
Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Pathogenesis of Otomycosis
4. Clinical Presentation
5. Diagnostic Procedure
6. Treatment
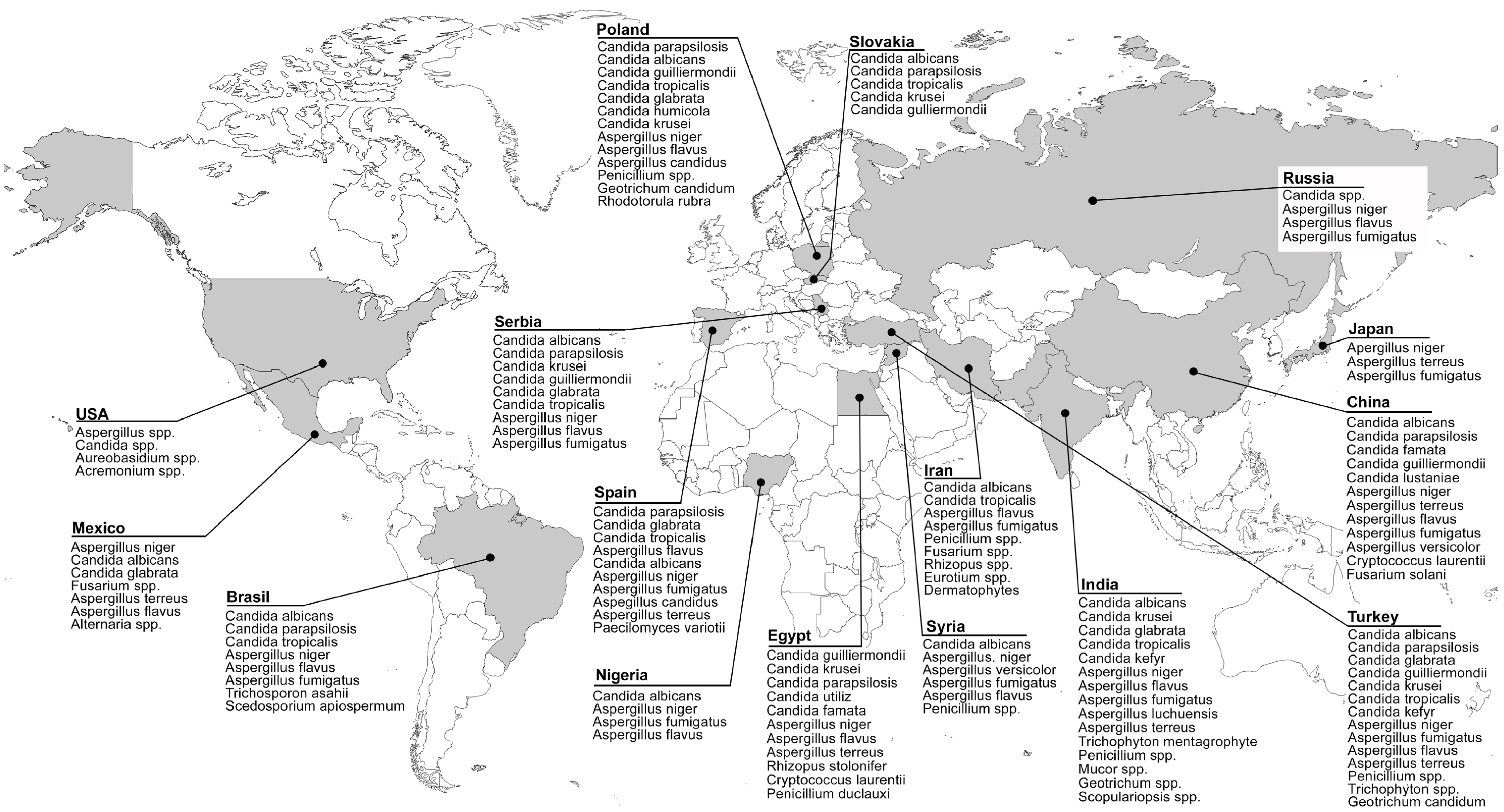
7. Epidemiology
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fasunla, J.; Ibekwe, T.; Onakoya, P. Otomycosis in western Nigeria. Mycoses 2008, 51, 67–70. [Google Scholar] [CrossRef]
- Agarwal, P.; Devi, L.S. Otomycosis in a Rural Community Attending a Tertiary Care Hospital: Assessment of Risk Factors and Identification of Fungal and Bacterial Agents. J. Clin. Diagn. Res. 2017, 11, Dc14–Dc18. [Google Scholar] [CrossRef] [PubMed]
- Mofatteh, M.R.; Naseripour Yazdi, Z.; Yousefi, M.; Namaei, M.H. Comparison of the recovery rate of otomycosis using betadine and clotrimazole topical treatment. Braz. J. Otorhinolaryngol. 2018, 84, 404–409. [Google Scholar] [CrossRef]
- Tasić-Otašević, S.; Golubović, M.; Đenić, S.; Ignjatović, A.; Stalević, M.; Momčilović, S.; Bojanović, M.; Arsić-Arsenijević, V. Species distribution patterns and epidemiological characteristics of otomycosis in Southeastern Serbia. J. De Mycol. Médicale 2020, 30, 101011. [Google Scholar] [CrossRef]
- Kamali Sarvestani, H.; Seifi, A.; Falahatinejad, M.; Mahmoudi, S. Black aspergilli as causes of otomycosis in the era of molecular diagnostics, a mini-review. J. Mycol. Med. 2022, 32, 101240. [Google Scholar] [CrossRef] [PubMed]
- Aneja, K.R.; Sharma, C.; Joshi, R. Fungal infection of the ear: A common problem in the north eastern part of Haryana. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Buonafina-Paz, M.D.; Santos, F.A.; Leite-Andrade, M.C.; Alves, A.I.; Bezerra, J.D.; Leal, M.C.; Robert, E.; Pape, P.L.; Lima-Neto, R.G.; Neves, R.P. Otomycosis caused by the cryptic and emerging species Aspergillus sydowii: Two case reports. Future Microbiol. 2022, 17, 1437–1443. [Google Scholar] [CrossRef]
- Değerli, K.; Ecemiş, T.; Günhan, K.; Başkesen, T.; Kal, E. Agents of otomycosis in Manisa region, Turkey, 1995–2011. Mikrobiyol. Bul. 2012, 46, 79–84. [Google Scholar]
