
Comparative Efficacies of Antimicrobial Catheter Lock Solutions for Fungal Biofilm Eradication in an in Vitro Model of Catheter-Related Fungemia

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Lock Solutions
2.2. Fungal Strains
2.3. Assessment of Time to Biofilm Eradication
2.4. Statistical Analyses
3. Results
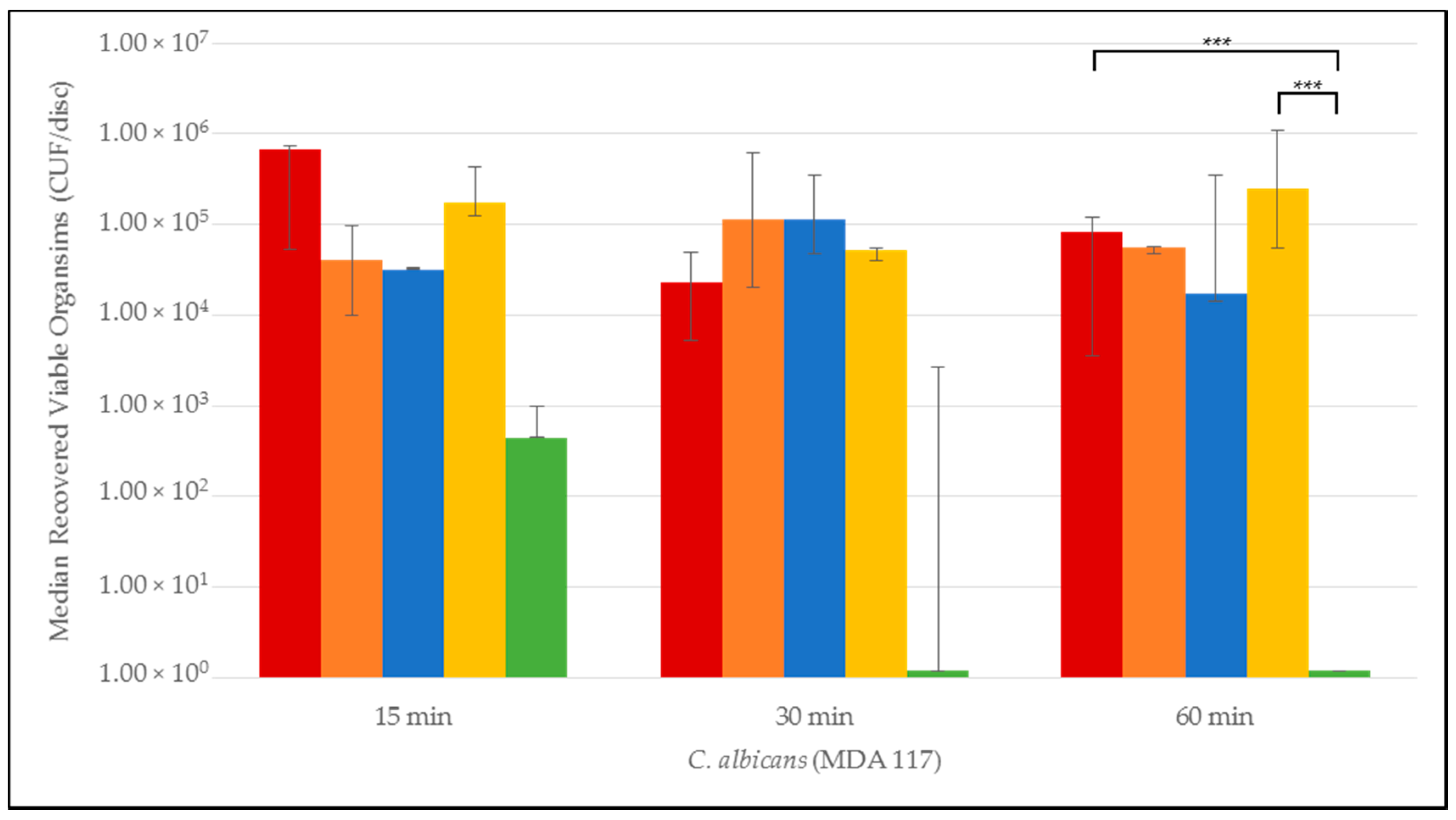
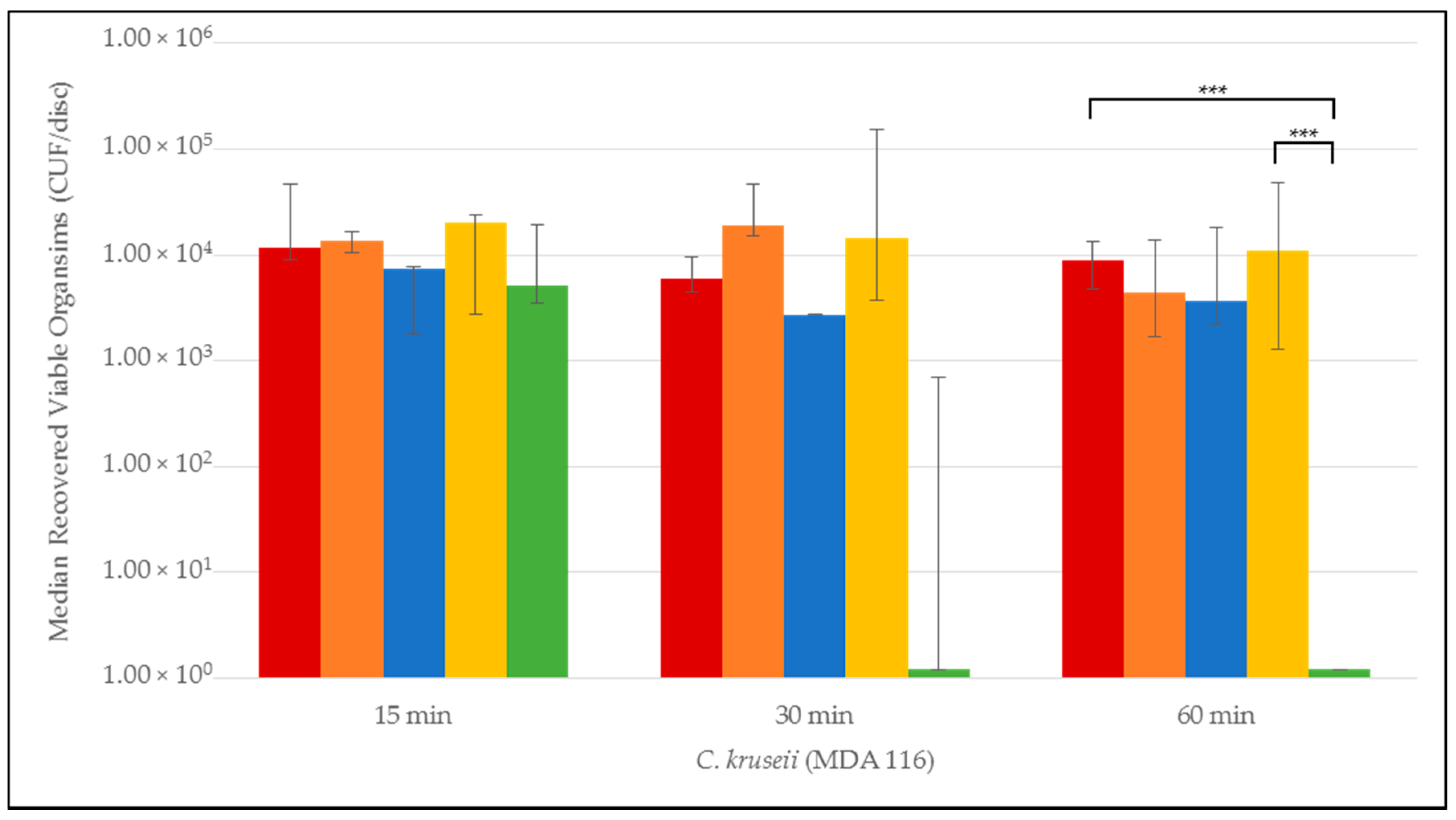
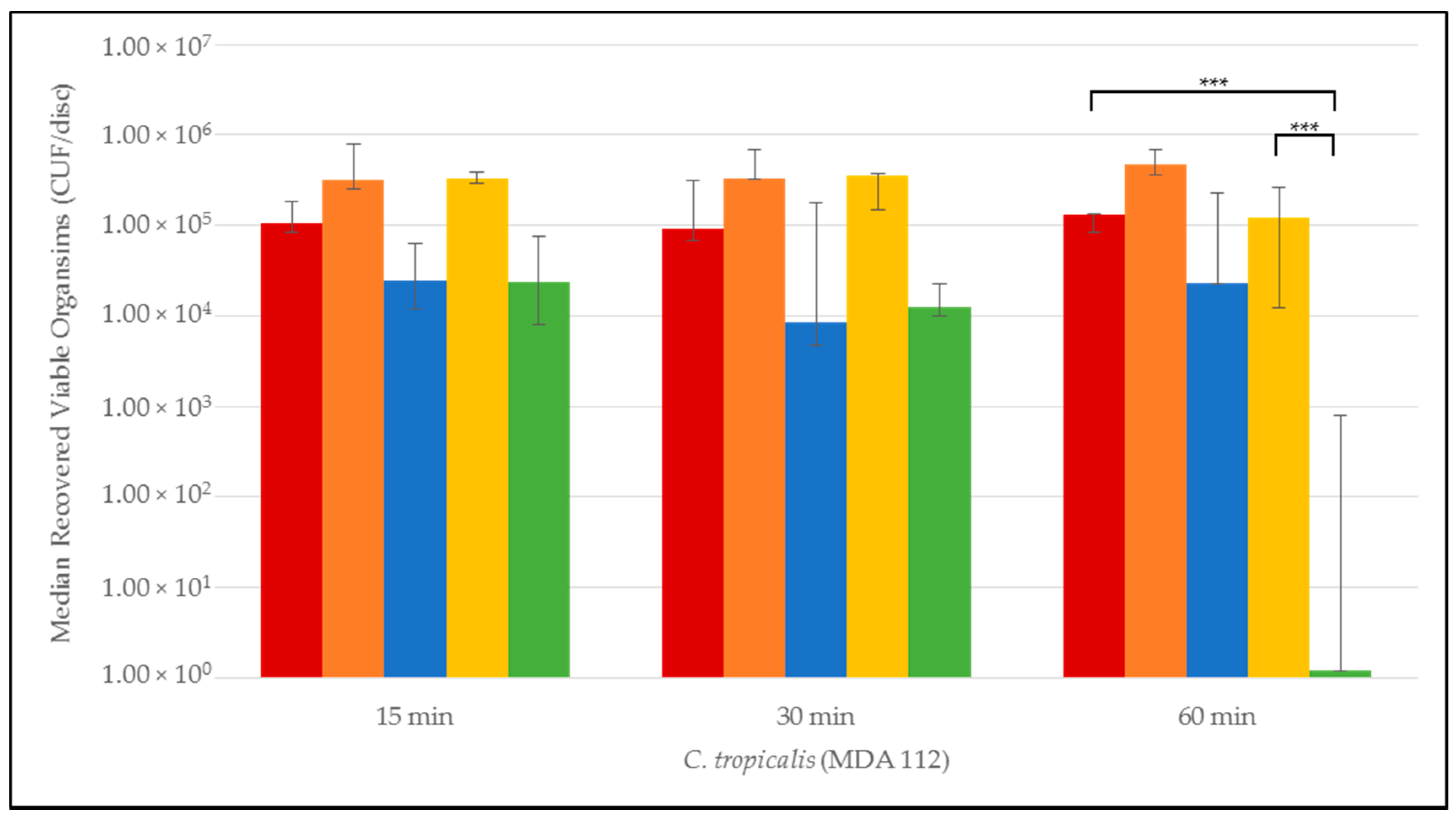
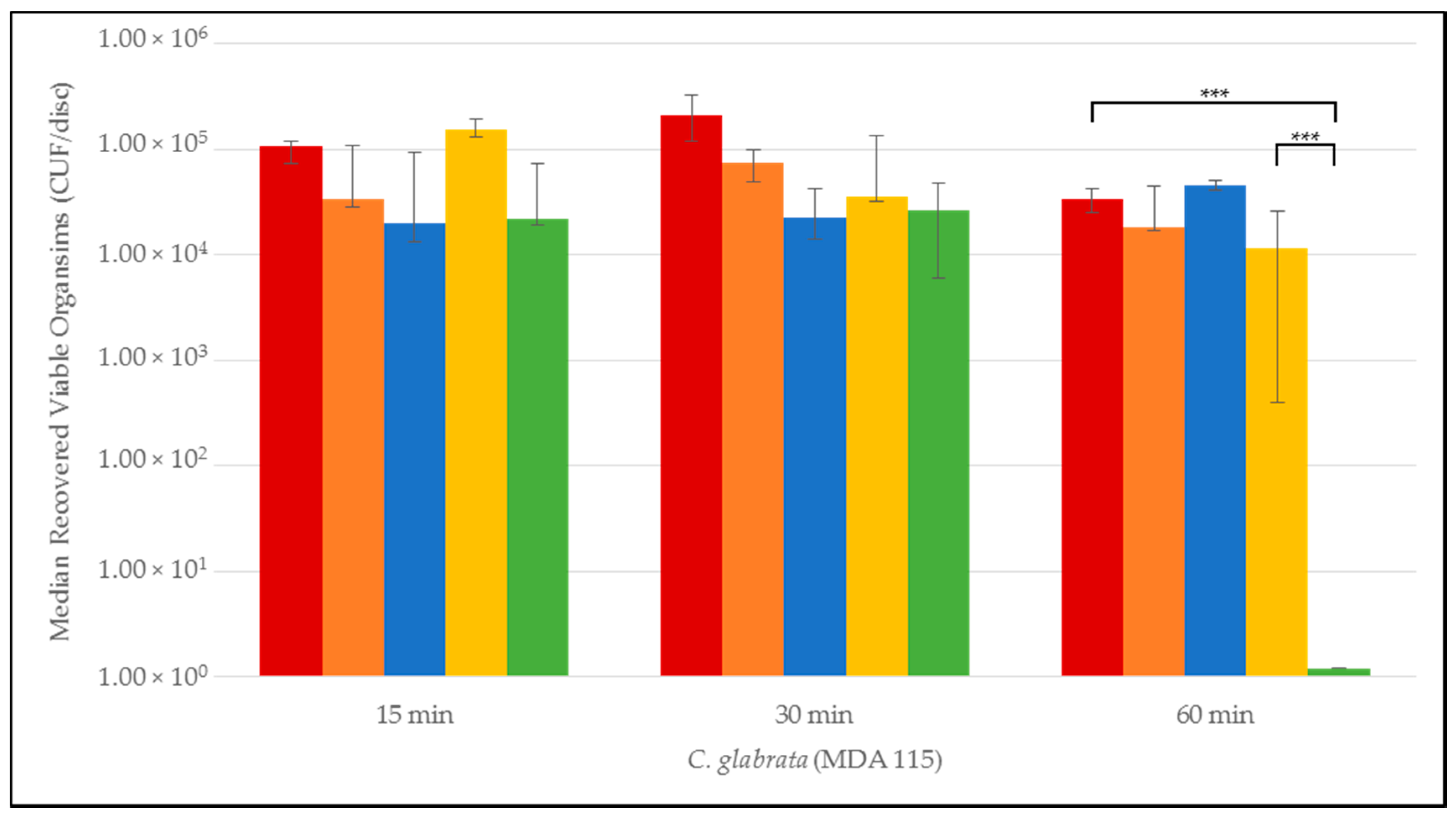
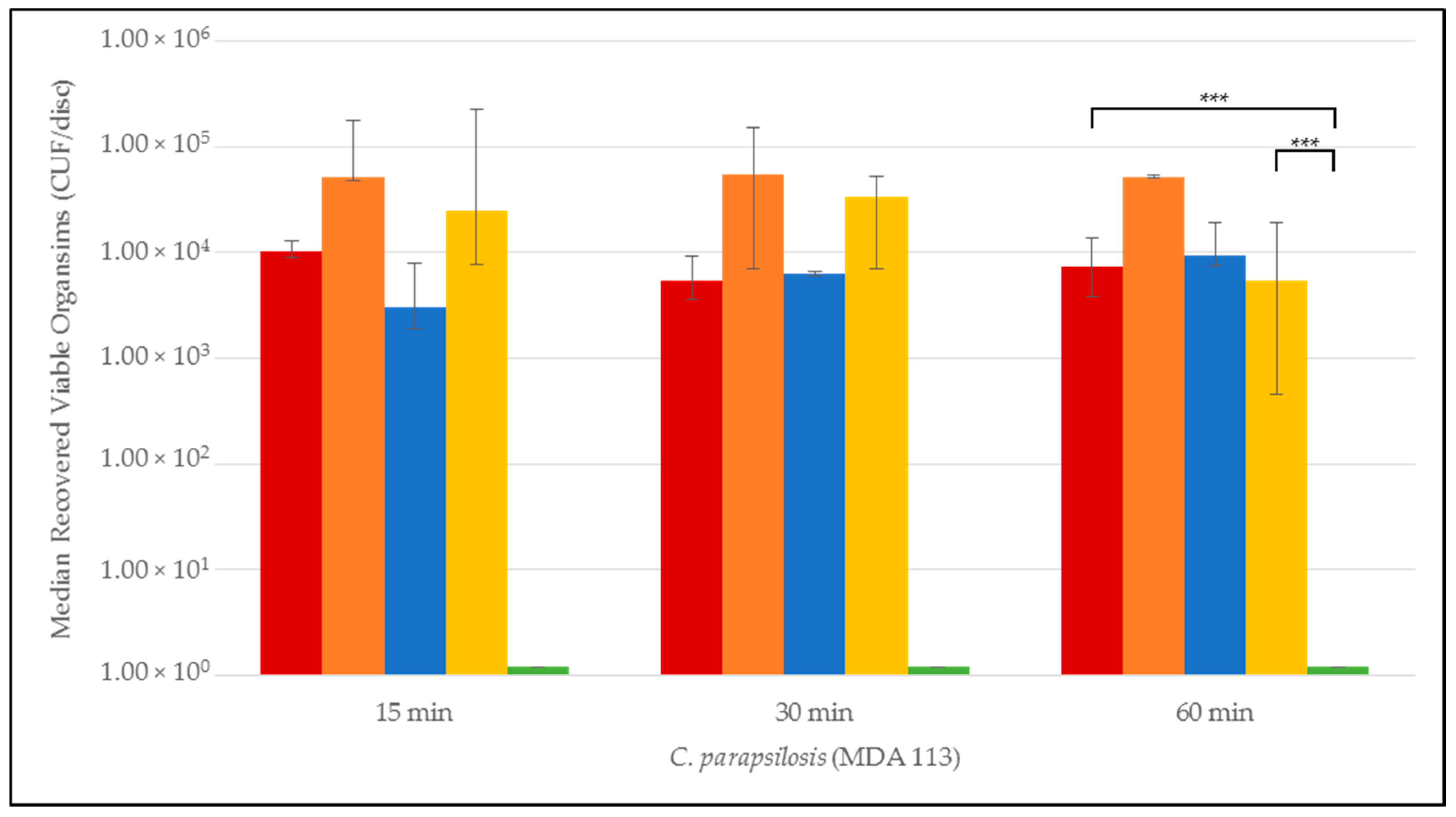
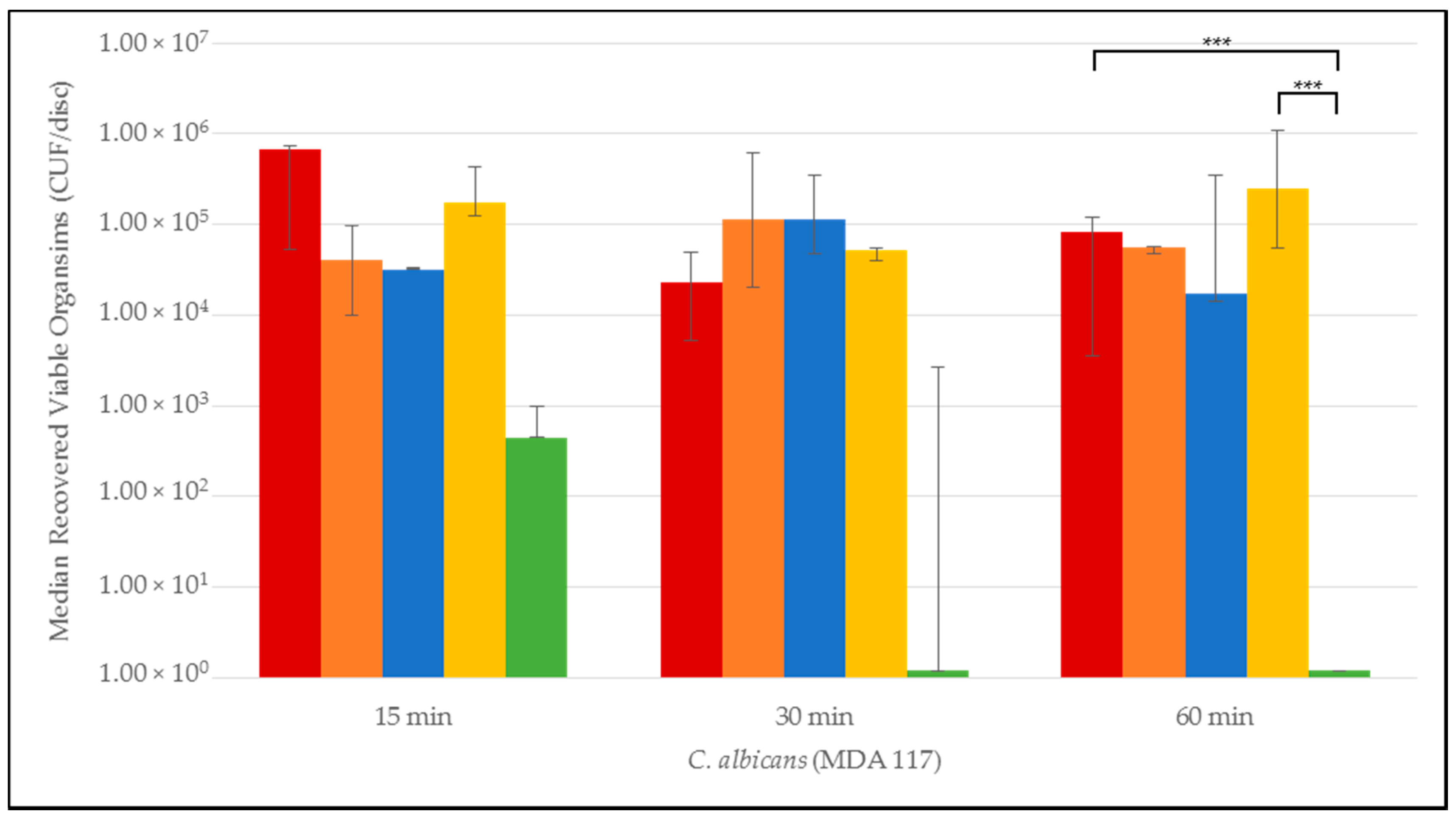
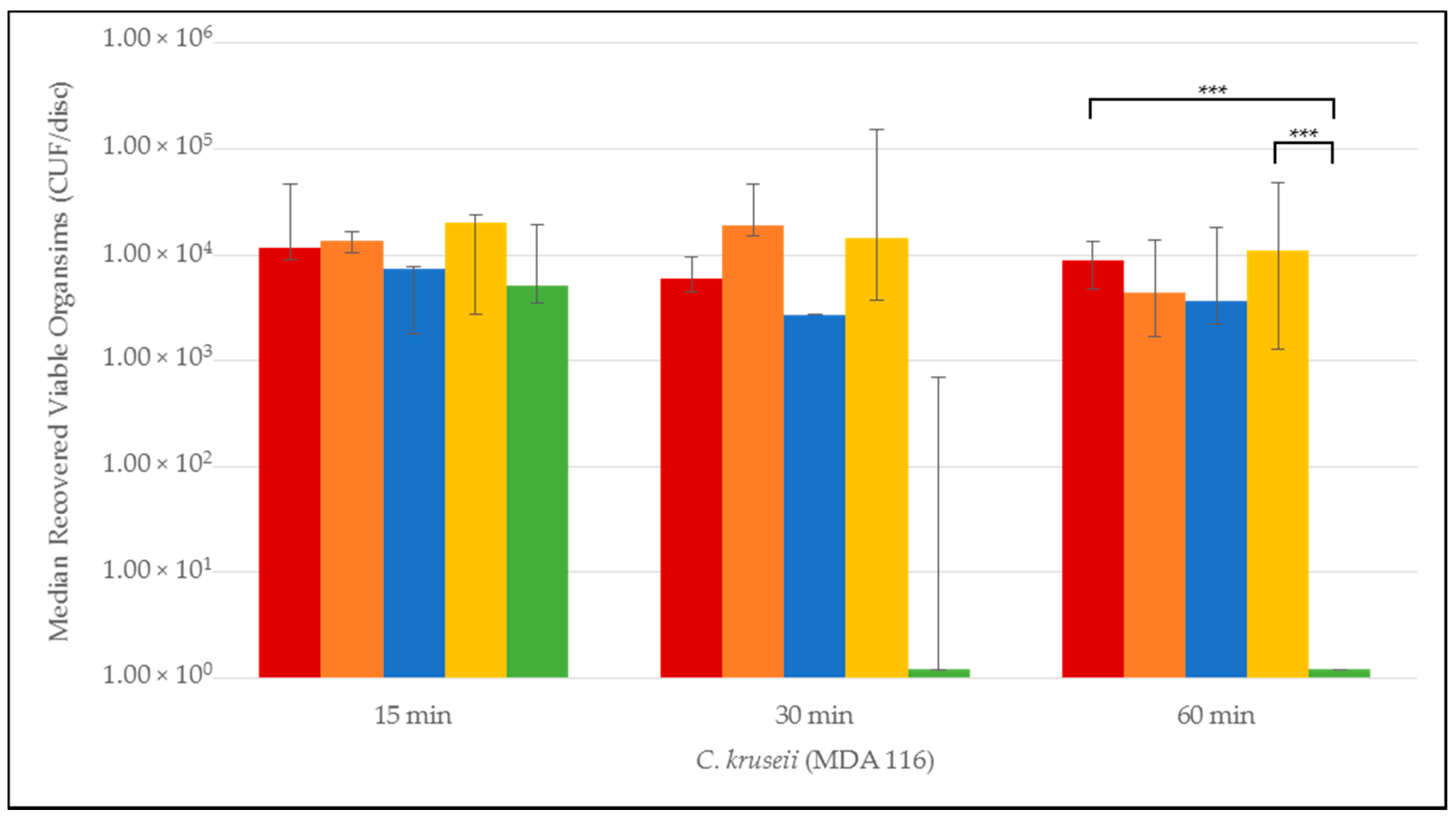
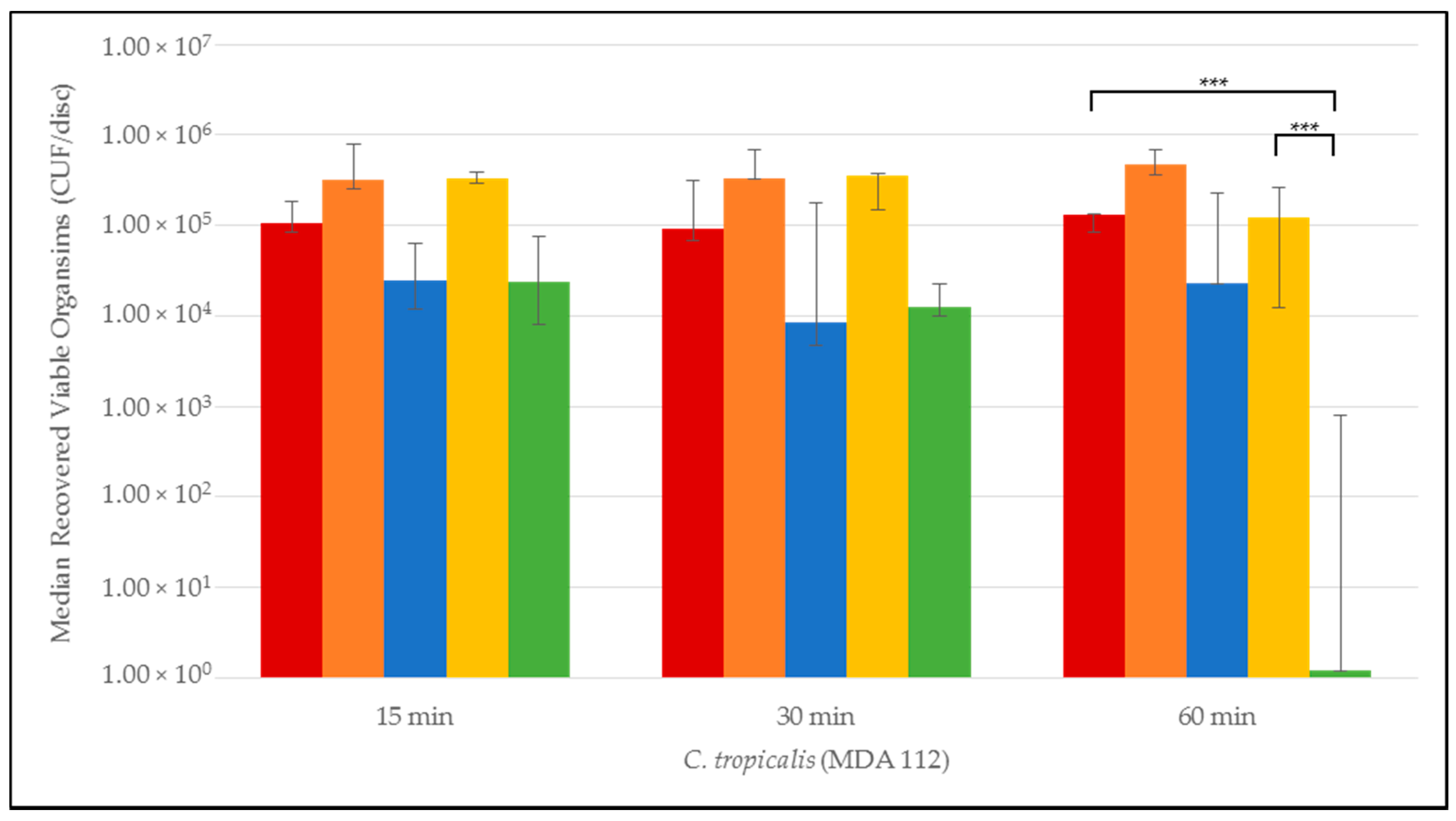
3.1. Time to Biofilm Eradication
3.2. Statistical Comparison of Antimicrobial Activity of NiCE and Taurolidine + Citrate + Heparin Lock Solutions
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Klevens, R.M.; Edwards, J.R.; Richards, C.L., Jr.; Horan, T.C.; Gaynes, R.P.; Pollock, D.A.; Cardo, D.M. Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007, 122, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Warren, D.K.; Quadir, W.W.; Hollenbeak, C.S.; Elward, A.M.; Cox, M.J.; Fraser, V.J. Attributable cost of catheter-associated bloodstream infections among intensive care patients in a nonteaching hospital. Crit. Care Med. 2006, 34, 2084–2089. [Google Scholar] [CrossRef] [PubMed]
- Pronovost, P.; Needham, D.; Berenholtz, S.; Sinopoli, D.; Chu, H.; Cosgrove, S.; Sexton, B.; Hyzy, R.; Welsh, R.; Roth, G.; et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N. Engl. J. Med. 2006, 355, 2725–2732. [Google Scholar] [CrossRef] [PubMed]
