
Chronic Pulmonary Aspergillosis—Where Are We? and Where Are We Going?


Abstract
:1. Introduction
2. At Risk Individuals
2.1. Phenotypes in CPA
2.2. Immune Deficiency and CPA
2.3. Genetic Susceptibility and CPA
3. Clinical Manifestations
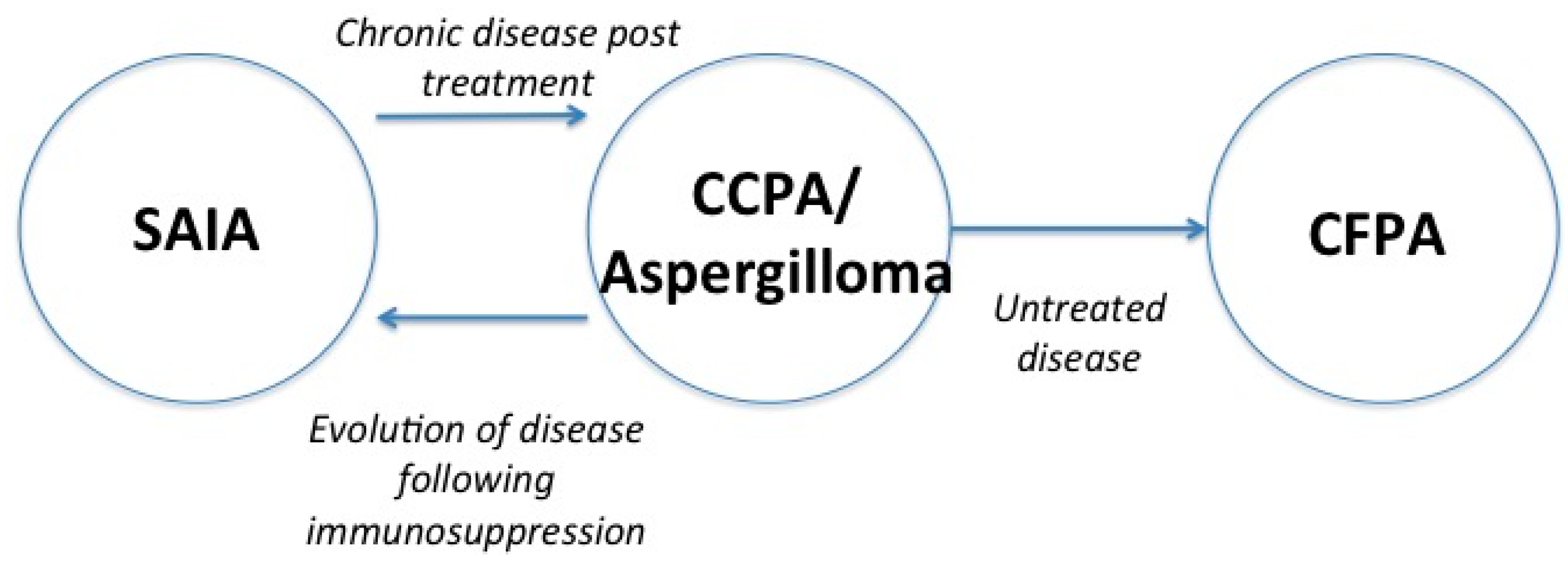
3.1. Aspergilloma
3.2. Chronic Cavitary Pulmonary Aspergillosis (CCPA)
3.3. Chronic Fibrosing Pulmonary Aspergillosis (CFPA)
3.4. Subacute Invasive Aspergillosis (SAIA)
3.5. Aspergillus nodules
4. Diagnosis and Diagnostic Barriers
4.1. Symptoms
4.2. Radiology
4.3. Serology and Immunology
4.4. Histopathology
4.5. Culture of Respiratory Secretions
4.6. PCR of Respiratory Secretions
4.7. Galactomannan Assay of Respiratory Secretions and Serum
4.8. New and Emerging Technologies
4.8.1. MALDI-TOF Mass Spectrometry in the Detection of Aspergillus spp.
4.8.2. The Future
5. Treatment Options
5.1. Current Antifungal Agents—Azoles, Echinocandins and Liposomal Amphotericin B
5.1.1. Triazole Therapy
5.1.2. Intravenous Therapy—Liposomal Amphotericin B and Echinocandins
5.1.3. Novel Antifungal Therapies
5.2. Adjunctive Therapies
5.2.1. Gamma Interferon Replacement Therapy
5.2.2. Surgical Management of CPA
5.2.3. Haemoptysis and Bronchial Artery Embolisation
6. Treatments Barriers
6.1. Side Effects
6.1.1. Itraconazole
6.1.2. Voriconazole
6.2. Drug Interactions
6.3. Drug Resistance in A. fumigatus—An Emerging Problem
6.4. Other Barriers to Treatment of CPA
7. Long Term Management Goals
8. Conclusions
Acknowledgments
Conflicts of Interest
Abbreviations
| ABPA | allergic bronchopulmonary aspergillosis |
| CPA | chronic pulmonary aspergillosis |
| CCPA | chronic cavitary pulmonary aspergillosis |
| CFPA | chronic fibrosing pulmonary aspergillosis |
| CNPA | chronic necrotizing pulmonary aspergillosis |
| COPD | chronic obstructive pulmonary disease |
| CT | computed tomography |
| CXR | chest X-ray |
| CRP | C-reactive protein |
| EBUS | endobronchial ultrasound |
| ESCMID | European Society of Clinical Microbiology and Infectious Diseases |
| ESR | erythrocyte sedimentation rate |
| ERS | European Respiratory Society |
| GAFFI | Global Action for Fungal Infections |
| GM | galactomannan |
| IDSA | Infectious Diseases Society of America |
| LFD | lateral flow device |
| MALDI-TOF | matrix-assisted laser desorption/ionization time-of-flight |
| MIC | minimum inhibitory concentration |
| NTM | nontuberculous mycobacteria |
| ODI | optical density index |
| PET | positron emission tomography |
| POC | point of care |
| PCR | polymerase chain reaction |
| PV | plasma viscosity |
| SAIA | subacute invasive aspergillosis |
| SNP | single nucleotide point mutation |
| TB | tuberculosis |
References
- Lowes, D.; Chishimba, L.; Greaves, M.; Denning, D.W. Development of chronic pulmonary aspergillosis in adult asthmatics with abpa. Respir. Med. 2015, 109, 1509–1515. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Pleuvry, A.; Cole, D.C. Global burden of chronic pulmonary aspergillosis as a sequel to pulmonary tuberculosis. Bull. World Health Organ. 2011, 89, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W. The Ambitious “95–95 by 2025” Roadmap for The Diagnosis and Management of Fungal Diseases; Thorax: London, UK, 2015; Volume 70, pp. 613–614. [Google Scholar]
- Denning, D.W. Available online: http://www.gaff.org/roadmap/ (accessed on 16 March 2016).