- Abastabar, M.; Haghani, I.; Ahangarkani, F.; Rezai, M.S.; Taghizadeh Armaki, M.; Roodgari, S.; Kiakojuri, K.; Al-Hatmi, A.M.S.; Meis, J.F.; Badali, H. Candida auris otomycosis in Iran and review of recent literature. Mycoses 2019, 62, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Ali, K.; Hamed, M.A.; Hassan, H.; Esmail, A.; Sheneef, A. Identification of Fungal Pathogens in Otomycosis and Their Drug Sensitivity: Our Experience. Int. Arch. Otorhinolaryngol. 2018, 22, 400–403. [Google Scholar] [CrossRef] [Green Version]
- Prasad, S.C.; Kotigadde, S.; Shekhar, M.; Thada, N.D.; Prabhu, P.; D’ Souza, T.; Prasad, K.C. Primary otomycosis in the Indian subcontinent: Predisposing factors, microbiology, and classification. Int. J. Microbiol. 2014, 2014, 636493. [Google Scholar] [CrossRef] [PubMed]
- Alarid-Coronel, J.; Celis-Aguilar, E.; Escobar-Aispuro, L.; Muñoz-Estrada, V. Otomycosis in immunocompetent patients: Clinical and mycological features. Our experience with 40 cases. Clin. Otolaryngol. 2018, 43, 373–377. [Google Scholar] [CrossRef]
- García-Agudo, L.; Aznar-Marín, P.; Galán-Sánchez, F.; García-Martos, P.; Marín-Casanova, P.; Rodríguez-Iglesias, M. Otomycosis due to filamentous fungi. Mycopathologia 2011, 172, 307–310. [Google Scholar] [CrossRef]
- Ho, T.; Vrabec, J.T.; Yoo, D.; Coker, N.J. Otomycosis: Clinical features and treatment implications. Otolaryngol. Head Neck Surg. 2006, 135, 787–791. [Google Scholar] [CrossRef]
- Rawat, S.; Saxena, N.; Chad, A.; Garg, N.; Sharma, K. Cinicomycological study of otomycosis with antifungal drug susceptibility testing of Candida isolates using disk diffusion method in Kota region, Rajasthan. Int. J. Curr. Microbiol. App. Sci. 2017, 6, 3356–3366. [Google Scholar] [CrossRef]
- Trabelsi, H.; Neji, S.; Hadrich, I.; Sellami, M.; Khemakhem, N.; Sellami, H.; Makni, F.; Hammami, B.; Ayadi, A. Unusual case of otomycosis caused by Saksenaea vasiformis. Med. Mycol. Case Rep. 2020, 27, 68–71. [Google Scholar] [CrossRef]
- Baumgartner, B.J.; Rakita, R.M.; Backous, D.D. Scedosporium apiospermum otomycosis. Am. J. Otolaryngol. 2007, 28, 254–256. [Google Scholar] [CrossRef]
- Kelly, K.E.; Mohs, D.C. The external auditory canal. Anatomy and physiology. Otolaryngol. Clin. N. Am. 1996, 29, 725–739. [Google Scholar] [CrossRef]
- Linstrom, J.C.; Lucente, F.E. Infections of the External Ear. In Head & Neck Surgery–Otolaryngology, 4th ed.; Bailey, B.J., Johnson, J.T., Newlands, S.D., Eds.; Lippincott Williams & Wilkins: New York, NY, USA, 2006; pp. 1988–2000. [Google Scholar]