- Lipitz-Snyderman, A.; Needham, D.M.; Colantuoni, E.; Goeschel, C.A.; Marsteller, J.A.; Thompson, D.A.; Berenholtz, S.M.; Lubomski, L.H.; Watson, S.; Pronovost, P.J. The ability of intensive care units to maintain zero central line-associated bloodstream infections. Arch. Intern. Med. 2011, 171, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Raad, I.; Chaftari, A.M. Advances in prevention and management of central line-associated bloodstream infections in patients with cancer. Clin. Infect. Dis. 2014, 59, S340–S343. [Google Scholar] [CrossRef] [PubMed]
- Mermel, L.A.; Allon, M.; Bouza, E.; Craven, D.E.; Flynn, P.; O’Grady, N.P.; Raad, I.I.; Rijnders, B.J.A.; Sherertz, R.J.; Warren, D.K. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 49, 1–45. [Google Scholar] [CrossRef] [PubMed]
- NNIS System. National Nosocomial Infections Surveillance (NNIS) System Report. Data summary from January 1990–May 1999, issued June 1999. A report from the NNIS system. Am. J. Infect. Control 1999, 27, 520–532. [Google Scholar]
- Hidron, A.I.; Edwards, J.R.; Patel, J.; Horan, T.C.; Sievert, D.M.; Pollock, D.A.; Fridkin, S.K. NHSN annual update: Antimicrobial-resistant pathogens associated with healthcare-associated infections: Annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect. Control Hosp. Epidemiol. 2008, 29, 996–1011. [Google Scholar] [CrossRef] [PubMed]
- Sievert, D.M.; Ricks, P.; Edwards, J.R.; Schneider, A.; Patel, J.; Srinivasan, A.; Kallen, A.; Limbago, B.; Fridkin, S. Antimicrobial-resistant pathogens associated with healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect. Control Hosp. Epidemiol. 2013, 34, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Moet, G.J.; Messer, S.A.; Jones, R.N.; Castanheira, M. Candida bloodstream infections: Comparison of species distributions and antifungal resistance patterns in community-onset and nosocomial isolates in the SENTRY Antimicrobial Surveillance Program, 2008–2009. Antimicrob. Agents Chemother. 