
Analysis and Interpretation of Automated Blood Count in the Treatment of Chronic Paracoccidioidomycosis

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Ethical Aspects
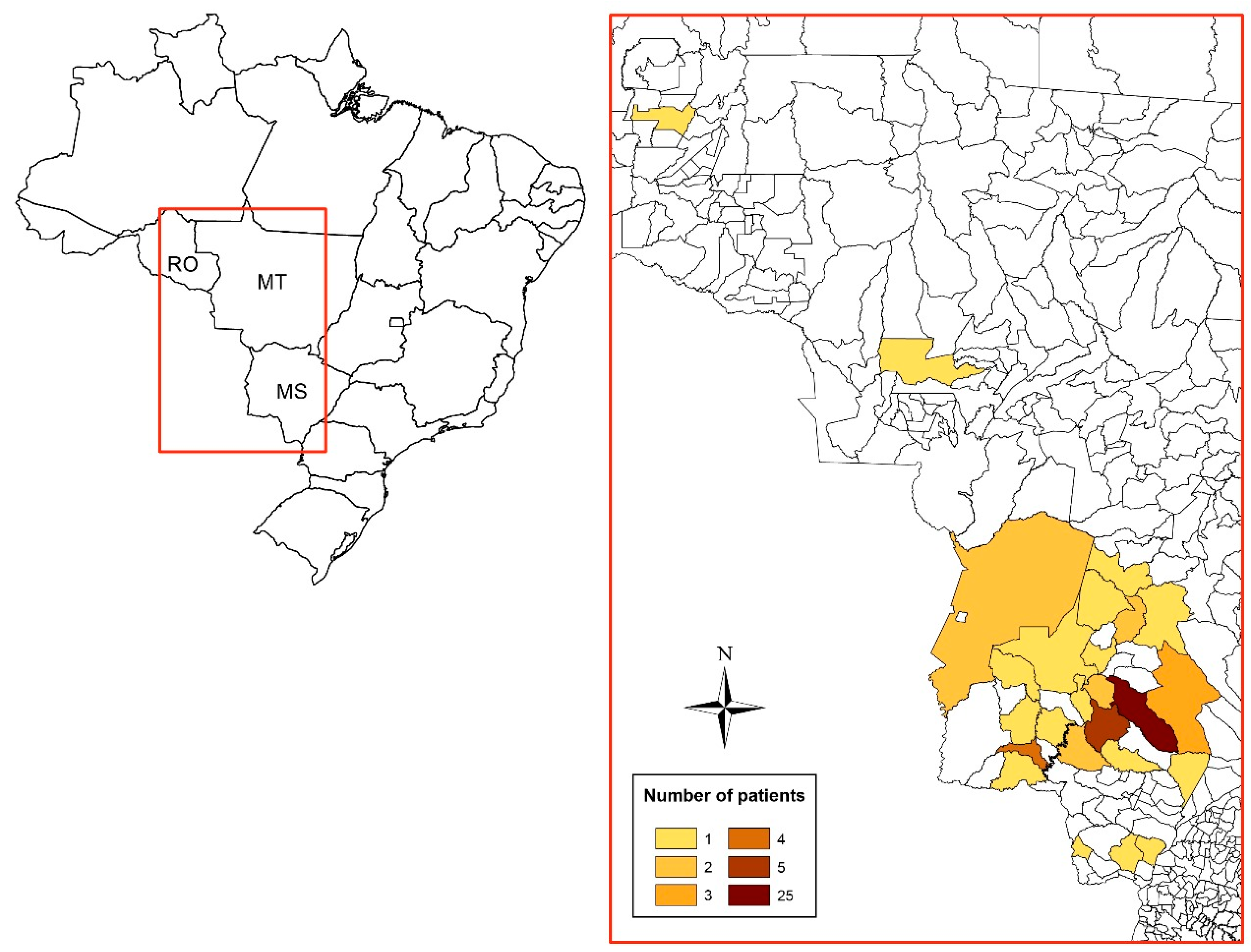
2.2. Design, Place, and Period of Study
2.3. Inclusion and Exclusion Criteria
2.4. Case Definition
2.5. Clinical and Demographic Data
2.6. Laboratory Procedures
2.7. Statistical Analysis
3. Results


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) | 95% CI | |
|---|---|---|---|
| Sex | |||
| Male | 60 (96.8) | 88.8 | 99.6 |
| Female | 02 (3.2) | 0.4 | 11.2 |
| Rural activity | |||
| Yes ‡ | 55 (88.7) | 78.1 | 95.3 |
| Never | 06 (9.7) | 3.6 | 19.8 |
| Ignored | 01 (1.6) | 0.0 | 8.6 |
| Use of Tobacco | |||
| Regularly | 51 (82.3) | 70.5 | 90.8 |
| Former smoker | 07 (11.3) | 4.6 | 21.9 |
| Never | 04 (6.5) | 1.8 | 15.7 |
| Degree of severity of PCM | |||
| Moderate | 37 (59.7) | 46.5 | 72.0 |
| Severe | 17 (27.4) | 16.8 | 40.2 |
| Mild | 08 (12.9) | 5.7 | 23.8 |
| Antifungal treatment | |||
| Itraconazole | 39 (62.9) | 49.7 | 74.8 |
| Cotrimoxazole | 23 (37.1) | 25.2 | 50.3 |

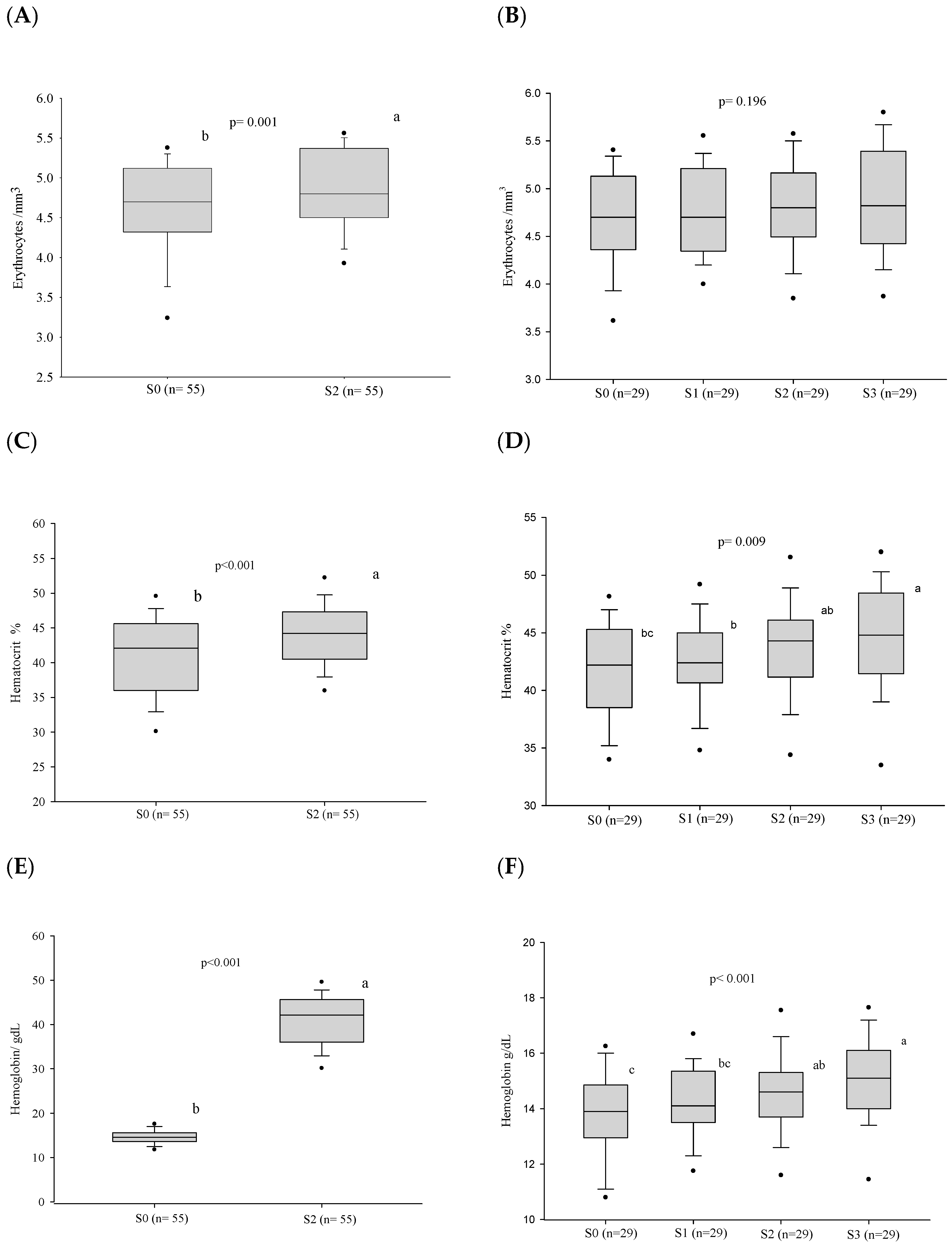
3.1. Red Blood Series
| Variable | Patients (n) | S0 n (%) | S1 n (%) | S2 n (%) | S3 n (%) | p Value |
|---|---|---|---|---|---|---|
| Anemia | 62 | 28 (45.2) | ... | ... | ... | ... |
| 55 * | 21 (39.3) | ... | 11 (20.0) | ... | 0.008 | |
| 29 ** | 08 (27.6) | 06 (20.7) | 06 (20.7) | 03 (10.3) | 0.063 |

