NADA Protocol for Behavioral Health. Putting Tools in the Hands of Behavioral Health Providers: The Case for Auricular Detoxification Specialists


Abstract
:1. Introduction
History and Background
2. Materials and Methods
- (1)
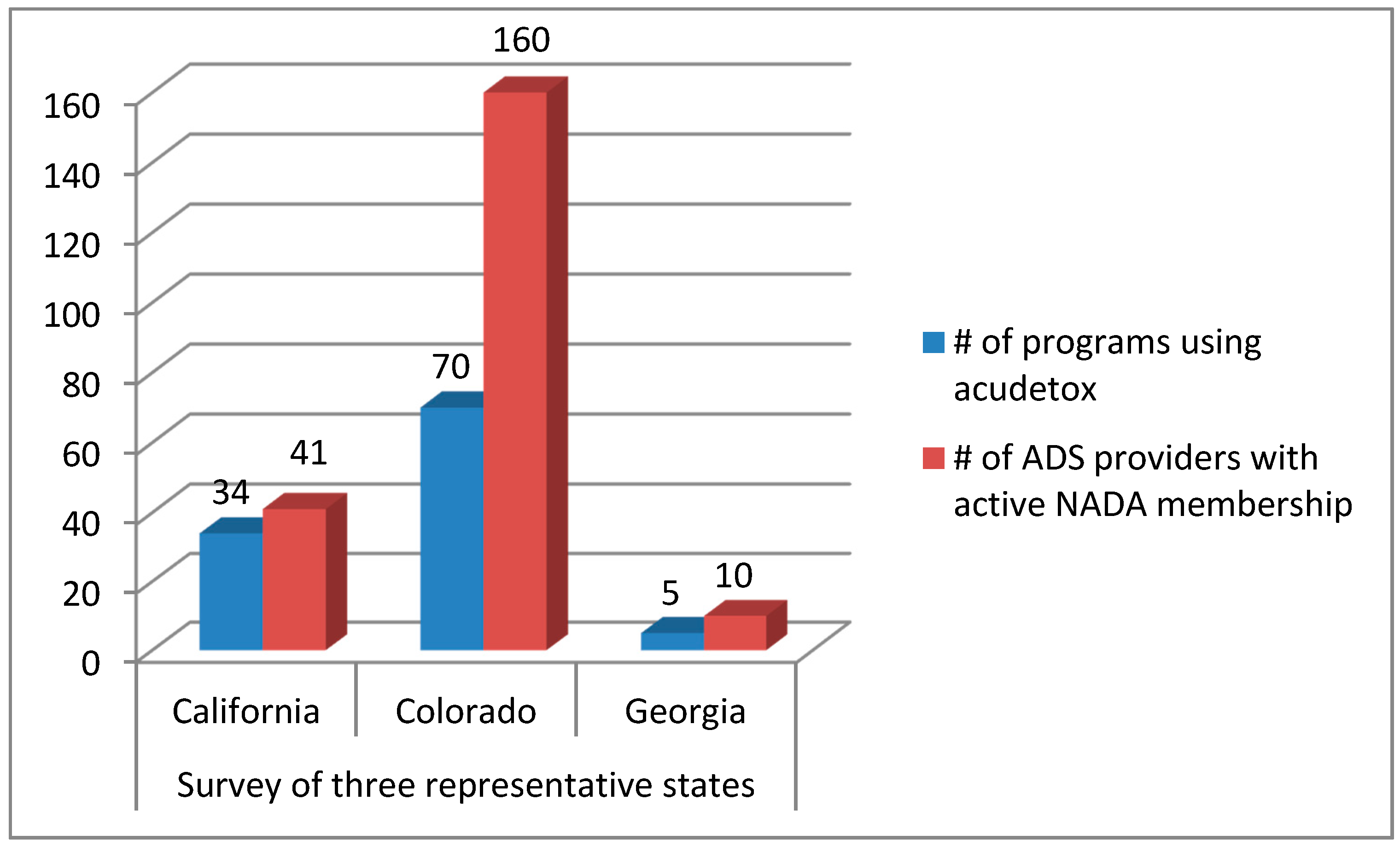
- Survey: A simple two-question email survey was sent to all NADA-trained persons (740) in the following states: California (CA), Colorado (CO), and Georgia (GA), chosen as representative of the range of ADS practice. 1-CA, a state with many licensed acupuncturists and no ADS statute, 2-CO, a state with a recent and more flexible ADS law with no supervision requirement, 3-GA, a state that has an ADS law but requires direct supervision by an acupuncturist.
