
Association between Auricular Signals and the Risk Factors of Metabolic Syndrome

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Settings and Participants
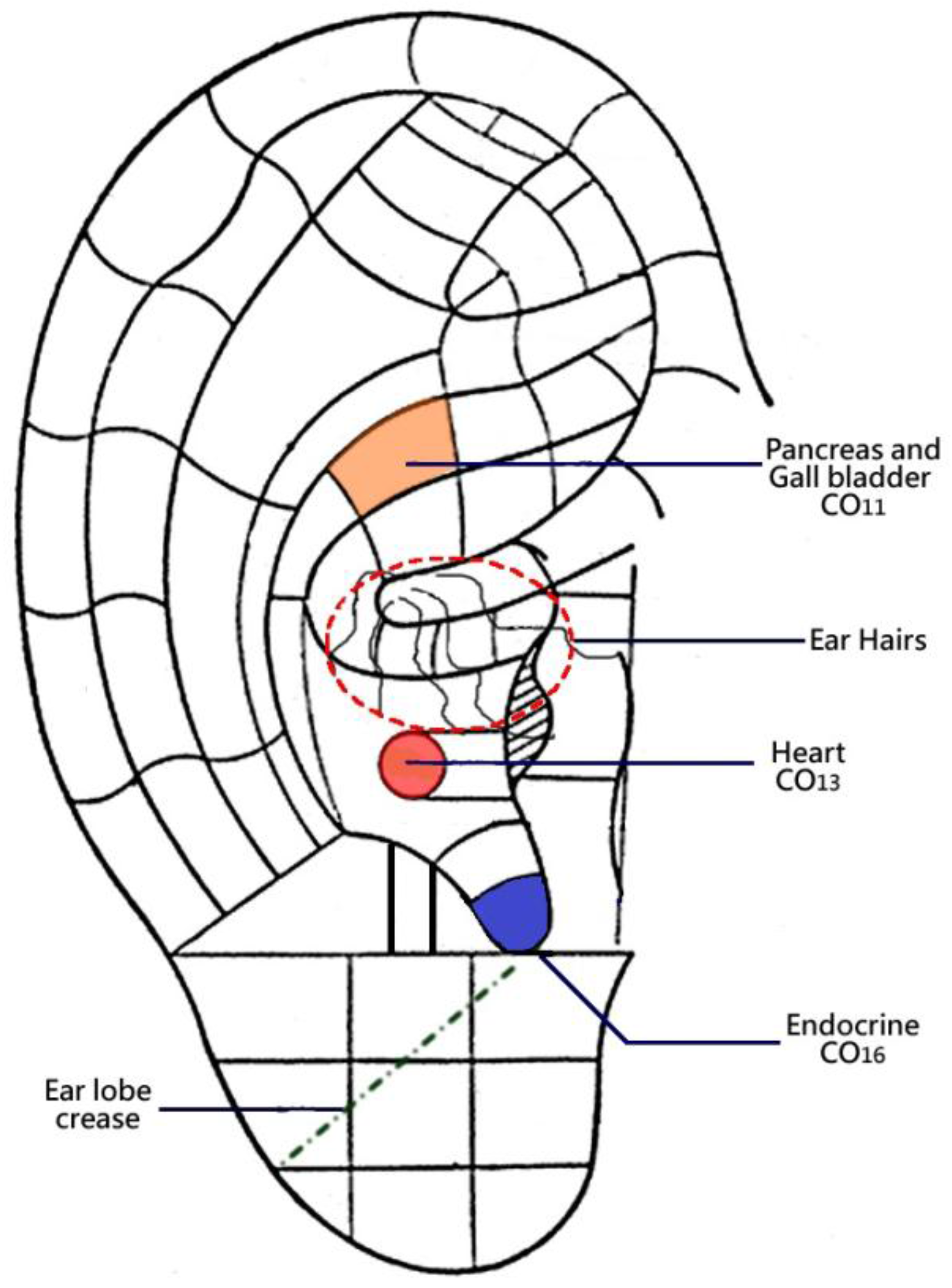
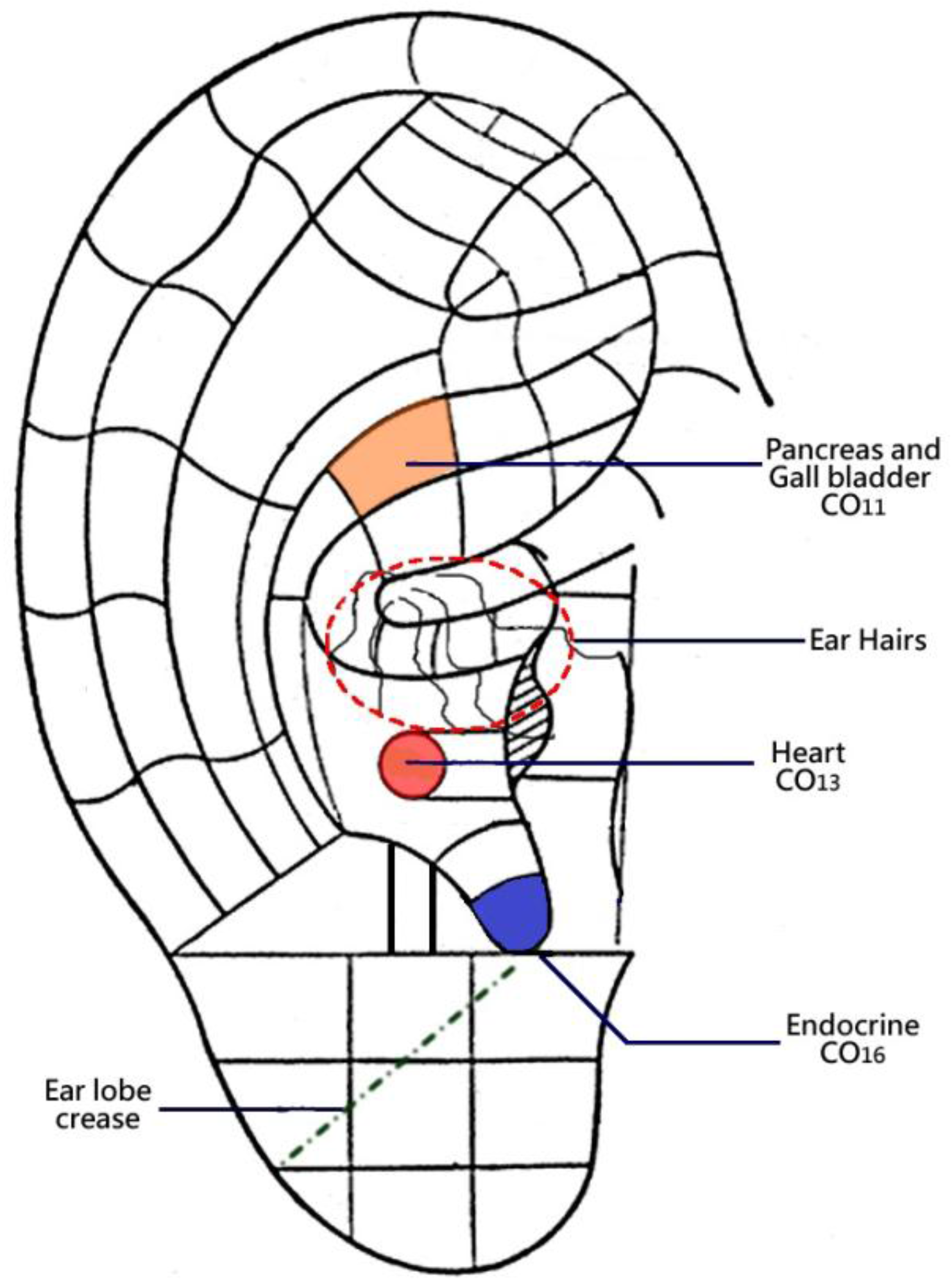
2.2. Selection of Specific Auricular Points
2.3. Auricular Assessment
2.4. Validity and Reliability
2.5. Data Analyses
2.6. Ethical Considerations
3. Results
3.1. Demographic Characteristics, Family History, and Medical Conditions of the Participants
3.2. Association of Auricular Signals between Cases and Controls
3.3. Association between Auricular Signals and Risk Factors of MS
3.4. Association between Auricular Signals under Testing
3.5. Predictive Power of Auricular Signals on the Risk of MS
4. Discussion
4.1. Visual Inspection
4.2. Electrical Skin Resistance Measurement
4.3. Tenderness Testing
4.4. Implications of the Findings
4.5. Study Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Alberti, K.G.; Zimmet, P.; Shaw, J. IDF Epidemiology Task Force Consensus Group (2005). The metabolic syndrome-a new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Sayage, P.J.; Smith, S.C.J.; et al. Diagnosis and management of the metabolic syndrome. An American Heart Association/National Heart, Lung and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Shaper, A.G.; Lennon, L.; Morris, R.W. Metabolic syndrome vs framingham risk score for prediction of coronary heart disease, stroke, and type 2 diabetes mellitus. Arch. Intern. Med. 2005, 165, 2644–2650. