
Urinary Malondialdehyde (MDA) Concentrations in the General Population—A Systematic Literature Review and Meta-Analysis

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Interpretation of Findings
4.2. Heterogeneity
4.2.1. Heterogeneity in Data Collection of Demographics
4.2.2. Heterogeneity in Collection of Biological Samples
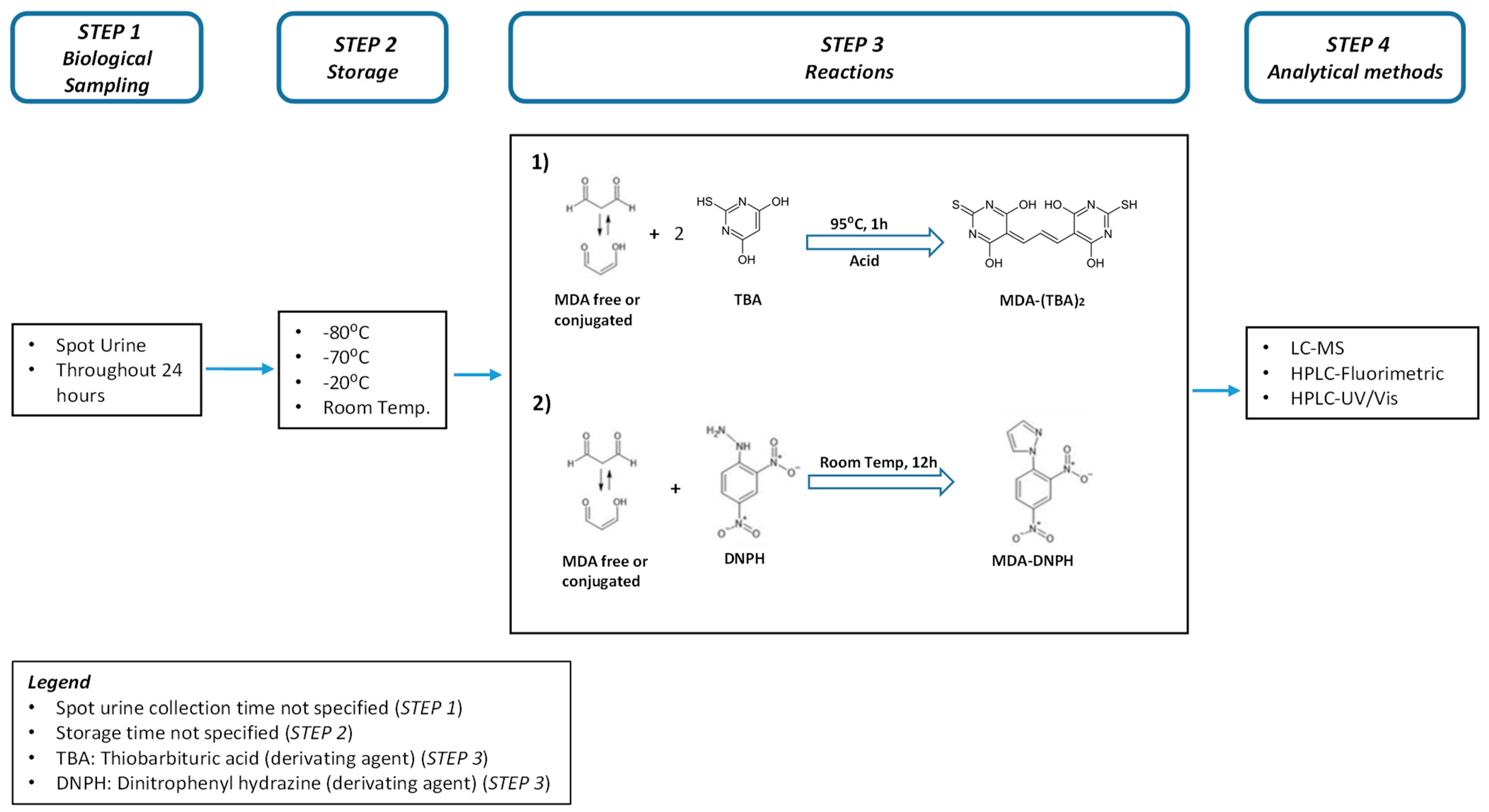
4.2.3. Heterogeneity in MDA Analysis
4.3. Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MDA | Malondialdehyde |
| TBARS | Thiobarbituric acid reactive substances |
| ROS | Reactive oxygen species |
| GM | Geometric mean |
| GSD | Geometric standard deviation |
| BMI | Body mass index |
| SD | Standard deviation |
| SEM | Standard error of the mean |
| CV | Coefficient of variation |
| IQR | Interquartile range |
References
- Lushchak, V.I. Free radicals, reactive oxygen species, oxidative stress and its classification. Chem. Biol. Interact. 2014, 224, 164–175. [Google Scholar] [CrossRef]
- Del Rio, D.; Stewart, A.J.; Pellegrini, N. A review of recent studies on malondialdehyde as toxic molecule and biological marker of oxidative stress. Nutr. Metab. Cardiovasc. Dis. 2005, 15, 316–328. [Google Scholar] [CrossRef]
- Repetto, M.; Semprine, J.; Boveris, A. Lipid Peroxidation: Chemical Mechanism, Biological Implications and Analytical Determination. In Lipid Peroxidation; Catala, A., Ed.; IntechOpen: London, UK, 2012. [Google Scholar]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid peroxidation: Production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxidative Med. Cell Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef]
- Jové, M.; Mota-Martorell, N.; Pradas, I.; Martín-Gari, M.; Ayala, V.; Pamplona, R. The Advanced Lipoxidation End-Product Malondialdehyde-Lysine in Aging and Longevity. Antioxidants 2020, 9, 1132. [Google Scholar] [CrossRef]
- Tsikas, D. Assessment of lipid peroxidation by measuring malondialdehyde (MDA) and relatives in biological samples: Analytical and biological challenges. Anal. Biochem. 2017, 524, 13–30. [Google Scholar] [CrossRef]
- Wang, J.P.; Maddalena, R.; Zheng, B.; Zai, C.; Liu, F.; Ng, J.C. Arsenicosis status and urinary malondialdehyde (MDA) in people exposed to arsenic contaminated-coal in China. Environ. Int. 2009, 35, 502–506. [Google Scholar] [CrossRef]
- García-Ruiz, I.; de la Torre, P.; Díaz, T.; Esteban, E.; Fernández, I.; Muñoz-Yagüe, T.; Solís-Herruzo, J.A. Sp1 and Sp3 Transcription Factors Mediate Malondialdehyde-induced Collagen α1(I) Gene Expression in Cultured Hepatic Stellate Cells. J. Biol. Chem. 2002, 277, 30551–30558. [Google Scholar] [CrossRef] [Green Version]
- Onyango, A.N.; Baba, N. New hypotheses on the pathways of formation of malondialdehyde and isofurans. Free Radic. Biol. Med. 2010, 49, 1594–1600. [Google Scholar] [CrossRef]