- (2)
- Search and compilation of state data: The U.S. government, through SAMHSA, conducts the annual National Survey of Substance Abuse Treatment Services (N-SSATS) as mentioned above. This information provides a snapshot of the substance abuse services being used in the public/private addiction treatment sector. Specifically, we looked at SAMHSA’s 2016 data which we combined with the NADA database of trained NADA providers who are active members of NADA, and state-reported data about licensed acupuncturists.
- (3)
- To illustrate the type of implementation that can occur with supportive legislative changes, we conducted brief interviews with programs which have added acudetox into integrated health settings.
3. Results
3.1. Three-State Survey
3.2. Compilation of State-by-State Data
3.3. Program Profiles Based on Personal Interviews
3.3.1. Pueblo Community Health Center—Pueblo, Colorado
3.3.2. Marillac Clinic—Grand Junction, Colorado
3.3.3. St. Mary Corwin Hospital—Pueblo, Colorado
3.3.4. Southern Colorado Harm Reduction Association—Pueblo, Colorado
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Stuyt, E.B.; Voyles, C.A. The National Acupuncture Detoxification Association protocol, auricular acupuncture to support patients with substance abuse and behavioral health disorders: Current perspectives. Subst. Abuse Rehabil. 2016, 7, 169–180. [Google Scholar] [CrossRef] [PubMed]
- What Is Integrated Behavioral Health Care (IBHC)? | AHRQ Academy. Available online: https://integrationacademy.ahrq.gov/resources/ibhc-measures-atlas/what-integrated-behavioral-health-care-ibhc (accessed on 29 November 2017).
- Mitchell, E.R. Fighting Drug Abuse with Acupuncture: The Treatment That Works; Pacific View Press: Berkeley, CA, USA, 1995; ISBN 978-1-881896-12-8. [Google Scholar]
- Wen, H.; Cheng, S. Treatment of drug addiction by acupuncture and electrical stimulation. Asian J. Med. 1973, 9, 138–141. [Google Scholar]
- About NADA. Available online: https://www.acudetox.com/index.php/about-nada (accessed on 27 November 2017).
- How Do State Laws Differ? Available online: https://acudetox.com/how-do-state-laws-differ (accessed on 30 November 2017).
- Bemis, R. Evidence for the NADA Ear Acupuncture Protocol: Summary of Research; NADA Literature Clearinghouse: Laramie, WY, USA, 2013. [Google Scholar]
- Substance Abuse Facilities Data/NSSATS. Available online: https://wwwdasis.samhsa.gov/dasis2/nssats.htm (accessed on 22 December 2017).
- Sherman, B.; Sanders, L.; Trinh, C. Addiction and Pregnancy: Empowering Recovery Through Peer Counseling; Praeger: Westport, CT, USA, 1998. [Google Scholar]
- Acuff, K.; Spolarich, A.W.; Andrulis, D.P.; Gerstein, S. Vulnerable Women and Visionary Programs: Safety Net Programs for Drug-Involved Women and Their Children; The National Public Health and Hospital Institute: Washington, DC, USA, 1994. [Google Scholar]
- Mercier, D. The Kent-Sussex Program: A Case for Acupuncture Specialists; NADA Paper: Launching and Running a Program; NADA Literature Clearinghouse: Laramie, WY, USA, 1994. [Google Scholar]
- Renaud, J. Texas Cancels Acu Care by Detox Specialists. Guid. Acupunct. Recover. 1996, 2. [Google Scholar]
- Maine Association of Acupuncture and Oriental Medicine MAAOM Newsletter. Available online: http://mailchi.mp/cc9fc1460a32/maaom-newsletter (accessed on 23 December 2017).