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.; Hosker, J.; Rudenski, A.; Naylor, B.; Treacher, D.; Turner, R. Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Salas, F.A.; Maldonado, H.J.; Martinez, B.A.; Martinez, R.G.; Jasso, S.F. The 13 C-glucose breath test is a valid non-invasive screening tool to identify metabolic syndrome in adolescents. Clin. Chem. Lab. Med. 2015, 53, 133–138. [Google Scholar]
- Simren, M.; Stotzer, P.O. Use and abuse of hydrogen breath tests. Gut 2006, 55, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Abbate, S.B. Chinese Auricular Acupuncture, 2nd ed.; CRC Press: Boca Raton, CA, USA, 2015. [Google Scholar]
- Oleson, T. Auriculotherapy Manual, 4th ed.; Churchill Livingstone Elsevier: Edinburgh, UK, 2014. [Google Scholar]
- Romoli, M. Auricular Acupuncture Diagnosis; Elsevier, Churchill Livingstone: Edinburgh, UK, 2010. [Google Scholar]
- Feng, C.X.; Bai, X.H.; Du, Y. Chinese Auricular Therapy; Scientific and Technical Documents Publishing House: Beijing, China, 1994. [Google Scholar]
- Suen, L.K.P.; Lau, Y.K.; Ma, H.C.; Lai, K.W.; Holroyd, E. Predictive value of auricular diagnosis on coronary heart disease. Evid. Based Complement. Alternat. Med. 2012. [Google Scholar] [CrossRef]