2011, 55, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.; Negri, M.; Henriques, M.; Oliveira, R.; Williams, D.W.; Azeredo, J. Candida glabrata, Candida parapsilosis and Candida tropicalis: Biology, epidemiology, pathogenicity and antifungal resistance. FEMS Microbiol. Rev. 2012, 36, 288–305. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Diekema, D.J. Epidemiology of invasive candidiasis: A persistent public health problem. Clin. Microbiol. Rev. 2007, 20, 133–163. [Google Scholar] [CrossRef] [PubMed]
- Khatib, R.; Johnson, L.B.; Fakih, M.G.; Riederer, K.; Briski, L. Current trends in candidemia and species distribution among adults: Candida glabrata surpasses C. albicans in diabetic patients and abdominal sources. Mycoses 2016. [Google Scholar] [CrossRef] [PubMed]
- Palkar, V.; Patel, V.; Jacob, C.; Paul, S.; Andrade, J. The impact of disinfectant cap implementation on central line-associated bloodstream infections. Infect. Dis. 2016, 48, 646–648. [Google Scholar] [CrossRef] [PubMed]
- Viola, G.M.; Rosenblatt, J.; Raad, I.I. Drug eluting antimicrobial vascular catheters: Progress and promise. Adv. Drug Deliv. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Rozen-Zvi, B.; Gafter-Gvili, A.; Leibovici, L.; Gafter, U.; Paul, M. Antimicrobial lock solutions for the prevention of infections associated with intravascular catheters in patients undergoing hemodialysis: Systematic review and meta-analysis of randomized, controlled trials. Clin. Infect. Dis. 2008, 47, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Bertoglio, S.; Solari, N.; Meszaros, P.; Vassallo, F.; Bonvento, M.; Pastorino, S.; Bruzzi, P. Efficacy of normal saline versus heparinized saline solution for locking catheters of totally implantable long-term central vascular access devices in adult cancer patients. Cancer Nurs. 2012, 35, E35–E42. [Google Scholar] [CrossRef] [PubMed]
- Shanks, R.M.; Donegan, N.P.; Graber, M.L.; Buckingham, S.E.; Zegans, M.E.; Cheung, A.L.; O’Toole, G.A. Heparin stimulates Staphylococcus aureus biofilm formation. Infect. Immun. 2005, 73, 4596–4606. [Google Scholar] [CrossRef] [PubMed]
- Sherertz, R.J.; Boger, M.S.; Collins, C.A.; Mason, L.; Raad, I.I. Comparative in vitro efficacies of various catheter lock solutions. Antimicrob. Agents Chemother. 2006, 50, 1865–1868. [Google Scholar] [CrossRef] [PubMed]
- Hogan, S.; Zapotoczna, M.; Stevens, N.T.; Humphreys, H.; O’Gara, J.P.; O’Neill, E. In vitro approach for identification of the most effective agents for antimicrobial lock therapy in the treatment of intravascular catheter-related infections caused by Staphylococcus aureus. Antimicrob. Agents Chemother. 2016, 60, 2923–2931. [Google Scholar] [CrossRef] [PubMed]
- Walraven, C.J.; Lee, S.A. Antifungal lock therapy. Antimicrob. Agents Chemother. 2013, 57, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Reitzel, R.A.; Rosenblatt, J.; Hirsh-Ginsberg, C.; Murray, K.; Chaftari, A.M.; Hachem, R.; Raad, I. Optimized Nitroglycerin-Citrate-Ethanol (NiCE), non-antibiotic, antimicrobial, catheter lock solution for prevention of central line associated blood stream infections (CLABSI)—An in vitro assessment of antimicrobial efficacy. Antimicrob. Agents Chemother. 2016, 60, 5175–5181. [Google Scholar] [CrossRef] [PubMed]
