; Duan, Q.; Khan, U.; Hu, Y.; Yao, X. Changes of serum albumin level and systemic inflammatory response in inoperable non-small cell lung cancer patients after chemotherapy. J. Cancer Res. Ther. 2014, 10, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Iivanainen, S.; Ahvonen, J.; Knuuttila, A.; Tiainen, S.; Koivunen, J.P. Elevated crp levels indicate poor progression-free and overall survival on cancer patients treated with pd-1 inhibitors. ESMO Open 2019, 4, e000531. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | N | Results |
|---|---|---|---|
| A. Tufman et al. [13] | 2021 | 78 | Tumor PD-L1 expression did not correlate with PFS or OS. |
| T. Tokito et al. [12] | 2016 | 74 | PD-L1 expression < 1% associated with favorable OS. |
| K. Gennen et al. [11] | 2020 | 31 | PD-L1 expression < 1% associated with improved OS, PFS, and local control. |
| M. Vrankar et al. [14] | 2020 | 117 | Tumor PD-L1 expression did not correlate with PFS or OS. |
| Variable | Total (n) | % |
|---|---|---|
| Patients | 99 | 100 |
| Observation period * | ||
| Alive | 32 | 32.3 |
| Dead | 67 | 67.7 |
| Age (years), median (range) | 61 (52.8–69.2) | |
| Sex | ||
| Male | 64 | 64.6 |
| Female | 35 | 35.4 |
| Pack Years | 40 | |
| Smoking Status | ||
| Light Smoker | 2 | 2.0 |
| Ex-Heavy Smoker | 48 | 48.5 |
| Current Smoker | 38 | 38.4 |
| Never Smoker | 4 | 4.0 |
| Unknown | 7 | 7.1 |
| Tumor histology type | ||
| Non-squamous | 51 | 51.5 |
| Squamous | 48 | 48.5 |
| Chemotherapy | ||
| Cisplatin | 20 | 20.2 |
| Cisplatin + Pemetrexed | 7 | 7.1 |
| Cisplatin + Vinorelbine | 58 | 58.7 |
| Cisplatin + Etoposid | 2 | 2.0 |
| Cisplatin + Paclitaxel | 3 | 3.0 |
| Carboplatin | 9 | 9.1 |
| ECOG status | ||
| 0 | 33 | 33.3 |
| 1 | 45 | 45.5 |
| 2 | 4 | 4.0 |
| Missing | 17 | 17.2 |
| Mean Albumin | 3.3 | |
| Mean CRP | 3.0 | |
| Mean Gy | 63.2 | |
| PD-L1 status | ||
| <1% | 34 | 34.3 |
| ≥1% | 65 | 65.7 |
| Multivariate Analysis | ||||
|---|---|---|---|---|
| OS | ||||
| Covariate | Category | HR | 95%-CI | p Value |
| Sex | Male | 0.293 | 0.758–2.371 | 0.132 |
| Female (RC) | ||||
| Histology | Non-squamous | 0.179 | 0.699–2.047 | 0.514 |
| Squamous (RC) | ||||
| Radiation dose (Gy) | ≥60 | 0.675 | 1.142–3.377 | 0.015 |
| <60 (RC) | ||||
| Age at diagnosis (y) | >60 | 0.497 | 0.953–2.832 | 0.074 |
| ≤60 (RC) | ||||
| ECOG | 0–1 | 0.411 | 0.749–3.035 | 0.250 |
| ≥2 (RC) | ||||
| Smoking status | never/light | 0.521 | 0.566–5.010 | 0.349 |
| current/ex heavy (RC) | ||||
| PD-L1 (%) | <50 | 0.276 | 0.742–2.339 | 0.346 |
| ≥50 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, J.N.; Roeper, J.; Heukamp, L.; Falk, M.; Willborn, K.; Griesinger, F. Evaluation of the Prognostic Impact of SP263-Evaluated PD-L1 Expression in Patients with Stage III Non-Small Cell Lung Cancer (NSLC) Treated with Radio-Chemotherapy. Biomedicines 2024, 12, 688. https://doi.org/10.3390/biomedicines12030688
Wagner JN, Roeper J, Heukamp L, Falk M, Willborn K, Griesinger F. Evaluation of the Prognostic Impact of SP263-Evaluated PD-L1 Expression in Patients with Stage III Non-Small Cell Lung Cancer (NSLC) Treated with Radio-Chemotherapy. Biomedicines. 2024; 12(3):688. https://doi.org/10.3390/biomedicines12030688
Chicago/Turabian StyleWagner, Jan Nicolai, Julia Roeper, Lukas Heukamp, Markus Falk, Kay Willborn, and Frank Griesinger. 2024. "Evaluation of the Prognostic Impact of SP263-Evaluated PD-L1 Expression in Patients with Stage III Non-Small Cell Lung Cancer (NSLC) Treated with Radio-Chemotherapy" Biomedicines 12, no. 3: 688. https://doi.org/10.3390/biomedicines12030688