Assessment of Cardiac Autonomic Function in Relation to Methylmercury Neurotoxicity

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Extraction
2.2. Physiological Background
2.3. Interpretation of HRV Parameters
3. Results
3.1. Relations of Methylmercury to HRV
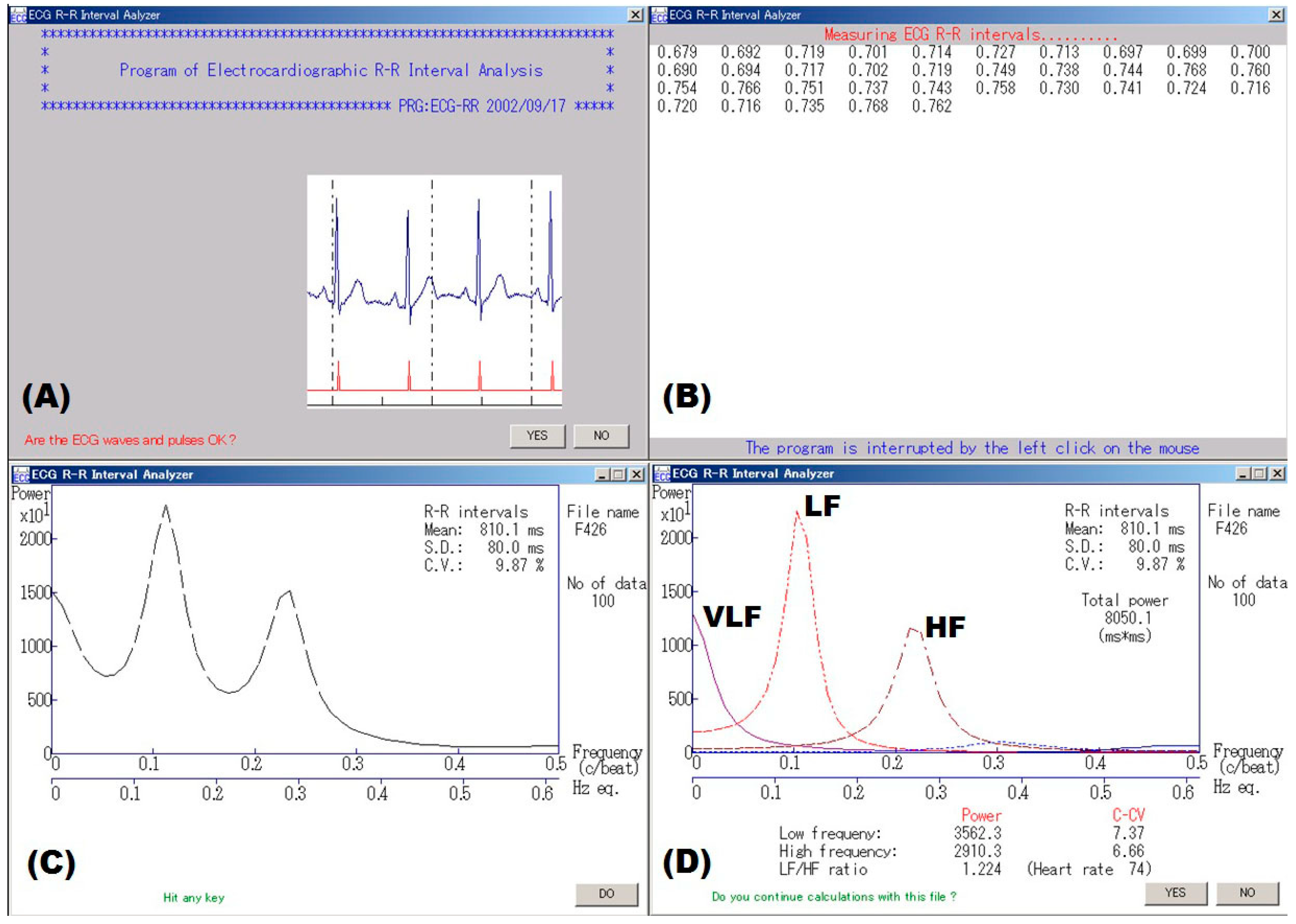
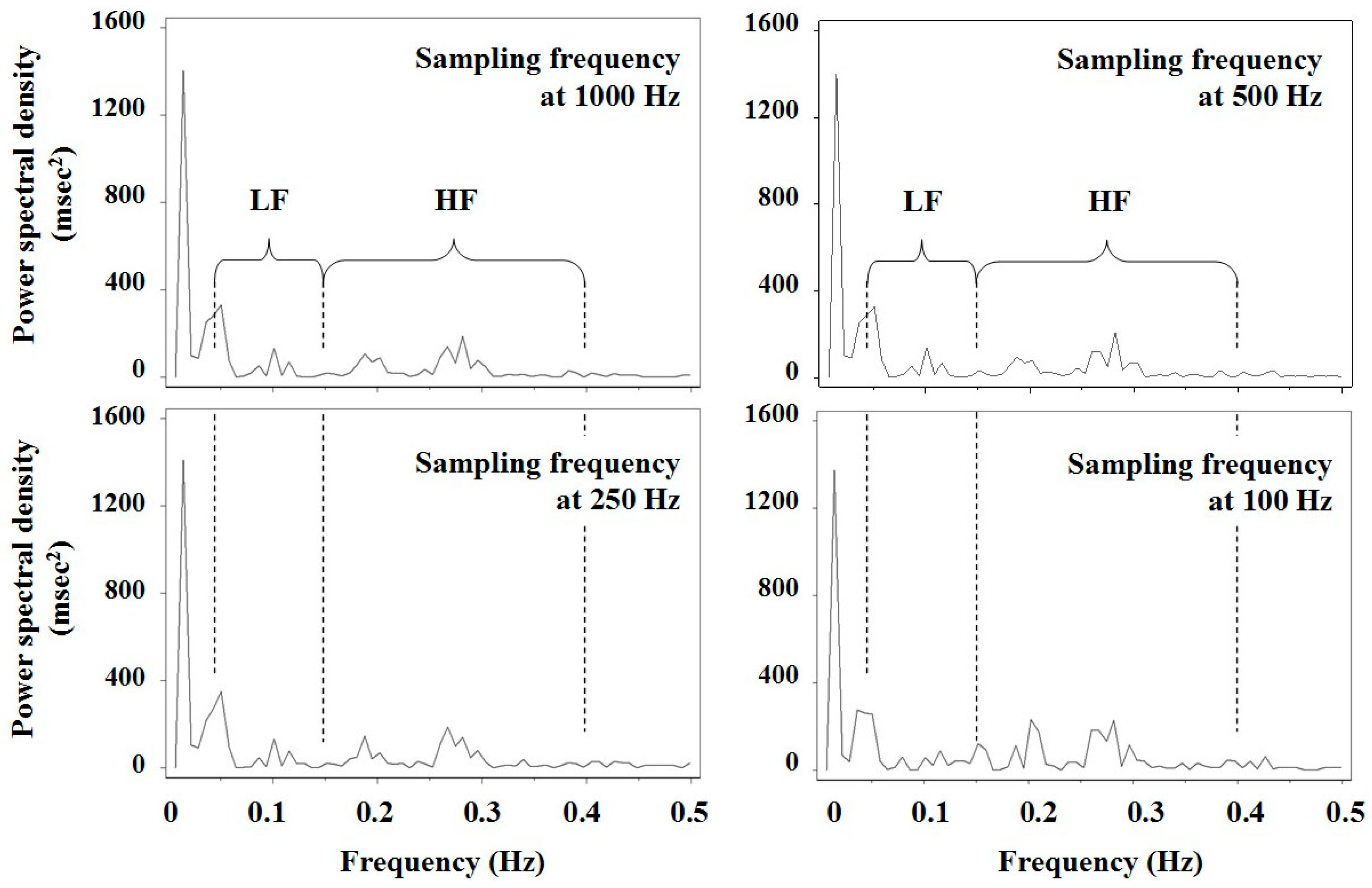
3.2. Measurement of HRV
4. Discussion
4.1. Assessment of Methylmercury Neurotoxicity
4.2. Factors Affecting the Assessment of Cardiac Autonomic Function
5. Conclusions
Author Contributions
Funding
Conflict of Interest
References
- Bannister, R.; Mathias, C.J. (Eds.) Autonomic Failure: A Textbook of Clinical Disorders of the Autonomic Nervous System, 3rd ed.; Oxford University Press: Oxford, UK, 1992. [Google Scholar]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.; Coumel, P.; Fallen, E.; Kennedy, H.; Kleiger, R.E.; et al. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Murata, K.; Araki, S. Assessment of autonomic neurotoxicity in occupational and environmental health as determined by ECG R–R interval variability: A review. Am. J. Ind. Med. 1996, 30, 155–163. [Google Scholar] [CrossRef]
- Wheeler, T.; Watkins, P.J. Cardiac denervation in diabetes. Br. Med. J. 1973, 8, 584–586. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA). Scientific opinion on the risk for public health related to the presence of mercury and methylmercury in food. EFSA J. 2012, 10, 2985. [Google Scholar] [CrossRef]
- Gribble, M.O.; Cheng, A.; Berger, R.D.; Rosman, L.; Guallar, E. Mercury exposure and heart rate variability: A systematic review. Curr. Environ. Health Rep. 2015, 2, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Oka, T.; Matsukura, M.; Okamoto, M.; Harada, N.; Kitano, T.; Miike, T.; Futatsuka, M. Autonomic nervous functions in fetal type Minamata disease patients: Assessment of heart rate variability. Tohoku J. Exp. Med. 2003, 198, 215–221. [Google Scholar] [CrossRef]