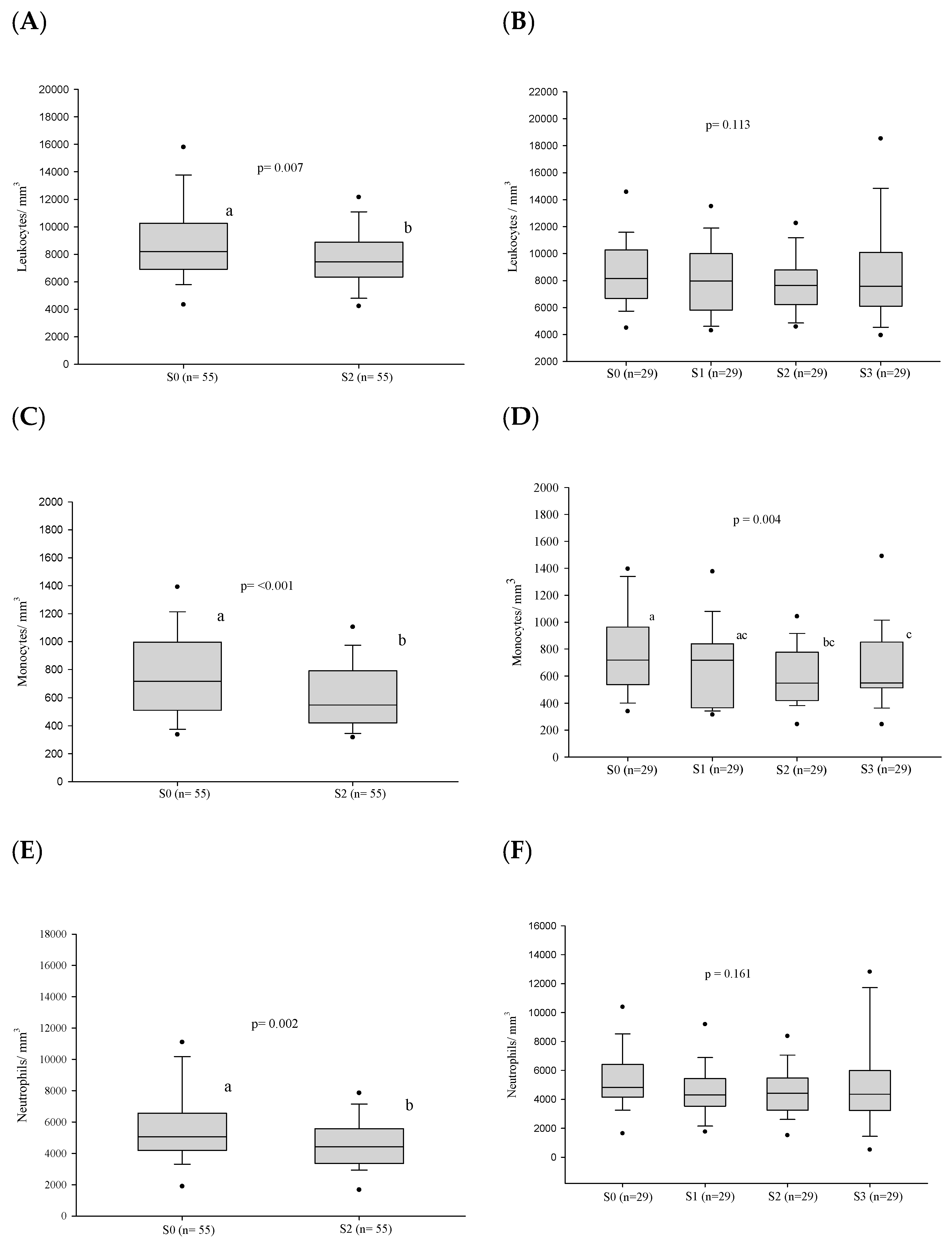
3.2. White Blood Series
3.2.1. Frequency of Alterations
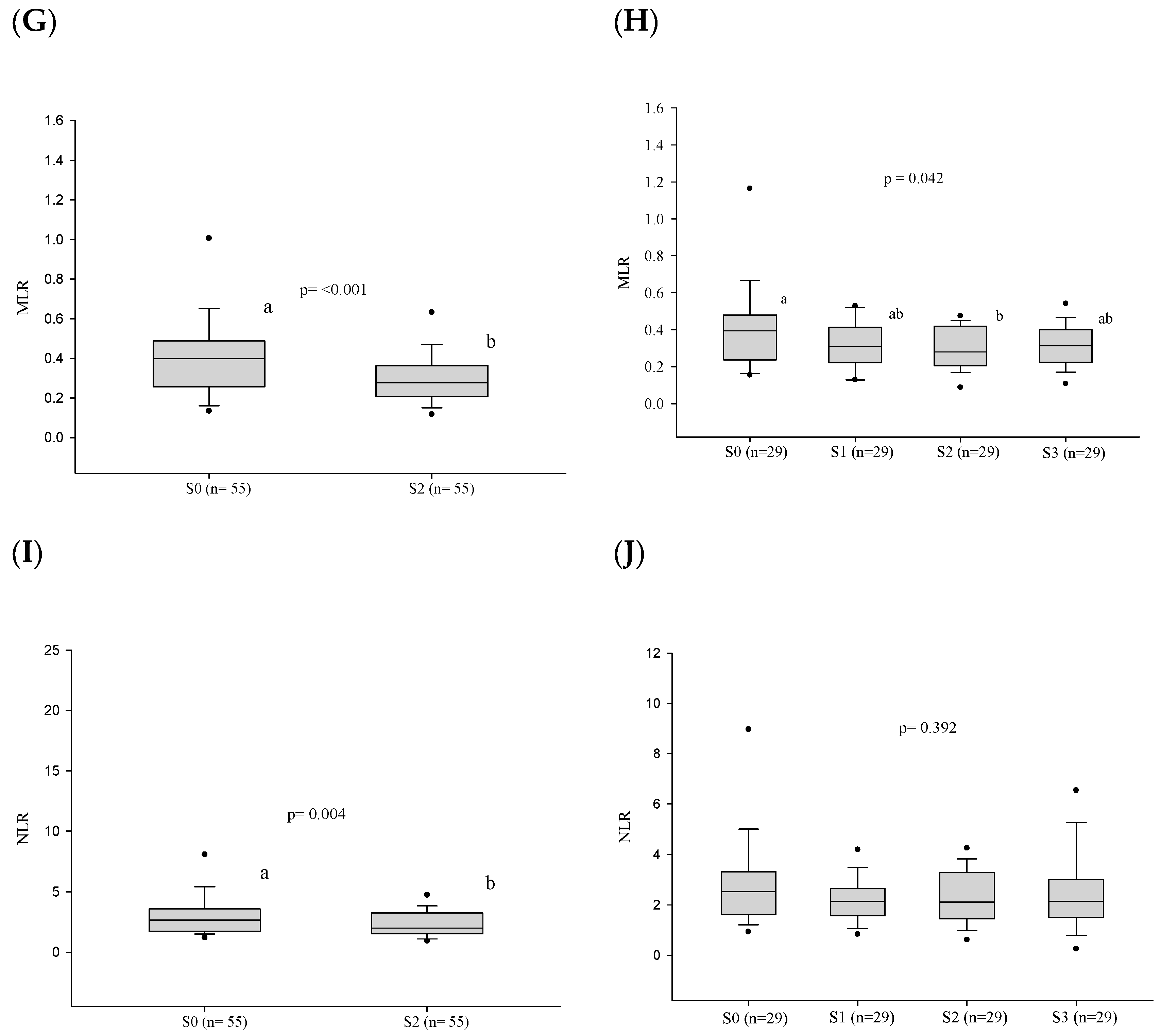
3.2.2. White Blood Cell Counts
3.3. Platelet Series
3.4. Cellular Immaturity
3.5. Influence of the Severity of Paracoccidioidomycosis in Patients on Hematologic Alterations
3.6. Influence of the Antifungal on the Hematologic Alterations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mendes, R.P.; Cavalcante, R.d.S.; Marques, S.A.; Marques, M.E.A.; Venturini, J.; Sylvestre, T.F.; Paniago, A.M.M.; Pereira, A.C.; da Silva, J.d.F.; Fabro, A.T.; et al. Paracoccidioidomycosis: Current Perspectives from Brazil. Open Microbiol. J. 2017, 11, 224–282. [Google Scholar] [CrossRef]
- Coutinho, Z.F.; Wanke, B.; Travassos, C.; Oliveira, R.M.; Xavier, D.R.; Coimbra, C.E.A. Hospital Morbidity Due to Paracoccidioidomycosis in Brazil (1998-2006). Trop. Med. Int. Health 2015, 20, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Giusiano, G. The Trojan Horse Model in Paracoccidioides: A Fantastic Pathway to Survive Infecting Human Cells. Front. Cell. Infect. Microbiol. 2021, 10, 605679. [Google Scholar] [CrossRef] [PubMed]
- Londero, A.T. Paracoccidioidomicose: Patogenia, Formas Clínicas, Manifestações Pulmonares e Diagnóstico. J. Pneumol. 1986, 2, 41–57. [Google Scholar]