- Weijmer, M.C.; van den Dorpel, M.A.; Van de Ven, P.J.; ter Wee, P.M.; van Geelen, J.A.; Groeneveld, J.O.; van Jaarsveld, B.C.; Koopmans, M.G.; le Poole, C.Y.; Schrander-Van der Meer, A.M.; et al. Randomized, clinical trial comparison of trisodium citrate 30% and heparin as catheter-locking solution in hemodialysis patients. J. Am. Soc. Nephrol. 2005, 16, 2769–2777. [Google Scholar] [CrossRef] [PubMed]
- Betjes, M.G.; van Agteren, M. Prevention of dialysis catheter-related sepsis with a citrate-taurolidine-containing lock solution. Nephrol. Dial. Transplant. 2004, 19, 1546–1551. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, D.M.; George, T.; Chandra, J.; Mukherjee, P.K.; Ghannoum, M.A. Antifungal susceptibility of Candida biofilms: Unique efficacy of amphotericin B lipid formulations and echinocandins. Antimicrob. Agents Chemother. 2002, 46, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Chaftari, A.M.; Hachem, R.; Szvalb, A.; Taremi, M.; Granwehr, B.; Viola, G.M.; Sapna, A.; Assaf, A.; Numan, Y.; Shah, P.; et al. A Novel Non-Antibiotic Nitroglycerin Based Catheter Lock Solution for the Prevention of Intraluminal Central Venous Catheter Related Bloodstream Infections (CRBSI) in Cancer Patients; Infectious Diseaes Society of America—IDWeek: New Orleans, LA, USA, 2016. [Google Scholar]
- Raad, I.I.; Fang, X.; Keutgen, X.M.; Jiang, Y.; Sherertz, R.; Hachem, R. The role of chelators in preventing biofilm formation and catheter-related bloodstream infections. Curr. Opin. Infect. Dis. 2008, 21, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Green, J.V.; Orsborn, K.I.; Zhang, M.; Tan, Q.K.; Greis, K.D.; Porollo, A.; Andes, D.R.; Long Lu, J.; Hostetter, M.K. Heparin-binding motifs and biofilm formation by Candida albicans. J. Infect. Dis. 2013, 208, 1695–1704. [Google Scholar] [CrossRef] [PubMed]