- Ito, K.; Watanabe, C.; Nakamura, A.; Oikawa-Tada, S.; Murata, M. Reduced Coenzyme Q10 Decreases Urinary 8-Oxo-7,8-Dihydro-2′-Deoxyguanosine Concentrations in Healthy Young Female Subjects. J. Med. Food 2015, 18, 835–840. [Google Scholar] [CrossRef]
- Hardt, U.; Larsson, A.; Gunnarsson, I.; Clancy, R.M.; Petri, M.; Buyon, J.P.; Silverman, G.J.; Svenungsson, E.; Grönwall, C. Autoimmune reactivity to malondialdehyde adducts in systemic lupus erythematosus is associated with disease activity and nephritis. Arthritis Res. Ther. 2018, 20, 36. [Google Scholar] [CrossRef] [Green Version]
- Duryee, M.J.; Klassen, L.W.; Schaffert, C.S.; Tuma, D.J.; Hunter, C.D.; Garvin, R.P.; Anderson, D.R.; Thiele, G.M. Malondialdehyde–acetaldehyde adduct is the dominant epitope after MDA modification of proteins in atherosclerosis. Free Radic. Biol. Med. 2010, 49, 1480–1486. [Google Scholar] [CrossRef] [Green Version]
- Cui, X.; Gong, J.; Han, H.; He, L.; Teng, Y.; Tetley, T.; Sinharay, R.; Chung, K.F.; Islam, T.; Gilliland, F.; et al. Relationship between free and total malondialdehyde, a well-established marker of oxidative stress, in various types of human biospecimens. J. Thorac. Dis. 2018, 10, 3088–3197. [Google Scholar] [CrossRef]
- Cherubini, A.; Ruggiero, C.; Polidori, M.C.; Mecocci, P. Potential markers of oxidative stress in stroke. Free Radic. Biol. Med. 2005, 39, 841–852. [Google Scholar] [CrossRef]
- Paliogiannis, P.; Fois, A.G.; Sotgia, S.; Mangoni, A.A.; Zinellu, E.; Pirina, P.; Carru, C.; Zinellu, A. Circulating malondialdehyde concentrations in patients with stable chronic obstructive pulmonary disease: A systematic review and meta-analysis. Biomark. Med. 2018, 12, 771–781. [Google Scholar] [CrossRef]
- Kurutas, E.B.; Gumusalan, Y.; Cetinkaya, A.; Dogan, E. Evaluation of method performance for oxidative stress biomarkers in urine and biological variations in urine of patients with type 2 diabetes mellitus and diabetic nephropathy. Biol. Proced. Online 2015, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- Cvetković, T.; Mitić, B.; Lazarević, G.; Vlahović, P.; Antić, S.; Stefanović, V. Oxidative stress parameters as possible urine markers in patients with diabetic nephropathy. J. Diabetes Complicat. 2009, 23, 337–342. [Google Scholar] [CrossRef]
- Gong, J.; Zhu, T.; Kipen, H.; Wang, G.; Hu, M.; Ohman-Strickland, P.; Lu, S.-E.; Zhang, L.; Wang, Y.; Zhu, P.; et al. Malondialdehyde in exhaled breath condensate and urine as a biomarker of air pollution induced oxidative stress. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 322–327. [Google Scholar] [CrossRef] [Green Version]
- Mendonça, R.; Gning, O.; Di Cesaré, C.; Lachat, L.; Bennett, N.C.; Helfenstein, F.; Glauser, G. Sensitive and selective quantification of free and total malondialdehyde in plasma using UHPLC-HRMS. J. Lipid Res. 2017, 58, 1924–1931. [Google Scholar] [CrossRef] [Green Version]
