
Fungal Density in Lobomycosis in French Guiana: A Proposal for a New Clinico-Histological and Therapeutic Classification
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion
2.2. Data Collected
- socio-demographic characteristics (age, gender, ethnicity, country of origin, occupation, possible exposure factors, date of arrival in French Guiana)
- clinical characteristics (date of lesions onset, skin trauma, duration of disease, size, number and body location of the lesions, lymphadenopathy)
- treatment history (abstention, local or systemic treatment, duration of treatment, drugs/treatments used)
- outcome. The different responses to treatment were defined according to the method in Gonçalves [20], as follows: partial response (50% decrease or atrophy of lesions at the last follow-up visit), complete response (total regression of lesions at the last follow-up visit without relapse for 2 years after the end of treatment). Treatment failure included cases with no response (<50% decrease or increase in number or size of lesions) and cases with relapse (resurgence of lesions after initial remission); data were collected on the type and number of relapses, as well as the presence of a local (on the site of the previous lesion) or distant relapse.
2.3. Histopathology
2.4. Ethics
2.5. Statistical Analysis
3. Results
3.1. Patient’s Characteristics
3.2. Clinical Features at Diagnosis
3.3. Evolution
3.4. Histological Analysis
4. Discussion
4.1. Epidemiologic Data
4.2. Clinical Data
4.3. Pathological Data
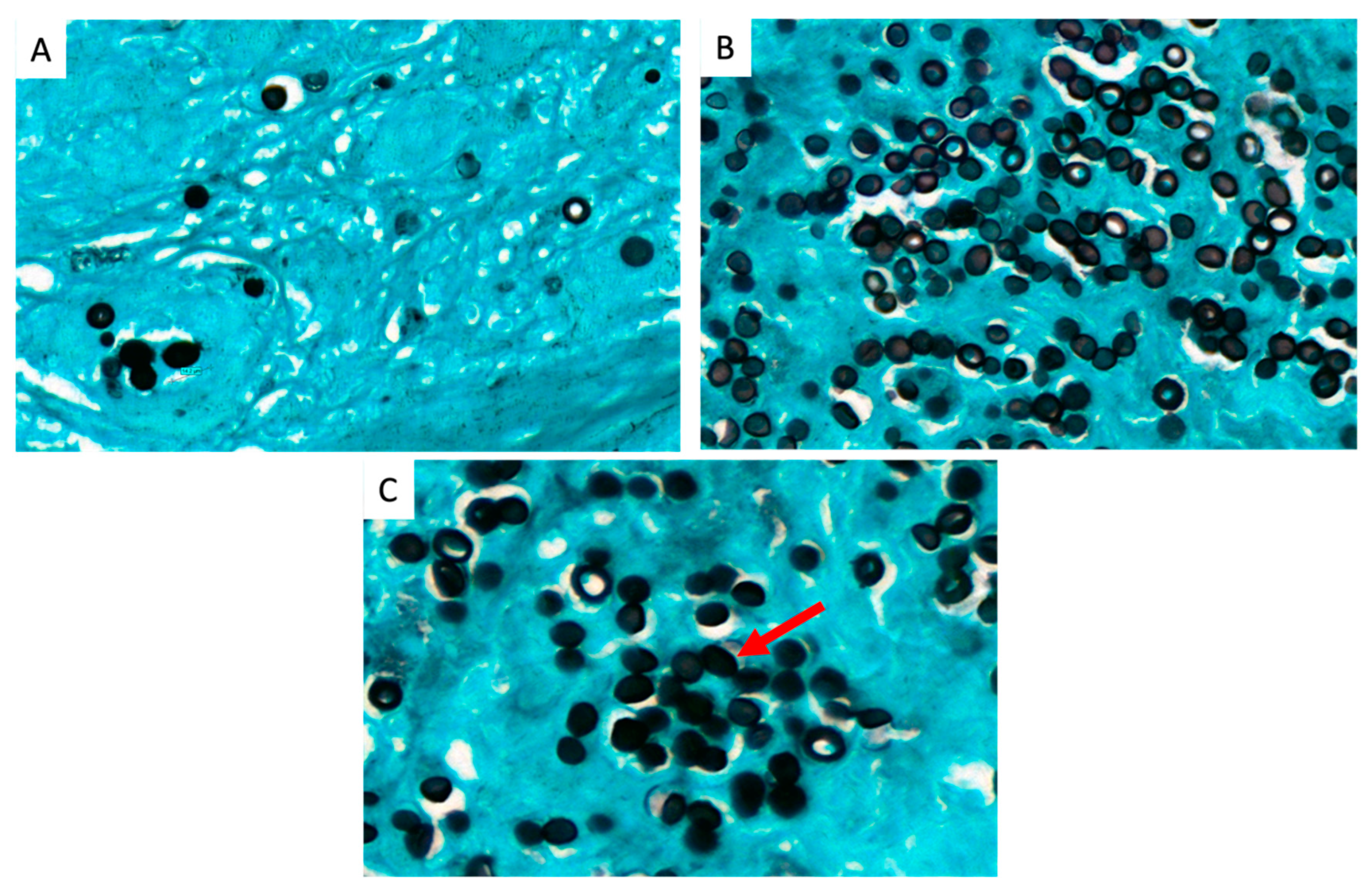
- Patients with low fungal density (<400 yeasts/field) had single or multiple localized involvements. They all showed a partial or complete therapeutic response, and none progressed to a major form.
- Patients with high fungal density (>800 yeasts/field) presented a multifocal form and did not respond to first-line treatment.
- Concerning patients with medium fungal density (400–800 yeasts/field), they had unifocal or multifocal forms, and those who received treatment had a partial response. Some of them were still under treatment at the time of the study, and adjuvant surgery could be performed after debulking with antifungals.