- Smith, N.L.; Denning, D.W. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. Eur. Respir. J. 2011, 37, 865–872. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Who Global Tuberculosis Report 2015; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- Osmanov, A.; Denning, D.W. Burden of serious fungal infections in Ukraine. Mycoses 2015, 58, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Hedayati, M.T.; Azimi, Y.; Droudinia, A.; Mousavi, B.; Khalilian, A.; Hedayati, N.; Denning, D.W. Prevalence of chronic pulmonary aspergillosis in patients with tuberculosis from Iran. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1759–1765. [Google Scholar] [CrossRef] [PubMed]
- Beardsley, J.; Denning, D.W.; Chau, N.V.; Yen, N.T.; Crump, J.A.; Day, J.N. Estimating the burden of fungal disease in Vietnam. Mycoses 2015, 58, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Riniotis, K.; Dobrashian, R.; Sambatakou, H. Chronic cavitary and fibrosing pulmonary and pleural aspergillosis: Case series, proposed nomenclature change, and review. Clin. Infect. Dis. 2003, 37, S265–S280. [Google Scholar] [CrossRef] [PubMed]
- Camuset, J.; Nunes, H.; Dombret, M.C.; Bergeron, A.; Henno, P.; Philippe, B.; Dauriat, G.; Mangiapan, G.; Rabbat, A.; Cadranel, J. Treatment of chronic pulmonary aspergillosis by voriconazole in nonimmunocompromised patients. Chest 2007, 131, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Saraceno, J.L.; Phelps, D.T.; Ferro, T.J.; Futerfas, R.; Schwartz, D.B. Chronic necrotizing pulmonary aspergillosis: Approach to management. Chest 1997, 112, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Camara, B.; Reymond, E.; Saint-Raymond, C.; Roth, H.; Brenier-Pinchart, M.P.; Pinel, C.; Cadranel, J.; Ferretti, G.; Pelloux, H.; Pison, C. Characteristics and outcomes of chronic pulmonary aspergillosis: A retrospective analysis of a tertiary hospital registry. Clin. Respir. J. 2014, 9, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Bhat, J.; Rajhan, A.; Agarwal, S.; Middleton, M.; Lehm, S. Non-tuberculous Mycobacterium incidence & treatment rates in university hospitals of North Midlands (UK). Eur. Respir. J. 2015, 46, PA2683. [Google Scholar]
- Lim, J.; Lyu, J.; Choi, C.M.; Oh, Y.M.; Lee, S.D.; Kim, W.S.; Kim, D.S.; Lee, H.; Shim, T.S. Non-tuberculous mycobacterial diseases presenting as solitary pulmonary nodules. Int. J. Tuberc. Lung Dis. 2010, 14, 1635–1640. [Google Scholar] [PubMed]
- Hafeez, I.; Muers, M.F.; Murphy, S.A.; Evans, E.G.; Barton, R.C.; McWhinney, P. Non-tuberculous mycobacterial lung infection complicated by chronic necrotising pulmonary aspergillosis. Thorax 2000, 55, 717–719. [Google Scholar] [CrossRef] [PubMed]
- Kobashi, Y.; Fukuda, M.; Yoshida, K.; Miyashita, N.; Niki, Y.; Oka, M. Chronic necrotizing pulmonary aspergillosis as a complication of pulmonary Mycobacterium avium complex disease. Respirology 2006, 11, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Kokkonouzis, I.; Athanasopoulos, I.; Doulgerakis, N.; Tsonis, G.; Lampaditis, I.; Saridis, N.; Skoufaras, V. Fatal hemoptysis due to chronic cavitary pulmonary aspergillosis complicated by nontuberculous mycobacterial tuberculosis. Case Rep. Infect. Dis. 2011, 2011, 837146. [Google Scholar] [CrossRef] [PubMed]
- Kunst, H.; Wickremasinghe, M.; Wells, A.; Wilson, R. Nontuberculous mycobacterial disease and Aspergillus-related lung disease in bronchiectasis. Eur. Respir. J. 2006, 28, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Takeda, K.; Imamura, Y.; Takazono, T.; Yoshida, M.; Ide, S.; Hirano, K.; Tashiro, M.; Saijo, T.; Kosai, K.; Morinaga, Y.; et al. The risk factors for developing of chronic pulmonary aspergillosis in nontuberculous mycobacteria patients and clinical characteristics and outcomes in chronic pulmonary aspergillosis patients coinfected with nontuberculous mycobacteria. Med. Mycol. 2015, 54, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Pleuvry, A.; Cole, D.C. Global burden of chronic pulmonary aspergillosis complicating sarcoidosis. Eur. Respir. J. 2013, 41, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Pena, T.A.; Soubani, A.O.; Samavati, L. Aspergillus lung disease in patients with sarcoidosis: A case series and review of the literature. Lung 2011, 189, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Keir, G.J.; Garfield, B.; Hansell, D.M.; Loebinger, M.R.; Wilson, R.; Renzoni, E.A.; Wells, A.U.; Maher, T.M. Cyclical caspofungin for chronic pulmonary aspergillosis in sarcoidosis. Thorax 2014, 69, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Lachkar, S.; Dominique, S.; Thiberville, L.; Nouvet, G.; Genevois, A. Aspergillosis and sarcoidosis. Rev. Mal. Respir. 2007, 24, 943–953. [Google Scholar] [CrossRef]
- Tamura, A.; Suzuki, J.; Fukami, T.; Matsui, H.; Akagawa, S.; Ohta, K.; Hebisawa, A.; Takahashi, F. Chronic pulmonary aspergillosis as a sequel to lobectomy for lung cancer. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Daste, A.; Gross-Goupil, M.; Ravaud, A. Pulmonary aspergilloma: An unexpected complication of radiofrequency ablation in the management of targeted therapy for a patient with metastatic renal cell carcinoma. Clin. Genitourin. Cancer 2014, 12, e115–e116. [Google Scholar] [CrossRef] [PubMed]
- Hiraki, T.; Gobara, H.; Mimura, H.; Sano, Y.; Takigawa, N.; Tanaka, T.; Kanazawa, S. Aspergilloma in a cavity formed after percutaneous radiofrequency ablation for lung cancer. J. Vasc. Interv. Radiol. 2009, 20, 1499–1500. [Google Scholar] [CrossRef] [PubMed]
- Alberti, N.; Frulio, N.; Trillaud, H.; Jougon, J.; Jullie, M.L.; Palussiere, J. Pulmonary aspergilloma in a cavity formed after percutaneous radiofrequency ablation. Cardiovasc. Interv. Radiol. 2014, 37, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2015, 47, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Koyama, K.; Ohshima, N.; Suzuki, J.; Kawashima, M.; Okuda, K.; Sato, R.; Suzukawa, M.; Nagai, H.; Matsui, H.; Ohta, K. Evaluation of clinical characteristics and prognosis of chronic pulmonary aspergillosis depending on the underlying lung diseases: Emphysema vs prior tuberculosis. J. Infect. Chemother. 2015, 21, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Kosmidis, C.; Denning, D.W. The clinical spectrum of pulmonary aspergillosis. Thorax 2014, 70, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Bafadhel, M.; McKenna, S.; Agbetile, J.; Fairs, A.; Desai, D.; Mistry, V.; Morley, J.P.; Pancholi, M.; Pavord, I.D.; Wardlaw, A.J.; et al. Aspergillus fumigatus during stable state and exacerbations of COPD. Eur. Respir. J. 2014, 43, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Lambourne, J.; Agranoff, D.; Herbrecht, R.; Troke, P.F.; Buchbinder, A.; Willis, F.; Letscher-Bru, V.; Agrawal, S.; Doffman, S.; Johnson, E.; et al. Association of mannose-binding lectin deficiency with acute invasive aspergillosis in immunocompromised patients. Clin. Infect. Dis. 2009, 49, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Crosdale, D.J.; Poulton, K.V.; Ollier, W.E.; Thomson, W.; Denning, D.W. Mannose-binding lectin gene polymorphisms as a susceptibility factor for chronic necrotizing pulmonary aspergillosis. J. Infect. Dis. 2001, 184, 653–656. [Google Scholar] [CrossRef] [PubMed]
- Doffinger, R.; Harris, C.; Lear, S.; Newton, P.; Alachkar, H.; Kumararatne, D.; Barcenas-Morales, G.; Denning, D. Impaired Th1 and Th17 immunity in chronic pulmonary aspergillosis. In Proceedings of the Advances against Aspergillosis, Madrid, Spain, 27 February–1 March 2014.
- Kelleher, P.; Goodsall, A.; Mulgirigama, A.; Kunst, H.; Henderson, D.C.; Wilson, R.; Newman-Taylor, A.; Levin, M. Interferon-γ therapy in two patients with progressive chronic pulmonary aspergillosis. Eur. Respir. J. 2006, 27, 1307–1310. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.L.; Denning, D.W. Clinical implications of interferon-γ genetic and epigenetic variants. Immunology 2014, 143, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.L.; Hankinson, J.; Simpson, A.; Bowyer, P.; Denning, D.W. A prominent role for the IL1 pathway and IL15 in susceptibility to chronic cavitary pulmonary aspergillosis. Clin. Microbiol. Infect. 2014, 20, O480–O488. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.L.; Hankinson, J.; Simpson, A.; Denning, D.W.; Bowyer, P. Reduced expression of TLR3, TLR10 and TREM1 by human macrophages in CCPA, and novel associations of VEGFA, DENND1B and PLAT. Clin. Microbiol. Infect. 2014, 20, O960–O968. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.L.; Bromley, M.J.; Denning, D.W.; Simpson, A.; Bowyer, P. Elevated levels of the neutrophil chemoattractant pro-platelet basic protein in macrophages from individuals with chronic and allergic aspergillosis. J. Infect. Dis. 2015, 211, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Hope, W.W.; Walsh, T.J.; Denning, D.W. The invasive and saprophytic syndromes due to Aspergillus spp. Med. Mycol. 2005, 43, S207–S238. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.R.; Hedayati, V.; Patel, K.; Hansell, D.M. Chronic aspergillosis of the lungs: Unravelling the terminology and radiology. Eur. Radiol. 2015, 25, 3100–3107. [Google Scholar] [CrossRef] [PubMed]