- Grandjean, P.; Murata, K.; Budtz-Jørgensen, E.; Weihe, P. Cardiac autonomic activity in methylmercury neurotoxicity: 14-year follow-up of a Faroese birth cohort. J. Pediatr. 2004, 144, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murata, K.; Sakamoto, M.; Nakai, K.; Dakeishi, M.; Iwata, T.; Liu, X.J.; Satoh, H. Subclinical effects of prenatal methylmercury exposure on cardiac autonomic function in Japanese children. Int. Arch. Occup. Environ. Health 2006, 79, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Valera, B.; Dewailly, E.; Poirier, P. Cardiac autonomic activity and blood pressure among Nunavik Inuit adults exposed to environmental mercury: A cross-sectional study. Environ. Health 2008, 7, 29. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.L.; Weihe, P.; Budtz-Jørgensen, E.; Jørgensen, P.J.; Salonen, J.T.; Tuomainen, T.P.; Murata, K.; Nielsen, H.P.; Petersen, M.S.; Askham, J.; et al. Methylmercury exposure and adverse cardiovascular effects in Faroese whaling men. Environ. Health Perspect. 2009, 117, 367–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaginuma-Sakurai, K.; Murata, K.; Shimada, M.; Nakai, K.; Kurokawa, N.; Kameo, S.; Satoh, H. Intervention study on cardiac autonomic nervous effects of methylmercury from seafood. Neurotoxicol. Teratol. 2010, 32, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Chung, H.U.; Paek, D. Low dose mercury and heart rate variability among community residents nearby to an industrial complex in Korea. Neurotoxicology 2010, 31, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Valera, B.; Dewailly, E.; Poirier, P. Impact of mercury exposure on blood pressure and cardiac autonomic activity among Cree adults (James