- Hemmendinger, M.; Sauvain, J.-J.; Hopf, N.B.; Wild, P.; Suárez, G.; Canu, I.G. Method Validation and Characterization of the Associated Uncertainty for Malondialdehyde Quantification in Exhaled Breath Condensate. Antioxidants 2021, 10, 1661. [Google Scholar] [CrossRef]
- Martinez-Moral, M.-P.; Kannan, K. How stable is oxidative stress level? An observational study of intra- and inter-individual variability in urinary oxidative stress biomarkers of DNA, proteins, and lipids in healthy individuals. Environ. Int. 2019, 123, 382–389. [Google Scholar] [CrossRef]
- Yuan, Y.; Hunt, R.H. Systematic Reviews: The Good, the Bad and the Ugly. Am. J. Gastroenterol. 2009, 104, 1086–1092. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Siddaway, A.P.; Wood, A.M.; Hedges, L.V. How to Do a Systematic Review: A Best Practice Guide for Conducting and Reporting Narrative Reviews, Meta-Analyses, and Meta-Syntheses. Annu. Rev. Psychol. 2019, 70, 747–770. [Google Scholar] [CrossRef]
- Hemmendinger, M.; Wild, P.; Shoman, Y.; Graille, M.; Bergamaschi, E.; Hopf, N.; Canu, I.G. Reference ranges of oxidative stress biomarkers selected for non-invasive biological surveillance of nanotechnology workers: Study protocol and meta-analysis results for 8-OHdG in exhaled breath condensate. Toxicol. Lett. 2020, 327, 41–47. [Google Scholar] [CrossRef]
- Graille, M.; Wild, P.; Sauvain, J.-J.; Hemmendinger, M.; Canu, I.G.; Hopf, N. Urinary 8-isoprostane as a biomarker for oxidative stress. A systematic review and meta-analysis. Toxicol. Lett. 2020, 328, 19–27. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Adetona, O.; Zhang, J.; Hall, D.B.; Wang, J.-S.; Vena, J.E.; Naeher, L.P. Occupational exposure to woodsmoke and oxidative stress in wildland firefighters. Sci. Total Environ. 2013, 449, 269–275. [Google Scholar] [CrossRef]
- He, L.; Cui, X.; Xia, Q.; Li, F.; Mo, J.; Gong, J.; Zhang, Y.; Zhang, J. Effects of personal air pollutant exposure on oxidative stress: Potential confounding by natural variation in melatonin levels. Int. J. Hyg. Environ. Health 2020, 223, 116–123. [Google Scholar] [CrossRef]
- Ke, Y.; Huang, L.; Xia, J.; Xu, X.; Liu, H.; Li, Y.R. Comparative study of oxidative stress biomarkers in urine of cooks exposed to three types of cooking-related particles. Toxicol. Lett. 2016, 255, 36–42. [Google Scholar] [CrossRef]
- Lin, Y.; Qiu, X.; Yu, N.; Yang, Q.; Araujo, J.A.; Zhu, Y. Urinary Metabolites of Polycyclic Aromatic Hydrocarbons and the Association with Lipid Peroxidation: A Biomarker-Based Study between Los Angeles and Beijing. Environ. Sci. Technol. 2016, 50, 3738–3745. [Google Scholar] [CrossRef]