- Godet, C.; Laurent, F.; Beraud, G.; Toper, C.; Camara, B.; Philippe, B.; Germaud, P.; Cottin, V.; Beigelman-Aubry, C.; Khalil, A.; et al. Phenotyping chronic pulmonary aspergillosis by cluster analysis. Eur. Respir. J. 2015, 46, 1509–1512. [Google Scholar] [CrossRef] [PubMed]
- Izumikawa, K. Recent advances in chronic pulmonary aspergillosis. Respir. Investig. 2016, 54, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Izumikawa, K.; Tashiro, T.; Tashiro, M.; Takazono, T.; Kosai, K.; Morinaga, Y.; Kurihara, S.; Nakamura, S.; Imamura, Y.; Miyazaki, T.; et al. Pathogenesis and clinical features of chronic pulmonary aspergillosis—Is it possible to distinguish CNPA and CCPA clinically? J. Infect. Chemother. 2014, 20, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Al-Alawi, A.; Ryan, C.F.; Flint, J.D.; Muller, N.L. Aspergillus-related lung disease. Can. Respir. J. 2005, 12, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Godet, C.; Philippe, B.; Laurent, F.; Cadranel, J. Chronic pulmonary aspergillosis: An update on diagnosis and treatment. Respiration 2014, 88, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Jhun, B.W.; Jeon, K.; Eom, J.S.; Lee, J.H.; Suh, G.Y.; Kwon, O.J.; Koh, W.J. Clinical characteristics and treatment outcomes of chronic pulmonary aspergillosis. Med. Mycol. 2013, 51, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Patterson, K.C.; Strek, M.E. Diagnosis and treatment of pulmonary aspergillosis syndromes. Chest 2014, 146, 1358–1368. [Google Scholar] [CrossRef] [PubMed]
- Schweer, K.E.; Bangard, C.; Hekmat, K.; Cornely, O.A. Chronic pulmonary aspergillosis. Mycoses 2014, 57, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Attaway, A.H.; Jacono, F.; Gilkeson, R.; Faress, J.A. Subacute invasive pulmonary aspergillosis (SIPA) associated with ankylosing spondylitis (AS). Am. J. Respir. Crit. Care Med. 2015, 193, 572–573. [Google Scholar] [CrossRef] [PubMed]
- Nasim, A.; Baqi, S.; Zeeshan, S.M.; Aziz, T. Chronic necrotizing pulmonary aspergillosis in a renal transplant recipient. J. Pak. Med. Assoc. 2011, 61, 1242–1244. [Google Scholar] [PubMed]
- Denning, D.W.; Follansbee, S.E.; Scolaro, M.; Norris, S.; Edelstein, H.; Stevens, D.A. Pulmonary aspergillosis in the acquired immunodeficiency syndrome. N. Engl. J. Med. 1991, 324, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Franquet, T.; Muller, N.L.; Gimenez, A.; Domingo, P.; Plaza, V.; Bordes, R. Semiinvasive pulmonary aspergillosis in chronic obstructive pulmonary disease: Radiologic and pathologic findings in nine patients. AJR Am. J. Roentgenol. 2000, 174, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Ahn, B.C.; Lee, S.W.; Lee, J.; Kim, C. Pulmonary aspergilloma mimicking metastasis from papillary thyroid cancer. Thyroid 2011, 21, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Baser, S.; Onn, A.; Lin, E.; Morice, R.C.; Duvic, M. Pulmonary manifestations in patients with cutaneous t-cell lymphomas. Cancer 2007, 109, 1550–1555. [Google Scholar] [CrossRef] [PubMed]
- Sakuraba, M.; Sakao, Y.; Yamazaki, A.; Fukai, R.; Shiomi, K.; Sonobe, S.; Saito, Y.; Imashimizu, K.; Matsunaga, T.; Miyamoto, H. A case of aspergilloma detected after surgery for pneumothorax. Ann. Thorac. Cardiovasc. Surg. 2006, 12, 267–269. [Google Scholar] [PubMed]
- Yasuda, M.; Nagashima, A.; Haro, A.; Saitoh, G. Aspergilloma mimicking a lung cancer. Int. J. Surg. Case Rep. 2013, 4, 690–692. [Google Scholar] [CrossRef] [PubMed]
- Das, C.J.; Seith, A.; Debnath, J.; Kumar, U.; Sharma, S.G.; Aron, M. Aspergillus colonisation of pulmonary rheumatoid nodules: A rare cause of “bull’s eye” appearance. Indian J. Chest Dis. Allied Sci. 2009, 51, 41–43. [Google Scholar] [PubMed]
- Paone, G.; Nicastri, E.; Lucantoni, G.; Dello Iacono, R.; Battistoni, P.; D’Angeli, A.L.; Galluccio, G. Endobronchial ultrasound-driven biopsy in the diagnosis of peripheral lung lesions. Chest 2005, 128, 3551–3557. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Chenna, P.; Loiselle, A.; Massoni, J.; Mayse, M.; Misselhorn, D. Radial probe endobronchial ultrasound for peripheral pulmonary lesions. A 5-year institutional experience. Ann. Am. Thorac. Soc. 2014, 11, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Chenna, P.; Chen, A.C. Radial probe endobronchial ultrasound and novel navigation biopsy techniques. Semin. Respir. Crit. Care Med. 2014, 35, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Mudambi, L.; Ost, D.E. Advanced bronchoscopic techniques for the diagnosis of peripheral pulmonary lesions. Curr. Opin. Pulm. Med. 2016, 22, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.M.; Citron, K.M.; Strickland, B. Intrathoracic aspergilloma: Role of CT in diagnosis and treatment. Radiology 1987, 165, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Franquet, T.; Muller, N.L.; Gimenez, A.; Guembe, P.; de La Torre, J.; Bague, S. Spectrum of pulmonary aspergillosis: Histologic, clinical, and radiologic findings. Radiographics 2001, 21, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Soubani, A.O.; Chandrasekar, P.H. The clinical spectrum of pulmonary aspergillosis. Chest 2002, 121, 1988–1999. [Google Scholar] [CrossRef] [PubMed]
- Baxter, C.G.; Bishop, P.; Low, S.E.; Baiden-Amissah, K.; Denning, D.W. Pulmonary aspergillosis: An alternative diagnosis to lung cancer after positive [18F]FDG positron emission tomography. Thorax 2011, 66, 638–640. [Google Scholar] [CrossRef] [PubMed]
- Greene, R. The radiological spectrum of pulmonary aspergillosis. Med. Mycol. 2005, 43, S147–S154. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Lee, K.S.; Han, J.; Kim, J.; Kim, T.S.; Choo, S.W.; Kim, S.J. Semiinvasive pulmonary aspergillosis: CT and pathologic findings in six patients. AJR Am. J. Roentgenol. 2000, 174, 795–798. [Google Scholar] [CrossRef] [PubMed]
- Gefter, W.B.; Weingrad, T.R.; Epstein, D.M.; Ochs, R.H.; Miller, W.T. “Semi-invasive” Pulmonary aspergillosis: A new look at the spectrum of Aspergillus infections of the lung. Radiology 1981, 140, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Rajalingham, S.; Anshar, F.M. Chronic necrotizing pulmonary aspergillosis presenting as bilateral pleural effusion: A case report. J. Med. Case Rep. 2012, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Baliko, Z.; Sarosi, V.; Illes, M.B.; Varga, Z.; Hegedus, G.; Molnar, P.; Szakall, S. PET-CT imaging and reality. Pathol. Oncol. Res. 2011, 17, 393–395. [Google Scholar] [CrossRef] [PubMed]
- Felton, T.W.; Baxter, C.; Moore, C.B.; Roberts, S.A.; Hope, W.W.; Denning, D.W. Efficacy and safety of posaconazole for chronic pulmonary aspergillosis. Clin. Infect. Dis. 2010, 51, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Cadranel, J.; Philippe, B.; Hennequin, C.; Bergeron, A.; Bergot, E.; Bourdin, A.; Cottin, V.; Jeanfaivre, T.; Godet, C.; Pineau, M.; et al. Voriconazole for chronic pulmonary aspergillosis: A prospective multicenter trial. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 3231–3239. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Vishwanath, G.; Aggarwal, A.N.; Garg, M.; Gupta, D.; Chakrabarti, A. Itraconazole in chronic cavitary pulmonary aspergillosis: A randomised controlled trial and systematic review of literature. Mycoses 2013, 56, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Godet, C.; Laurent, F.; Bergeron, A.; Ingrand, P.; Beigelman-Aubry, C.; Camara, B.; Cottin, V.; Germaud, P.; Philippe, B.; Pison, C.; et al. Computed tomography assessment of response to treatment in chronic pulmonary aspergillosis. Chest 2016, 46, PA573. [Google Scholar] [CrossRef] [PubMed]
