
Role of Four-Chamber Heart Ultrasound Images in Automatic Assessment of Fetal Heart: A Systematic Understanding

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
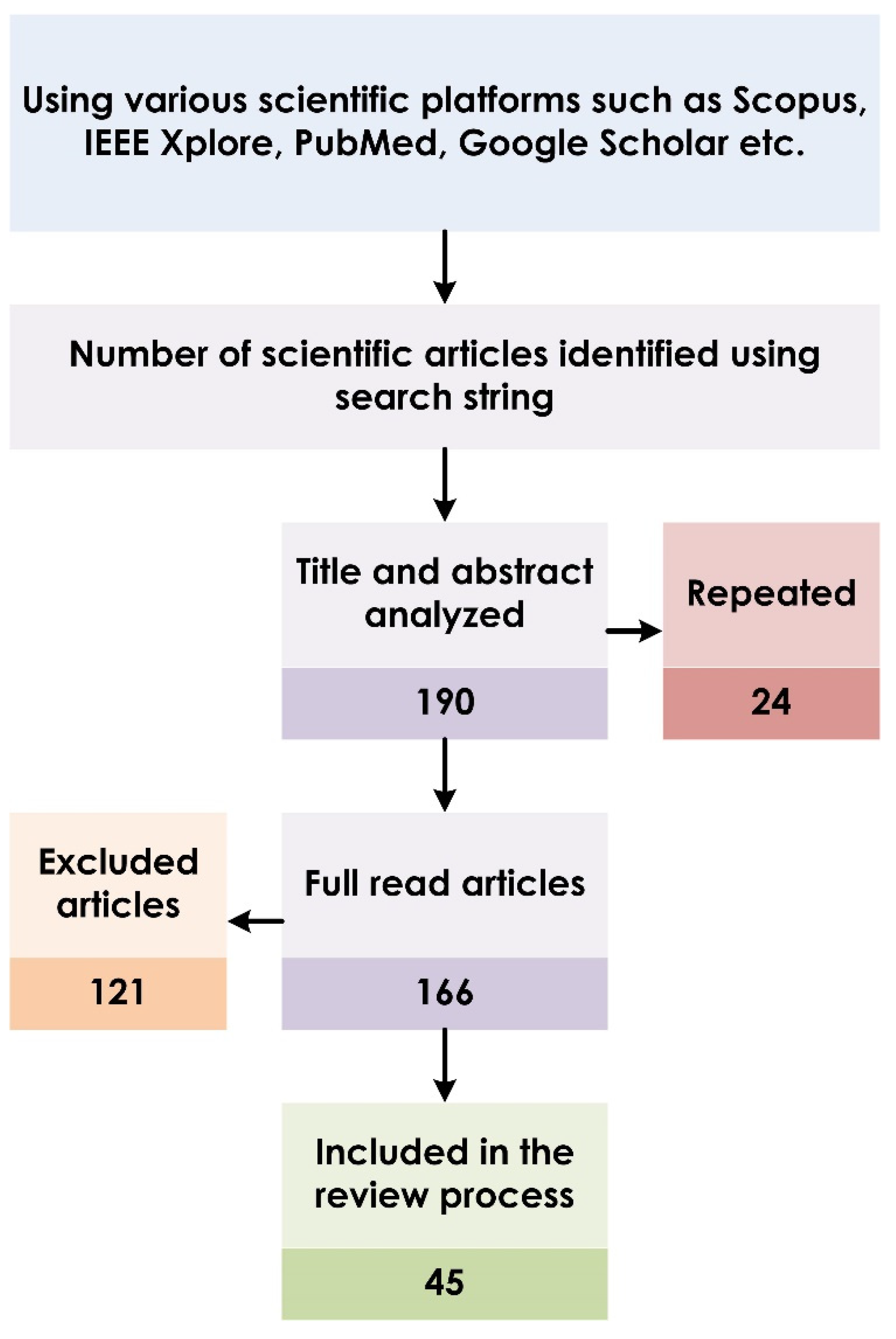
2. Article Selection for Systematic Review
3. AI in Fetal Echocardiography
3.1. Segmentation of Fetal Heart Structures
3.1.1. Nondeep Learning (non-DL) Approaches
3.1.2. Deep Learning (DL) Approaches
3.2. Classification of Fetal Abnormality
4. Analysis of CHD Using Four-Chamber US Images
4.1. Data Description
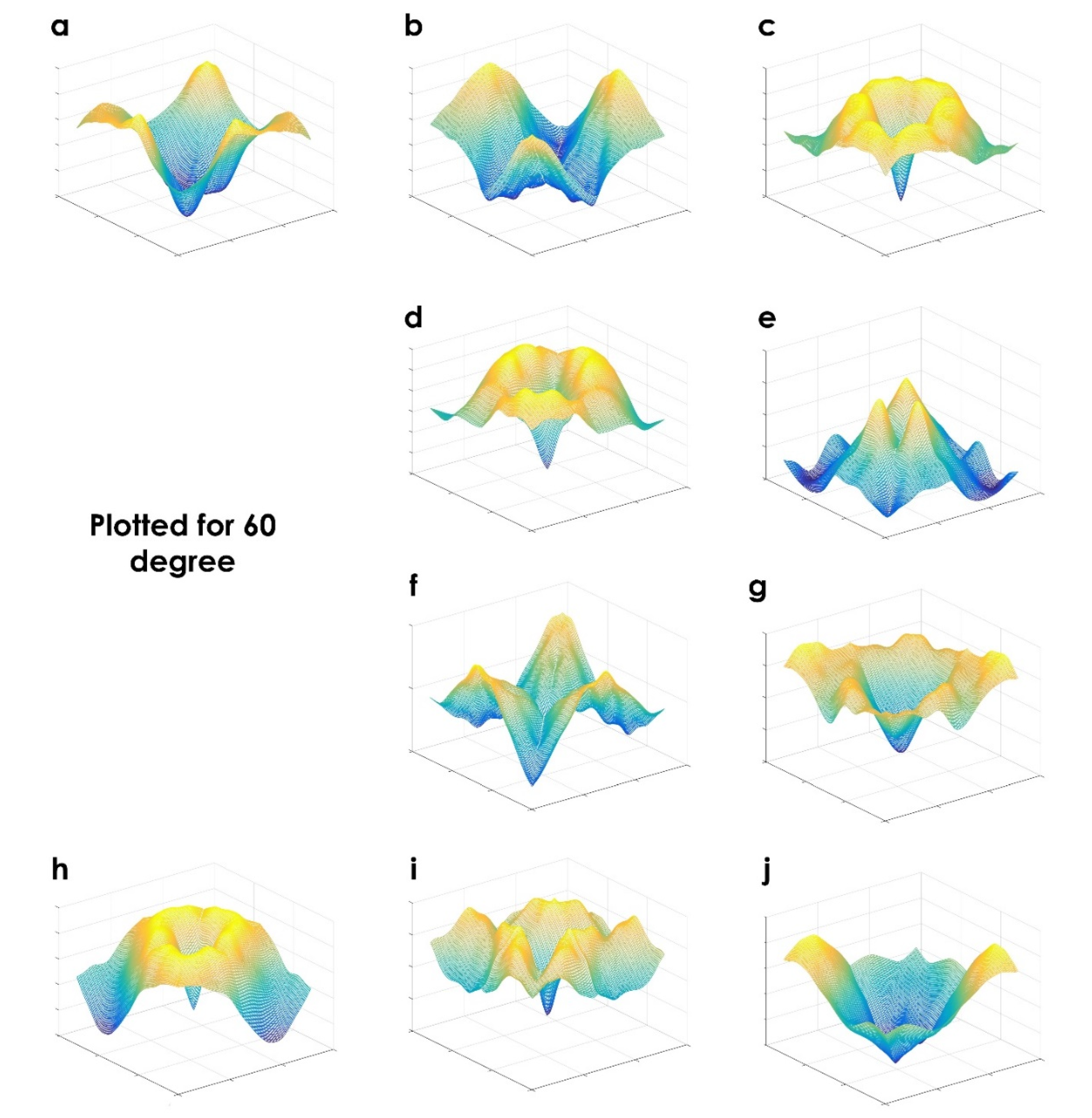
4.2. Analysis Using Various Approaches
5. Results and Discussion
5.1. Future Scope
5.2. Limitations of the Current Study
- This review considers only manuscripts written in English.
- The articles are based on specific keywords used. We may have overlooked potential studies based on non-DL and DL approaches.
- The study targets AI-based techniques for fetal heart assessment using only four-chamber US images and did not consider other views or other imaging modalities.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoffman, J.I. The global burden of congenital heart disease. Cardiovasc. J. Afr. 2013, 24, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolk, H.; Loane, M.; Garne, E. European Surveillance of Congenital Anomalies Working Group: Congenital heart defects in Europe: Prevalence and perinatal mortality, 2000 to 2005. Circulation 2011, 123, 841–849. [Google Scholar] [CrossRef] [Green Version]
- Nayak, K.; Chandra, G.S.N.; Shetty, R.; Narayan, P.K. Evaluation of fetal echocardiography as a routine antenatal screening tool for detection of congenital heart disease. Cardiovasc. Diagn. Ther. 2016, 6, 4. [Google Scholar] [CrossRef]
- Rajiah, P.; Mak, C.; Dubinksy, T.J.; Dighe, M. Ultrasound of fetal cardiac anomalies. Am. J. Roentgenol. 2011, 197, W747–W760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamm, E.R. ; Drose JAThe fetal heart In Diagnostic Ultrasound, 2nd ed.; Rumack, C.A., Wilson, S.R., Charboneau, W.J., Eds.; Mosby: St. Louis, MO, USA, 1998; pp. 1123–1159. [Google Scholar]
- Small, M.; Copel, J.A. Indications for fetal echocardiography. Pediatr. Cardiol. 2004, 25, 210–222. [Google Scholar] [CrossRef] [PubMed]
- International Society of Ultrasound in Obstetric and Gynecology. Cardiac screening examination of the fetus: Guidelines for performing the “basic” and “extended basic” cardiac scan. Ultrasound Obstet. Gynecol. 2006, 27, 107–113. [Google Scholar]
- Dudnikov, O.; Quinton, A.E.; Alphonse, J. The detection rate of first trimester ultrasound in the diagnosis of congenital heart defects: A narrative review. Sonography 2021, 8, 36–42. [Google Scholar] [CrossRef]
- Charafeddine, F.; Hachem, A.; Kibbi, N.; AbuTaqa, M.; Bitar, F.; Bulbul, Z.; El-Rassi, I.; Arabi, M. The first fetal echocardiography experience for prenatal diagnosis of congenital heart disease in lebanon: Successes and challenges. J. Saudi Heart Assoc. 2019, 31, 125–129. [Google Scholar] [CrossRef]
- Sriraam, N. A Primitive Survey on Ultrasonic Imaging-Oriented Segmentation Techniques for Detection of Fetal Cardiac Chambers. Int. J. Biomed. Clin. Eng. 2019, 8, 69–79. [Google Scholar]
- Carvalho, J.S.; Ho, S.Y.; Shinebourne, E.A. Sequential segmental analysis in complex fetal cardiac abnormalities: A logical approach to diagnosis. Ultrasound Obstet. Gynecol. 2005, 26, 105–111. [Google Scholar] [CrossRef]