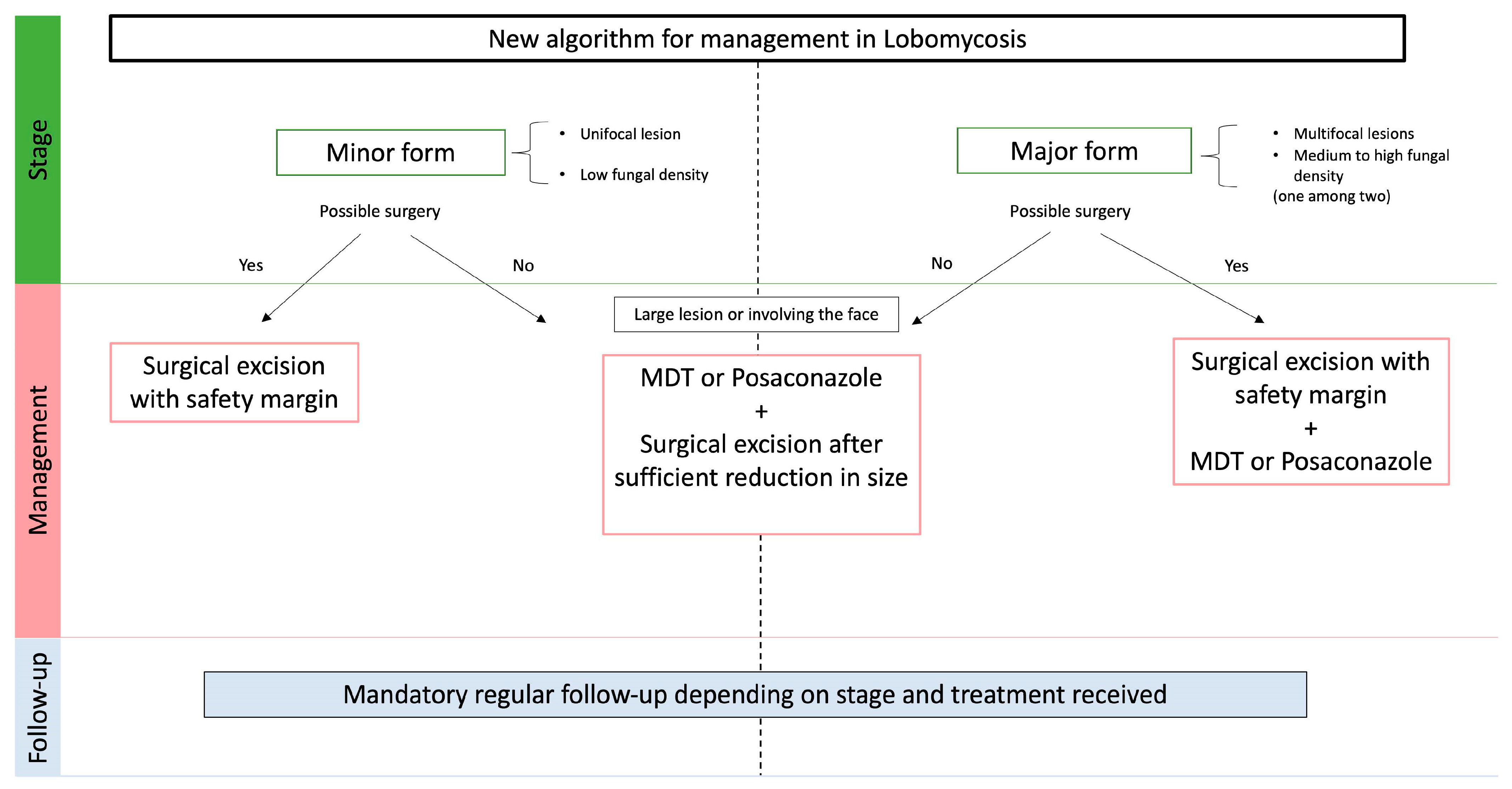
4.4. Therapeutic Strategy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vilela, R.; De Hoog, S.; Bensch, K.; Bagagli, E.; Mendoza, L. A taxonomic review of the genus Paracoccidioides, with focus on the uncultivable species. PLoS Negl. Trop. Dis. 2023, 17, e0011220. [Google Scholar] [CrossRef] [PubMed]
- Talhari, S.; Talhari, C. Lobomycosis. Clin. Dermatol. 2012, 30, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Hornberger, M.M.; Farnsworth, G.S.; Vilela, R.; Mendoza, L.; Bandino, J.P. Extensive, multifocal lobomycosis. J. Cutan. Pathol. 2021, 49, 957–959. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, F.G.; Rosa, P.S.; Belone, A.d.F.F.; Carneiro, L.B.; de Barros, V.L.Q.; Bispo, R.F.; Sbardelott, Y.A.d.S.; Neves, S.A.V.M.; Vittor, A.Y.; Woods, W.J.; et al. Lobomycosis Epidemiology and Management: The Quest for a Cure for the Most Neglected of Neglected Tropical Diseases. J. Fungi 2022, 8, 494. [Google Scholar] [CrossRef] [PubMed]
- Arenas, C.M.; Rodriguez-Toro, G.; Ortiz-Florez, A.; Serrato, I. Lobomycosis in Soldiers, Colombia. Emerg. Infect. Dis. 2019, 25, 654–660. [Google Scholar] [CrossRef]
- Francesconi, F.; Francesconi do Valle, V.; Klein, A.P.; Botelho Gualda Santos, A.P.; Ramasawmy, R. Lobomycosis: Epidemiology, clinical presentation, and management options. Ther. Clin. Risk Manag. 2014, 10, 851. [Google Scholar] [CrossRef]
- De Carvalho, K.A.; Floriano, M.C.; Enokihara, M.M.S.e.S.; Mascarenhas, M.R.M. Jorge Lobo’s disease. An. Bras. Dermatol. 2015, 90, 586–588. [Google Scholar] [CrossRef]
- Queiroz-Telles, F.; Nucci, M.; Colombo, A.L.; Tobón, A.; Restrepo, A. Mycoses of implantation in Latin America: An overview of epidemiology, clinical manifestations, diagnosis and treatment. Med. Mycol. 2011, 49, 225–236. [Google Scholar] [CrossRef]