- Bellissimo-Rodrigues, F.; Bollela, V.R.; Da Fonseca, B.A.L.; Martinez, R. Endemic Paracoccidioidomycosis: Relationship between Clinical Presentation and Patients’ Demographic Features. Med. Mycol. 2013, 51, 313–318. [Google Scholar] [CrossRef]
- Matos, W.B.d.; Santos, G.M.C.d.; Silva, V.E.B.d.; Gonçalves, E.d.G.d.R.; Silva, A.R.d. Paracoccidioidomycosis in the State of Maranhão, Brazil: Geographical and Clinical Aspects. Rev. Soc. Bras. Med. Trop. 2012, 45, 385–389. [Google Scholar] [CrossRef]
- Paniago, A.M.M.; Aguiar, J.I.A.; Aguiar, E.S.; Cunha, R.V.d.; Pereira, G.R.d.O.L.; Londero, A.T.; Wanke, B. Paracoccidioidomicose: Estudo Clínico e Epidemiológico de 422 Casos Observados no Estado de Mato Grosso do Sul. Rev. Soc. Bras. Med. Trop. 2003, 36, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.M.; Bucaretchi, F.; Barison, E.d.M.; Hessel, G.; Tresoldi, A.T. Paracoccidioidomycosis in Children: Clinical Presentation, Follow-up and Outcome. Rev. Inst. Med. Trop. São Paulo 2004, 46, 127–131. [Google Scholar] [CrossRef]
- de Castro, L.F.; Ferreira, M.C.; da Silva, R.M.; Blotta, M.H.d.S.L.; Longhi, L.N.A.; Mamoni, R.L. Characterization of the Immune Response in Human Paracoccidioidomycosis. J. Infect. 2013, 67, 470–485. [Google Scholar] [CrossRef]
- Cezar-dos-Santos, F.; Assolini, J.P.; Okuyama, N.C.M.; Viana, K.F.; de Oliveira, K.B.; Itano, E.N. Unraveling the Susceptibility of Paracoccidioidomycosis: Insights towards the Pathogen-Immune Interplay and Immunogenetics. Infect Genet. Evol. 2020, 86, 104586. [Google Scholar] [CrossRef]