- Naderi, S.; McGahan, J.P. A primer for fetal cardiac imaging: A stepwise approach for 2-D imaging. Ultrasound Q. 2008, 24, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Donofrio, M.T.; Moon-Grady, A.J.; Hornberger, L.K.; Copel, J.A.; Sklansky, M.S.; Abuhamad, A.; Cuneo, B.F.; Huhta, J.C.; Jonas, R.A.; Krishnan, A.; et al. American Heart Association Adults With Congenital Heart Disease Joint Committee of the Council on Cardiovascular Disease in the Young and Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Council on Cardiovascular and Stroke Nursing. Diagnosis and treatment of fetal cardiac disease: A scientific statement from the American Heart Association. Circulation 2014, 129, 2183–2242. [Google Scholar] [PubMed]
- Makikallio, K.; Rasanen, J.; Makikallio, T.; Vuolteenaho, O.; Huhta, J.C. Human fetal cardiovascular profile score and neonatal outcome in intrauterine growth restriction. Ultrasound Obstet. Gynecol. 2008, 31, 48–54. [Google Scholar] [CrossRef]
- Bahtiyar, M.O.; Copel, J.A. Cardiac changes in the intrauterine growth restricted fetus. Semin Perinatol. 2008, 32, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Wang, Y.; Yang, X.; Lei, B.; Liu, L.; Li, S.X.; Ni, D.; Wang, T. Deep Learning in Medical Ultrasound Analysis: A Review. Engineering 2019, 5, 261–275. [Google Scholar] [CrossRef]
- Garcia-Canadilla, P.; Sanchez-Martinez, S.; Crispi, F.; Bijnens, B. Machine learning in fetal cardiology: What to expect. Fetal Diagn. Ther. 2020, 47, 363–372. [Google Scholar] [CrossRef]
- de Siqueira, V.S.; Borges, M.M.; Furtado, R.G.; Dourado, C.N.; da Costa, R.M. Artificial intelligence applied to support medical decisions for the automatic analysis of echocardiogram images: A systematic review. Artif. Intell. Med. 2021, 120, 102165. [Google Scholar] [CrossRef] [PubMed]
- Rawat, V.; Jain, A.; Shrimali, V. Automated techniques for the interpretation of fetal abnormalities: A review. Appl. Bionics Biomech. 2018, 2018, 6452050. [Google Scholar] [CrossRef] [Green Version]
- Day, T.G.; Kainz, B.; Hajnal, J.; Razavi, R.; Simpson, J.M. Artificial intelligence, fetal echocardiography, and congenital heart disease. Prenat. Diagn. 2021, 41, 733–742. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred reporting items for systematic reviews and meta—analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Sudarshan, V.; Acharya, U.R.; Ng, E.Y.-K.; Meng, C.S.; Tan, R.S.; Ghista, D.N. Automated Identification of Infarcted Myocardium Tissue Characterization Using Ultrasound Images: A Review. IEEE Rev. Biomed. Eng. 2015, 8, 86–97. [Google Scholar] [CrossRef]
- Raghavendra, U.; Acharya, U.R.; Gudigar, A.; Shetty, R.; Krishnananda, N.; Pai, U.; Samanth, J.; Nayak, C. Automated screening of congestive heart failure using variational mode decomposition and texture features extracted from ultrasound images. Neural Comput. Appl. 2017, 28, 2869–2878. [Google Scholar] [CrossRef]
- Raghavendra, U.; Fujita, H.; Gudigar, A.; Shetty, R.; Nayak, K.; Pai, U.; Samanth, J.; Acharya, U. Automated technique for coronary artery disease characterization and classification using DD-DTDWT in ultrasound images. Biomed. Signal Processing Control. 2018, 40, 324–334. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Devasia, T.; Nayak, K.; Danish, S.M.; Kamath, G.; Samanth, J.; Pai, U.M.; Nayak, V.; Tan, R.S.; et al. Global weighted LBP based entropy features for the assessment of pulmonary hypertension. Pattern Recognit. Lett. 2019, 125, 35–41. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Samanth, J.; Gangavarapu, M.R.; Kudva, A.; Paramasivam, G.; Nayak, K.; Tan, R.-S.; Molinari, F.; Ciaccio, E.J.; et al. Automated detection of chronic kidney disease using image fusion and graph embedding techniques with ultrasound images. Biomed. Signal Process. Control 2021, 68, 102733. [Google Scholar] [CrossRef]