- Suen, L.K.P.; Yeh, C.H.; Kwan, J.Y.M.; Lee, P.H.; Yeung, G.S.P.; Wong, E.C.Y.; Lau, B.C.; Tsang, S.C.H.; Cheung, A.S.P.; Yeung, V.T.F. Association of auricular reflective points and status of Type 2 diabetes mellitus: A matched case-control study. Evid. Based Complement. Alternat. Med. 2015. [Google Scholar] [CrossRef] [PubMed]
- Cheung, B.M.Y.; Wat, N.M.S.; Tam, S.; Thomas, N.; Leung, G.M.; Cheng, C.H.; Woo, J.; Janus, E.D.; Lau, C.P.; Lam, T.H.; Lam, K.S.L. Components of the metabolic syndrome predictive of its development: A 6-year longitudinal study in Hong Kong Chinese. Clin. Endocrinol. 2008, 68, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.C. Auricular Diagnosis with Color Photos; Longevity Press: Bellaire, TX, USA, 1999. [Google Scholar]
- Southern California Endocrine Medical Group Common Endocrine Diseases. Available online: http://www.socalendocrine.com/Endocrine_Diseases.html (Retrieved on 5 February 2017).
- Chinese Committee of Diagnosis and Treatment of Auricular Acupuncture Points Affiliated to the China Association of Acupuncture-Moxibustion, Nomenclature and Location of Auricular Acupuncture Points of the National Standard of the People’s Republic of China; China Standard Press: Beijing, China, 2008.