- Weiss, G.; Ganz, T.; Goodnough, L.T. Anemia of Inflammation. Blood 2019, 133, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Tsioumpekou, M.; Krijgsman, D.; Leusen, J.H.W.; Olofsen, P.A. The Role of Cytokines in Neutrophil Development, Tissue Homing, Function and Plasticity in Health and Disease. Cells 2023, 12, 1981. [Google Scholar] [CrossRef] [PubMed]
- Burger, E. Paracoccidioidomycosis Protective Immunity. J. Fungi. 2021, 7, 137. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Custódio, J.M.; Enokida, I.M.; Gonçalves, D.A.; Leone de Oliveira, S.M.d.V.; Venturini, J.; Carvalho, L.R.; Mendes, R.P.; Paniago, A.M.M. Dynamics of Plasma Micronutrient Concentrations and their Correlation with Serum Proteins and Thyroid Hormones in Patients with Paracoccidioidomycosis. PLoS ONE 2019, 14, e0226609. [Google Scholar] [CrossRef] [PubMed]
- Doedens, A.L.; Phan, A.T.; Stradner, M.H.; Fujimoto, J.K.; Nguyen, J.V.; Yang, E.; Johnson, R.S.; Goldrath, A.W. Hypoxia-Inducible Factors Enhance the Effector Responses of CD8+ T Cells to Persistent Antigen. Nat. Immunol. 2013, 14, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Venturini, J.; Cavalcante, R.S.; de Assis Golim, M.; Marchetti, C.M.; de Azevedo, P.Z.; Amorim, B.C.; de Arruda, M.S.P.; Mendes, R.P. Phenotypic and Functional Evaluations of Peripheral Blood Monocytes from Chronic-Form Paracoccidioidomycosis Patients before and after Treatment. BMC Infect. Dis. 2014, 14, 552. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Chaudhury, A.; Zhang, M.; Savoldo, B.; Metelitsa, L.S.; Rodgers, J.; Yustein, J.T.; Neilson, J.R.; Dotti, G. Glycolysis Determines Dichotomous Regulation of T Cell Subsets in Hypoxia. J. Clin. Investig. 2016, 126, 2678–2688. [Google Scholar] [CrossRef] [PubMed]
- Shikanai-Yasuda, M.A.; Mendes, R.P.; Colombo, A.L.; Queiroz-Telles, F.d.; Kono, A.S.G.; Paniago, A.M.M.; Nathan, A.; Valle, A.C.F.d.; Bagagli, E.; Benard, G.; et al. Brazilian Guidelines for the Clinical Management of Paracoccidioidomycosis. Rev. Soc. Bras. Med. Trop. 2017, 50, 715–740. [Google Scholar] [CrossRef]
- Hoffbrand, A.V.; Steensma, D.P. Hoffbrand’s Essential Haematology, 8th ed.; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2020; ISBN 978-1-119-49595-6. [Google Scholar]
- Pekelharing, J.M.; Hauss, O.; Jonge, R.d.; Lokhof, J.; Sodikromo, J.; Spaans, M.; Brouwer, R.; Lathouder, S.d.; Hinzmann, R. Haematology Reference Intervals for Established and Novel Parameters in Healthy Adults. Sysmex J. Int. 2010, 20, 1–11. [Google Scholar]
- Camargo, Z.P.; Berzaghi, R.; Amaral, C.C.; Silva, S.H.M. Simplified Method for Producing Paracoccidioides brasiliensis Exoantigens for Use in Immunodiffusion Tests. Med. Mycol. 2003, 41, 539–542. [Google Scholar] [CrossRef]
- The Jamovi Project. Jamovi (Version 1.6) [Computer Software]. Sydney, Australia. Available online: https://www.jamovi.org (accessed on 20 January 2022).