- Deng, L.; Yu, D. Deep learning: Methods and applications. Found. Trends Signal Process. 2014, 7, 197–387. [Google Scholar] [CrossRef] [Green Version]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, L.; Wu, L.; Wang, Y.; Ni, D.; Qin, J.; Heng, P.-A. Fine-grained recurrent neural networks for automatic prostate segmentation in ultrasound images. In Proceedings of the 31st AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017; AAAI Press: San Francisco, California USA, 2017; pp. 1633–1639. [Google Scholar]
- Deng, Y.; Wang, Y.; Chen, P. Automated detection of fetal cardiac structure from first-trimester ultrasound sequences. In Proceedings of the 2010 3rd International Conference on Biomedical Engineering and Informatics, Yantai, China, 16–18 October 2010; pp. 127–131. [Google Scholar] [CrossRef]
- Deng, Y.; Wang, Y.; Shen, Y.; Chen, P. Active cardiac model and its application on structure detection from early fetal ultrasound sequences. Comput. Med. Imaging Graph. 2012, 36, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Sampath, S.; Sivaraj, N. Fuzzy Connectedness Based Segmentation of Fetal Heart from Clinical Ultrasound Images. In Advanced Computing, Networking and Informatics—Volume 1. Smart Innovation, Systems and Technologies; Kumar Kundu, M., Mohapatra, D., Konar, A., Chakraborty, A., Eds.; Springer: Cham, Switzerland, 2014; Volume 27. [Google Scholar] [CrossRef]
- Guo, Y.; Wang, Y.; Nie, S.; Yu, J.; Chen, P. Automatic segmentation of a fetal echocardiogram using modified active appearance models and sparse representation. IEEE Trans. Biomed. Eng. 2013, 61, 1121–1133. [Google Scholar] [CrossRef] [PubMed]
- Vijayalakshmi, S.; Sriraam, N.; Suresh, S.; Muttan, S. Automated region mask for four-chamber fetal heart biometry. J. Clin. Monit. Comput. 2013, 27, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Punya Prabha, V.; Sriraam, N.; Suresh, S. Hybrid Segmentation Approach to Segment Fetal Cardiac Chambers of Ultrasound images. In Proceedings of the 2019 1st International Conference on Advanced Technologies in Intelligent Control, Environment, Computing & Communication Engineering (ICATIECE), Bangalore, India, 19–20 March 2019; pp. 331–334. [Google Scholar] [CrossRef]
- Vargas-Quintero, L.; Escalante-Ramírez, B.; Camargo Marín, L.; Guzmán Huerta, M.; Arámbula Cosio, F.; Borboa Olivares, H. Left ventricle segmentation in fetal echocardiography using a multi-texture active appearance model based on the steered Hermite transform. Comput. Methods Programs Biomed. 2016, 137, 231–245. [Google Scholar] [CrossRef]
- Bridge, C.P.; Noble, J.A. Object localisation in fetal ultrasound images using invariant features. In Proceedings of the 2015 IEEE 12th International Symposium on Biomedical Imaging (ISBI), Brooklyn, NY, USA, 16–19 April 2015; pp. 156–159. [Google Scholar] [CrossRef]
- Sardsud; Auephanwiriyakul, S.; Theera-Umpon, N.; Tongsong, T. Sardsud; Auephanwiriyakul, S.; Theera-Umpon, N.; Tongsong, T.Patch-Based Fetal Heart Chamber Segmentation in Ultrasound Sequences Using Possibilistic Clustering. In Proceedings of the 2015 Seventh International Conference on Computational Intelligence, Modelling and Simulation (CIMSim), Kuantan, Malaysia,, 27–29 July 2015; pp. 43–48. [Google Scholar] [CrossRef]
- Femina, M.A.; Raajagopalan, S.P. Anatomical structure segmentation from early fetal ultrasound sequences using global pollination CAT swarm optimizer–based Chan–Vese model. Med. Biol. Eng. Comput. 2019, 57, 1763–1782. [Google Scholar] [CrossRef] [PubMed]
- Nageswari, C.S.; Prabha, K.H. Preserving the border and curvature of fetal heart chambers through TDyWT perspective geometry wrap segmentation. Multimed. Tools Appl. 2018, 77, 10235–10250. [Google Scholar] [CrossRef]