- Frank, S.T. Aural sign of coronary-artery disease. N. Engl. J. Med. 1973, 289, 327–328. [Google Scholar] [PubMed]
- Pointer Plus™ (EC Certificate Registration Number: DD600751270001). Tens Plus Industrial Company: Hong Kong.
- Huang, L.C. Auricular Diagnosis and Treatment; Scientific Technology Publisher: Beijing, China, 1995. [Google Scholar]
- Suen, L.K.P.; Wong, T.K.S.; Leung, A.W.N. Is there a place for auricular therapy in the realm of nursing? Complement. Ther. Nurs. Midwifery 2001, 7, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Via-Sosa, M.A.; Toro, C.; Trave, P.; March, M.A. Screening premorbid metabolic syndrome in community pharmacies: A cross-sectional descriptive study. BMC Public Health. 2014, 14, 487. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.T.; Chan, J.C.; Tsang, L.W.; Yeung, V.T.; Chow, C.C.; Cockram, C.S. Outcomes of screening for diabetes in high-risk Hong Kong Chinese subjects. Diabetes Care 2000, 23, 1290–1294. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.L.; Zhang, C.J.; Zhang, Y.Y. Study on the relationship between ear lobe crease and coronary artery imaging in male patients with coronary heart disease. Mod. Prev. Med. 2012, 39, 1553–1555. [Google Scholar]
- Shmilovich, H.; Cheng, V.Y.; Rajani, R.; Dey, D.; Tamarappoo, B.K.; Nakazato, R.; Smith, T.W. Relation of diagnonal ear lobe crease to the presence, extent, and severity of coronary artery disease determined by coronary computed tomography angiography. Am. J. Cardiol. 2012, 109, 1283–1287. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.K.; Khamesra, R.; Mehta, L.K.; Bordia, A. Ear-lobe crease and ear-canal hair as predictors of coronary artery disease in Indian population. Indian Heart J. 1989, 41, 86–91. [Google Scholar] [PubMed]
- Wang, L. Auricular Acupuncture-Diagnostic Therapy; Science and Technology Publishing Co.: Beijing, China, 2000. [Google Scholar]
- Oleson, T.; Kroening, R.J.; Bresler, D.E. An experimental evaluation of auricular diagnosis: The somatotopic mapping of musculoskeletal pain at ear acupuncture points. Pain 1980, 9, 217–229. [Google Scholar] [CrossRef]
- Usichenko, T.I.; Lysenyukm, V.P.; Groth, M.H.; Pavolvic, D. Detection of ear acupuncture points by measuring the electrical skin resistance in patients before, during and after otheopedic surgery performed under general anesthesia. Acupunct. Electrother. Res. 2003, 28, 167–173. [Google Scholar] [CrossRef]
- Yuan, L.R. A brief introduction to ear diagnosis. Eur J Orient. Med. 1997, 34–37. [Google Scholar]
- Oleson, T. Electrophysiological research on the differential localization of auricular acupuncture points. Med. Acupunct. 1999, 11, 25–31. [Google Scholar]


{kind=link}
{kind=link}
| Variables | MS+ (n = 102) | MS− (n = 102) | Test Statistics McNemar (unless indicated) |
|---|---|---|---|
| Age
(mean 61.16, sd 10.33) | 61.47 (10.109) | 60.88 (10.551) | p > 0.05 (Paired t-test) |
| Gender