Bay, Quebec, Canada). Environ. Res. 2011, 111, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Valera, B.; Dewailly, E.; Poirier, P.; Counil, E.; Suhas, E. Influence of mercury exposure on blood pressure, resting heart rate and heart rate variability in French Polynesians: A cross-sectional study. Environ. Health 2011, 10, 99. [Google Scholar] [CrossRef] [PubMed]
- Valera, B.; Muckle, G.; Poirier, P.; Jacobson, S.W.; Jacobson, J.L.; Dewailly, E. Cardiac autonomic activity and blood pressure among Inuit children exposed to mercury. Neurotoxicology 2012, 33, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Periard, D.; Begiraj, B.; Hayoz, D.; Viswanathan, B.; Evans, K.; Thurston, S.W.; Davidson, P.W.; Myers, G.J.; Bovet, P. Associations of baroreflex sensitivity, heart rate variability, and initial orthostatic hypotension with prenatal and recent postnatal methylmercury exposure in the Seychelles Child Development study at age 19 years. Int. J. Environ. Res. Public Health 2015, 12, 3395–3405. [Google Scholar] [CrossRef] [PubMed]
- Gump, B.B.; Dykas, M.J.; MacKenzie, J.A.; Dumas, A.K.; Hruska, B.; Ewart, C.K.; Parsons, P.J.; Palmer, C.D.; Bendinskas, K. Background lead and mercury exposures: Psychological and behavioral problems in children. Environ. Res. 2017, 158, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; Karimi, R.; Silbernagel, S.; Kostrubiak, D.; Schiavone, F.; Zhang, Q.; Yang, J.; Rashba, E.; Meliker, J.R. Mercury, omega-3 fatty acids, and seafood intake are not associated with heart rate variability or QT interval. Arch. Environ. Occup. Health 2018, 73, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Stein, P.K. Evaluation of Heart Rate Variability. 2018. Available online: https://www.uptodate.com/contents/evaluation-of-heart-rate-variability (accessed on 20 March 2017).