- Jacop, R.M.R.; Prabakar, S.; Porkumaran, D.R.K. Fetal cardiac structure detection from ultrasound sequences. Int. J. Instrum. Control Autom. 2013, 2, 12–16. [Google Scholar] [CrossRef]
- Yu, L.; Guo, Y.; Wang, Y.; Yu, J.; Chen, P. Determination of fetal left ventricular volume based on two-dimensional echocardiography. J. Healthc. Eng. 2017, 9, 4797315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prabha, V.P.; Sriraam, N.; Suresh, S. Ultrasonic imaging based fetal cardiac chambers segmentation using discrete wavelet transform. In Proceedings of the 2016 International Conference on Circuits, Controls, Communications and Computing (I4C), Bangalore, India, 4–6 October 2016; pp. 1–4. [Google Scholar] [CrossRef]
- Yu, L.; Guo, Y.; Wang, Y.; Yu, J.; Chen, P. Segmentation of Fetal Left Ventricle in Echocardiographic Sequences Based on Dynamic Convolutional Neural Networks. IEEE Trans. Biomed. Eng. 2017, 64, 1886–1895. [Google Scholar] [CrossRef] [PubMed]
- Patra, A.; Noble, J.A. Multi-anatomy localization in fetal echocardiography videos. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 1761–1764. [Google Scholar]
- Xu, L.; Liu, M.; Zhang, J.; He, Y. Convolutional-neural-network-based approach for segmentation of apical four-chamber view from fetal echocardiography. IEEE Access 2020, 8, 80437–80446. [Google Scholar] [CrossRef]
- Pu, B.; Zhu, N.; Li, K.; Li, S. Fetal cardiac cycle detection in multi-resource echocardiograms using hybrid classification framework. Future Gener. Comput. Syst. 2021, 115, 825–836. [Google Scholar] [CrossRef]
- Sundaresan, V.; Bridge, C.P.; Ioannou, C.; Noble, J.A. Automated characterization of the fetal heart in ultrasound images using fully convolutional neural networks. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging, Melbourne, Australia, 18–21 April 2017; pp. 671–674. [Google Scholar] [CrossRef]
- Dozen, A.; Komatsu, M.; Sakai, A.; Komatsu, R.; Shozu, K.; Machino, H.; Yasutomi, S.; Arakaki, T.; Asada, K.; Kaneko, S.; et al. Image Segmentation of the Ventricular Septum in Fetal Cardiac Ultrasound Videos Based on Deep Learning Using Time-Series Information. Biomolecules 2020, 10, 1526. [Google Scholar] [CrossRef]
- Xu, L.; Liu, M.; Shen, Z.; Wang, H.; Liu, X.; Wang, X.; Wang, S.; Li, T.; Yu, S.; Hou, M.; et al. DW-Net: A cascaded convolutional neural network for apical four-chamber view segmentation in fetal echocardiography. Comput. Med. Imaging Graph. 2020, 80, 101690. [Google Scholar] [CrossRef]
- Nurmaini, S.; Rachmatullah, M.N.; Sapitri, A.I.; Darmawahyuni, A.; Jovandy, A.; Firdaus, F.; Tutuko, B.; Passarella, R. Accurate detection of septal defects with fetal ultrasonography images using deep learning-based multiclass instance segmentation. IEEE Access 2020, 8, 196160–196174. [Google Scholar] [CrossRef]
- Philip, M.E.; Sowmya, A.; Avnet, H.; Ferreira, A.; Stevenson, G.; Welsh, A. Convolutional Neural Networks for Automated Fetal Cardiac Assessment using 4D B-Mode Ultrasound. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 824–828. [Google Scholar] [CrossRef]
- Baumgartner, C.F.; Kamnitsas, K.; Matthew, J.; Fletcher, T.P.; Smith, S.; Koch, L.M.; Kainz, B.; Rueckert, D. SonoNet: Real-time detection and localisation of fetal standard scan planes in freehand ultrasound. IEEE Trans. Med. Imaging 2017, 36, 2204–2215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, S.; Pang, S.; Luo, G.; Pan, S.; Chen, T.; Lv, Z. FLDS: An Intelligent Feature Learning Detection System for Visualizing Medical Images Supporting Fetal Four-chamber Views. IEEE J. Biomed. Health Informatics 2021. [Google Scholar] [CrossRef] [PubMed]