1 = male 2 = female | 51 51 | 51 51 | p > 0.05 |
| Employment status 1 = full time 2 = part time 3 = retired/housewife/unemployed | 37 16 49 | 44 13 45 | p > 0.05 |
| Smoking status
1 = never 2 = given up, occasionally, regularly | 72 30 | 76 26 | p > 0.05 |
| Alcohol consumption No Social drinker Regular | 66 31 5 | 61 33 8 | p > 0.05 (Wilcoxon) |
| Body mass index (kg/m2) | 27.06 (3.87) | 22.85 (2.64) | p < 0.001 *** (paired t-test) |
| Central obesity (male) 0 = no 1 = yes | 0 51 | 51 0 | p < 0.001 *** |
| Central obesity (female) 0 = no 1 = yes | 0 51 | 51 0 | p < 0.001 *** |
| Waist circumference (cm) | 95.58 (10.17) | 82.86 (7.41) | p < 0.001 *** (paired t-test) |
| HDL-cholesterol (mmol/L) | 1.24 (0.31) | 1.47 (0.42) | p < 0.001 *** (paired t-test) |
| LDL-cholesterol (mmol/L) | 2.84 (1.04) | 2.92 (0.96) | p > 0.05 (paired t-test) |
| Triglycerides (mmol/L) | 1.72 (1.04) | 1.13 (0.64) | p < 0.001 *** (paired t-test) |
| Fasting glucose (mmol/L) | 6.92 (2.24) | 6.41 (2.52) | p > 0.05 (paired t-test) |
| Blood pressure (mmHg) SBP DBP | 142.51 (17.97) 81.15 (11.45) | 139.03 (21.43) 81.54 (12.67) | p > 0.05 p > 0.05 (paired t-test) |
| Family history on hyperlipidemia 1 = no 2 = yes | 77 25 | 88 14 | p < 0.05 * |
| Family history on diabetes 1 = no 2 = yes | 54 48 | 73 29 | p < 0.01 ** |
| Family history on coronary heart disease 1 = no 2 = yes | 85 17 | 83 19 | p > 0.05 |
| Family history on hypertension 1 = no 2 = yes | 35 67 | 58 44 | p < 0.01 ** |
| Having hyperlipidemia 1 = no 2 = yes | 31 71 | 68 34 | p < 0.05 * |
| Having diabetes 1 = no 2 = yes | 27 75 | 57 45 | p < 0.01 ** |
| Having coronary heart disease 1 = no 2 = yes | 91 11 | 86 16 | p > 0.05 |
| Having hypertension 1 = no 2 = yes | 40 62 | 63 39 | p < 0.01 ** |
| Comorbid illness 0 = no 1 = yes | 10 92 | 30 72 | p < 0.001*** |
| Number of IDF criteria (cases, with central obesity) # Central obesity + 2 Central obesity + 3 | 47 55 | ||
| Number of IDF criteria (controls, with no central obesity) # 0 1 2 3 4 | 26 29 13 14 20 |
| Auricular Signals | MS+ (n = 102) | MS− (n = 102) | Test Statistics (McNemar Test) |
|---|---|---|---|
| Visual inspection | |||
| Oily complexion of ears (Rt) No Yes | 62 40 | 88 14 | p < 0.001 *** |
| Oily complexion of ears (Lt) No Yes | 61 41 | 88 14 | p < 0.001 *** |
| Ear hairs (Rt) 1 = Absent 2 = Present | 83 19 | 76 26 | p > 0.05 |
| Ear hairs (Lt) 1 = Absent 2 = Present | 82 20 | 77 25 | p > 0.05 |
| Ear lobe crease (Rt) 0 = Absent 1 = Present | 70 32 | 57 45 | p > 0.05 |
| Ear lobe crease (Lt) 0 = Absent 1 = Present | 65 37 | 61 41 | p > 0.05 |
| Electrical skin resistance test | |||
| Heart (Rt) 1 = Absent 2 = Present | 56 46 | 52 50 | p > 0.05 |
| Heart (Lt)v1 = Absent 2 = Present | 54 48 | 60 42 | p > 0.05 |
| Pancreas and gall bladder (Rt) 1 = Absent 2 = Present | 81 21 | 84 18 | p > 0.05 |
| Pancreas and gall bladder (Lt) 1 = Absent 2 = Present | 78 24 | 78 24 | p = 1.000 |