- Paniz-Mondolfi, A.; Talhari, C.; Sander Hoffmann, L.; Connor, D.L.; Talhari, S.; Bermudez-Villapol, L.; Hernandez-Perez, M.; Van Bressem, M.F. Lobomycosis: An emerging disease in humans and delphinidae: Lobomycosis in humans and delphinidae. Mycoses 2012, 55, 298–309. [Google Scholar] [CrossRef]
- Miranda, M.F.R.; Silva, A.J.G. Vinyl adhesive tape also effective for direct microscopy diagnosis of chromomycosis, lobomycosis, and paracoccidioidomycosis. Diagn. Microbiol. Infect. Dis. 2005, 52, 39–43. [Google Scholar] [CrossRef]
- Talhari, C.; Chrusciak-Talhari, A.; de Souza, J.V.B.; Araújo, J.R.; Talhari, S. Exfoliative cytology as a rapid diagnostic tool for lobomycosis. Mycoses 2009, 52, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Florian, M.C.; Rodrigues, D.A.; de Mendonça, S.B.M.; Colombo, A.L.; Tomimori, J. Epidemiologic and Clinical Progression of Lobomycosis among Kaiabi Indians, Brazil, 1965–2019. Emerg. Infect. Dis. 2020, 26, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, A. Treatment of tropical mycoses. J. Am. Acad. Dermatol. 1994, 31, S91–S102. [Google Scholar] [CrossRef]
- Carneiro, F.P.; Maia, L.B.; Moraes, M.A.P.; de Magalhães, A.V.; Vianna, L.M.d.S.; Zancanaro, P.C.Q.; Reis, C.M. Lobomycosis: Diagnosis and management of relapsed and multifocal lesions. Diagn. Microbiol. Infect. Dis. 2009, 65, 62–64. [Google Scholar] [CrossRef]
- Araújo, M.G.; Cirilo, N.S.; dos Santos, S.N.M.B.; Aguilar, C.R.; Guedes, A.C.M. Lobomycosis: A therapeutic challenge. An. Bras. Dermatol. 2018, 93, 279–281. [Google Scholar] [CrossRef]
- Fischer, M.; Chrusciak Talhari, A.; Reinel, D.; Talhari, S. Sucessful treatment with clofazimine and itraconazole in a 46 year old patient after 32 years duration of disease. Hautarzt 2002, 53, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Bustamante, B.; Seas, C.; Salomon, M.; Bravo, F. Lobomycosis successfully treated with posaconazole. Am. J. Trop. Med. Hyg. 2013, 88, 1207–1208. [Google Scholar] [CrossRef] [PubMed]
- Rosa, P.S. Ten years experience with Jorge Lobo’s disease in the state of Acre, Amazon region, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2010, 52, 273–278. [Google Scholar] [CrossRef]