- Shozu, K.; Komatsu, M.; Sakai, A.; Komatsu, R.; Dozen, A.; Machino, H.; Yasutomi, S.; Arakaki, T.; Asada, K.; Kaneko, S.; et al. Model-agnostic method for thoracic wall segmentation in fetal ultrasound videos. Biomolecules 2020, 10, 1691. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, M.; Sakai, A.; Komatsu, R.; Matsuoka, R.; Yasutomi, S.; Shozu, K.; Dozen, A.; Machino, H.; Hidaka, H.; Arakaki, T.; et al. Detection of Cardiac Structural Abnormalities in Fetal Ultrasound Videos Using Deep Learning. Appl. Sci. 2021, 11, 371. [Google Scholar] [CrossRef]
- Yang, T.; Han, J.; Zhu, H.; Li, T.; Liu, X.; Gu, X.; Liu, X.; An, S.; Zhang, Y.; Zhang, Y.; et al. Segmentation of five components in four chamber view of fetal echocardiography. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; pp. 1962–1965. [Google Scholar] [CrossRef]
- Sapitri, A.I.; Nurmaini, S.; Sukemi, M.; Rachmatullah, M.N.; Darmawahyuni, A. Segmentation atrioventricular septal defect by using convolutional neural networks based on U-NET architecture. IAES Int. J. Artif. Intell. 2021, 10, 553–562. [Google Scholar] [CrossRef]
- Rachmatullah, M.N.; Nurmaini, S.; Sapitri, A.I.; Darmawahyuni, A.; Tutuko, B.; Firdaus, F. Convolutional neural network for semantic segmentation of fetal echocardiography based on four-chamber view. Bull. Electr. Eng. Inform. 2021, 10, 1987–1996. [Google Scholar] [CrossRef]
- Athira, P.; Mathew, L. Fetal anomaly detection in ultrasound image. Int. J. Comput. Appl. 2015, 129, 8887. [Google Scholar]
- Sridevi, S.; Nirmala, S. ANFIS based decision support system for prenatal detection of Truncus Arteriosus congenital heart defect. Appl. Soft Comput. 2016, 46, 577–587. [Google Scholar] [CrossRef]
- Budd, S.; Sinclair, M.; Day, T.; Vlontzos, A.; Tan, J.; Liu, T.; Matthew, J.; Skelton, E.; Simpson, J.; Razavi, R.; et al. Detecting Hypo-plastic Left Heart Syndrome in Fetal Ultrasound via Disease-Specific Atlas Maps. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Strasbourg, France, 2021; pp. 207–217. [Google Scholar]
- Gong, Y.; Zhang, Y.; Zhu, H.; Lv, J.; Cheng, Q.; Zhang, H.; He, Y.; Wang, S. Fetal Congenital Heart Disease Echocardiogram Screening Based on DGACNN: Adversarial One-Class Classification Combined with Video Transfer Learning. IEEE Trans. Med. Imaging. 2020, 39, 1206–1222. [Google Scholar] [CrossRef] [PubMed]
- Gudigar, A.; Samanth, J.; Raghavendra, U.; Dharmik, C.; Vasudeva, A.; Padmakumar, R.; Tan, R.-S.; Ciaccio, E.J.; Molinari, F.; Acharya, U.R. Local preserving class separation framework to identify gestational diabetes mellitus mother using ultrasound fetal cardiac image. IEEE Access 2020, 8, 229043–229051. [Google Scholar] [CrossRef]
- Ji, L.; Gu, Y.; Sun, K.; Yang, J.; Qiao, Y. Congenital heart disease (CHD) discrimination in fetal echocardiogram based on 3D feature fusion. In Proceedings of the 2016 IEEE International Conference on Image Processing (ICIP), Phoenix, AZ, USA, 25–28 September 2016; pp. 3419–3423. [Google Scholar] [CrossRef]
- Arnaout, R.; Curran, L.; Chinn, E.; Zhao, Y.; Moon-Grady, A.J. Deep-learning models improve on community-level diagnosis for common congenital heart disease lesions. arXiv 2018, arXiv:1809.06993v1. [Google Scholar]
- Arnaout, R.; Curran, L.; Zhao, Y.; Levine, J.C.; Chinn, E.; Moon-Grady, A.J. An ensemble of neural networks provides expert-level prenatal detection of complex congenital heart disease. Nat. Med. 2021, 27, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Chotzoglou, E.; Day, T.; Tan, J.; Matthew, J.; Lloyd, D.; Razavi, R.; Simpson, J.; Kainz, B. Learning normal appearance for fetal anomaly screening: Application to the unsupervised detection of Hypoplastic Left Heart Syndrome. J. Mach. Learn. Biomed. Imaging 2021, 12, 1–25. [Google Scholar]