- Sakaguchi, C.; Miura, N.; Ohara, H.; Nagata, Y. Effects of reduced exposure to cigarette smoking on changes in biomarkers of potential harm in adult smokers: Results of combined analysis of two clinical studies. Biomarkers 2019, 24, 457–468. [Google Scholar] [CrossRef]
- Weinbrenner, T.; Fitó, M.; de la Torre, R.; Sáez, G.; Rijken, P.; Tormos, C.; Coolen, S.; Albaladejo, M.F.; Abanades, S.; Schroder, H.; et al. Olive Oils High in Phenolic Compounds Modulate Oxidative/Antioxidative Status in Men. J. Nutr. 2004, 134, 2314–2321. [Google Scholar] [CrossRef] [Green Version]
- Al-Saleh, I.; Abduljabbar, M.; Al-Rouqi, R.; Elkhatib, R.; Alshabbaheen, A.; Shinwari, N. Mercury (Hg) Exposure in Breast-Fed Infants and Their Mothers and the Evidence of Oxidative Stress. Biol. Trace Elem. Res. 2013, 153, 145–154. [Google Scholar] [CrossRef]
- Chen, J.-L.; Huang, Y.-J.; Pan, C.-H.; Hu, C.-W.; Chao, M.-R. Determination of urinary malondialdehyde by isotope dilution LC-MS/MS with automated solid-phase extraction: A cautionary note on derivatization optimization. Free Radic. Biol. Med. 2011, 51, 1823–1829. [Google Scholar] [CrossRef]
- Huang, Y.-L. Lipid Peroxidation in Workers Exposed to Hexavalent Chromium. J. Toxicol. Environ. Health Part A 1999, 56, 235–247. [Google Scholar] [CrossRef]
- Jacob, R.A.; Aiello, G.M.; Stephensen, C.B.; Blumberg, J.B.; Milbury, P.E.; Wallock, L.M.; Ames, B.N. Moderate Antioxidant Supplementation Has No Effect on Biomarkers of Oxidant Damage in Healthy Men with Low Fruit and Vegetable Intakes. J. Nutr. 2003, 133, 740–743. [Google Scholar] [CrossRef] [Green Version]
- Korchazhkina, O.; Exley, C.; Spencer, S.A. Measurement by reversed-phase high-performance liquid chromatography of malondialdehyde in normal human urine following derivatisation with 2,4-dinitrophenylhydrazine. J. Chromatogr. B 2003, 794, 353–362. [Google Scholar] [CrossRef]
- Łuczaj, W.; Moniuszko, A.; Rusak, M.; Pancewicz, S.; Zajkowska, J.; Skrzydlewska, E. Lipid peroxidation products as potential bioindicators of Lyme arthritis. Eur. J. Clin. Microbiol. 2010, 30, 415–422. [Google Scholar] [CrossRef]
- Na, H.-K.; Kim, M.; Chang, S.-S.; Kim, S.-Y.; Park, J.Y.; Chung, M.W.; Yang, M. Tobacco smoking-response genes in blood and buccal cells. Toxicol. Lett. 2015, 232, 429–437. [Google Scholar] [CrossRef]
- Pan, C.-H.; Jeng, H.A.; Lai, C.-H. Biomarkers of oxidative stress in electroplating workers exposed to hexavalent chromium. J. Expo. Sci. Environ. Epidemiol. 2018, 28, 76–83. [Google Scholar] [CrossRef]
- Wilber, R.L.; Holm, P.L.; Morris, D.M.; Dallam, G.M.; Subudhi, A.W.; Murray, D.M.; Callan, S.D. Effect of FIO2 on Oxidative Stress during Interval Training at Moderate Altitude. Med. Sci. Sports Exerc. 2004, 36, 1888–1894. [Google Scholar] [CrossRef] [Green Version]