- Uffredi, M.L.; Mangiapan, G.; Cadranel, J.; Kac, G. Significance of Aspergillus fumigatus isolation from respiratory specimens of nongranulocytopenic patients. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Van Hoeyveld, E.; Dupont, L.; Bossuyt, X. Quantification of IgG antibodies to Aspergillus fumigatus and pigeon antigens by immunocap technology: An alternative to the precipitation technique? Clin. Chem. 2006, 52, 1785–1793. [Google Scholar] [CrossRef] [PubMed]
- Barton, R.C.; Hobson, R.P.; Denton, M.; Peckham, D.; Brownlee, K.; Conway, S.; Kerr, M.A. Serologic diagnosis of allergic bronchopulmonary aspergillosis in patients with cystic fibrosis through the detection of immunoglobulin g to Aspergillus fumigatus. Diagn. Microbiol. Infect. Dis. 2008, 62, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Page, I.D.; Richardson, M.D.; Denning, D.W. Comparison of six Aspergillus-specific IgG assays for the diagnosis of chronic pulmonary aspergillosis (CPA). J. Infect. 2016, 72, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Oliva, A.; Flori, P.; Hennequin, C.; Dubus, J.; Reynaud-Gaubert, M.; Charpin, D.; Vergnon, J.M.; Gay, P.; Colly, A.; Piarroux, R.; et al. Evaluation of the Aspergillus western blot IgG kit for diagnosis of chronic aspergillosis. J. Clin. Microbiol. 2015, 53, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Guitard, J.; Sendid, B.; Thorez, S.; Gits, M.; Hennequin, C. Evaluation of a recombinant antigen-based enzyme immunoassay for the diagnosis of noninvasive aspergillosis. J. Clin. Microbiol. 2012, 50, 762–765. [Google Scholar] [CrossRef] [PubMed]
- Dumollard, C.; Bailly, S.; Perriot, S.; Brenier-Pinchart, M.P.; Saint-Raymond, C.; Camara, B.; Gangneux, J.P.; Persat, F.; Valot, S.; Grenouillet, F.; et al. Prospective evaluation of a new Aspergillus IgG enzyme immunoassay kit for diagnosis of chronic and allergic pulmonary aspergillosis. J. Clin. Microbiol. 2016, 54, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Page, I.D.; Richardson, M.; Denning, D.W. Antibody testing in aspergillosis—Quo vadis? Med. Mycol. 2015, 53, 417–439. [Google Scholar] [CrossRef] [PubMed]
- Jain, L.R.; Denning, D.W. The efficacy and tolerability of voriconazole in the treatment of chronic cavitary pulmonary aspergillosis. J. Infect. 2006, 52, e133–e137. [Google Scholar] [CrossRef] [PubMed]
- Yousem, S.A. The histological spectrum of chronic necrotizing forms of pulmonary aspergillosis. Hum. Pathol. 1997, 28, 650–656. [Google Scholar] [CrossRef]
- Tochigi, N.; Ishiwatari, T.; Okubo, Y.; Ando, T.; Shinozaki, M.; Aki, K.; Gocho, K.; Hata, Y.; Murayama, S.Y.; Wakayama, M.; et al. Histological study of chronic pulmonary aspergillosis. Diagn. Pathol. 2015, 10, 153. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.D.; Warnock, D.W. Fungal Infection Diagnosis and Management, 4th ed.; Wiley-Blackwell: Singapore, 2012; pp. 167–200. [Google Scholar]
- Arvanitis, M.; Anagnostou, T.; Fuchs, B.B.; Caliendo, A.M.; Mylonakis, E. Molecular and nonmolecular diagnostic methods for invasive fungal infections. Clin. Microbiol. Rev. 2014, 27, 490–526. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.S.; Jeon, K.; Um, S.W.; Suh, G.Y.; Chung, M.P.; Kim, H.; Kwon, O.J.; Koh, W.J. Clinical characteristics and treatment outcomes of chronic necrotizing pulmonary aspergillosis: A review of 43 cases. Int. J. Infect. Dis. 2010, 14, e479–e482. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W. Chronic forms of pulmonary aspergillosis. Clin. Microbiol. Infect. 2001, 7, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Pashley, C.H.; Fairs, A.; Morley, J.P.; Tailor, S.; Agbetile, J.; Bafadhel, M.; Brightling, C.E.; Wardlaw, A.J. Routine processing procedures for isolating filamentous fungi from respiratory sputum samples may underestimate fungal prevalence. Med. Mycol. 2012, 50, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Fraczek, M.G.; Kirwan, M.B.; Moore, C.B.; Morris, J.; Denning, D.W.; Richardson, M.D. Volume dependency for culture of fungi from respiratory secretions and increased sensitivity of Aspergillus quantitative PCR. Mycoses 2014, 57, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Horvath, J.A.; Dummer, S. The use of respiratory-tract cultures in the diagnosis of invasive pulmonary aspergillosis. Am. J. Med. 1996, 100, 171–178. [Google Scholar] [CrossRef]
- Howard, S.J.; Cerar, D.; Anderson, M.J.; Albarrag, A.; Fisher, M.C.; Pasqualotto, A.C.; Laverdiere, M.; Arendrup, M.C.; Perlin, D.S.; Denning, D.W. Frequency and evolution of azole resistance in Aspergillus fumigatus associated with treatment failure. Emerg. Infect. Dis. 2009, 15, 1068–1076. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Perlin, D.S. Azole resistance in Aspergillus: A growing public health menace. Future Microbiol. 2011, 6, 1229–1232. [Google Scholar] [CrossRef] [PubMed]
- Langridge, P.J.; Sheehan, R.L.; Denning, D.W. Microbial yield from physiotherapy assisted sputum production in respiratory outpatients. BMC Pulm. Med. 2016, 16, 23. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Park, S.; Lass-Florl, C.; Fraczek, M.G.; Kirwan, M.; Gore, R.; Smith, J.; Bueid, A.; Moore, C.B.; Bowyer, P.; et al. High-frequency triazole resistance found in nonculturable Aspergillus fumigatus from lungs of patients with chronic fungal disease. Clin. Infect. Dis. 2011, 52, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Baxter, C.G.; Dunn, G.; Jones, A.M.; Webb, K.; Gore, R.; Richardson, M.D.; Denning, D.W. Novel immunologic classification of aspergillosis in adult cystic fibrosis. J. Allergy Clin. Immunol. 2013, 132, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Baxter, C.G.; Jones, A.M.; Webb, K.; Denning, D.W. Homogenisation of cystic fibrosis sputum by sonication--an essential step for Aspergillus PCR. J. Microbiol. Methods 2011, 85, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Baxter, C.G.; Rautemaa, R.; Jones, A.M.; Webb, A.K.; Bull, M.; Mahenthiralingam, E.; Denning, D.W. Intravenous antibiotics reduce the presence of Aspergillus in adult cystic fibrosis sputum. Thorax 2013, 68, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Arvanitis, M.; Ziakas, P.D.; Zacharioudakis, I.M.; Zervou, F.N.; Caliendo, A.M.; Mylonakis, E. PCR in diagnosis of invasive aspergillosis: A meta-analysis of diagnostic performance. J. Clin. Microbiol. 2014, 52, 3731–3742. [Google Scholar] [CrossRef] [PubMed]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised definitions of invasive fungal disease from the european organization for research and treatment of cancer/invasive fungal infections cooperative group and the national institute of allergy and infectious diseases mycoses study group (EORTC/MSG) consensus group. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [PubMed]
- Mennink-Kersten, M.A.; Ruegebrink, D.; Klont, R.R.; Warris, A.; Blijlevens, N.M.; Donnelly, J.P.; Verweij, P.E. Improved detection of circulating Aspergillus antigen by use of a modified pretreatment procedure. J. Clin. Microbiol. 2008, 46, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Penack, O.; Rempf, P.; Graf, B.; Blau, I.W.; Thiel, E. Aspergillus galactomannan testing in patients with long-term neutropenia: Implications for clinical management. Ann. Oncol. 2008, 19, 984–989. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Lee, S.O.; Choi, S.H.; Jeong, J.Y.; Sung, H.; Kim, M.N.; Choi, C.M.; Hong, S.B.; Oh, Y.M.; Shim, T.S.; et al. Serum and bronchoalveolar lavage fluid galactomannan assays in patients with pulmonary aspergilloma. Clin. Infect. Dis. 2011, 52, e149–e152. [Google Scholar] [CrossRef] [PubMed]
- Racil, Z.; Kocmanova, I.; Wagnerova, B.; Winterova, J.; Mayer, J. Contribution of galactomannan antigen detection to early diagnosis of invasive aspergillosis. Klin. Mikrobiol. Infekc. Lek. 2007, 13, 176–183. [Google Scholar] [PubMed]
- Wheat, L.J.; Walsh, T.J. Diagnosis of invasive aspergillosis by galactomannan antigenemia detection using an enzyme immunoassay. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Marr, K.A.; Balajee, S.A.; McLaughlin, L.; Tabouret, M.; Bentsen, C.; Walsh, T.J. Detection of galactomannan antigenemia by enzyme immunoassay for the diagnosis of invasive aspergillosis: Variables that affect performance. J. Infect. Dis. 2004, 190, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.J.; Shoham, S.; Petraitiene, R.; Sein, T.; Schaufele, R.; Kelaher, A.; Murray, H.; Mya-San, C.; Bacher, J.; Petraitis, V. Detection of galactomannan antigenemia in patients receiving piperacillin-tazobactam and correlations between in vitro, in vivo, and clinical properties of the drug-antigen interaction. J. Clin. Microbiol. 2004, 42, 4744–4748. [Google Scholar] [CrossRef] [PubMed]
