
Ex Vivo Model to Assess the Exposure of Patients to Plasticizers from Medical Devices during Pre-CAR-T Cells’ Apheresis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Drugs and Medical Devices
2.2. Reagents
2.3. Gas Chromatography–Mass Spectrometry (GC–MS)
2.4. Methods
2.5. Analysis of Plasticizers in MDs
2.6. Analysis of Plasticizers in the Apheresis Model
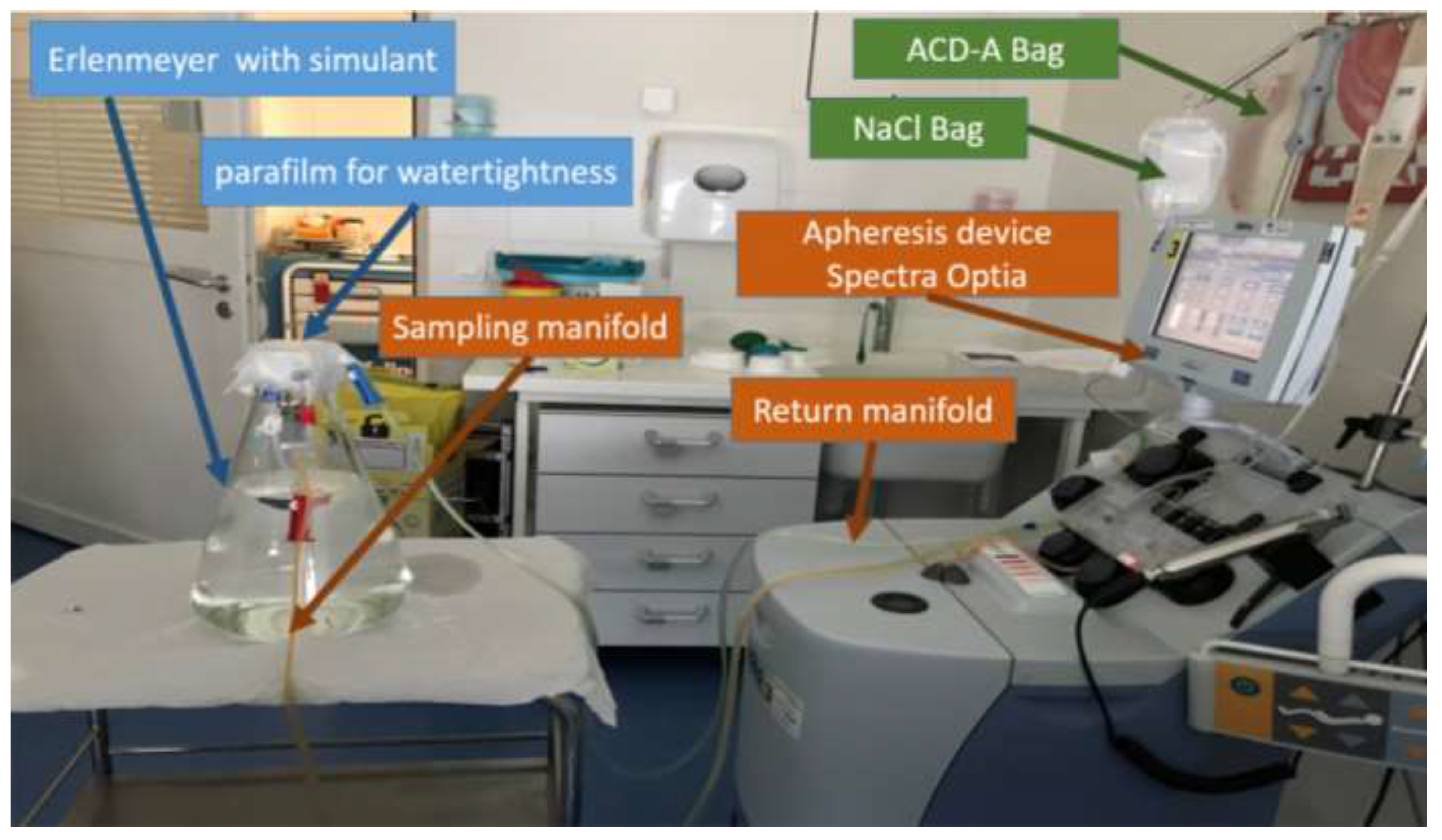
Model
- -
- Simulant:
- A 50/50 v/v mixture of absolute ethanol and water was chosen to simulate the blood due to its similar but higher capacity to extract DEHP from the PVC matrix than that of blood, along with the absence of the enzymes likely to metabolize DEHP [19];
- The simulant volume was 5 L in order to correspond to the mean blood volume of a normal adult; it was contained in a closed 5 L glass flask;
- -
- Flow rates were set up in accordance with the pre-CAR-T cells’ leukapheresis standard. Blood sampling rate was set up at 65 mL/min, and ACD-A flow rate at 1.1 mL/min;
- -
- Contact time: The collection time was dependent on the patient. In the literature, the average collection time was 2–5 h [20]; therefore, the experiment was performed for a duration of 185 min, which is the average duration of a pre-CAR-T cell collection procedure performed in our hospital (n = 7).