- Bemis, R. West Coast NADA Report: Where Acupuncturists are Many, Services for Addicts Suffer. Guid. Acupunct. Recover. 2012, 8–10. [Google Scholar]
- Carter, K.O.; Olshan-Perlmutter, M.; James Norton, H.; Smith, M.O. NADA Acupuncture Prospective Trial in Patients with Substance Use Disorders and Seven Common Health Symptoms. Med. Acupunct. 2011, 23, 131–135. [Google Scholar] [CrossRef]
- Yeh, C.H.; Chiang, Y.C.; Hoffman, S.L.; Liang, Z.; Klem, M.L.; Tam, W.W.S.; Chien, L.-C.; Suen, L.K.-P. Efficacy of Auricular Therapy for Pain Management: A Systematic Review and Meta-Analysis. Available online: https://www.hindawi.com/journals/ecam/2014/934670/abs/ (accessed on 1 February 2018).
- Jan, A.L.; Aldridge, E.S.; Rogers, I.R.; Visser, E.J.; Bulsara, M.K.; Niemtzow, R.C. Does Ear Acupuncture Have a Role for Pain Relief in the Emergency Setting? A Systematic Review and Meta-Analysis. Med. Acupunct. 2017, 29, 276–289. [Google Scholar] [CrossRef] [PubMed]
- Santasiero, R.P.; Neussle, G. Cost-effectiveness of auricular acupuncture for treating substance abuse in an HMO setting: A pilot study. Med. Acupunct. 2005, 16, 39–42. [Google Scholar]
- Smith, D.M.O. The Use of Acupuncture in Addiction Treatment Programs. Huffington Post 2012, 16. [Google Scholar]
- Acupuncturists without Borders | Community-based Acupuncture Services and Training. Available online: http://www.acuwithoutborders.org/ (accessed on 26 December 2017).
- Carter, K.; Olshan-Perlmutter, M. NADA protocol: Integrative acupuncture in addictions. J. Addict. Nurs. 2014, 25, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.G. Foundations of Oriental Medicine Biomedicine Acupuncture with Point Location Chinese Herbology Job Analysis Report. 2013. Available online: http://www.nccaom.org/wp-content/uploads/pdf/NCCAOM_2013_JA_Report.pdf (accessed on 26 December 2017).

{kind=link}
{kind=link}
| State | % Acu 1 | SA Programs | ADS 2 | LAc 3 | ADS Rank | Limitations to ADS |
|---|---|---|---|---|---|---|
| Virginia | 17 | 229 | 94 | 507 | 1 | |
| Connecticut | 13.8 | 224 | 91 | 400 | 1 | |
| Michigan | 12.7 | 479 | 178 | 171 | 1 | |
| Wyoming | 10.3 | 58 | 17 | Unavailable 4 | 1 | |
| Colorado | 9.8 | 399 | 160 | 1513 | 1 | |
| New Mexico | 16.2 | 154 | 32 | 737 | 2 | Supervision & Training |
| Rhode Island | 11.5 | 52 | 5 | 166 | 2 | Addiction only |
| Maryland | 11.2 | 402 | 54 | 1138 | 2 | Addiction only |
| Vermont | 8.7 | 34 | 9 | 192 | 2 | Addiction only |
| Arizona | 8.1 | 46 | 51 | 35 | 2 | Board-approved programs only |
| Tennessee | 6.6 | 1430 | 48 | 217 | 2 | Addiction only, Supervision |
| Washington | 5.6 | 227 | 47 | 1550 | 2 | Nurses, Physician Delegation |
| New Hampshire | 4.7 | 60 | 5 | 133 | 2 | New legislation |
| Texas | 4.7 | 64 | 82 | 1265 | 2 | Addiction only |
| Louisiana | 4.5 | 488 | 13 | 55 | 2 | Supervision |
| Missouri | 3.5 | 80 | 9 | 132 | 2 | Supervision |
| Indiana | 3.4 | 268 | 36 | 115 | 2 | Addiction only |