- Malliani, A.; Pagani, M.; Lombardi, F.; Cerutti, S. Cardiovascular neural regulation explored in the frequency domain. Circulation 1991, 84, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Yokoyama, K.; Sata, F.; Yamashita, K.; Ono, Y. Autonomic neurotoxicity of alcohol assessed by heart rate variability. J. Auton. Nerv. Syst. 1994, 48, 105–111. [Google Scholar] [CrossRef]
- Murata, K.; Araki, S. Autonomic nervous system dysfunction in workers exposed to lead, zinc, and copper in relation to peripheral nerve conduction: A study of R–R interval variability. Am. J. Ind. Med. 1991, 20, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Maeda, K. Autonomic and peripheral nervous system dysfunction in workers exposed to hand-arm vibration: A study of R–R interval variability and distribution of nerve conduction velocities. Int. Arch. Occup. Environ. Health 1991, 63, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Yokoyama, K.; Maeda, K. Autonomic and peripheral nervous system dysfunction in workers exposed to mixed organic solvent. Int. Arch. Occup. Environ. Health 1991, 63, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Yokoyama, K. Assessment of the peripheral, central and autonomic nervous system function in styrene workers. Am. J. Ind. Med. 1991, 20, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Yokoyama, K.; Tanigawa, T.; Yamashita, K.; Okajima, F.; Sakai, T.; Matsunaga, C.; Suwa, K. Cardiac autonomic dysfunction in rotogravure printers exposed to toluene in relation to peripheral nerve conduction. Ind. Health 1993, 31, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Yokoyama, K.; Yamashita, K.; Okajima, F.; Nakaaki, K. Changes in autonomic function as determined by ECG R–R interval variability in sandal, shoe and leather workers exposed to n-hexane, xylene, and toluene. Neurotoxicology 1994, 15, 867–876. [Google Scholar] [PubMed]
- Murata, K.; Araki, S.; Yokoyama, K.; Nomiyama, K.; Nomiyama, H.; Tao, Y.X.; Liu, S.J. Autonomic and central nervous system effects of lead in female glass workers in China. Am. J. Ind. Med. 1995, 28, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Okajima, F.; Nakao, M.; Suwa, K.; Matsunaga, C. Effects of occupational use of vibrating tools in the autonomic, central and peripheral nervous system. Int. Arch. Occup. Environ. Health 1997, 70, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Yokoyama, K.; Okumura, T.; Ishimatsu, S.; Takasu, N.; White, R.F. Asymptomatic sequelae to acute sarin poisoning in the central and autonomic nervous system 6 months after the Tokyo subway attack. J. Neurol. 1997, 244, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, T.; Nishikido, N.; Kobayashi, T.; Kurokawa, Y.; Kabuto, M. Commuting, overtime, and cardiac autonomic activity in Tokyo. Lancet 1997, 350, 639. [Google Scholar] [CrossRef]
- Pagani, M.; Lucini, D.; Mela, G.S.; Langewitz, W.; Malliani, A. Sympathetic overactivity in subjects complaining of unexplained fatigue. Clin. Sci. 1994, 87, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Akagi, H.; Grandjean, P.; Takizawa, T.; Weihe, P. Methylmercury dose estimation from umbilical cord concentrations in patients with Minamata disease. Environ. Res. 1998, 77, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Arai, K.; Nakagawa, Y.; Iwata, T.; Horiguchi, H.; Murata, K. Relationships between QT interval and heart rate variability at rest and the covariates in healthy young adults. Auton. Neurosci. 2013, 173, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrome, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E.; et al. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circulation Res. 1986, 59, 178–193. [Google Scholar] [CrossRef] [PubMed]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Harada, M. Minamata disease: Methylmercury poisoning in Japan caused by environmental pollution. Crit. Rev. Toxicol. 1995, 25, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F.; Araki, S.; Yokoyama, K.; Murata, K.; Sørensen, N.; Dahl, R. Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicol. Teratol. 1997, 19, 417–428. [Google Scholar] [CrossRef]
- Debes, F.; Budtz-Jørgensen, E.; Weihe, P.; White, R.F.; Grandjean, P. Impact of prenatal methylmercury exposure on neurobehavioral function at age 14 years. Neurotoxicol. Teratol. 2006, 28, 536–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandjean, P.; Satoh, H.; Murata, K.; Eto, K. Adverse effects of methylmercury: Environmental health research implications. Environ. Health Perspect. 2010, 118, 1137–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatsuta, N.; Nakai, K.; Iwai-Shimada, M.; Suzuki, T.; Satoh, H.; Murata, K. Total mercury levels in hair of children aged 7 years before and after the Great East Japan earthquake. Sci. Total Environ. 2017, 596–597, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Weihe, P.; Renzoni, A.; Debes, F.; Vasconcelos, R.; Zino, F.; Araki, S.; Jørgensen, P.J.; White, R.F.; Grandjean, P. Delayed evoked potentials in children exposed to methylmercury from seafood. Neurotoxicol. Teratol. 1999, 21, 343–348. [Google Scholar] [CrossRef]
- Murata, K.; Sakamoto, M.; Nakai, K.; Weihe, P.; Dakeishi, M.; Iwata, T.; Liu, X.J.; Ohno, T.; Kurosawa, T.; Kamiya, K.; et al. Effects of methylmercury on neurodevelopment in Japanese children in relation to the Madeiran study. Int. Arch. Occup. Environ. Health 2004, 77, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Sampei, M.; Murata, K.; Dakeishi, M.; Wood, D.C. Cardiac autonomic hypofunction in preschool children with short nocturnal sleep. Tohoku J. Exp. Med. 2006, 208, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Sampei, M.; Dakeishi, M.; Wood, D.C.; Iwata, T.; Murata, K. Spontaneous awakening from nocturnal sleep and cardiac autonomic function in preschool children. Auton. Neurosci. 2007, 133, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Yaginuma-Sakurai, K.; Murata, K.; Iwai-Shimada, M.; Nakai, K.; Kurokawa, N.; Tatsuta, N.; Satoh, H. Hair-to-blood ratio and biological half-life of mercury: Experimental study of methylmercury exposure through fish consumption in humans. J. Toxicol. Sci. 2012, 37, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Mahaffey, K.R.; Clickner, R.P.; Jeffries, R.A. Methylmercury and omega-3 fatty acids: Co-occurrence of dietary sources with emphasis on fish and shellfish. Environ. Res. 2008, 107, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Strain, J.J.; Davidson, P.W.; Bonham, M.P.; Duffy, E.M.; Stokes-Riner, A.; Thurston, S.W.; Wallace, J.M.; Robson, P.J.; Shamlaye, C.F.; Georger, L.A.; et al. Associations of maternal long-chain polyunsaturated fatty acids, methylmercury, and infant development in the Seychelles Child Development Nutrition study. Neurotoxicology 2008, 29, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Hachiya, N.; Murata, K.Y.; Nakanishi, I.; Kondo, T.; Yasutake, A.; Miyamoto, K.; Ser, P.H.; Omi, S.; Furusawa, H.; et al. Methylmercury exposure and neurological outcomes in Taiji residents accustomed to consuming whale meat. Environ. Int. 2014, 68, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Weihe, P.; Budtz-Jørgensen, E.; Jørgensen, P.J.; Grandjean, P. Delayed brainstem auditory evoked potential latencies in 14-year-old children exposed to methylmercury. J. Pediatr. 2004, 144, 177–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimomura, C.; Matsuzaka, T.; Koide, E.; Kinoshita, S.; Ono, Y.; Tsuji, Y.; Kawasaki, C.; Suzuki, Y. Spectral analysis of heart rate variability in the dysfunction of brainstem. Brain Dev. 1991, 23, 26–31. (In Japanese) [Google Scholar]