- Talhari, C.; Oliveira, C.B.; de Souza Santos, M.N.; Ferreira, L.C.; Talhari, S. Disseminated lobomycosis. Int. J. Dermatol. 2008, 47, 582–583. [Google Scholar] [CrossRef]
- Gonçalves, F.G.; Rosa, P.S.; de Farias Fernandes Belone, A.; Carneiro, L.B.; Queiroz de Barros, V.L.; Bispo, R.F.; Alves da Silva Sbardelott, Y.; Viana Macedo Neves, S.A.; Vittor, A.Y.; Woods, W.J.; et al. Multidrug Therapy for Leprosy Can Cure Patients with Lobomycosis in Acre State, Brazil: A Proof of Therapy Study. Am. J. Trop. Med. Hyg. 2021, 104, 634–639. [Google Scholar] [CrossRef]
- Garcia, M.; Chanlin, R.; Blanchet, D.; Demar, M.; Couppie, P.; Blaizot, R. An atypical keloid in a Brazilian man. Med. Sante Trop. 2019, 29, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Linck, V.; Sambourg, E.; Demar, M.; Graille, J.; Blanchet, D.; Darrigade, A.-S.; Dufour, J.; Sainte-Marie, D.; Pradinaud, R.; Labbe, S.; et al. La lobomycose en Guyane française: À propos de 20 observations. Ann. Dermatol. Vénéréologie 2014, 141, S456. [Google Scholar] [CrossRef]
- Mouchard, A.; Chanlin, R.; Blanchet, D.; Pierre-Demar, M.; Drak Alsibai, K.; Couppie, P.; Blaizot, R. Lobomycose en Guyane, revue sur 10 ans d’une mycose exotique. Ann. Dermatol. Vénéréologie 2020, 147, A297–A298. [Google Scholar] [CrossRef]
- Roche, J.C.; Monod, L. 10th case of lobomycosis observed in French Guiana. Bull. Soc. Pathol. Exot. Filiales 1976, 69, 540–546. [Google Scholar] [PubMed]
- Heleine, M.; Blaizot, R.; Cissé, H.; Labaudinière, A.; Guerin, M.; Demar, M.; Blanchet, D.; Couppie, P. A case of disseminated paracoccidioidomycosis associated with cutaneous lobomycosis. J. Eur. Acad. Dermatol. Venereol. JEADV 2020, 34, e18–e20. [Google Scholar] [CrossRef]
- Opromolla, D.; Belone, A.; Taborda, P.; Taborda, V. Clinicopathological correlation in 40 new cases of lobomycosis (in Portuguese). An. Bras. Dermatol. 2000, 75, 425–434. [Google Scholar]
- Baruzzi, R.G.; Lacaz, C.d.S.; de Souza, F.A. Natural history of Jorge Lobo’s disease. Occurrence among the Caiabi Indians (Central Brazil). Rev. Inst. Med. Trop. Sao Paulo 1979, 21, 303–338. [Google Scholar]