| New York | 2.5 | 229 | 78 | 4398 | 2 | Addiction only |
| Ohio | 1.5 | 64 | 15 | 249 | 2 | Nurses, Physician Delegation |
| Wisconsin | 1.4 | 136 | 8 | 545 | 2 | Physician Delegation |
| North Carolina | 1.2 | 280 | 17 | 586 | 2 | NP and PA, Physician Delegation |
| Arkansas | 0.9 | 489 | 1 | 32 | 2 | Addiction only |
| Delaware | 0 | 201 | 18 | 7 | 2 | High fees |
| Florida | 11.2 | 716 | 22 | 2452 | 3 | LAcs and Physicians Only |
| Oregon | 10.3 | 223 | 38 | 1481 | 3 | LAcs and Physicians Only |
| California | 8 | 358 | 41 | 17,959 | 3 | LAcs and Physicians Only |
| North Dakota Minnesota | 5 4.1 | 428 157 | 9 7 | See note 5 606 | 3 3 | LAcs and Physicians Only LAcs and Physicians Only |
| Hawaii | 4 | 370 | 17 | 702 | 3 | LAcs Only |
| Nevada | 3.8 | 174 | 1 | 61 | 3 | LAcs and Physicians Only |
| Massachusetts | 3.1 | 265 | 13 | 1095 | 3 | LAcs and Physicians Only |
| New Jersey | 3 | 355 | 11 | 1000 | 3 | LAcs and Physicians Only |
| Utah | 3 | 371 | 2 | 167 | 3 | LAcs and Physicians Only |
| Illinois | 2.8 | 235 | 20 | 813 | 3 | LAcs and Physicians Only |
| Pennsylvania | 2.7 | 675 | 15 | 711 | 3 | LAcs and Physicians Only |
| Maine | 2.6 | 528 | 17 | 171 | 3 | LAcs and Physicians Only |
| Iowa | 2.5 | 922 | 0 | 66 | 3 | LAcs and Physicians Only |
| Alaska | 2.1 | 163 | 2 | 118 | 3 | LAcs and Physicians Only |
| South Carolina | 1.8 | 84 | 7 | 158 | 3 | Direct Supervision |
| South Dakota | 1.6 | 114 | 18 | Unavailable 4 | 3 | Not regulated |
| Georgia | 1.6 | 62 | 10 | No response 4 | 3 | Direct Supervision |
| Montana | 1.6 | 314 | 2 | 160 | 3 | LAcs and Physicians Only |
| Nebraska | 1.5 | 406 | 4 | 32 | 3 | LAcs and Physicians Only |
| West Virginia | 0.9 | 113 | 7 | 43 | 3 | LAcs and Physicians Only |
| Kentucky | 0.8 | 106 | 2 | 87 | 3 | LAcs and Physicians Only |
| Alabama | 0.7 | 363 | 8 | N/A | 3 | Physician only |
| Idaho | 0.7 | 136 | 1 | 157 | 3 | LAcs and Physicians Only |
| Oklahoma | 0.5 | 143 | 7 | Unavailable 4 | 3 | Not regulated |
| Kansas | 0.5 | 204 | 2 | Unavailable 4 | 3 | New legislation |
| Mississippi | 0 | 47 | 2 | 11 | 3 | LAcs and Physicians Only |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stuyt, E.B.; Voyles, C.A.; Bursac, S. NADA Protocol for Behavioral Health. Putting Tools in the Hands of Behavioral Health Providers: The Case for Auricular Detoxification Specialists. Medicines 2018, 5, 20. https://doi.org/10.3390/medicines5010020
Stuyt EB, Voyles CA, Bursac S. NADA Protocol for Behavioral Health. Putting Tools in the Hands of Behavioral Health Providers: The Case for Auricular Detoxification Specialists. Medicines. 2018; 5(1):20. https://doi.org/10.3390/medicines5010020
Chicago/Turabian StyleStuyt, Elizabeth B, Claudia A Voyles, and Sara Bursac. 2018. "NADA Protocol for Behavioral Health. Putting Tools in the Hands of Behavioral Health Providers: The Case for Auricular Detoxification Specialists" Medicines 5, no. 1: 20. https://doi.org/10.3390/medicines5010020