2.7. Extraction of Plasticizers from the Model
2.8. Identification and Quantification of Released Plasticizers
Expression of Results
- Dp = (Cp × Vsimulant)/BW;
- Cp = measured concentration of plasticizer (mg/L);
- Dp = administered daily intake of plasticizer (mg/kg/d);
- Vsimulant = volume of the simulant (5 L);
- BW = body weight (70 kg).
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Akinyemiju, T.F.; Al Lami, F.H.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018, 4, 1553. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef]
- Schuster, S.J.; Svoboda, J.; Chong, E.A.; Nasta, S.D.; Mato, A.R.; Anak, Ö.; Brogdon, J.L.; Pruteanu-Malinici, I.; Bhoj, V.; Landsburg, D.; et al. Chimeric Antigen Receptor T Cells in Refractory B-Cell Lymphomas. N. Engl. J. Med. 2017, 377, 2545–2554. [Google Scholar] [CrossRef]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Wu, X.; Sun, Z.; Xun, R.; Liu, M.; Hu, R.; Huang, J. Efficacy and Safety of CAR-T Cell Products Axicabtagene Ciloleucel, Tisagenlecleucel, and Lisocabtagene Maraleucel for the Treatment of Hematologic Malignancies: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 698607. [Google Scholar] [CrossRef] [PubMed]
- Westin, J.R.; Kersten, M.J.; Salles, G.; Abramson, J.S.; Schuster, S.J.; Locke, F.L.; Andreadis, C. Efficacy and Safety of CD19-Directed CAR-T Cell Therapies in Patients with Relapsed/Refractory Aggressive B-Cell Lymphomas: Observations from the JULIET, ZUMA-1, and TRANSCEND Trials. Am. J. Hematol. 2021, 96, 1295–1312. [Google Scholar] [CrossRef]
- Food and Drug Administration. FDA Approves Lisocabtagene Maraleucel for Relapsed or Refractory Large B-Cell Lymphoma. 2021. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-lisocabtagene-maraleucel-relapsed-or-refractory-large-b-cell-lymphoma (accessed on 9 April 2021).
- Abramson, J.S.; Palomba, M.L.; Gordon, L.I.; Lunning, M.A.; Wang, M.; Arnason, J.; Mehta, A.; Purev, E.; Maloney, D.G.; Andreadis, C.; et al. Lisocabtagene Maraleucel for Patients with Relapsed or Refractory Large B-Cell Lymphomas (TRANSCEND NHL 001): A Multicentre Seamless Design Study. Lancet 2020, 396, 839–852. [Google Scholar] [CrossRef]
- Fesnak, A.; Lin, C.; Siegel, D.L.; Maus, M.V. CAR-T Cell Therapies from the Transfusion Medicine Perspective. Transfus. Med. Rev. 2016, 30, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Tyagarajan, S.; Schmitt, D.; Acker, C.; Rutjens, E. Autologous Cryopreserved Leukapheresis Cellular Material for Chimeric Antigen Receptor–T Cell Manufacture. Cytotherapy 2019, 21, 1198–1205. [Google Scholar] [CrossRef]
- Hanawa, T.; Muramatsu, E.; Asakawa, K.; Suzuki, M.; Tanaka, M.; Kawano, K.; Seki, T.; Juni, K.; Nakajima, S. Investigation of the Release Behavior of Diethylhexyl Phthalate from the Polyvinyl-Chloride Tubing for Intravenous Administration. Int. J. Pharm. 2000, 210, 109–115. [Google Scholar] [CrossRef]
- Koch, H.M.; Bolt, H.M.; Preuss, R.; Eckstein, R.; Weisbach, V.; Angerer, J. Intravenous Exposure to Di(2-Ethylhexyl)Phthalate (DEHP): Metabolites of DEHP in Urine after a Voluntary Platelet Donation. Arch. Toxicol. 2005, 79, 689–693. [Google Scholar] [CrossRef]
- Buchta, C.; Bittner, C.; Höcker, P.; Macher, M.; Schmid, R.; Seger, C.; Dettke, M. Donor Exposure to the Plasticizer Di(2-Ethylhexyl)Phthalate during Plateletpheresis. Transfusion 2003, 43, 1115–1120. [Google Scholar] [CrossRef] [Green Version]
- European Chemicals Agency. Recommendation of the European Chemicals Agency of 10 July 2019 to Amend the Annex XIV Entries to REACH of DEHP, BBP, DBP and DIBP. Available online: https://echa.europa.eu/documents/10162/13640/axiv_amend_recommendation_phthalates_july2019_en.pdf/1889866a-bec3-fe16-6322-67c16a13b09d (accessed on 10 August 2020).