- Vilela, R.; Mendoza, L.; Rosa, P.S.; Belone, A.F.F.; Madeira, S.; Opromolla, D.V.A.; de Resende, M.A. Molecular Model for Studying the Uncultivated Fungal Pathogen Lacazia loboi. J. Clin. Microbiol. 2005, 43, 3657–3661. [Google Scholar] [CrossRef]
- Herr, R.A.; Tarcha, E.J.; Taborda, P.R.; Taylor, J.W.; Ajello, L.; Mendoza, L. Phylogenetic Analysis of Lacazia loboi Places This Previously Uncharacterized Pathogen within the Dimorphic Onygenales. J. Clin. Microbiol. 2001, 39, 309–314. [Google Scholar] [CrossRef]
- Azulay, R.D.; Carneiro, J.A.; Da Graça, M.; Cunha, S.; Reis, L.T. Keloidal blastomycosis (Lobo’s disease) with lymphatic involvement: A case report. Int. J. Dermatol. 1976, 15, 40–42. [Google Scholar] [CrossRef]
- Opromolla, D.V.A.; Belone, A.F.F.; Taborda, P.R.; Rosa, P.S. Lymph node involvement in Jorge Lobo’s disease: Report of two cases. Int. J. Dermatol. 2003, 42, 938–941. [Google Scholar] [CrossRef] [PubMed]
- Drak Alsibai, K.; Aissaoui, H.; Adenis, A.; Bourne-Watrin, M.; Djossou, F.; Epelboin, L.; Blanchet, D.; Demar, M.; Couppié, P.; Nacher, M. Cytological Spectrum of Pulmonary Histoplasmosis Diagnosed by Bronchoalveolar Lavage: 12 Years of Experience in French Guiana. J. Fungi 2021, 7, 576. [Google Scholar] [CrossRef] [PubMed]
- Premalatha, P.; Renuka, I.V.; Meghana, A.; Devi, S.I.; Charyulu, P.; Sampoorna, G. Utility of Bacillary Index in Slit Skin Smears in Correlation with Clinical and Histopathological Alterations in Hansen’s Disease: An Attempt to Revive a Simple Useful Procedure. Ann. Med. Health Sci. Res. 2016, 6, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Pasqualotto, A.C.; Jaskulski Filho, S.D.; de Sena, M.G.; Santos, A.F.D.; Severo, M.M.S. Posaconazole for lobomycosis. Braz. J. Infect. Dis. 2021, 25, 101576. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | Group 2 | Total | OR [95% CI] | p-Value | |
|---|---|---|---|---|---|
| Year of Diagnosis | 1959–1992 n = 15 | 2010–2022 n = 16 | Total n = 31 | ||
| Age | |||||