- Eom, S.-Y.; Seo, M.-N.; Lee, Y.-S.; Park, K.-S.; Hong, Y.-S.; Sohn, S.-J.; Kim, Y.-D.; Choi, B.-S.; Lim, J.-A.; Kwon, H.-J.; et al. Low-Level Environmental Cadmium Exposure Induces Kidney Tubule Damage in the General Population of Korean Adults. Arch. Environ. Contam. Toxicol. 2017, 73, 401–409. [Google Scholar] [CrossRef]
- Łuczaj, W.; Moniuszko, A.; Jarocka-Karpowicz, I.; Pancewicz, S.; Andrisic, L.; Zarkovic, N.; Skrzydlewska, E. Tick-borne encephalitis--lipid peroxidation and its consequences. Scand. J. Clin. Lab. Investig. 2016, 76, 1–9. [Google Scholar] [CrossRef]
- Moniuszko-Malinowska, A.; Łuczaj, W.; Jarocka-Karpowicz, I.; Pancewicz, S.; Zajkowska, J.; Andrisic, L.; Zarkovic, N.; Skrzydlewska, E. Lipid peroxidation in the pathogenesis of neuroborreliosis. Free Radic. Biol. Med. 2016, 96, 255–263. [Google Scholar] [CrossRef]
- Thompson, H.J.; Heimendinger, J.; Haegele, A.; Sedlacek, S.M.; Gillette, C.; O’Neill, C.; Wolfe, P.; Conry, C. Effect of increased vegetable and fruit consumption on markers of oxidative cellular damage. Carcinogenesis 1999, 20, 2261–2266. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.; Kalansooriya, A.; Holbrook, I.; Haddad, F.; Jennings, P. The relationship between chronic glycaemic control and oxidative stress in type 2 diabetes mellitus. Br. J. Biomed. Sci. 2008, 65, 71–74. [Google Scholar] [CrossRef]
- Yang, Y.J.; Hong, Y.-C.; Oh, S.-Y.; Park, M.-S.; Kim, H.; Leem, J.-H.; Ha, E.-H. Bisphenol A exposure is associated with oxidative stress and inflammation in postmenopausal women. Environ. Res. 2009, 109, 797–801. [Google Scholar] [CrossRef]
- Yu, N.; Shu, S.; Lin, Y.; She, J.; Ip, H.S.S.; Qiu, X.; Zhu, Y. High efficiency cabin air filter in vehicles reduces drivers’ roadway particulate matter exposures and associated lipid peroxidation. PLoS ONE 2017, 12, e0188498. [Google Scholar] [CrossRef]
- Adetona, A.; Martin, W.K.; Warren, S.H.; Hanley, N.M.; Adetona, O.; Zhang, J.; Simpson, C.; Paulsen, M.H.; Rathbun, S.L.; Wang, J.-S.; et al. Urinary mutagenicity and other biomarkers of occupational smoke exposure of wildland firefighters and oxidative stress. Inhal. Toxicol. 2019, 31, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R. Proinflammatory effects of oxidative stress in chronic kidney disease: Role of additional angiotensin II blockade. Am. J. Physiol. Renal Physiol. 2003, 284, F863–F869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Chase, S.D. Rapid, fluorimetric–liquid chromatographic determination of malondialdehyde in biological samples. J. Chromatogr. B 2002, 775, 121–126. [Google Scholar] [CrossRef]
- Boyle, S.P.; Dobson, V.L.; Duthie, S.; Hinselwood, D.C.; Kyle, J.; Collins, A. Bioavailability and efficiency of rutin as an antioxidant: A human supplementation study. Eur. J. Clin. Nutr. 2000, 54, 774–782. [Google Scholar] [CrossRef] [PubMed]