- Neary, P.M.; Hallihan, P.; Wang, J.H.; Pfirrmann, R.W.; Bouchier-Hayes, D.J.; Redmond, H.P. The evolving role of taurolidine in cancer therapy. Ann. Surg. Oncol. 2010, 17, 1135–1143. [Google Scholar] [CrossRef] [PubMed]
- Jurewitsch, B.; Lee, T.; Park, J.; Jeejeebhoy, K. Taurolidine 2% as an antimicrobial lock solution for prevention of recurrent catheter-related bloodstream infections. JPEN J. Parenter. Enter. Nutr. 1998, 22, 242–244. [Google Scholar] [CrossRef]
- Shah, C.B.; Mittelman, M.W.; Costerton, J.W.; Parenteau, S.; Pelak, M.; Arsenault, R.; Mermel, L.A. Antimicrobial activity of a novel catheter lock solution. Antimicrob. Agents Chemother. 2002, 46, 1674–1679. [Google Scholar] [CrossRef] [PubMed]
- Chandra, J.; Mukherjee, P.K. Candida biofilms: Development, architecture, and resistance. Microbiol. Spectr. 2015, 3. [Google Scholar] [CrossRef] [PubMed]
- Caruso, F.; Darnowski, J.W.; Opazo, C.; Goldberg, A.; Kishore, N.; Agoston, E.S.; Rossi, M. Taurolidine antiadhesive properties on interaction with E. coli; its transformation in biological environment and interaction with bacteria cell wall. PLoS ONE 2010, 5, e8927. [Google Scholar] [CrossRef] [PubMed]
- Gorman, S.P.; McCafferty, D.F.; Woolfson, A.D.; Jones, D.S. Reduced adherence of micro-organisms to human mucosal epithelial cells following treatment with Taurolin, a novel antimicrobial agent. J. Appl. Bacteriol. 1987, 62, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Handrup, M.M.; Fuursted, K.; Funch, P.; Moller, J.K.; Schroder, H. Biofilm formation in long-term central venous catheters in children with cancer: A randomized controlled open-labelled trial of taurolidine versus heparin. APMIS Acta Pathol. Microbiol. Immunol. Scand. 