- Hayano, J.; Mukai, S.; Sakakibara, M.; Okada, A.; Takata, K.; Fujinami, T. Effects of respiratory interval on vagal modulation of heart rate. Am. J. Physiol. 1994, 267, H33–H40. [Google Scholar] [CrossRef] [PubMed]
- Merri, M.; Farden, D.C.; Mottley, J.G.; Titlebaum, E.L. Sampling frequency of the electrocardiogram for spectral analysis of the heart rate variability. IEEE Trans. Biomed. Eng. 1990, 37, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Landrigan, P.J.; Araki, S. Effects of age, heart rate, gender, tobacco and alcohol ingestion on R–R interval variability in human ECG. J. Auton. Nerv. Syst. 1992, 37, 199–206. [Google Scholar] [CrossRef]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef] [PubMed]
- Valera, B.; Suhas, E.; Counil, E.; Poirier, P.; Dewailly, E. Influence of polyunsaturated fatty acids on blood pressure, resting heart rate and heart rate variability among French Polynesians. J. Am. Coll. Nutr. 2014, 33, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Konishi, Y.; Kuwabara, K.; Hori, S. Continuous survellance of organochlorine compounds in human breast milk from 1972 to 1998 in Osaka, Japan. Arch. Environ. Contam. Toxicol. 2001, 40, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Debes, F.; Weihe, P.; Grandjean, P. Prenatal exposure to lead and cognitive deficit in 7- and 14-year-old children in the presence of concomitant exposure to similar molar concentration of methylmercury. Neurotoxicol. Teratol. 2011, 33, 205–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatsuta, N.; Kurokawa, N.; Nakai, K.; Suzuki, K.; Iwai-Shimada, M.; Murata, K.; Satoh, H. Effects of intrauterine exposures to polychlorinated biphenyls, methylmercury, and lead on birth weight in Japanese male and female newborn. Environ. Health Prev. Med. 2017, 22, 39. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Yano, E.; Shinozaki, T. Impact of shift work on cardiovascular functions in a 10-year follow-up study. Scand. J. Work Environ. Health 1999, 25, 272–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murata, K.; Yano, E.; Shinozaki, T. Cardiovascular dysfunction due to shift work. J. Occup. Enviorn. Med. 1999, 41, 748–753. [Google Scholar] [CrossRef]
- Ishii, N.; Dakeishi, M.; Sasaki, M.; Iwata, T.; Murata, K. Cardiac autonomic imbalance in female nurses with shift work. Auton. Neurosci. 2005, 122, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Rautaharju, P.M.; Surawicz, B.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Deal, B.J.; Gorgels, A.; Hancock, E.W.; Josephson, M.; Kligfield, P.; et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part IV: The ST segment, T and U waves, and the QT interval: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: Endorsed by the International Society for Computerized Electrocardiology. Circulation 2009, 119, e241–e250. [Google Scholar] [CrossRef] [PubMed]