- Boyle, S.P.; Dobson, V.L.; Duthie, S.; Kyle, J.A.M.; Collins, A. Absorption and DNA protective effects of flavonoid glycosides from an onion meal. Eur. J. Nutr. 2000, 39, 213–223. [Google Scholar] [CrossRef]
- Domijan, A.M.; Miletić-Medved, M.; Peraica, M.; Loft, S. Malondialdehyde and 8-oxo-7.8-dihydro-2′deoxyguanosine in the urine of residents from Balkan endemic nephropathy area in Croatia—A pilot study. Coll. Antropol. 2013, 37, 1195–1198. [Google Scholar]
- Duthie, S.J.; Jenkinson, A.M.E.; Crozier, A.; Mullen, W.; Pirie, L.; Kyle, J.; Yap, L.S.; Christen, P.; Duthie, G.G. The effects of cranberry juice consumption on antioxidant status and biomarkers relating to heart disease and cancer in healthy human volunteers. Eur. J. Nutr. 2005, 45, 113–122. [Google Scholar] [CrossRef]
- Huang, M.; Choi, S.-J.; Kim, D.-W.; Kim, N.-Y.; Park, C.-H.; Yu, S.-D.; Kim, D.-S.; Park, K.-S.; Song, J.-S.; Kim, H.; et al. Risk Assessment of Low-Level Cadmium and Arsenic on the Kidney. J. Toxicol. Environ. Health Part A 2009, 72, 1493–1498. [Google Scholar] [CrossRef]
- Kim, J.-A.; Noh, S.R.; Cheong, H.-K.; Ha, M.; Eom, S.-Y.; Kim, H.; Park, M.-S.; Chu, Y.; Lee, S.-H.; Choi, K. Urinary oxidative stress biomarkers among local residents measured 6 years after the Hebei Spirit oil spill. Sci. Total Environ. 2017, 580, 946–952. [Google Scholar] [CrossRef]
- Lee, K.-H.; Shu, X.-O.; Gao, Y.-T.; Ji, B.-T.; Yang, G.; Blair, A.; Rothman, N.; Zheng, W.; Chow, W.-H.; Kang, D. Breast Cancer and Urinary Biomarkers of Polycyclic Aromatic Hydrocarbon and Oxidative Stress in the Shanghai Women’s Health Study. Cancer Epidemiol. Biomark. Prev. 2010, 19, 877–883. [Google Scholar] [CrossRef] [Green Version]
- Shih, Y.-M.; Cooke, M.; Pan, C.-H.; Chao, M.-R.; Hu, C.-W. Clinical relevance of guanine-derived urinary biomarkers of oxidative stress, determined by LC-MS/MS. Redox Biol. 2018, 20, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Łuczaj, W.; Gindzienska-Sieskiewicz, E.; Jarocka-Karpowicz, I.; Andrisic, L.; Sierakowski, S.; Zarkovic, N.; Waeg, G.; Skrzydlewska, E. The onset of lipid peroxidation in rheumatoid arthritis: Consequences and monitoring. Free Radic. Res. 2016, 50, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Bokov, A.; Chaudhuri, A.; Richardson, A. The role of oxidative damage and stress in aging. Mech. Ageing Dev. 2004, 125, 811–826. [Google Scholar] [CrossRef] [PubMed]
- Egea, J.; Fabregat, I.; Frapart, Y.M.; Ghezzi, P.; Görlach, A.; Kietzmann, T.; Kubaichuk, K.; Knaus, U.G.; Lopez, M.G.; Olaso-Gonzalez, G.; et al. European contribution to the study of ROS: A summary of the findings and prospects for the future from the COST action BM1203 (EU-ROS). Redox Biol. 2017, 13, 94–162. [Google Scholar] [CrossRef] [Green Version]
- Ruano, D. Proteostasis Dysfunction in Aged Mammalian Cells. The Stressful Role of Inflammation. Front. Mol. Biosci. 2021, 8, 658742. [Google Scholar] [CrossRef]