- Pedersen, K.M.; Çolak, Y.; Ellervik, C.; Hasselbalch, H.C.; Bojesen, S.E.; Nordestgaard, B.G. Smoking and Increased White and Red Blood Cells: A Mendelian Randomization Approach in the Copenhagen General Population Study. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 965–977. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, R.d.S.; Sylvestre, T.F.; Levorato, A.D.; de Carvalho, L.R.; Mendes, R.P. Comparison between Itraconazole and Cotrimoxazole in the Treatment of Paracoccidiodomycosis. PLoS Negl. Trop. Dis. 2014, 8, e2793. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, G.E. The Anemia of Chronic Disorders. Semin. Hematol. 1966, 3, 351–375. [Google Scholar] [PubMed]
- de Brito, E.d.C.A.; Siqueira, I.V.; Venturini, J.; Félix, V.L.T.; dos Santos, A.O.G.M.; Mendes, R.P.; Weber, S.S.; Paniago, A.M.M. Iron Metabolism Disorders of Patients with Chronic Paracoccidioidomycosis. PLoS ONE 2023, 18, e0282218. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T.; Nemeth, E. Iron Sequestration and Anemia of Inflammation. Semin. Hematol. 2009, 46, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Kang, Y.A.; Yoon, Y.S.; Um, S.-W.; Lee, S.M.; Yoo, C.-G.; Kim, Y.W.; Han, S.K.; Shim, Y.-S.; Yim, J.-J. The Prevalence and Evolution of Anemia Associated with Tuberculosis. J. Korean Med. Sci. 2006, 21, 1028. [Google Scholar] [CrossRef] [PubMed]
- Minchella, P.A.; Donkor, S.; Owolabi, O.; Sutherland, J.S.; McDermid, J.M. Complex Anemia in Tuberculosis: The Need to Consider Causes and Timing When Designing Interventions. Clin. Infect. Dis. 2015, 60, 764–772. [Google Scholar] [CrossRef]
- Bailão, E.F.L.C.; Parente, J.A.; Pigosso, L.L.; Castro, K.P.d.; Fonseca, F.L.; Silva-Bailão, M.G.; Báo, S.N.; Bailão, A.M.; Rodrigues, M.L.; Hernandez, O.; et al. Hemoglobin Uptake by Paracoccidioides spp. Is Receptor-Mediated. PLoS Negl. Trop. Dis. 2014, 8, e2856. [Google Scholar] [CrossRef] [PubMed]
- Chinudomwong, P.; Binyasing, A.; Trongsakul, R.; Paisooksantivatana, K. Diagnostic Performance of Reticulocyte Hemoglobin Equivalent in Assessing the Iron Status. Clin. Lab. Anal. 2020, 34, e23225. [Google Scholar] [CrossRef]
- Benard, G. An Overview of the Immunopathology of Human Paracoccidioidomycosis. Mycopathologia 2008, 165, 209–221. [Google Scholar] [CrossRef]
- Loures, F.V.; Pina, A.; Felonato, M.; Araújo, E.F.; Leite, K.R.M.; Calich, V.L.G. Toll-like Receptor 4 Signaling Leads to Severe Fungal Infection Associated with Enhanced Proinflammatory Immunity and Impaired Expansion of Regulatory T Cells. Infect. Immun. 2010, 78, 1078–1088. [Google Scholar] [CrossRef]
- Goihman-Yahr, M.; Rothenberg, A.; Bretaña, A.; Istúriz, G.; Rosquete, R.; Avila-Millán, E.; Viloria, N.; de Borges, N.S.; Carrasquero, M.; de Fernández, B.P.; et al. Digestion of Killed Paracoccidioides brasiliensis by Neutrophils. Mycopathologia 1989, 106, 53–58. [Google Scholar] [CrossRef]
- Schaffner, A.; Davis, C.E.; Schaffner, T.; Markert, M.; Douglas, H.; Braude, A.I. In Vitro Susceptibility of Fungi to Killing by Neutrophil Granulocytes Discriminates between Primary Pathogenicity and Opportunism. J. Clin. Investig. 1986, 78, 511–524. [Google Scholar] [CrossRef]
- Xidieh, C.F.; Lenzi, H.L.; Calich, V.L.G.; Burger, E. Influence of the Genetic Background on the Pattern of Lesions Developed by Resistant and Susceptible Mice Infected with Paracoccidioides brasiliensis. Med. Microbiol. Immunol. 1999, 188, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.; Peraçoli, M.T.; Soares, A.; Montenegro, R.; Mendes, R.P.; Meira, D.A. Host-Parasite Relationship in Paracoccidioidomycosis. Curr. Top. Med. Mycol. 1993, 5, 115–149. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, F.; Miyazaki, S. New Biodefense Strategies by Neutrophils. Arch. Immunol. Ther. Exp. (Warsz) 2005, 53, 226–233. [Google Scholar] [PubMed]