2012, 120, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, J.; Reitzel, R.; Dvorak, T.; Jiang, Y.; Hachem, R.Y.; Raad, I.I. Glyceryl trinitrate complements citrate and ethanol in a novel antimicrobial catheter lock solution to eradicate biofilm organisms. Antimicrob. Agents Chemother. 2013, 57, 3555–3560. [Google Scholar] [CrossRef] [PubMed]
- Palmeira-de-Oliveira, A.; Ramos, A.R.; Gaspar, C.; Palmeira-de-Oliveira, R.; Gouveia, P.; Martinez-de-Oliveira, J. In vitro anti-Candida activity of lidocaine and nitroglycerin: Alone and combined. Infect. Dis. Obstet. Gynecol. 2012, 2012, 727248. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, P.K.; Mohamed, S.; Chandra, J.; Kuhn, D.; Liu, S.; Antar, O.S.; Munyon, R.; Mitchell, A.P.; Andes, D.; Chance, M.R.; et al. Alcohol dehydrogenase restricts the ability of the pathogen Candida albicans to form a biofilm on catheter surfaces through an ethanol-based mechanism. Infect. Immun. 2006, 74, 3804–3816. [Google Scholar] [CrossRef] [PubMed]
- Schilcher, G.; Schlagenhauf, A.; Schneditz, D.; Scharnagl, H.; Ribitsch, W.; Krause, R.; Rosenkranz, A.R.; Stojakovic, T.; Horina, J.H. Ethanol causes protein precipitation—New safety issues for catheter locking techniques. PLoS ONE 2013, 8, e84869. [Google Scholar] [CrossRef] [PubMed]
- Mermel, L.A.; Alang, N. Adverse effects associated with ethanol catheter lock solutions: A systematic review. J. Antimicrob. Chemother. 2014, 69, 2611–2619. [Google Scholar] [CrossRef] [PubMed]