- Testai, E.; Hartemann, P.; Rastogi, S.C.; Bernauer, U.; Piersma, A.; De Jong, W.; Gulliksson, H.; Sharpe, R.; Schubert, D.; Rodríguez-Farre, E.; et al. The Safety of Medical Devices Containing DEHP Plasticized PVC or Other Plasticizers on Neonates and Other Groups Possibly at Risk (2015 Update). Regul. Toxicol. Pharmacol. 2016, 76, 209–210. [Google Scholar] [CrossRef] [PubMed]
- The Danish Environmental Protection Agency. Alternatives to Classified Phthalates in Medical Devices; Environmental Project No. 1557; The Danish Environmental Protection Agency: Copenhagen, Denmark, 2014.
- Bis(2-ethylhexyl) Phthalate—Substance Information—ECHA. Available online: https://echa.europa.eu/fr/substance-information/-/substanceinfo/100.003.829 (accessed on 9 April 2021).
- Bourdeaux, D.; Yessaad, M.; Chennell, P.; Larbre, V.; Eljezi, T.; Bernard, L.; Sautou, V. Analysis of PVC Plasticizers in Medical Devices and Infused Solutions by GC–MS. J. Pharm. Biomed. Anal. 2016, 118, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Sun, G.; Shi, Y.; Shen, Y.; Xu, K. Evaluation of the Di(2-Ethylhexyl)Phthalate Released from Polyvinyl Chloride Medical Devices That Contact Blood. SpringerPlus 2014, 3, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korell, F.; Laier, S.; Sauer, S.; Veelken, K.; Hennemann, H.; Schubert, M.-L.; Sauer, T.; Pavel, P.; Mueller-Tidow, C.; Dreger, P.; et al. Current Challenges in Providing Good Leukapheresis Products for Manufacturing of CAR-T Cells for Patients with Relapsed/Refractory NHL or ALL. Cells 2020, 9, 1225. [Google Scholar] [CrossRef]
- Thelliez, A.; Hénard, G.; Delorme, B.; Chatellier, S.; Danel, C.; Ducoroy, L.; Dupont, A.; Garrigue, D.; Genay, S.; Goossens, J.-F.; et al. Specification and Evaluation of Plasticizer Migration Simulants for Human Blood Products: A Delphi Study. Biomolecules 2021, 11, 1081. [Google Scholar] [CrossRef]
- Andra, S.S.; Makris, K.C. Thyroid Disrupting Chemicals in Plastic Additives and Thyroid Health. J. Environ. Sci. Health Part C 2012, 30, 107–151. [Google Scholar] [CrossRef]
- Huang, P.-C.; Chang, W.-H.; Wu, M.-T.; Chen, M.-L.; Wang, I.-J.; Shih, S.-F.; Hsiung, C.A.; Liao, K.-W. Characterization of Phthalate Exposure in Relation to Serum Thyroid and Growth Hormones, and Estimated Daily Intake Levels in Children Exposed to Phthalate-Tainted Products: A Longitudinal Cohort Study. Environ. Pollut. 2020, 264, 114648. [Google Scholar] [CrossRef] [PubMed]
- Engel, A.; Buhrke, T.; Imber, F.; Jessel, S.; Seidel, A.; Völkel, W.; Lampen, A. Agonistic and Antagonistic Effects of Phthalates and Their Urinary Metabolites on the Steroid Hormone Receptors ERα, ERβ, and AR. Toxicol. Lett. 2017, 277, 54–63. [Google Scholar] [CrossRef]
- Mankidy, R.; Wiseman, S.; Ma, H.; Giesy, J.P. Biological Impact of Phthalates. Toxicol. Lett. 2013, 217, 50–58. [Google Scholar] [CrossRef]
- Kambia, N.K.; Séverin, I.; Farce, A.; Moreau, E.; Dahbi, L.; Duval, C.; Dine, T.; Sautou, V.; Chagnon, M.-C. In Vitro and in Silico Hormonal Activity Studies of Di-(2-Ethylhexyl)Terephthalate, a Di-(2-Ethylhexyl)Phthalate Substitute Used in Medical Devices, and Its Metabolites. J. Appl. Toxicol. JAT 2019, 39, 1043–1056. [Google Scholar] [CrossRef] [Green Version]
- Règlement (UE) 2017/745 du Parlement Européen et du Conseil. 2017. Available online: https://eur-lex.europa.eu/legal-content/FR/TXT/PDF/?uri=CELEX:32017R0745 (accessed on 9 April 2021).