- Freeman, W.T.; Adelson, E.H. The design and use of steerable filters. IEEE Trans. Pattern Anal. Mach. Intell. 1991, 13, 891–906. [Google Scholar] [CrossRef]
- Beil, W. Steerable filters and invariance theory. Pattern Recognit. Lett. 1994, 15, 453–460. [Google Scholar] [CrossRef]
- Oliva, A.; Torralba, A. Modeling the shape of the scene: A holistic representation of the spatial envelope. Int. J. Compu.t Vis. 2001, 42, 145–175. [Google Scholar] [CrossRef]
- Chua, K.C.; Chandran, V.; Acharya, U.R.; Lim, C.M. Application of higher order statistics/spectra in biomedical signals—A review. Med. Eng. Phys. 2010, 32, 679–689. [Google Scholar] [CrossRef] [Green Version]
- Oliva, A.; Torralba, A.B.; Guerin-Dugue, A.; Herault, J. Global semantic classification of scenes using power spectrum templates. In Proceedings of the 1999 International Conference on Challenge of Image retrieval, Swindon, UK, 25–26 February 1999; pp. 1–12. [Google Scholar]
- Siagian, C.; Itti, L. Rapid biologically-inspired scene classification using features shared with visual attention. IEEE Trans. Pattern Anal. Mach. Intell. 2007, 29, 300–312. [Google Scholar] [CrossRef]
- Raghavendra, U.; Acharya, U.R.; Fujita, H.; Gudigar, A.; Tan, J.H.; Chokkadi, S. Application of Gabor wavelet and locality sensitive discriminant analysis for automated identification of breast cancer using digitized mammogram images. Appl. Soft Comput. 2016, 46, 151–161. [Google Scholar] [CrossRef]
- Fujita, H.; Raghavendra, U.; Gudigar, A.; Vadakkepat, V.V.; Acharya, U.R. Automated Characterization of Breast Cancer Using Steerable Filters. In New Trends in Intelligent Software Methodologies, Tools and Techniques; Frontiers in Artificial Intelligence and Applications; IOS Press: Amsterdam, The Netherlands, 2017; Volume 297, pp. 321–327. [Google Scholar] [CrossRef]
- Ghasemzadeh, A.; Azad, S.S.; Esmaeili, E. Breast cancer detection based on Gabor-wavelet transform and machine learning methods. Int. J. Mach. Learn. Cyber. 2019, 10, 1603–1612. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Samanth, J.; Dharmik, C.; Gangavarapu, M.R.; Nayak, K.; Ciaccio, E.J.; Tan, R.; Molinari, F.; Acharya, U.R. Novel Hypertrophic Cardiomyopathy Diagnosis Index Using Deep Features and Local Directional Pattern Techniques. J. Imaging 2022, 8, 102. [Google Scholar] [CrossRef]
- Raghavendra, U.; Bhandary, S.V.; Gudigar, A.; Acharya, U.R. Novel expert system for glaucoma identification using non-parametric spatial envelope energy spectrum with fundus images. Biocybern. Biomed. Eng. 2018, 38, 170–180. [Google Scholar] [CrossRef]
- Molinari, F.; Raghavendra, U.; Gudigar, A.; Meiburger, K.M.; Rajendra Acharya, U. An efficient data mining framework for the characterization of symptomatic and asymptomatic carotid plaque using bidimensional empirical mode decomposition technique. Med. Biol. Eng. Comput. 2018, 56, 1579–1593. [Google Scholar] [CrossRef] [PubMed]
- Gudigar, A.; Raghavendra, U.; Ciaccio, E.J.; Arunkumar, N.; Abdulhay, E.; Acharya, U.R. Automated categorization of multi-class brain abnormalities using decomposition techniques with MRI images: A comparative study. IEEE Access 2019, 7, 28498–28509. [Google Scholar] [CrossRef]
- Zhou, N.; Wang, L. A modified T-test feature selection method and its application on the HapMap genotype data. Genom. Proteom. Bioinform. 2007, 5, 242–249. [Google Scholar] [CrossRef] [Green Version]
- Glen, S. “T Test (Student’s T-Test): Definition and Examples” From StatisticsHowTo.com: Elementary Statistics for the Rest of Us! 2017. Available online: https://www.statisticshowto.com/probability-and-statistics/t-test/ (accessed on 31 January 2021).