- Roland, P.S.; Marple, B.F. Disorders of the external auditory canal. J. Am. Acad. Audiol. 1997, 8, 367–378. [Google Scholar] [PubMed]
- Lum, C.L.; Jeyanthi, S.; Prepageran, N.; Vadivelu, J.; Raman, R. Antibacterial and antifungal properties of human cerumen. J. Laryngol. Otol. 2009, 123, 375–378. [Google Scholar] [CrossRef]
- Clark, W.B.; Brook, I.; Bianki, D.; Thompson, D.H. Microbiology of otitis externa. Otolaryngol. Head Neck Surg. 1997, 116, 23–25. [Google Scholar] [CrossRef] [PubMed]
- Edward, Y.; Irfandy, D. Otomycosis. J. Kesehat. Andalas 2012, 1, 101–106. [Google Scholar] [CrossRef] [Green Version]
- Abdelazeem, M.; Gamea, A.; Mubarak, H.; Elzawawy, N. Epidemiology, causative agents, and risk factors affecting human otomycosis infections. Turk. J. Med. Sci. 2015, 45, 820–826. [Google Scholar] [CrossRef]
- Anwar, K.; Gohar, M.S. Otomycosis; clinical features, predisposing factors and treatment implications. Pak. J. Med. Sci. 2014, 30, 564–567. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.M.; Brown, L.; Cannon, C.R.; Dolor, R.J.; Ganiats, T.G.; Hannley, M.; Kokemueller, P.; Marcy, S.M.; Roland, P.S.; Shiffman, R.N.; et al. Clinical practice guideline: Acute otitis externa. Otolaryngol. Head Neck Surg. 2006, 134, S4–S23. [Google Scholar] [CrossRef]
- Sander, R. Otitis externa: A practical guide to treatment and prevention. Am. Fam. Physician 2001, 63, 927–936, 941–922. [Google Scholar] [PubMed]
- Beers, S.L.; Abramo, T.J. Otitis externa review. Pediatr. Emerg. Care 2004, 20, 250–256. [Google Scholar] [CrossRef]
- Wiegand, S.; Berner, R.; Schneider, A.; Lundershausen, E.; Dietz, A. Otitis Externa. Dtsch. Arztebl. Int. 2019, 116, 224–234. [Google Scholar] [CrossRef]
- Roohi, B.; Nemati, S.; Alipour, A.; Faeli, L.; Mayahi, S.; Haghani, I.; Shalchizadeh, M.; Darini, A.; Al-Hatmi, A.M.S.; Abastabar, M.; et al. Otomycosis: The foremost aetiological agent causing otitis externa and the antifungal susceptibility pattern in North-Western Iran. Mycoses 2023, 66, 87–97. [Google Scholar] [CrossRef]