- Eljezi, T.; Pinta, P.; Nativel, F.; Richard, D.; Pinguet, J.; Roy, O.; Sautou, V.; Grimandi, G.; Moreau, E. In Vitro Cytotoxic Effects of Secondary Metabolites of DEHP and Its Alternative Plasticizers DINCH and DINP on a L929 Cell Line. Int. J. Hyg. Environ. Health 2019, 222, 583–589. [Google Scholar] [CrossRef]
- Wittassek, M.; Wiesmüller, G.A.; Koch, H.M.; Eckard, R.; Dobler, L.; Müller, J.; Angerer, J.; Schlüter, C. Internal Phthalate Exposure over the Last Two Decades—A Retrospective Human Biomonitoring Study. Int. J. Hyg. Environ. Health 2007, 210, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Canal, C.; Pinta, P.-G.; Eljezi, T.; Larbre, V.; Kauffmann, S.; Camilleri, L.; Cosserant, B.; Bernard, L.; Pereira, B.; Constantin, J.-M.; et al. Patients’ Exposure to PVC Plasticizers from ECMO Circuits. Expert Rev. Med. Devices 2018, 15, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.H.; Petricciani, J.C.; Crouch, M.L.; Wenger, S. An Evaluation of the Effects of Diethylhexyl Phthalate (DEHP) on Mitotically Capable Cells in Blood Packs. Transfusion 1974, 14, 560–566. [Google Scholar] [CrossRef]
- Rosado-Berrios, C.A.; Vélez, C.; Zayas, B. Mitochondrial Permeability and Toxicity of Diethylhexyl and Monoethylhexyl Phthalates on TK6 Human Lymphoblasts Cells. Toxicol. In Vitro 2011, 25, 2010–2016. [Google Scholar] [CrossRef] [Green Version]
- Nygaard, U.C.; Ulriksen, E.S.; Hjertholm, H.; Sonnet, F.; Bølling, A.K.; Andreassen, M.; Husøy, T.; Dirven, H. Immune Cell Profiles Associated with Measured Exposure to Phthalates in the Norwegian EuroMix Biomonitoring Study—A Mass Cytometry Approach in Toxicology. Environ. Int. 2021, 146, 106283. [Google Scholar] [CrossRef]
- Han, Y.; Wang, X.; Pang, X.; Hu, M.; Lu, Y.; Qu, J.; Chen, G. Di-(2-Ethylhexyl)-Phthalate Interferes with T-Follicular Helper Cell Differentiation and Cytokine Secretion through Signaling Lymphocytic Activation Molecule Family Member-1. J. Immunotoxicol. 2019, 16, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, U.; Sugiura, T.; Kuroda, E. Effect of Endocrine Disrupters on Immune Responses In Vitro. J. UOEH 2002, 24, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, U.; Sugiura, T.; Yoshida, Y.; Kuroda, E. Effect of Endocrine Disrupters on Thymocytes In Vitro. J. UOEH 2003, 25, 161–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, P.-S.; Lim, K.-T. Suppressive Effect of CTB Glycoprotein (75 KDa) on IL-4 Expression in Primary-Cultured Lymphocytes Treated with Di(2-Ethylhexyl) Phthalate. Naunyn. Schmiedebergs Arch. Pharmacol. 2009, 380, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Pei, X.; Duan, Z.; Ma, M.; Zhang, Y.; Guo, L. Role of Ca/CaN/NFAT Signaling in IL-4 Expression by Splenic Lymphocytes Exposed to Phthalate (2-Ethylhexyl) Ester in Spleen Lymphocytes. Mol. Biol. Rep. 2014, 41, 2129–2142. [Google Scholar] [CrossRef]
- Gimeno, P.; Thomas, S.; Bousquet, C.; Maggio, A.-F.; Civade, C.; Brenier, C.; Bonnet, P.-A. Identification and Quantification of 14 Phthalates and 5 Non-Phthalate Plasticizers in PVC Medical Devices by GC-MS. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2014, 949–950, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Rock, G.; Tocchi, M.; Ganz, P.R.; Tackaberry, E.S. Incorporation of Plasticizer into Red Cells during Storage. Transfusion 1984, 24, 493–498. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Name | Supplier | Batch Number | Shelf-Life | Use |