- Izumikawa, K.; Yamamoto, Y.; Mihara, T.; Takazono, T.; Morinaga, Y.; Kurihara, S.; Nakamura, S.; Imamura, Y.; Miyazaki, T.; Nishino, T.; et al. Bronchoalveolar lavage galactomannan for the diagnosis of chronic pulmonary aspergillosis. Med. Mycol. 2012, 50, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Kono, Y.; Tsushima, K.; Yamaguchi, K.; Kurita, N.; Soeda, S.; Fujiwara, A.; Sugiyama, S.; Togashi, Y.; Kasagi, S.; To, M.; et al. The utility of galactomannan antigen in the bronchial washing and serum for diagnosing pulmonary aspergillosis. Respir. Med. 2013, 107, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Shin, B.; Koh, W.J.; Jeong, B.H.; Yoo, H.; Park, H.Y.; Suh, G.Y.; Kwon, O.J.; Jeon, K. Serum galactomannan antigen test for the diagnosis of chronic pulmonary aspergillosis. J. Infect. 2014, 68, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Kitasato, Y.; Tao, Y.; Hoshino, T.; Tachibana, K.; Inoshima, N.; Yoshida, M.; Takata, S.; Okabayashi, K.; Kawasaki, M.; Iwanaga, T.; et al. Comparison of Aspergillus galactomannan antigen testing with a new cut-off index and Aspergillus precipitating antibody testing for the diagnosis of chronic pulmonary aspergillosis. Respirology 2009, 14, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Sav, H.; Atalay, M.A.; Demir, G.; Akif Ozdemir, M.; Nedret Koc, A. Early diagnosis of cerebral aspergillosis with various methods: A case report. Infez. Med. 2013, 21, 134–138. [Google Scholar] [PubMed]
- Tanase, A.D.; Colita, A.; Marculescu, A.; Berteanu, C.; Streinu Cercel, A.; Stoica, M.; Stoica, A.; Cernea, D.; Copotoiu, S.; Brinzaniuc, K.; et al. Using the galactomannan antigen assay in the diagnosis of invasive aspergillosis after hematopoietic stem cell transplantation. Rom. J. Morphol. Embryol. 2012, 53, 379–382. [Google Scholar] [PubMed]
- Clark, A.E.; Kaleta, E.J.; Arora, A.; Wolk, D.M. Matrix-assisted laser desorption ionization-time of flight mass spectrometry: A fundamental shift in the routine practice of clinical microbiology. Clin. Microbiol. Rev. 2013, 26, 547–603. [Google Scholar] [CrossRef] [PubMed]
- Normand, A.C.; Cassagne, C.; Ranque, S.; L’Ollivier, C.; Fourquet, P.; Roesems, S.; Hendrickx, M.; Piarroux, R. Assessment of various parameters to improve MALDI-TOF MS reference spectra libraries constructed for the routine identification of filamentous fungi. BMC Microbiol. 2013, 13, 76. [Google Scholar] [CrossRef] [PubMed]
- Posteraro, B.; De Carolis, E.; Vella, A.; Sanguinetti, M. Maldi-tof mass spectrometry in the clinical mycology laboratory: Identification of fungi and beyond. Expert Rev. Proteom. 2013, 10, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Cassagne, C.; Ranque, S.; Normand, A.C.; Fourquet, P.; Thiebault, S.; Planard, C.; Hendrickx, M.; Piarroux, R. Mould routine identification in the clinical laboratory by matrix-assisted laser desorption ionization time-of-flight mass spectrometry. PLoS ONE 2011, 6, e28425. [Google Scholar] [CrossRef] [PubMed]
- Sanguinetti, M.; Posteraro, B. Maldi-tof mass spectrometry: Any use for aspergilli? Mycopathologia 2014, 178, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.; Paterson, R.R.; Venancio, A.; Lima, N. Filamentous fungal characterizations by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. J. Appl. Microbiol. 2010, 108, 375–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welker, M. Proteomics for routine identification of microorganisms. Proteomics 2011, 11, 3143–3153. [Google Scholar] [CrossRef] [PubMed]
- Prattes, J.; Lackner, M.; Eigl, S.; Reischies, F.; Raggam, R.B.; Koidl, C.; Flick, H.; Wurm, R.; Palfner, M.; Wolfler, A.; et al. Diagnostic accuracy of the Aspergillus-specific bronchoalveolar lavage lateral-flow assay in haematological malignancy patients. Mycoses 2015, 58, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Chambers, S.T.; Syhre, M.; Murdoch, D.R.; McCartin, F.; Epton, M.J. Detection of 2-pentylfuran in the breath of patients with Aspergillus fumigatus. Med. Mycol. 2009, 47, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, B.; Basanta, M.; Cadden, P.; Singh, D.; Douce, D.; Woodcock, A.; Fowler, S.J. Non-invasive phenotyping using exhaled volatile organic compounds in asthma. Thorax 2011, 66, 804–809. [Google Scholar] [CrossRef] [PubMed]
- Basanta, M.; Ibrahim, B.; Dockry, R.; Douce, D.; Morris, M.; Singh, D.; Woodcock, A.; Fowler, S.J. Exhaled volatile organic compounds for phenotyping chronic obstructive pulmonary disease: A cross-sectional study. Respir. Res. 2012, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Bazemore, R.A.; Feng, J.; Cseke, L.; Podila, G.K. Biomedically important pathogenic fungi detection with volatile biomarkers. J. Breath Res. 2012, 6, 016002. [Google Scholar] [CrossRef] [PubMed]
- Chambers, S.T.; Scott-Thomas, A.; Epton, M. Developments in novel breath tests for bacterial and fungal pulmonary infection. Curr. Opin. Pulm. Med. 2012, 18, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Heddergott, C.; Calvo, A.M.; Latge, J.P. The volatome of Aspergillus fumigatus. Eukaryot. Cell 2014, 13, 1014–1025. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.; Thomas, H.R.; Daniels, S.D.; Lynch, R.C.; Fortier, S.M.; Shea, M.M.; Rearden, P.; Comolli, J.C.; Baden, L.R.; Marty, F.M. A breath fungal secondary metabolite signature to diagnose invasive aspergillosis. Clin. Infect. Dis. 2014, 59, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.J.; Anaissie, E.J.; Denning, D.W.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Segal, B.H.; Steinbach, W.J.; Stevens, D.A.; et al. Treatment of aspergillosis: Clinical practice guidelines of the infectious diseases society of america. Clin. Infect. Dis. 2008, 46, 327–360. [Google Scholar] [CrossRef] [PubMed]
- Farid, S.; Mohamed, S.; Devbhandari, M.; Kneale, M.; Richardson, M.; Soon, S.Y.; Jones, M.T.; Krysiak, P.; Shah, R.; Denning, D.W.; et al. Results of surgery for chronic pulmonary aspergillosis, optimal antifungal therapy and proposed high risk factors for recurrence—A national centre’s experience. J. Cardiothorac. Surg. 2013, 8, 180. [Google Scholar] [CrossRef] [PubMed]
- Brik, A.; Salem, A.M.; Kamal, A.R.; Abdel-Sadek, M.; Essa, M.; El Sharawy, M.; Deebes, A.; Bary, K.A. Surgical outcome of pulmonary aspergilloma. Eur. J. Cardiothorac. Surg. 2008, 34, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Regnard, J.F.; Icard, P.; Nicolosi, M.; Spagiarri, L.; Magdeleinat, P.; Jauffret, B.; Levasseur, P. Aspergilloma: A series of 89 surgical cases. Ann. Thorac. Surg. 2000, 69, 898–903. [Google Scholar] [CrossRef]
- Judson, M.A.; Stevens, D.A. The treatment of pulmonary aspergilloma. Curr. Opin. Investig. Drugs 2001, 2, 1375–1377. [Google Scholar] [PubMed]
- De Beule, K.; De Doncker, P.; Cauwenbergh, G.; Koster, M.; Legendre, R.; Blatchford, N.; Daunas, J.; Chwetzoff, E. The treatment of aspergillosis and aspergilloma with itraconazole, clinical results of an open international study (1982–1987). Mycoses 1988, 31, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Dupont, B. Itraconazole therapy in aspergillosis: Study in 49 patients. J. Am. Acad. Dermatol. 1990, 23, 607–614. [Google Scholar] [CrossRef]
- Gupta, P.R.; Jain, S.; Kewlani, J.P. A comparative study of itraconazole in various dose schedules in the treatment of pulmonary aspergilloma in treated patients of pulmonary tuberculosis. Lung India 2015, 32, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Cucchetto, G.; Cazzadori, A.; Conti, M.; Cascio, G.L.; Braggio, P.; Concia, E. Treatment of chronic pulmonary aspergillosis with voriconazole: Review of a case series. Infection 2015, 43, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Fujiuchi, S.; Tao, Y.; Sasaki, Y.; Ogawa, K.; Suzuki, K.; Tada, A.; Kuba, M.; Kato, T.; Kawabata, M.; et al. Efficacy and safety of voriconazole in the treatment of chronic pulmonary aspergillosis: Experience in Japan. Infection 2012, 40, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Al-Shair, K.; Atherton, G.T.; Harris, C.; Ratcliffe, L.; Newton, P.J.; Denning, D.W. Long-term antifungal treatment improves health status in patients with chronic pulmonary aspergillosis: A longitudinal analysis. Clin. Infect. Dis. 2013, 57, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Al-shair, K.; Atherton, G.T.; Kennedy, D.; Powell, G.; Denning, D.W.; Caress, A. Validity and reliability of the St. George’s respiratory questionnaire in assessing health status in patients with chronic pulmonary aspergillosis. Chest 2013, 144, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Miceli, M.H.; Kauffman, C.A. Isavuconazole: A new broad-spectrum triazole antifungal agent. Clin. Infect. Dis. 2015, 61, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Schmitt-Hoffmann, A.; Roos, B.; Heep, M.; Schleimer, M.; Weidekamm, E.; Brown, T.; Roehrle, M.; Beglinger, C. Single-ascending-dose pharmacokinetics and safety of the novel broad-spectrum antifungal triazole bal4815 after intravenous infusions (50, 100, and 200 milligrams) and oral administrations (100, 200, and 400 milligrams) of its prodrug, BAL8557, in healthy volunteers. Antimicrob. Agents Chemother. 2006, 50, 279–285. [Google Scholar] [PubMed]