| Endocrine (Rt) 1 = Absent 2 = Present | 56 46 | 71 31 | p < 0.05 * |
| Endocrine (Lt) 1 = Absent 2 = Present | 58 44 | 64 38 | p > 0.05 |
| Pain pressure test | |||
| Heart (Rt) No Yes | 40 62 | 60 42 | p < 0.01 ** |
| Heart (Lt) No Yes | 41 61 | 70 32 | p < 0.001 *** |
| Pancreas and gall bladder (Rt) No Yes | 45 57 | 59 43 | p > 0.05 |
| Pancreas and gall bladder (Lt) No Yes | 49 53 | 63 39 | p > 0.05 |
| Endocrine (Rt) No Yes | 40 62 | 58 44 | p < 0.05 * |
| Endocrine (Lt) No Yes | 41 61 | 66 36 | p < 0.01 *** |
| Age | Gender | Smoking | Alcohol Consumption | Family History (DM) | Diabetes | Hypertension | CHD | Hyperlipidemia | Central Obesity | Comorbid Illnesses | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Visual inspection | |||||||||||
| Oily complexion on ears (Rt) | p < 0.01 | p < 0.05 | p < 0.05 | ||||||||
| Oily complexion on ears (Lt) | p < 0.05 | p < 0.05 | p < 0.001 | ||||||||
| Ear hairs (Rt) | p < 0.001 | p < 0.001 | p < 0.01 | p < 0.01 | p < 0.05 | p < 0.05 | |||||
| Ear hairs (Lt) | p < 0.001 | p < 0.001 | p < 0.01 | p < 0.001 | p < 0.05 | p < 0.05 | |||||
| Ear lobe crease (Rt) | p < 0.001 | p < 0.05 | p < 0.01 | p < 0.01 | |||||||
| Ear lobe crease (Lt) | p < 0.001 | p < 0.05 | p < 0.05 | p < 0.05 | p < 0.01 | ||||||
| Electrical skin resistance test | |||||||||||
| Heart (Rt) | p < 0.05 | p < 0.001 | p < 0.01 | p < 0.05 | p < 0.001 | p < 0.01 | p < 0.05 | p < 0.01 | p < 0.05 | p < 0.001 | |
| Heart (Lt) | p < 0.001 | p < 0.001 | p < 0.01 | p < 0.05 | p < 0.01 | p < 0.001 | |||||
| Pancreas and gallbladder (Rt) | p < 0.05 | p < 0.05 | p < 0.01 | ||||||||
| Pancreas and gallbladder (Lt) | p < 0.01 | p < 0.01 | p < 0.05 | p < 0.001 | p < 0.01 | p < 0.05 | p < 0.01 | p < 0.01 | |||
| Endocrine (Rt) | p < 0.001 | p < 0.01 | p < 0.001 | p < 0.001 | p < 0.01 | p < 0.001 | |||||
| Endocrine (Lt) | p < 0.05 | p < 0.001 | p < 0.001 | p < 0.05 | p < 0.001 | p < 0.001 | p < 0.05 | p < 0.01 | p < 0.001 | ||
| Pain pressure test | |||||||||||
| Heart (Rt) | p < 0.05 | p < 0.001 | |||||||||
| Heart (Lt) | |||||||||||
| Pancreas and gallbladder (Rt) | p < 0.001 | p < 0.05 | p < 0.05 | p < 0.05 | |||||||
| Pancreas and gallbladder (Lt) | p < 0.01 | p < 0.05 | |||||||||
| Endocrine (Rt) | p < 0.05 | p < 0.05 | |||||||||
| Endocrine (Lt) | p < 0.05 | p < 0.05 | p < 0.01 | ||||||||
| Visual inspection (V) | Va | Vb | Vc | Vd | Ve | Vf | Ea | Eb | Ec | Ed | Ee | Ef | Pa | Pb | Pc | Pd | Pe | Pf |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Va | --- | *** | * | |||||||||||||||
| Vb | --- | * | ||||||||||||||||
| Vc | --- | *** | ** | * | *** | ** | ||||||||||||
| Vd | *** | --- | * | *** | * | ** | *** | * | ||||||||||
| Ve | --- | *** | ** | * | ** | |||||||||||||
| Vf | * | *** | --- | * | * | * | * | |||||||||||
| Electrical skin resistance test (E) | ||||||||||||||||||
| Ea | ** | *** | ** | * | --- | *** | *** | *** | *** | *** | *** | |||||||
| Eb | *** | --- | *** | *** | *** | *** | ||||||||||||