- Haralick, R.M.; Shanmugam, K.; Dinstein, I.H. Textural features for image classification. IEEE Trans. Syst. Man Cybern. 1973, 3, 610–621. [Google Scholar] [CrossRef] [Green Version]
- Gudigar, A.; Chokkadi, S.; Raghavendra, U.; Acharya, U.R. Local texture patterns for traffic sign recognition using higher order spectra. Pattern Recognit. Lett. 2017, 94, 202–210. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Paper | Method | Goal | Dataset | Result |
|---|---|---|---|---|
| [30] | Rayleigh-trimmed anisotropic diffusion + AAM | The structure detection of the fetal heart | Images: 258 | Detection = 74 |
| [31] | Active cardiac model | The detection of cardiac structure | 738 images | Point position error = 7.11 ± 6.77 |
| [32] | PPBMLE + fuzzy connectedness | Fetal heart structure delineation | First image | DC = 0.985 |
| [33] | Improved AAM + sparse representation | The segmentation of LV | Training: 23 images Testing: 23 images | AO = 84.39 |
| [34] | Connected component analysis | Heart detection | 13 cine-loop sequences | |
| [35] | RG + PCM clustering | The segmentation of fetal heart chambers | Images: 93 | |
| [36] | Multitexture AAM with HT | The segmentation of LV | Training: 98 images Validation: 45 images | DC = 0.8631 |
| [37] | FOH + circular basis functions + SVM | Heart detection | Videos: 63 | Acc. = 88 |
| [38] | Horn–Schunck’s optical flow + PCM | Fetal heart chamber segmentation | 70 frames | Segmentation Error = 2.17% |
| [39] | Improved RCV model | The segmentation of anatomical structure | Videos: 12 subjects | SPM = more than 99.95 HF = 2.5204 ± 1.2503 |
| [40] | TDyWT | Preserving curvature and border of the chambers | Images: 100 normal and abnormal | Contrast = 85% improvement |
| [41] | k-means clustering + AAM | The detection of fetal cardiac structure | Three ultrasound sequences | |
| [42] | 16 distances from border to center + back-propagation neural network (BPNN) | LV volume prediction | 50 cases | Highest intraclass correlation coefficient and concordance correlation coefficient |
| [43] | Discrete Haar wavelet transform | Chamber segmentation | 73 cine loop sequences | LV/RV ratio = 0.97 |
| Paper | Method | Goal | Dataset | Result |
|---|---|---|---|---|
| [52] | CNN | Fetal annulus segmentation | 250 cases | DS = 0.78 |
| [46] | CU-Net + SSIM | Fetal heart segmentation | Training: 1284 Images Testing: 428 images | DS = 0.856 HF = 3.33 Pixel Acc. = 92.9 |
| [53] | CNN | Localization | 2694 examinations | Acc. = 77.8 |
| [47] | Deep learning hybrid approach | Localization of end-systolic (ES) and end-diastolic (ED) frames | 350 pregnant women | Avg. Acc. = 94.84 |
| [45] | VGG-16 + modified RCNN | The detection of anatomical structures | 91 videos from 12 subjects | Acc. = 82.31 |
| [50] | DW-Net | The segmentation of anatomical structures | 895 views | DC = 0.827 PA = 93.3 AUC = 0.990 |
| [54] | Feature learning detection system with multistage residual hybrid attention module | The detection of anatomical structures | 1250 views from 1000 healthy pregnant women | Precision = 0.919, Recall = 0.971, F1 score = 0.944, and mAP = 0.953 |
| [44] | Dynamic CNN | LV segmentation | 51 sequences | DC = 94.5 |
| [49] | Cropping–segmentation–calibration | Ventricular septum segmentation | 615 images from 211 pregnant women | mIoU = 0.5543 mDC = 0.6891 |
| [55] | Multiframe + cylinder based on ensemble learning | Thoracic wall segmentation | 538 frames from 256 normal cases | mIoU = 0.493 |
| [56] | Supervised object detection with normal data only based on CNN | The detection of structure abnormalities | 349 normal cases 14 CHD cases | Area under ROC Heart = 0.787 Vessel = 0.891 |
| [57] | DeeplabV3 + U-net | Multidisease segmentation | 602 Frames from 301 patients | mIoU = 0.768 ± 0.035 DC = 0.926 ± 0.020 for Ebstein’s anomaly |