| Mean (min–max) | 61 (45–83) | 49 (33–75) | 54 (33–83) | ||
| Median (Q1–Q3) | 60 (53–65) | 46.5 (40.5–57) | 55 (43–62) | ||
| <60 years | 7 | 15 | 17.14 [1.59–809.71] | 0.0039 * | |
| ≥60 years | 8 | 1 | |||
| Gender (%) | |||||
| Women | 1 (7.0) | 4 (25.0) | 5 (16.1) | 4.67 [0.37–245.87] | 0.1655 |
| Men | 14 (93.0) | 12 (75.0) | 26 (83.9) | ||
| Country of birth (%) | |||||
| Brazil | 1 (6.7) | 13 (81.3) | 14 (45.2) | 0.02 [0.01–0.21] 1 | <0.0001 * |
| French Guiana | 7 (46.7) | 1 (6.3) | 8 (25.8) | ||
| Suriname | 4 (26.7) | 1 (6.3) | 5 (16.1) | ||
| France (mainland) | 0 (0) | 1 (6.3) | 1 ((3.2) | ||
| Guyana | 1 (6.7) | 0 (0) | 1 (3.2) | ||
| India | 1 (6.7) | 0 (0) | 1 (3.2) | ||
| Saint Lucia | 1 (6.7) | 0 (0) | 1 (3.2) | ||
| Ethnicity (%) | |||||
| Brazilian | 0 (0) | 13 (81.3) | 13 (41.9) | 17.14 [1.59–809.71] 2 | 0.0039 * |
| Creole | 8 (53.3) | 1 (6.3) | 9 (29.0) | ||
| Maroon | 5 (33.3) | 1 (6.3) | 6 (19.4) | ||
| Amerindian | 1 (6.7) | 0 (0) | 1 (3.2) | ||
| Caucasian | 0 (0) | 1 (6.3) | 1 (3.2) | ||
| Unknown | 1 (6.7) | 0 (0) | 1 (3.2) | ||
| Occupation (%) | |||||
| Gold digger | 3 (23.1) | 9 (60.0) | 12 (42.9) | 0.19 [0.03–1.19] 3 | 0.0384 * |
| Fisherman/sailor | 4 (30.7) | 2 (13.3) | 6 (21.4) | ||
| Farmer | 2 (15.4) | 2 (13.3) | 4 (14.3) | ||
| Logging/forestry | 3 (23.1) | 0 (0) | 3 (10.7) | ||
| Other | 1 (7.7) | 2 (13.3) | 3 (10.7) | ||
| Duration before diagnosis (years) | |||||
| Mean (min–max) | 12 (0.5–40) | 4.25 (0.23–20) | 7.24 (0.5–40) | ||
| Median (Q1–Q3) | 8.25 (3–10) | 2.33 (1–4) | 3.5 (1.5–9) | 4.67 [0.47–60.97] | 0.1054 |
| ≥10 months | 4 | 2 | |||
| <10 months | 6 | 14 | |||
| History of skin trauma n (%) | |||||
| 3 (20) | 4 (25) | 7 (22.6) | |||
| Number of lesions n (%) | |||||
| Unique | 6 (40) | 7 (43.8) | 13 (41.9) | ||
| Multiple unifocal | 5 (33.3) | 2 (12.5) | 7 (22.6) | ||
| Multifocal | 4 (26.7) | 7 (43.8) | 11 (35.5) | ||
| Topography n (%) | |||||
| Head | 3 (20.0) | 4 (25.0) | 7 (22.6) | ||
| Lower limbs | 9 (60.0) | 8 (50.0) | 17 (54.8) | ||
| Upper limbs | 6 (40.0) | 8 (50.0) | 14 (45.2) | ||