- Moscardi-Bacchi, M.; Brummer, E.; Stevens, D.A. Support of Paracoccidioides brasiliensis Multiplication by Human Monocytes or Macrophages: Inhibition by Activated Phagocytes. J. Med. Microbiol. 1994, 40, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Calvi, S.A.; Soares, A.M.V.C.; Peraçoli, M.T.S.; Franco, M.; Ruiz, R.L.; Marcondes-Machado, J.; Fecchio, D.; Mattos, M.C.I.; Mendes, R.P. Study of Bronchoalveolar Lavage Fluid in Paracoccidioidomycosis: Cytopathology and Alveolar Macrophage Function in Response to Gamma Interferon; Comparison with Blood Monocytes. Microbes Infect. 2003, 5, 1373–1379. [Google Scholar] [CrossRef]
- Bava, A.J.; Mistchenko, A.S.; Palacios, M.F.; Estevez, M.E.; Tiraboschi, N.I.; Sen, L.; Negroni, R.; Diez, R.A. Lymphocyte Subpopulations and Cytokine Production in Paracoccidioidomycosis Patients. Microbiol. Immunol. 1991, 35, 167–174. [Google Scholar] [CrossRef]
- Braga, F.G.; Ruas, L.P.; Pereira, R.M.; Lima, X.T.; Antunes, E.; Mamoni, R.L.; Blotta, M.H.S.L. Functional and Phenotypic Evaluation of Eosinophils from Patients with the Acute Form of Paracoccidioidomycosis. PLoS Negl. Trop. Dis. 2017, 11, e0005601. [Google Scholar] [CrossRef]
- Shikanai-Yasuda, M.A.; Higaki, Y.; Uip, D.E.; Mori, N.S.; Del Negro, G.; Melo, N.T.; Hutzler, R.U.; Amato Neto, V. [Bone Marrow Involvement Associated with Eosinophilia in Paracoccidioidomycosis]. Rev. Inst. Med. Trop. Sao Paulo 1992, 34, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Gorelik, O.; Izhakian, S.; Barchel, D.; Almoznino-Sarafian, D.; Tzur, I.; Swarka, M.; Beberashvili, I.; Feldman, L.; Cohen, N.; Shteinshnaider, M. Prognostic Significance of Platelet Count Changes during Hospitalization for Community-Acquired Pneumonia. Platelets 2017, 28, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Semple, J.W.; Freedman, J. Platelets and Innate Immunity. Cell Mol. Life Sci. 2010, 67, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.; Kerrigan, S.W.; Watson, S.P. Platelets and the Innate Immune System: Mechanisms of Bacterial-Induced Platelet Activation. J. Thromb. Haemost. 2011, 9, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Pitchford, S.; Pan, D.; Welch, H.C.E. Platelets in Neutrophil Recruitment to Sites of Inflammation. Curr. Opin. Hematol. 2017, 24, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Morales, M.; Xue, X. Targeting Iron Metabolism in Cancer Therapy. Theranostics 2021, 11, 8412–8429. [Google Scholar] [CrossRef]
- Abakay, O.; Abakay, A.; Sen, H.S.; Tanrikulu, A.C. The Relationship between Inflammatory Marker Levels and Pulmonary Tuberculosis Severity. Inflammation 2015, 38, 691–696. [Google Scholar] [CrossRef]
- Nery, A.F.; de Camargo, Z.P.; Rodrigues, A.M.; Portela, T.F.; Hoffmann-Santos, H.D.; Pinheiro, B.G.; Possa, A.P.; Cavalcante, L.R.d.S.; Hagen, F.; Hahn, R.C. Puzzling Paracoccidioidomycosis: Factors Associated with the Severity of Paracoccidioides lutzii Infections. Int. J. Infect. Dis. 2021, 107, 284–290. [Google Scholar] [CrossRef]
- Vidal, M.S.M.; Del Negro, G.M.B.; Vicentini, A.P.; Svidzinski, T.I.E.; Mendes-Giannini, M.J.; Almeida, A.M.F.; Martinez, R.; de Camargo, Z.P.; Taborda, C.P.; Benard, G. Serological Diagnosis of Paracoccidioidomycosis: High Rate of Inter-Laboratorial Variability among Medical Mycology Reference Centers. PLoS Negl. Trop. Dis. 2014, 8, e3174. [Google Scholar] [CrossRef]
- Carmo, J.P.M.; Dias-Melicio, L.A.; Calvi, S.A.; Peraçoli, M.T.S.; Soares, A.M.V.C. TNF-α Activates Human Monocytes for Paracoccidioides brasiliensis Killing by an H2O2-Dependent Mechanism. Med. Mycol. 2006, 44, 363–368. [Google Scholar] [CrossRef]
- Gonzalez, A.; Sahaza, J.H.; Ortiz, B.L.; Restrepo, A.; Cano, L.E. Production of Pro-Inflammatory Cytokines during the Early Stages of Experimental Paracoccidioides brasiliensis Infection. Med. Mycol. 2003, 41, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.M.-W.; Juurlink, D.N. Considerations When Prescribing Trimethoprim-Sulfamethoxazole. Can. Med. Assoc. J. 2011, 183, 1851–1858. [Google Scholar] [CrossRef] [PubMed]
- Dosoo, D.K.; Kayan, K.; Adu-Gyasi, D.; Kwara, E.; Ocran, J.; Osei-Kwakye, K.; Mahama, E.; Amenga-Etego, S.; Bilson, P.; Asante, K.P.; et al. Haematological and Biochemical Reference Values for Healthy Adults in the Middle Belt of Ghana. PLoS ONE 2012, 7, e36308. [Google Scholar] [CrossRef] [PubMed]