| [58] | CNN-based U-Net | The segmentation of atrioventricular septal defect | AVSD: 337 images Normal: 332 images | DC = 96.02% |
| [51] | MRCNN | Multiclass segmentation | Images: 764 | Hole detection mIoU = 76 mAP = 99.48 DC = 87.78 |
| [59] | CNNs–U-Net and Otsu threshold | Fetal heart segmentation | Images: 519 | Mean Accuracy = 96.73 Error rate = 0.21% |
| Paper | Method | Dataset | Result | Classes |
|---|---|---|---|---|
| [60] | Patch-based WF + morphological operation + features from GLCM + BPNN | From fetal US image gallery | Correctly classified: 30 images Not correctly classified: 9 images | 3 (normal, hole in the heart, and defect in the valve.) |
| [61] | PPBMLE + fuzzy connectedness + statistical and texture features + FDR + ANFIS | Normal: 185 images TA-CHD heart: 39 images | ROC: 0.8954 F-score: 0.9673 | 2 (normal and truncus arteriosus (TA)) |
| [65] | SIFT + HOF + BoW + SVM | Normal: 240 cases Abnormal: 60 cases | Acc. (Avg.): 95.1% | 2 (normal and abnormal) |
| [66] | Deep learning model | Normal: 493 TOF: 87 HLHS: 105 | Normal heart vs. TOF: Sen: 75, Spe: 76 Normal vs. HLHS: Sen: 100, Spe: 90 | 3 (normal heart, tetralogy of Fallot (TOF), and hypoplastic left heart syndrome (HLHS)) |
| [64] | Texture features based on shearlet + LPCS + SVM | Normal: 221 images Pre-GDM/GDM: 212 images | Acc.: 98.15 PPV: 97.22 Sen: 99.05 Spe: 97.28 | 2 (normal and pre-GDM/ gestational diabetes mellitus (GDM)) |
| [63] | DGACNN | 3596 images and video slices | Acc.: 85 AUC: 0.881 | 2 (normal and diseased) |
| [62] | Atlas-ISTN + area ratios + Gaussian process | Normal: 1560 images HLHS: 68 images | AUC-ROC: 0.978 | 2 (normal and HLHS) |
| [68] | Auto-encoding generative adversarial network | Normal: 2224 cases Abnormal: 93 cases | AUC (avg.): 0.81 | 2 (normal and HLHS) |
| [67] | Ensemble of neural networks | 107,823 images | AUC: 0.99 Sen: 95 Spe: 96 NPV: 100 | 2 (normal and abnormal) |
| Gist Features | Normal | CHD | p-Value | t-Value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| g163 | 0.01452 | 0.012148 | 0.04007 | 0.004682 | 0.000232 | 5.58766 |
| g147 | 0.018778 | 0.016078 | 0.047104 | 0.003378 | 0.000282 | 5.447707 |
| g435 | 0.025952 | 0.023764 | 0.067444 | 0.005714 | 0.000359 | 5.27778 |
| g179 | 0.015138 | 0.014876 | 0.045054 | 0.005949 | 0.000364 | 5.267412 |
| g19 | 0.011812 | 0.010194 | 0.030654 | 0.003365 | 0.000417 | 5.173703 |
| g227 | 0.014975 | 0.010206 | 0.034879 | 0.003961 | 0.000421 | 5.167139 |
| g432 | 0.053077 | 0.002696 | 0.043768 | 0.002758 | 0.000473 | 5.086565 |
| g35 | 0.009664 | 0.007529 | 0.027647 | 0.004663 | 0.000512 | 5.032358 |
| g291 | 0.019373 | 0.015107 | 0.045137 | 0.004374 | 0.000578 | 4.950172 |
| g99 | 0.009573 | 0.00628 | 0.023637 | 0.003746 | 0.000697 | 4.825387 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gudigar, A.; U., R.; Samanth, J.; Vasudeva, A.; A. J., A.; Nayak, K.; Tan, R.-S.; Ciaccio, E.J.; Ooi, C.P.; Barua, P.D.; et al. Role of Four-Chamber Heart Ultrasound Images in Automatic Assessment of Fetal Heart: A Systematic Understanding. Informatics 2022, 9, 34. https://doi.org/10.3390/informatics9020034
Gudigar A, U. R, Samanth J, Vasudeva A, A. J. A, Nayak K, Tan R-S, Ciaccio EJ, Ooi CP, Barua PD, et al. Role of Four-Chamber Heart Ultrasound Images in Automatic Assessment of Fetal Heart: A Systematic Understanding. Informatics. 2022; 9(2):34. https://doi.org/10.3390/informatics9020034
Chicago/Turabian StyleGudigar, Anjan, Raghavendra U., Jyothi Samanth, Akhila Vasudeva, Ashwal A. J., Krishnananda Nayak, Ru-San Tan, Edward J. Ciaccio, Chui Ping Ooi, Prabal Datta Barua, and et al. 2022. "Role of Four-Chamber Heart Ultrasound Images in Automatic Assessment of Fetal Heart: A Systematic Understanding" Informatics 9, no. 2: 34. https://doi.org/10.3390/informatics9020034