- Gage, J.E.; Hess, O.M.; Murakami, T.; Ritter, M.; Grimm, J.; Krayenbuehl, H.P. Vasoconstriction of stenotic coronary arteries during dynamic exercise in patients with classic angina pectoris: Reversibility by nitroglycerin. Circulation 1986, 73, 865–876. [Google Scholar] [CrossRef] [PubMed]
- Rijnders, B.J.; van Wijngaerden, E.; Peetermans, W.E. Catheter-tip colonization as a surrogate end point in clinical studies on catheter-related bloodstream infection: How strong is the evidence? Clin. Infect. Dis. 2002, 35, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.; Henriques, M.; Martins, A.; Oliveira, R.; Williams, D.; Azeredo, J. Biofilms of non-Candida albicans Candida species: Quantification, structure and matrix composition. Med. Mycol. 2009, 47, 681–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]

© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosenblatt, J.; Reitzel, R.A.; Vargas-Cruz, N.; Chaftari, A.-M.; Hachem, R.; Raad, I.I. Comparative Efficacies of Antimicrobial Catheter Lock Solutions for Fungal Biofilm Eradication in an in Vitro Model of Catheter-Related Fungemia. J. Fungi 2017, 3, 7. https://doi.org/10.3390/jof3010007
Rosenblatt J, Reitzel RA, Vargas-Cruz N, Chaftari A-M, Hachem R, Raad II. Comparative Efficacies of Antimicrobial Catheter Lock Solutions for Fungal Biofilm Eradication in an in Vitro Model of Catheter-Related Fungemia. Journal of Fungi. 2017; 3(1):7. https://doi.org/10.3390/jof3010007
Chicago/Turabian StyleRosenblatt, Joel, Ruth A. Reitzel, Nylev Vargas-Cruz, Anne-Marie Chaftari, Ray Hachem, and Issam I. Raad. 2017. "Comparative Efficacies of Antimicrobial Catheter Lock Solutions for Fungal Biofilm Eradication in an in Vitro Model of Catheter-Related Fungemia" Journal of Fungi 3, no. 1: 7. https://doi.org/10.3390/jof3010007