| Variable | Patients (Number) | S0 n (%) | S1 n (%) | S2 n (%) | S3 n (%) | p Value |
|---|---|---|---|---|---|---|
| Leukopenia * | 55 | 02 (3.6) | ... | 02 (3.6) | ... | 0.564 |
| Leukopenia † | 29 | 01 (3.4) | - | - | 02 (6.9) | 0.317 |
| Leukocytosis * | 55 | 11 (20.0) | ... | 08 (14.5) | ... | 0.366 |
| Leukocytosis † | 29 | 06 (20.7) | 05 (17.2) | 06 (20.7) | 05 (17.2) | 0.940 |
| Neutropenia * | 55 | 01 (1.8) | ... | 03 (5.5) | ... | 0.157 |
| Neutropenia † | 29 | 01 (3.4) | 01 (3.4) | 02 (6.9) | 03 (10.3) | 0.194 |
| Neutrophilia * | 55 | 08 (14.5) | ... | 04 (7.3) | ... | 0.206 |
| Neutrophilia † | 29 | 03 (10.3) | 02 (6.9) | 02 (6.9) | 05 (17.2) | 0.429 |
| Eosinophilia * | 55 | 14 (25.4) | ... | 14 (25.4) | ... | 1.000 |
| Eosinophilia † | 29 | 09 (31.0) | 12 (41.4) | 10 (34.5) | 08 (27.6) | 0.274 |
| Monocytosis * | 55 | 22 (40.0) | ... | 09 (16.4) | ... | 0.003 |
| Monocytosis † | 29 | 11 (37.9) | 06 (20.7) | 04 (13.8) | 07 (24.1) | 0.059 |
| Lymphopenia * | 55 | 14 (25.5) | ... | 11 (20.0) | ... | 0.366 |
| Lymphopenia † | 29 | 06 (20.7) | 06 (20.7) | 06 (20.7) | 07 (24.1) | 0.954 |
| Lymphocytosis * | 55 | 03 (5.5) | ... | 03 (5.5) | ... | 1.000 |
| Lymphocytosis † | 29 | 03 (10.3) | 03 (10.3) | 02 (6.9) | 03 (10.3) | 0.801 |
| Variables | S0 Mean ± SD Median (Q1; Q3) | S2 Mean ± SD Median (Q1; Q3) | p Value |
|---|---|---|---|
| IGs † | 0.0 (0.0; 0.1) | 0.0 (0.0; 0.1) | 0.756 |
| IGs (%) † | 0.5 (0.3; 0.7) | 0.2 (0.0; 0.3) | 0.037 |
| Ret (%) * | 1.3 ± 0.6 | 3.3 ± 8.1 | 0.942 |
| IRF * | 6.8 ± 2.8 | 7.0 ± 4.0 | 0.441 |
| Ret-He * | 31.4 ± 3.0 | 33.5 ± 1.7 | 0.016 |
| IPF † | 31.6 (29.5; 33.9) | 33.7 (32.8; 34.3) | 0.056 |
| Variables | Severe (n = 17) n (%) | Mild + Moderate (n = 45) n (%) | p Value |
|---|---|---|---|
| Anemia | 12 (70.6) | 16 (35.6) | 0.013 |
| Leukopenia * | 0 (0.0) | 03 (6.7) | 0.555 |
| Leukocytosis | 02 (11.8) | 09 (20.0) | 0.712 |
| Neutropenia * | 0 (0.0) | 02 (4.4) | 1.000 |
| Neutrophilia * | 02 (11.8) | 06 (13.3) | 1.000 |
| Monocytosis | 07 (41.2) | 17 (37.8) | 0.806 |
| Eosinophilia | 02 (11.8) | 04 (8.9) | 0.662 |
| Lymphopenia | 02 (11.8) | 04 (8.9) | 0.662 |
| Lymphocytosis | 02 (11.8) | 09 (20.0) | 0.712 |
| Thrombocytosis * | 03 (17.6) | 03 (6.7) | 0.333 |
| Alteration before Treatment (Frequency) | Mechanism | Involved Cytokines | Related References |
|---|---|---|---|
| Anemia (45.2%) | - Erythropoietin inhibition - Erythrocyte ingestion by macrophages - Iron retention in macrophages | IL-6, IFN-γ, TNF-α, IL-1β, IL-10 | [10,11,26] |
| Monocytosis (38.7%) | - Monocyte activation | TNF- α | [16,52] |
| Lymphopenia (30.6%) | - CD4+ cell recruitment to the site of infection | IL-17 and IFN-γ | [10,32,41] |
| Eosinophilia (24.2%) | - Stimulation of eosinophil production | IL-5 | [10,13,32] |
| Neutrophilia (12.9%) | - Stimulation of production in the bone marrow and recruitment to the site of infection | TNFα, IL6, IL1 β, CXCL8 | [10,13,53] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brito, E.d.C.A.d.; França, A.d.O.; Siqueira, I.V.; Félix, V.L.T.; Rezende, A.A.; Amorim, B.C.; Silva, S.E.R.d.; Mendes, R.P.; Weber, S.S.; Paniago, A.M.M. Analysis and Interpretation of Automated Blood Count in the Treatment of Chronic Paracoccidioidomycosis. J. Fungi 2024, 10, 317. https://doi.org/10.3390/jof10050317
Brito EdCAd, França AdO, Siqueira IV, Félix VLT, Rezende AA, Amorim BC, Silva SERd, Mendes RP, Weber SS, Paniago AMM. Analysis and Interpretation of Automated Blood Count in the Treatment of Chronic Paracoccidioidomycosis. Journal of Fungi. 2024; 10(5):317. https://doi.org/10.3390/jof10050317
Chicago/Turabian StyleBrito, Eliana da Costa Alvarenga de, Adriana de Oliveira França, Igor Valadares Siqueira, Vinícius Lopes Teodoro Félix, Amanda Alves Rezende, Bárbara Casella Amorim, Suzane Eberhart Ribeiro da Silva, Rinaldo Poncio Mendes, Simone Schneider Weber, and Anamaria Mello Miranda Paniago. 2024. "Analysis and Interpretation of Automated Blood Count in the Treatment of Chronic Paracoccidioidomycosis" Journal of Fungi 10, no. 5: 317. https://doi.org/10.3390/jof10050317