- Maeda, E.; Iwata, T.; Murata, K. Effect of work stress and home stress on autonomic nervous function in Japanese male workers. Ind. Health 2015, 53, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Enoki, M.; Maeda, E.; Iwata, T.; Murata, K. The association between work-related stress and autonomic imbalance among call center employees in Japan. Tohoku J. Exp. Med. 2017, 243, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.; Hwangbo, E.; Lee, J.; Chon, C.-R.; Kim, P.A.; Joeong, I.-H.; Park, M.; Park, R.; Kang, S.-J.; Choi, D. Analysis of an ECG record database reveals QT interval prolongation potential of famotidine in a large Korean population. Cardiovasc. Toxicol. 2015, 15, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.M.; Schouten, E.G.; Klootwijk, P.; Pool, J.; Swenne, C.A.; Kromhout, D. Heart rate variability from short electrocardiographic recordings predicts mortality from all causes in middle-aged and elderly men: The Zutphen study. Am. J. Epidemiol. 1997, 145, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Montanez, A.; Ruskin, J.N.; Hebert, P.R.; Lamas, G.A.; Hennekens, C.H. Prolonged QTc interval and risks of total and cardiovascular mortality and sudden death in the general population. Arch. Intern. Med. 2004, 164, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Straus, S.M.; Kors, J.A.; de Bruin, M.L.; van der Hooft, C.S.; Kofman, A.; Heeringa, J.; Deckers, J.W.; Kingma, J.H.; Sturkenboom, M.C.J.M.; Stricker, B.H.C.; et al. Prolonged QTc interval and risk of sudden cardiac death in a population of older adults. J. Am. Coll. Cardiol. 2006, 47, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Soliman, E.Z.; Howard, G.; Cushman, M.; Kissela, B.; Kleindorfer, D.; Le, A.; Judd, S.; McClure, L.A.; Howard, V.J. Prolongation of QTc and risk of stroke: The REGARDS study. J. Am. Coll. Cardiol. 2012, 59, 1460–1467. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors (Year) [Ref #] | Place | Subjects | Prenatal Exposure (Total Mercury Levels) * | Postnatal Exposure (Total Mercury Levels) |
|---|---|---|---|---|
| Oka et al. (2003) [7] | Minamata, Japan | 9 FMD patients and 13 controls | ||
| Grandjean et al. (2004) [8] | Faroe Islands, Denmark | 857 children aged 7 years | GM 22.6 µg/L, IQR 13.2~40.8 µg/L in cord blood; GM 4.22 µg/g, IQR 2.55~7.68 µg/g in maternal hair | GM 2.99 µg/g, IQR 1.69~6.20 µg/g in hair |
| 857 children aged 14 years | GM 0.96 µg/g, IQR 0.45~2.29 µg/g in hair | |||
| Murata et al. (2006) [9] | Japan | 136 children | Med 0.089 µg/g, range 0.017~0.367 µg/g in cord tissue | Med 1.66 µg/g, range 0.43~6.32 µg/g in hair |
| Valera et al. (2008) [10] | Nunavik, Canada | 205 Inuit adults | GM 19.6 µg/L, range 0.5~152 µg/L in blood | |
| Choi et al. (2009) [11] | Faroe Islands, Denmark | 42 whaling men | GM 7.31 µg/g, IQR 4.52~13.4 µg/g in hair; GM 29.5 µg/L, IQR 18.7~46.1 µg/L in blood | |
| Yaginuma-Sakurai et al. (2010) [12] | Sendai, Japan | Intervention group (IG): 27 adults Control group (CG): 27 adults | IG: 2.30 ± 1.08 µg/g (Mean ± SD, 0th week), 8.76 ± 2.01 µg/g (15th week); CG: 2.27 ± 1.2 µg/g (0th week), 2.14 ± 1.03 µg/g (15th week) in hair | |
| Lim et al. (2010) [13] | South Korea | 1589 adults | GM 0.83 µg/g, IQR 0.56~1.28 µg/g in hair | |
| Valera et al. (2011) [14] | Quebec, Canada | 724 Cree adults | Med 5.7 µg/L, IQR 1.2~8.8 µg/L in blood | |
| Valera et al. (2011) [15] | French Polynesia | 101 teenagers | Med 8.5 µg/L, IQR 6.3~11.0 µg/L in blood | |
| 180 adults | Med 13.5 µg/L, IQR 8.5~22.0 µg/L in blood | |||
| Valera et al. (2012) [16] | Nunavik, Canada | 226 Inuit children | Med 16.3 µg/L, IQR 9.0~28.0 µg/L in cord blood | Med 2.9 µg/L, IQR 1.5~5.6 µg/L in blood |
| Periard et al. (2015) [17] | Seychelles | 95 adolescents | Mean 6.7 µg/g, range 0.7~21.3 µg/g in maternal hair | Mean 9.5 µg/g, range 2.0~28.1 µg/g in hair |