- Bergin, P.; Leggett, A.; Cardwell, C.R.; Woodside, J.V.; Thakkinstian, A.; Maxwell, A.P.; McKay, G.J. The effects of vitamin E supplementation on malondialdehyde as a biomarker of oxidative stress in haemodialysis patients: A systematic review and meta-analysis. BMC Nephrol. 2021, 22, 126. [Google Scholar] [CrossRef]
- Huang, H.-Y.; Appel, L.J.; Croft, K.; Miller, E.R.; Mori, T.A.; Puddey, I.B. Effects of vitamin C and vitamin E on in vivo lipid peroxidation: Results of a randomized controlled trial. Am. J. Clin. Nutr. 2002, 76, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Hu, W.; Wang, Y.; Wang, T.; Ji, Q.; Jia, Q.; Meng, T.; Ma, S.; Zhang, Z.; Li, Y.; Chen, R.; et al. Ambient particulate matter compositions and increased oxidative stress: Exposure-response analysis among high-level exposed population. Environ. Int. 2021, 147, 106341. [Google Scholar] [CrossRef]
- Jia, X.-J.; Liu, L.-X.; Tian, Y.-M.; Wang, R.; Lu, Q. The correlation between oxidative stress level and intra-abdominal fat in obese males. Medicine 2019, 98, e14469. [Google Scholar] [CrossRef]
- Zhu, M.; Liu, Z.; Guo, Y.; Sultana, M.S.; Wu, K.; Lang, X.; Lv, Q.; Huang, X.; Yi, Z.; Li, Z. Sex difference in the interrelationship between TNF-α and oxidative stress status in first-episode drug-naïve schizophrenia. J. Neuroinflamm. 2021, 18, 202. [Google Scholar] [CrossRef]
- Ide, T.; Tsutsui, H.; Ohashi, N.; Hayashidani, S.; Suematsu, N.; Tsuchihashi, M.; Tamai, H.; Takeshita, A. Greater Oxidative Stress in Healthy Young Men Compared With Premenopausal Women. Arter. Thromb. Vasc. Biol. 2002, 22, 438–442. [Google Scholar] [CrossRef] [Green Version]
- Lykkesfeldt, J.; Viscovich, M.; Poulsen, H.E. Plasma malondialdehyde is induced by smoking: A study with balanced antioxidant profiles. Br. J. Nutr. 2004, 92, 203–206. [Google Scholar] [CrossRef] [Green Version]
- Lykkesfeldt, J. Malondialdehyde as biomarker of oxidative damage to lipids caused by smoking. Clin. Chim. Acta 2007, 380, 50–58. [Google Scholar] [CrossRef]
- Li, N.; Jia, X.; Chen, C.-Y.O.; Blumberg, J.B.; Song, Y.; Zhang, W.; Zhang, X.; Ma, G.; Chen, J. Almond Consumption Reduces Oxidative DNA Damage and Lipid Peroxidation in Male Smokers. J. Nutr. 2007, 137, 2717–2722. [Google Scholar] [CrossRef] [Green Version]
- Megson, I.L.; Haw, S.J.; Newby, D.E.; Pell, J.P. Association between Exposure to Environmental Tobacco Smoke and Biomarkers of Oxidative Stress Among Patients Hospitalised with Acute Myocardial Infarction. PLoS ONE 2013, 8, e81209. [Google Scholar] [CrossRef]
- Campos, C.; Guzmán, R.; López-Fernández, E.; Casado, Á. Urinary biomarkers of oxidative/nitrosative stress in healthy smokers. Inhal. Toxicol. 2011, 23, 148–156. [Google Scholar] [CrossRef]