- Newton, P.N.; Harris, C.; Denning, D.W. The clinical response to a short term course of intravenous liposomal amphotericin B therapy in patients with chronic pulmonary aspergillosis. Mycoses 2013, 56, 164–165. [Google Scholar]
- Kohno, S.; Izumikawa, K.; Kakeya, H.; Miyazaki, Y.; Ogawa, K.; Amitani, R.; Niki, Y.; Kurashima, A. Clinical efficacy and safety of micafungin in Japanese patients with chronic pulmonary aspergillosis: A prospective observational study. Med. Mycol. 2011, 49, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Ouchi, H.; Fujita, M.; Ikegame, S.; Inoshima, I.; Harada, E.; Nakanishi, Y. Successful treatment of refractory chronic necrotizing pulmonary aspergillosis with micafungin. J. Infect. Chemother. 2007, 13, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Izumikawa, K.; Ohtsu, Y.; Kawabata, M.; Takaya, H.; Miyamoto, A.; Sakamoto, S.; Kishi, K.; Tsuboi, E.; Homma, S.; Yoshimura, K. Clinical efficacy of micafungin for chronic pulmonary aspergillosis. Med. Mycol. 2007, 45, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Kohno, S.; Izumikawa, K.; Ogawa, K.; Kurashima, A.; Okimoto, N.; Amitani, R.; Kakeya, H.; Niki, Y.; Miyazaki, Y. Intravenous micafungin versus voriconazole for chronic pulmonary aspergillosis: A multicenter trial in Japan. J. Infect. 2010, 61, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Kohno, S.; Izumikawa, K.; Yoshida, M.; Takesue, Y.; Oka, S.; Kamei, K.; Miyazaki, Y.; Yoshinari, T.; Kartsonis, N.A.; Niki, Y. A double-blind comparative study of the safety and efficacy of caspofungin versus micafungin in the treatment of candidiasis and aspergillosis. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Ananda-Rajah, M.; Andes, D.; Arendrup, M.C.; Bruggemann, R.J.; Chowdhary, A.; Cornely, O.A.; Denning, D.W.; Groll, A.H.; Izumikawa, K.; et al. International expert opinion on the management of infection caused by azole-resistant Aspergillus fumigatus. Drug Resist. Updates 2015, 21–22, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Jensen, R.H.; Cuenca-Estrella, M. In vitro activity of Asp2397 against Aspergillus isolates with or without acquired azole resistance mechanisms. Antimicrob. Agents Chemother. 2015, 60, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Bromley, M.J. Infectious disease. How to bolster the antifungal pipeline. Science 2015, 347, 1414–1416. [Google Scholar] [CrossRef] [PubMed]
- Perfect, J.R. Is there an emerging need for new antifungals? Expert. Opin. Emerg. Drugs 2016. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F.; Juvvadi, P.R.; Steinbach, W.J. Editorial: Advances in Aspergillus fumigatus pathobiology. Front. Microbiol. 2016, 7, 43. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, W.J.; Garvey, E.P.; Moore, W.R.; Rafferty, S.W.; Yates, C.M.; Schotzinger, R.J. Design and optimization of highly-selective fungal CYP51 inhibitors. Bioorg. Med. Chem. Lett. 2014, 24, 3455–3458. [Google Scholar] [CrossRef] [PubMed]
- Warrilow, A.G.; Hull, C.M.; Parker, J.E.; Garvey, E.P.; Hoekstra, W.J.; Moore, W.R.; Schotzinger, R.J.; Kelly, D.E.; Kelly, S.L. The clinical candidate VT-1161 is a highly potent inhibitor of Candida albicans CYP51 but fails to bind the human enzyme. Antimicrob. Agents Chemother. 2014, 58, 7121–7127. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.K.; Jiang, G.N.; Ding, J.A. Surgical treatment for pulmonary aspergilloma: A 35-year experience in the Chinese population. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Muniappan, A.; Tapias, L.F.; Butala, P.; Wain, J.C.; Wright, C.D.; Donahue, D.M.; Gaissert, H.A.; Lanuti, M.; Mathisen, D.J. Surgical therapy of pulmonary aspergillomas: A 30-year North American experience. Ann. Thorac. Surg. 2014, 97, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Akbari, J.G.; Varma, P.K.; Neema, P.K.; Menon, M.U.; Neelakandhan, K.S. Clinical profile and surgical outcome for pulmonary aspergilloma: A single center experience. Ann. Thorac. Surg. 2005, 80, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Pratap, H.; Dewan, R.K.; Singh, L.; Gill, S.; Vaddadi, S. Surgical treatment of pulmonary aspergilloma: A series of 72 cases. Indian J. Chest Dis. Allied. Sci. 2007, 49, 23–27. [Google Scholar] [PubMed]
- Kim, Y.T.; Kang, M.C.; Sung, S.W.; Kim, J.H. Good long-term outcomes after surgical treatment of simple and complex pulmonary aspergilloma. Ann. Thorac. Surg. 2005, 79, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.K.; Chen, C.; Chen, X.F.; Jiang, G.N. Video-assisted thoracic surgery for pulmonary aspergilloma: A safe and effective procedure. Ann. Thorac. Surg. 2014, 97, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Yuan, P.; Wang, Z.; Bao, F.; Yang, Y.; Hu, J. Is video-assisted thoracic surgery a versatile treatment for both simple and complex pulmonary aspergilloma? J. Thorac. Dis. 2014, 6, 86–90. [Google Scholar] [PubMed]
- Sagan, D.; Gozdziuk, K. Surgery for pulmonary aspergilloma in immunocompetent patients: No benefit from adjuvant antifungal pharmacotherapy. Ann. Thorac. Surg. 2010, 89, 1603–1610. [Google Scholar] [CrossRef] [PubMed]
- Sagan, D.; Gozdziuk, K.; Korobowicz, E. Predictive and prognostic value of preoperative symptoms in the surgical treatment of pulmonary aspergilloma. J. Surg. Res. 2010, 163, e35–e43. [Google Scholar] [CrossRef] [PubMed]
- Benhamed, L.; Woelffle, D. Adjuvant antifungal therapy after pulmonary surgery for aspergilloma: Is it useful? Interact. Cardiovasc. Thorac. Surg. 2014, 18, 835–837. [Google Scholar] [CrossRef] [PubMed]
- Serasli, E.; Kalpakidis, V.; Iatrou, K.; Tsara, V.; Siopi, D.; Christaki, P. Percutaneous bronchial artery embolization in the management of massive hemoptysis in chronic lung diseases. Immediate and long-term outcomes. Int. Angiol. 2008, 27, 319–328. [Google Scholar] [PubMed]
- Swanson, K.L.; Johnson, C.M.; Prakash, U.B.; McKusick, M.A.; Andrews, J.C.; Stanson, A.W. Bronchial artery embolization: Experience with 54 patients. Chest 2002, 121, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Rumbak, M.; Kohler, G.; Eastrige, C.; Winer-Muram, H.; Gavant, M. Topical treatment of life threatening haemoptysis from aspergillomas. Thorax 1996, 51, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, J.N.; Berry, M.W.; Schabel, S.I.; Judson, M.A. A modern series of percutaneous intracavitary instillation of amphotericin B for the treatment of severe hemoptysis from pulmonary aspergilloma. Chest 2013, 143, 1414–1421. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, M.J.; Albelda, S.M.; Mayock, R.L.; McLean, G.K. Severe hemoptysis associated with pulmonary aspergilloma. Percutaneous intracavitary treatment. Chest 1988, 94, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Ribaud, P.; Milpied, N.; Caillot, D.; Herbrecht, R.; Thiel, E.; Haas, A.; Ruhnke, M.; Lode, H. Efficacy and safety of voriconazole in the treatment of acute invasive aspergillosis. Clin. Infect. Dis. 2002, 34, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Tucker, R.M.; Haq, Y.; Denning, D.W.; Stevens, D.A. Adverse events associated with itraconazole in 189 patients on chronic therapy. J. Antimicrob. Chemother. 1990, 26, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Poluzzi, E.; Koci, A.; Caraceni, P.; Ponti, F.D. Assessing liver injury associated with antimycotics: Concise literature review and clues from data mining of the faers database. World J. Hepatol. 2014, 6, 601–612. [Google Scholar] [PubMed]
- Lebeaux, D.; Lanternier, F.; Elie, C.; Suarez, F.; Buzyn, A.; Viard, J.P.; Bougnoux, M.E.; Lecuit, M.; Jullien, V.; Lortholary, O. Therapeutic drug monitoring of posaconazole: A monocentric study with 54 adults. Antimicrob. Agents Chemother. 2009, 53, 5224–5229. [Google Scholar] [CrossRef] [PubMed]