| Trunk | 2 (13.3) | 2 (12.5) | 4 (12.9) | ||
| Type of lesion n (%) | |||||
| Nodule | 13 (86.7) | 14 (87.5) | 27 (87.1) | ||
| Plaque | 0 (0) | 1 (6.25) | 1 (3.2) | ||
| Macule | 0 (0) | 1 (6.25) | 1 (3.2) | ||
| Ulcer | 2 (13.3) | 0 (0) | 2 (6.5) | ||
| Adenopathy n (%) | 4 (26.7) | 3 (18.8) | 7 (22.6) |
| Treatment | Daily Dosage | Duration | Number | Therapeutic Response | Follow-Up Time after Treatment | ||
|---|---|---|---|---|---|---|---|
| Complete Response | Partial Response | Treatment Failure | |||||
| 5-Fluorocytosine | 100–150 mg/kg | 1–3 mths | 3 | 0 | 0 | 3 | 12 yrs |
| Sulfamethoxypyridazine | 500 mg | 1 mth | 1 | 0 | 1 | 0 | 7 yrs |
| Miconazole injection | 0.5 mL/inj/mth | 5 mths | 1 | 0 | 0 | 1 | 7 mths |
| Terbinafine | 500 mg | 2–6 mths | 2 | 0 | 0 | 2 | 6 mths |
| Terbinafine + Surgical excision | 500 mg | 2 mths | 1 | 1 | 0 | 0 | 12 yrs |
| Itraconazole | 200–400 mg | 1–4 mths | 3 | 0 | 0 | 3 | 1–4 mths |
| Itraconazole Clofazimine + Surgical excision | 400 mg 100 mg | 1 mth | 1 | 0 | 0 | 1 | 3 yrs |
| Posaconazole | 800 mg | 18 mths | 1 ** | 0 | 1 | 0 | 18 mths |
| MDT * | - | 1–12 mths | 3 ** | 0 | 1 | 2 | 12 mths |
| Total | 16 | 1 | 3 | 12 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grotta, G.; Couppie, P.; Demar, M.; Drak Alsibai, K.; Blaizot, R. Fungal Density in Lobomycosis in French Guiana: A Proposal for a New Clinico-Histological and Therapeutic Classification. J. Fungi 2023, 9, 1005. https://doi.org/10.3390/jof9101005
Grotta G, Couppie P, Demar M, Drak Alsibai K, Blaizot R. Fungal Density in Lobomycosis in French Guiana: A Proposal for a New Clinico-Histological and Therapeutic Classification. Journal of Fungi. 2023; 9(10):1005. https://doi.org/10.3390/jof9101005
Chicago/Turabian StyleGrotta, Geoffrey, Pierre Couppie, Magalie Demar, Kinan Drak Alsibai, and Romain Blaizot. 2023. "Fungal Density in Lobomycosis in French Guiana: A Proposal for a New Clinico-Histological and Therapeutic Classification" Journal of Fungi 9, no. 10: 1005. https://doi.org/10.3390/jof9101005