- Kanabrocki, E.L.; Murray, D.; Hermida, R.C.; Scott, G.S.; Bremner, W.F.; Ryan, M.D.; Ayala, D.E.; Third, J.L.; Shirazi, P.; Nemchausky, B.A.; et al. Circadian variation in oxidative stress markers in healthy and type II diabetic men. Chronobiol. Int. 2002, 19, 423–439. [Google Scholar] [CrossRef]
- Stiegel, M.A.; Pleil, J.D.; Sobus, J.R.; Angrish, M.M.; Morgan, M.K. Kidney injury biomarkers and urinary creatinine variability in nominally healthy adults. Biomarkers 2015, 20, 436–452. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GM | 95% CI | Age Group | GM | 95% CI | |
|---|---|---|---|---|---|
| Overall | 0.10 | 0.07–0.12 | <30 | 0.05 | 0.03–0.10 |
| 30–40 | 0.09 | 0.06–0.13 | |||
| 40–50 | 0.13 | 0.08–0.17 | |||
| >50 | 0.12 | 0.09–0.18 |
| logGM | Coef. | Std. Err. | P > |z| | (95% Conf. Interval) | |
|---|---|---|---|---|---|
| CatCountry | |||||
| Latin America (n = 1) | −0.324 | 0.339 | 0.340 | −0.988 | 0.341 |
| North America (n = 9) | 0.283 | 0.156 | 0.070 | −0.024 | 0.590 |
| China/Taiwan (n = 10) | 0.490 | 0.164 | 0.003 | 0.169 | 0.812 |
| Korea (n = 10) | 0.421 | 0.199 | 0.034 | 0.032 | 0.811 |
| Other Asia (n = 4) | 0.384 | 0.257 | 0.134 | −0.119 | 0.890 |
| Europe (n = 13) | 0 | (base) | |||
| SmokCat | |||||
| non-smok (n = 17) | 0 | (base) | |||
| Mixed (n = 6) | 0.008 | 0.084 | 0.922 | −0.157 | 0.174 |
| Smokers (n = 5) | 0.102 | 0.061 | 0.096 | −0.018 | 0.221 |
| Not reported (n = 19) | 0.389 | 0.141 | 0.006 | 0.113 | 0.665 |
| MeanAgeCat | |||||
| <30 (n = 8) | 0 | (base) | |||
| 30–<40 (n = 11) | 0.240 | 0.175 | 0.170 | −0.103 | 0.584 |
| 40–<50 (n = 11) | 0.369 | 0.181 | 0.042 | 0.014 | 0.723 |
| >=50 (n = 17) | 0.403 | 0.177 | 0.023 | 0.056 | 0.750 |
| _cons | −1.75 | 0.181 | 0.000 | −2.107 | −1.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toto, A.; Wild, P.; Graille, M.; Turcu, V.; Crézé, C.; Hemmendinger, M.; Sauvain, J.-J.; Bergamaschi, E.; Guseva Canu, I.; Hopf, N.B. Urinary Malondialdehyde (MDA) Concentrations in the General Population—A Systematic Literature Review and Meta-Analysis. Toxics 2022, 10, 160. https://doi.org/10.3390/toxics10040160
Toto A, Wild P, Graille M, Turcu V, Crézé C, Hemmendinger M, Sauvain J-J, Bergamaschi E, Guseva Canu I, Hopf NB. Urinary Malondialdehyde (MDA) Concentrations in the General Population—A Systematic Literature Review and Meta-Analysis. Toxics. 2022; 10(4):160. https://doi.org/10.3390/toxics10040160
Chicago/Turabian StyleToto, Antonio, Pascal Wild, Mélanie Graille, Veronica Turcu, Camille Crézé, Maud Hemmendinger, Jean-Jacques Sauvain, Enrico Bergamaschi, Irina Guseva Canu, and Nancy B. Hopf. 2022. "Urinary Malondialdehyde (MDA) Concentrations in the General Population—A Systematic Literature Review and Meta-Analysis" Toxics 10, no. 4: 160. https://doi.org/10.3390/toxics10040160