- Foo, H.; Gottlieb, T. Lack of cross-hepatotoxicity between voriconazole and posaconazole. Clin. Infect. Dis. 2007, 45, 803–805. [Google Scholar] [CrossRef] [PubMed]
- Spellberg, B.; Rieg, G.; Bayer, A.; Edwards, J.E., Jr. Lack of cross-hepatotoxicity between fluconazole and voriconazole. Clin. Infect. Dis. 2003, 36, 1091–1093. [Google Scholar] [CrossRef] [PubMed]
- Baxter, C.G.; Marshall, A.; Roberts, M.; Felton, T.W.; Denning, D.W. Peripheral neuropathy in patients on long-term triazole antifungal therapy. J. Antimicrob. Chemother. 2011, 66, 2136–2139. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, F.; Akdogan, E.; Aydin, K.; Yilmaz, M.; Altunayoglu, V.; Sozen, E.E.; Omay, S.B.; Koksal, I. Voriconazole-induced neuropathy. Chemotherapy 2008, 54, 224–227. [Google Scholar] [CrossRef] [PubMed]
- Karadi, R.L.; Gow, D.; Kellett, M.; Denning, D.W.; O’Driscoll, R.B. Itraconazole associated quadriparesis and edema: A case report. J. Med. Case Rep. 2011, 5, 140. [Google Scholar] [CrossRef] [PubMed]
- Tsiodras, S.; Zafiropoulou, R.; Kanta, E.; Demponeras, C.; Karandreas, N.; Manesis, E.K. Painful peripheral neuropathy associated with voriconazole use. Arch. Neurol. 2005, 62, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Vollenbroich, R.; Maeder, M.T.; Weilenmann, D. Congestive heart failure related to antifungal therapy with itraconazole. Int. J. Cardiol. 2014, 172, e170–e171. [Google Scholar] [CrossRef] [PubMed]
- Hauben, M.; Hung, E.Y. A quantitative analysis of the spontaneous reporting of congestive heart failure-related adverse events with systemic anti-fungal drugs. J. Clin. Pharmacol. 2013, 53, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Kurashima, A.; Kamei, K.; Oritsu, M.; Ando, T.; Yamamoto, T.; Niki, Y. Efficacy and safety of short- and long-term treatment of itraconazole on chronic necrotizing pulmonary aspergillosis in multicenter study. J. Infect. Chemother. 2012, 18, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Fung, S.L.; Chau, C.H.; Yew, W.W. Cardiovascular adverse effects during itraconazole therapy. Eur. Respir. J. 2008, 32, 240. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.R.; Singer, S.J.; Leissa, B.G. Congestive heart failure associated with itraconazole. Lancet 2001, 57, 1766–1767. [Google Scholar] [CrossRef]
- Malani, A.N.; Aronoff, D.M. Voriconazole-induced photosensitivity. Clin. Med. Res. 2008, 6, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Vohringer, S.; Schrum, J.; Ott, H.; Hoger, P.H. Severe phototoxicity associated with long-term voriconazole treatment. J. Dtsch. Dermatol. Ges. 2011, 9, 274–276. [Google Scholar] [CrossRef] [PubMed]
- Goyal, R.K. Voriconazole-associated phototoxic dermatoses and skin cancer. Expert Rev. Anti Infect. Ther. 2015, 13. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Griffiths, C.E. Muco-cutaneous retinoid-effects and facial erythema related to the novel triazole antifungal agent voriconazole. Clin. Exp. Dermatol. 2001, 26, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.F.; Wang, T.; Altman, R.; Eshaghian, P.; Lynch, J.P., 3rd; Ross, D.J.; Belperio, J.A.; Weigt, S.S.; Saggar, R.; Gregson, A.; et al. Periostitis secondary to prolonged voriconazole therapy in lung transplant recipients. Am. J. Transpl. 2009, 9, 2845–2850. [Google Scholar] [CrossRef] [PubMed]
- Skiles, J.L.; Imel, E.A.; Christenson, J.C.; Bell, J.E.; Hulbert, M.L. Fluorosis because of prolonged voriconazole therapy in a teenager with acute myelogenous leukemia. J. Clin. Oncol. 2011, 29, e779–e782. [Google Scholar] [CrossRef] [PubMed]
- Wermers, R.A.; Cooper, K.; Razonable, R.R.; Deziel, P.J.; Whitford, G.M.; Kremers, W.K.; Moyer, T.P. Fluoride excess and periostitis in transplant patients receiving long-term voriconazole therapy. Clin. Infect. Dis. 2011, 52, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Rossier, C.; Dunet, V.; Tissot, F.; Aubry-Rozier, B.; Marchetti, O.; Boubaker, A. Voriconazole-induced periostitis. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 375–376. [Google Scholar] [CrossRef] [PubMed]
- Tailor, T.D.; Richardson, M.L. Case 215: Voriconazole-induced periostitis. Radiology 2015, 274, 930–935. [Google Scholar] [CrossRef] [PubMed]
- Moon, W.J.; Scheller, E.L.; Suneja, A.; Livermore, J.A.; Malani, A.N.; Moudgal, V.; Kerr, L.E.; Ferguson, E.; Vandenberg, D.M. Plasma fluoride level as a predictor of voriconazole-induced periostitis in patients with skeletal pain. Clin. Infect. Dis. 2014, 59, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, R. Fluoride and bone—Quantity versus quality. N. Engl. J. Med. 1990, 322, 845–846. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.C.; Sanchez, C.J., Jr.; Niece, K.L.; Wenke, J.C.; Akers, K.S. Voriconazole enhances osteogenic activity of human osteoblasts in vitro through a fluoride-independent mechanism. Antimicrob. Agents Chemother. 2015, 59, 7205–7213. [Google Scholar] [CrossRef] [PubMed]
- Xiong, W.H.; Brown, R.L.; Reed, B.; Burke, N.S.; Duvoisin, R.M.; Morgans, C.W. Voriconazole, an antifungal triazol that causes visual side effects, is an inhibitor of TRPM1 and TRPM3 channels. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1367–1373. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.B.; Kauffman, C.A. Voriconazole: A new triazole antifungal agent. Clin. Infect. Dis. 2003, 36, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Bayhan, G.I.; Garipardic, M.; Karaman, K.; Akbayram, S. Voriconazole-associated visual disturbances and hallucinations. Cutan. Ocul. Toxicol. 2015, 35, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Zonios, D.; Yamazaki, H.; Murayama, N.; Natarajan, V.; Palmore, T.; Childs, R.; Skinner, J.; Bennett, J.E. Voriconazole metabolism, toxicity, and the effect of cytochrome P450 2C19 genotype. J. Infect. Dis. 2014, 209, 1941–1948. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, J.S.; Banfield, S.; Atherton, G.T.; Denning, D.W. Comment on: Antifungal therapy: Drug-drug interactions at your fingertips. J. Antimicrob. Chemother. 2016. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.M.; Park, H.Y.; Jeong, B.H.; Jeon, K.; Lee, S.Y.; Koh, W.J. Effect of rifampin and rifabutin on serum itraconazole levels in patients with chronic pulmonary aspergillosis and coexisting nontuberculous mycobacterial infection. Antimicrob. Agents Chemother. 2015, 59, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Schwiesow, J.N.; Iseman, M.D.; Peloquin, C.A. Concomitant use of voriconazole and rifabutin in a patient with multiple infections. Pharmacotherapy 2008, 28, 1076–1080. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, H.; Li, R.; Bu, D.; Wan, Z. Mutations in the CYP51A gene and susceptibility to itraconazole in Aspergillus fumigatus serially isolated from a patient with lung aspergilloma. J. Antimicrob. Chemother. 2005, 55, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Howard, S.J.; Pasqualotto, A.C.; Denning, D.W. Azole resistance in allergic bronchopulmonary aspergillosis and Aspergillus bronchitis. Clin. Microbiol. Infect. 2010, 16, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Mavridou, E.; Mortensen, K.L.; Snelders, E.; Frimodt-Moller, N.; Khan, H.; Melchers, W.J.; Verweij, P.E. Development of azole resistance in Aspergillus fumigatus during azole therapy associated with change in virulence. PLoS ONE 2010, 5, e10080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Ingen, J.; van der Lee, H.A.; Rijs, A.J.; Snelders, E.; Melchers, W.J.; Verweij, P.E. High-level pan-azole-resistant aspergillosis. J. Clin. Microbiol. 2015, 53, 2343–2345. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Snelders, E.; Kema, G.H.; Mellado, E.; Melchers, W.J. Azole resistance in Aspergillus fumigatus: A side-effect of environmental fungicide use? Lancet Infect. Dis. 2009, 9, 789–795. [Google Scholar] [CrossRef]
- Snelders, E.; Camps, S.M.; Karawajczyk, A.; Schaftenaar, G.; Kema, G.H.; van der Lee, H.A.; Klaassen, C.H.; Melchers, W.J.; Verweij, P.E. Triazole fungicides can induce cross-resistance to medical triazoles in Aspergillus fumigatus. PLoS ONE 2012, 7, e31801. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Kathuria, S.; Xu, J.; Meis, J.F. Emergence of azole-resistant Aspergillus fumigatus strains due to agricultural azole use creates an increasing threat to human health. PLoS Pathog. 2013, 9, e1003633. [Google Scholar] [CrossRef]