| Gump et al. (2017) [18] | Syracuse, NY, USA | 203 children | Mean 0.4 µg/L, range 0.01~11.65 µg/L in blood | |
| Miller et al. (2017) [19] | Long Island, NY, USA | 94 fish consumers | 8.4 ± 8.6 (Mean ± SD) µg/L in blood |
| Authors (Year) [Ref #] | Mean Age at the Time of Examination | Exposure Period | HRV Parameters | |||
|---|---|---|---|---|---|---|
| CVRR | HF-Related Parameters | LF-Related Parameters | LF/HF Ratio | |||
| Oka et al. (2003) [7] | Patients 44.3 years, controls 42.9 years | prenatal | c(±) | c(‒) | c(±) | |
| Grandjean et al. (2004) [8] | 7 years | prenatal | r(±) | r(±) | r(‒) | r(±) |
| postnatal | r(±) | r(±) | r(‒) | r(±) | ||
| 14 years | prenatal | r(‒) | r(‒) | r(‒) | r(±) | |
| postnatal | r(±) | r(±) | r(±) | r(±) | ||
| Murata et al. (2006) [9] | 6.9 years | prenatal | r(‒) | r(±) | r(+) | |
| postnatal | r(±) | r(+) | r (±) | |||
| Valera et al. (2008) [10] | 52.1 years | postnatal | r(±) | r(±) | r(±) | r(±) |
| Choi et al. (2009) [11] | 58.9 years | postnatal | r(±) | r(±) | r(±) | |
| Yaginuma-Sakurai et al. (2010) [12] | Intervention 25.2 years; control 23.7 years | postnatal | c(±) | c(±) | c(+) | c(±) |
| r(±) | r(±) | r(+) | r(±) | |||
| Lim et al. (2010) [13] | 33 years | postnatal | r(‒) | r(±) | ||
| Valera et al. (2011) [14] | 35 years | postnatal | r(+) | r(+) | r(+) | |
| Valera et al. (2011) [15] | 14.2 years | postnatal | c(‒) | c(+) | c(+) | |
| 48.6 years | postnatal | c(±) | c(±) | c(±) | ||
| Valera et al. (2012) [16] | 11.3 years | prenatal | r(±) | r(±) | r(±) | r(±) |
| postnatal | r(‒) | r(±) | r(‒) | r(±) | ||
| Periard et al. (2015) [17] | 19.5 years | prenatal | r(±) | r(±) | ||
| postnatal | r(±) | r(±) | ||||
| Gump et al. (2017) [18] | 10.6 years | postnatal | r(±) | r(±) | r(±) | |
| Miller et al. (2017) [19] | 48.9 years | postnatal | r(±) | r(±) | r(±) | |
| Parameters | Sampling Frequency | |||||
|---|---|---|---|---|---|---|
| 1000 Hz | 500 Hz | 250 Hz | 200 Hz | 125 Hz | 100 Hz | |
| RRmean (msec) | 965.1 ± 162.9 | 965.1 ± 162.9 | 965.1 ± 162.9 | 965.1 ± 162.9 | 965.2 ± 162.9 * | 965.2 ± 162.9 |
| RRSD (msec) | 51.74 ± 21.35 | 51.75 ± 21.35 | 51.75 ± 21.34 | 51.75 ± 21.33 | 51.82 ± 21.29 * | 51.80 ± 21.27 * |
| CVRR (%) | 5.321 ± 1.902 | 5.322 ± 1.903 | 5.323 ± 1.903 | 5.323 ± 1.902 | 5.330 ± 1.896 * | 5.328 ± 1.896 * |
| log10 [LF (msec2)] | 4.862 ± 0.480 | 4.862 ± 0.480 | 4.863 ± 0.478 | 4.863 ± 0.478 | 4.864 ± 0.478 | 4.858 ± 0.486 * |
| log10 [HF (msec2)] | 4.931 ± 0.537 | 4.931 ± 0.537 | 4.932 ± 0.534 | 4.932 ± 0.533 | 4.936 ± 0.525 | 4.938 ± 0.521 * |
| %LF (%) | 46.91 ± 20.01 | 46.89 ± 20.00 | 46.88 ± 19.95 | 46.88 ± 19.96 | 46.68 ± 20.06 | 46.33 ± 20.14 * |
| log10 [LF/HF ratio] | −0.069 ± 0.416 | −0.069 ± 0.416 | −0.069 ± 0.415 | −0.069 ± 0.415 | −0.073 ± 0.416 | −0.081 ± 0.420 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karita, K.; Iwata, T.; Maeda, E.; Sakamoto, M.; Murata, K. Assessment of Cardiac Autonomic Function in Relation to Methylmercury Neurotoxicity. Toxics 2018, 6, 38. https://doi.org/10.3390/toxics6030038
Karita K, Iwata T, Maeda E, Sakamoto M, Murata K. Assessment of Cardiac Autonomic Function in Relation to Methylmercury Neurotoxicity. Toxics. 2018; 6(3):38. https://doi.org/10.3390/toxics6030038
Chicago/Turabian StyleKarita, Kanae, Toyoto Iwata, Eri Maeda, Mineshi Sakamoto, and Katsuyuki Murata. 2018. "Assessment of Cardiac Autonomic Function in Relation to Methylmercury Neurotoxicity" Toxics 6, no. 3: 38. https://doi.org/10.3390/toxics6030038