|---|---|---|---|---|
| ACD-A | Fresenius Kabi | FC19H21L | 2021/01 | Anticoagulation |
| 0.9% sodium chloride | B Braun Medical | 15PDD680 | 03/22 | Priming and restitution |
| Medical devices | ||||
| Spectra Optia® IDL Set (N°10315) | Terumo BCT | 1911273130 | 01/10/2021 | Apheresis device |
| Location of Cut | Detail Cut | Average Content of Plasticizer (% i.e., g/100 g of PVC) (Mean ± SD) | Relative Standard Deviation (RSD) |
|---|---|---|---|
| Inlet line (1) | Section 1 | DEHP 1 = 36.89 ± 2.03 | 5.5% |
| Section 2 | DEHP 1 = 34.43 ± 2.81 | 8.2% | |
| Section 3 | NA 2 | NA 2 | |
| Inlet line manifold (3) | Orange | DEHP 1 = 39.45 ± 1.94 DEHA 2 < LOQ | 4.9% |
| White | DEHP 1 = 40.55 ± 3.61 | 8.9% | |
| Green | DEHP 1 = 49.55 ± 1.30 | 2.6% | |
| Return line (6) | DEHP 1 = 30.69 ± 1.73 DEHA 2 < LOQ | 5.6% | |
| Manifold to channel (24) | White 1 | DEHP 1 = 29.06 ± 0.53 | 1.8% |
| White 2 | DEHP 1 = 28.69 ± 1.12 DEHA < LOQ | 3.9% | |
| Pink | DEHP 1 = 31.99 ± 1.56 DEHA 2 < LOQ | 4.9% | |
| Yellow | DEHP 1 = 27.45 ± 1.72 DEHA2 < LOQ | 6.3% | |
| Return line manifold (7) | White | DEHP 1 = 30.56 ±1.66 | 5.4% |
| Green | DEHP 1 = 31.13 ± 0.48 | 1.5% | |
| Channel (18) | NA 3 | NA 3 | |
| Anticoagulant (AC) line (9) | DEHP 1 = 32.45 ± 1.26 DEHA 2 < LOQ | 3.9% | |
| Saline line (10) | Section 1 | DEHP 1 = 59.44 ± 5.69 | 9.6% |
| Section 2 | DEHP 1 = 34.86 ± 1.56 | 4.5% | |
| Collect line (21) | DEHP 1 = 24.99 ± 0.97 DEHA 2 < LOQ | 3.9% | |
| Collection bag (20) | NA 3 | NA 3 | |
| Manifold | DEHP 1 = 28.34 ± 2.16 DEHA < LOQ | 7.6% | |
| ACD-A Bag | Spike port | DEHP 1 = 45.42 ± 20.17 | 44.4% |
| DEHP 1 = 28.29 ± 1.69 | 6.0% |
| Assay Number | CDEHP 1 in Each Sample (µg/mL) | Mean CDEHP 1 ± SD (µg/mL) | RSD | Calculated Dose (mg/kg/day) |
|---|---|---|---|---|
| 1 | 17.16 | 17.1 ± 0.70 | 4.1% | 1.2 |
| 17.82 | ||||
| 16.42 | ||||
| 2 | 19.86 | 19.9 ±0.09 | 0.4% | 1.4 |
| 20 | ||||
| 19.84 | ||||
| 3 | 22.28 | 22.3 ±0.52 | 2.3% | 1.6 |
| 21.8 | ||||
| 22.84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lautraite, R.; Bernard, L.; Halle, P.; Chennell, P.; Le Basle, Y.; Kanold, J.; Sautou, V. Ex Vivo Model to Assess the Exposure of Patients to Plasticizers from Medical Devices during Pre-CAR-T Cells’ Apheresis. Toxics 2022, 10, 79. https://doi.org/10.3390/toxics10020079
Lautraite R, Bernard L, Halle P, Chennell P, Le Basle Y, Kanold J, Sautou V. Ex Vivo Model to Assess the Exposure of Patients to Plasticizers from Medical Devices during Pre-CAR-T Cells’ Apheresis. Toxics. 2022; 10(2):79. https://doi.org/10.3390/toxics10020079
Chicago/Turabian StyleLautraite, Raphaëlle, Lise Bernard, Pascale Halle, Philip Chennell, Yoann Le Basle, Justyna Kanold, and Valérie Sautou. 2022. "Ex Vivo Model to Assess the Exposure of Patients to Plasticizers from Medical Devices during Pre-CAR-T Cells’ Apheresis" Toxics 10, no. 2: 79. https://doi.org/10.3390/toxics10020079