- Denning, D.W.; Venkateswarlu, K.; Oakley, K.L.; Anderson, M.J.; Manning, N.J.; Stevens, D.A.; Warnock, D.W.; Kelly, S.L. Itraconazole resistance in Aspergillus fumigatus. Antimicrob. Agents Chemother. 1997, 41, 1364–1368. [Google Scholar] [PubMed]
- Snelders, E.; van der Lee, H.A.; Kuijpers, J.; Rijs, A.J.; Varga, J.; Samson, R.A.; Mellado, E.; Donders, A.R.; Melchers, W.J.; Verweij, P.E. Emergence of azole resistance in Aspergillus fumigatus and spread of a single resistance mechanism. PLoS Med. 2008, 5, e219. [Google Scholar] [CrossRef] [PubMed]
- Lestrade, P.P.; Meis, J.F.; Arends, J.P.; van der Beek, M.T.; de Brauwer, E.; van Dijk, K.; de Greeff, S.C.; Haas, P.J.; Hodiamont, C.J.; Kuijper, E.J.; et al. Diagnosis and management of aspergillosis in The Netherlands: A national survey. Mycoses 2016, 59, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Bader, O.; Tunnermann, J.; Dudakova, A.; Tangwattanachuleeporn, M.; Weig, M.; Gross, U. Environmental isolates of azole-resistant Aspergillus fumigatus in Germany. Antimicrob. Agents Chemother. 2015, 59, 4356–4359. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; Kathuria, S.; Hagen, F.; Meis, J.F. Prevalence and mechanism of triazole resistance in Aspergillus fumigatus in a referral chest hospital in Delhi, India and an update of the situation in Asia. Front. Microbiol. 2015, 6, 428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Linden, J.W.; Arendrup, M.C.; Warris, A.; Lagrou, K.; Pelloux, H.; Hauser, P.M.; Chryssanthou, E.; Mellado, E.; Kidd, S.E.; Tortorano, A.M.; et al. Prospective multicenter international surveillance of azole resistance in Aspergillus fumigatus. Emerg. Infect. Dis. 2015, 21, 1041–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izumikawa, K.; Tashiro, M.; Kohno, S. Management of chronic pulmonary aspergillosis. Ann. N. Y. Acad. Sci. 2012, 1272, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, S.S.; Souza, A.C.; Chowdhary, A.; Meis, J.F.; Colombo, A.L. Epidemiology and molecular mechanisms of antifungal resistance in Candida and Aspergillus. Mycoses 2016, 59, 198–219. [Google Scholar] [CrossRef] [PubMed]
- Espinel-Ingroff, A.; Chowdhary, A.; Gonzalez, G.M.; Lass-Florl, C.; Martin-Mazuelos, E.; Meis, J.; Pelaez, T.; Pfaller, M.A.; Turnidge, J. Multicenter study of isavuconazole MIC distributions and epidemiological cutoff values for Aspergillus spp. for the CLSI M38-A2 broth microdilution method. Antimicrob. Agents Chemother. 2013, 57, 3823–3828. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; van den Boom, M.; Yntema, J.B.; Hagen, F.; Verweij, P.E.; Meis, J.F. Multi-azole-resistant Aspergillus fumigatus in the environment in Tanzania. J. Antimicrob. Chemother. 2014, 69, 2979–2983. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Kathuria, S.; Randhawa, H.S.; Gaur, S.N.; Klaassen, C.H.; Meis, J.F. Isolation of multiple-triazole-resistant Aspergillus fumigatus strains carrying the TR/L98H mutations in the CYP51A gene in India. J. Antimicrob. Chemother. 2012, 67, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Warn, P.A.; Sharp, A.; Denning, D.W. In vitro activity of a new triazole BAL4815, the active component of BAL8557 (the water-soluble prodrug), against Aspergillus spp. J. Antimicrob. Chemother. 2006, 57, 135–138. [Google Scholar] [CrossRef] [PubMed]
- White, P.L.; Posso, R.B.; Barnes, R.A. Analytical and clinical evaluation of the pathonostics aspergenius assay for detection of invasive aspergillosis and resistance to azole antifungal drugs during testing of serum samples. J. Clin. Microbiol. 2015, 53, 2115–2121. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, J.W.; Snelders, E.; Arends, J.P.; Daenen, S.M.; Melchers, W.J.; Verweij, P.E. Rapid diagnosis of azole-resistant aspergillosis by direct PCR using tissue specimens. J. Clin. Microbiol. 2010, 48, 1478–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, G.L.; van de Sande, W.W.; Dingemans, G.J.; Gaajetaan, G.R.; Vonk, A.G.; Hayette, M.P.; van Tegelen, D.W.; Simons, G.F.; Rijnders, B.J. Validation of a new Aspergillus real-time PCR assay for direct detection of Aspergillus and azole resistance of Aspergillus fumigatus on bronchoalveolar lavage fluid. J. Clin. Microbiol. 2015, 53, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Faini, D.; Maokola, W.; Furrer, H.; Hatz, C.; Battegay, M.; Tanner, M.; Denning, D.W.; Letang, E. Burden of serious fungal infections in Tanzania. Mycoses 2015, 58, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Badiane, A.S.; Ndiaye, D.; Denning, D.W. Burden of fungal infections in Senegal. Mycoses 2015, 58, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Gugnani, H.C.; Denning, D.W. Burden of serious fungal infections in the Dominican Republic. J. Infect. Public Health 2015, 9, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Denning, D.W.; Chakrabarti, A. Estimation of the burden of chronic and allergic pulmonary aspergillosis in India. PLoS ONE 2014, 9, e114745. [Google Scholar] [CrossRef] [PubMed]
- Khwakhali, U.S.; Denning, D.W. Burden of serious fungal infections in Nepal. Mycoses 2015, 58, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Pleuvry, A.; Cole, D.C. Global burden of allergic bronchopulmonary aspergillosis with asthma and its complication chronic pulmonary aspergillosis in adults. Med. Mycol. 2013, 51, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Koyama, K.; Ohshima, N.; Suzuki, J.; Kawashima, M.; Takeda, K.; Ando, T.; Sato, R.; Nagai, H.; Matsui, H.; Ohta, K. Recurrence of chronic pulmonary aspergillosis after discontinuation of maintenance treatment by antifungal triazoles. J. Infect. Chemother. 2014, 20, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, K.; Takayanagi, N.; Kanauchi, T.; Ishiguro, T.; Yanagisawa, T.; Sugita, Y. Prognostic factors in 194 patients with chronic necrotizing pulmonary aspergillosis. Intern. Med. 2013, 52, 727–734. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conditions Predisposing to SAIA |
|---|
| Diabetes mellitus |
| Malnutrition |
| Alcohol excess |
| Advancing age |
| Prolonged use of oral corticosteroids |
| Administration of immunosuppressive therapy e.g., In the treatment of connective tissue disease, post solid organ transplantation. |
| COPD |
| Radiotherapy |
| Nontuberculous mycobacterial infection |
| HIV infection |
| Immunology/Serology | Sputum Microbiology | Radiology |
|---|---|---|
| Aspergillus IgG/precipitins | Microscopy | CXR |
| Immunoglobulins and electrophoresis | Culture (including fungal culture) | |
| Functional antibody testing (Tetanus, Haemophilus, Pneumococcus) | Sensitivity (including resistance testing of any isolated Aspergillus spp.) | |
| Mannose binding lectin levels | Sputum Aspergillus PCR | CT thorax |
| Differential Diagnosis | |
|---|---|
| Malignancy | Lung cancer, pulmonary metastases |
| Vasculitis | Particularly granulomatosis with polyangiitis |
| Pulmonary infarction | For example following large pulmonary embolism |
| Post radiotherapy change | Extensive radiotherapy field often produce fibrotic change that can mimic CFPA |
| Mycobacterial infection * | M. tuberculosis, Nontuberculous mycobacteria |
| Fungal infection | Chronic cavitary pulmonary histoplasmosis, paracoccidioidomycosis and coccidioidomycosis |
| Bacterial infection * | Necrotizing pneumonia |
| Differential Diagnosis of a Positive Aspergillus IgG |
|---|
| Asymptomatic individual |
| Aspergillus bronchitis |
| Acute invasive aspergillosis |
| Subacute invasive aspergillosis |
| Chronic pulmonary aspergillosis |
| Allergic Bronchopulmonary aspergillosis/fungal sensitization |
| Recent primary community acquired pulmonary aspergillosis |
© 2016 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayes, G.E.; Novak-Frazer, L. Chronic Pulmonary Aspergillosis—Where Are We? and Where Are We Going? J. Fungi 2016, 2, 18. https://doi.org/10.3390/jof2020018
Hayes GE, Novak-Frazer L. Chronic Pulmonary Aspergillosis—Where Are We? and Where Are We Going? Journal of Fungi. 2016; 2(2):18. https://doi.org/10.3390/jof2020018
Chicago/Turabian StyleHayes, Gemma E., and Lilyann Novak-Frazer. 2016. "Chronic Pulmonary Aspergillosis—Where Are We? and Where Are We Going?" Journal of Fungi 2, no. 2: 18. https://doi.org/10.3390/jof2020018
APA StyleHayes, G. E., & Novak-Frazer, L. (2016). Chronic Pulmonary Aspergillosis—Where Are We? and Where Are We Going? Journal of Fungi, 2(2), 18. https://doi.org/10.3390/jof2020018