| Ec | * | * | *** | *** | --- | *** | *** | *** | * | * | ||||||||
| Ed | * | ** | *** | *** | *** | --- | *** | *** | ||||||||||
| Ee | *** | *** | *** | *** | --- | *** | ||||||||||||
| Ef | *** | *** | * | * | *** | *** | *** | *** | *** | --- | ||||||||
| Pain pressure test (P) | ||||||||||||||||||
| Pa | --- | * | *** | ** | *** | *** | ||||||||||||
| Pb | * | * | * | --- | ||||||||||||||
| Pc | * | *** | --- | *** | *** | ** | ||||||||||||
| Pd | ** | * | ** | *** | --- | *** | *** | |||||||||||
| Pe | *** | *** | *** | --- | * | |||||||||||||
| Pf | ** | * | *** | * | *** | ** | *** | * | --- |
| Auricular Signals | Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | Negative Predictive Value (%) |
|---|---|---|---|---|
| Visual inspection | ||||
| Oily complexion on ears (Rt) | 39.2 | 86.3 | 74.1 | 58.7 |
| Oily complexion on ears on ears (Lt) | 40.2 | 86.3 | 74.5 | 59.1 |
| Ear hairs (Rt) | 14.7 | 77.5 | 39.5 | 47.6 |
| Ear hairs (Lt) | 15.7 | 86.3 | 39.0 | 47.2 |
| Ear lobe crease (Rt) | 30.4 | 53.9 | 39.7 | 43.7 |
| Ear lobe crease (Lt) | 36.3 | 58.8 | 46.8 | 48.0 |
| Electrical skin resistance test | ||||
| Heart (Rt) | 46.0 | 51.0 | 48.5 | 48.6 |
| Heart (Lt) | 47.1 | 59.8 | 53.9 | 53.0 |
| Pancreas and gallbladder (Rt) | 20.6 | 82.4 | 53.8 | 50.9 |
| Pancreas and gallbladder (Lt) | 24.5 | 76.5 | 51.0 | 50.3 |
| Endocrine (Rt) | 46.1 | 69.6 | 60.3 | 56.3 |
| Endocrine (Lt) | 43.1 | 62.7 | 53.7 | 52.5 |
| Pain pressure test | ||||
| Heart (Rt) | 60.8 | 60.8 | 61.4 | 60.8 |
| Heart (Lt) | 31.4 | 70.6 | 52.5 | 50.7 |
| Pancreas and gallbladder (Rt) | 55.9 | 60.8 | 59.4 | 57.9 |
| Pancreas and gallbladder (Lt) | 52.0 | 62.7 | 58.9 | 56.6 |
| Endocrine (Rt) | 60.8 | 57.8 | 59.6 | 59.6 |
| Endocrine (Lt) | 59.8 | 64.7 | 63.5 | 61.7 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suen, L.K.P.; Yeh, C.H.; Yeung, S.K.W.; Kwan, J.Y.M.; Wong, H.F.; Chan, D.; Cheung, A.S.P.; Yeung, V.T.F. Association between Auricular Signals and the Risk Factors of Metabolic Syndrome. Medicines 2017, 4, 45. https://doi.org/10.3390/medicines4030045
Suen LKP, Yeh CH, Yeung SKW, Kwan JYM, Wong HF, Chan D, Cheung ASP, Yeung VTF. Association between Auricular Signals and the Risk Factors of Metabolic Syndrome. Medicines. 2017; 4(3):45. https://doi.org/10.3390/medicines4030045
Chicago/Turabian StyleSuen, Lorna Kwai Ping, Chao Hsing Yeh, Simon Kai Wang Yeung, Jojo Yee Mei Kwan, Hon Fat Wong, David Chan, Alice Siu Ping Cheung, and Vincent Tok Fai Yeung. 2017. "Association between Auricular Signals and the Risk Factors of Metabolic Syndrome" Medicines 4, no. 3: 45. https://doi.org/10.3390/medicines4030045
APA StyleSuen, L. K. P., Yeh, C. H., Yeung, S. K. W., Kwan, J. Y. M., Wong, H. F., Chan, D., Cheung, A. S. P., & Yeung, V. T. F. (2017). Association between Auricular Signals and the Risk Factors of Metabolic Syndrome. Medicines, 4(3), 45. https://doi.org/10.3390/medicines4030045