- Nemati, S.; Gerami, H.; Faghih Habibi, A.; Kazemnejad, E.; Shabani, N.; Aghsaghloo, V.; Montazeri, S. Sertaconazole versus Clotrimazole and Miconazole Creams in the Treatment of Otomycosis: A Placebo-Controlled Clinical Trial. Iran. J. Otorhinolaryngol. 2022, 34, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Vennewald, I.; Klemm, E. Otomycosis: Diagnosis and treatment. Clin. Dermatol. 2010, 28, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Viswanatha, B.; Naseeruddin, K. Fungal infections of the ear in immunocompromised host: A review. Mediterr. J. Hematol. Infect Dis. 2011, 3, e2011003. [Google Scholar] [CrossRef]
- Wu, S.; Cheng, Y.; Lin, S.; Liu, H. A Comparison of Antifungal Drugs and Traditional Antiseptic Medication for Otomycosis Treatment: A Systematic Review and Meta-Analysis. Front. Surg. 2021, 8, 739360. [Google Scholar] [CrossRef] [PubMed]
- Munguia, R.; Daniel, S.J. Ototopical antifungals and otomycosis: A review. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 453–459. [Google Scholar] [CrossRef]
- Panigrahi, M.; Paty, B.P.; Parida, B.; Padhi, S.; Kumari Sahu, S.; Narasimham, M.V.; Mohanty, I. Clinicomycological Study of Otomycosis with Antifungal Susceptibility Testing Of Fungal Isolates. IOSR-JDMS 2019, 18, 7–12. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., 3rd; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A. Fungal spectrum in Otomycosis patients. JK Sci. 2005, 7, 152–155. [Google Scholar]
- Otašević, S.; Momčilović, S.; Stojanović, N.M.; Skvarč, M.; Rajković, K.; Arsić-Arsenijević, V. Non-culture based assays for the detection of fungal pathogens. J. De Mycol. Médicale 2018, 28, 236–248. [Google Scholar] [CrossRef]
- Bojanović, M.; Ignjatović, A.; Stalević, M.; Arsić-Arsenijević, V.; Ranđelović, M.; Gerginić, V.; Stojanović-Radić, Z.; Stojković, O.; Živković-Marinkov, E.; Otašević, S. Clinical Presentations, Cluster Analysis and Laboratory-Based Investigation of Aspergillus Otomycosis-A Single Center Experience. J. Fungi 2022, 8, 315. [Google Scholar] [CrossRef]
- Rawson, T.M.; Fatania, N.; Abdolrasouli, A. UK standards for microbiology investigations of ear infection (SMI B1) are inadequate for the recovery of fungal pathogens and laboratory diagnosis of otomycosis: A real-life prospective evaluation. Mycoses 2022, 65, 490–495. [Google Scholar] [CrossRef]
- Chen, X.-F.; Hou, X.; Xiao, M.; Zhang, L.; Cheng, J.-W.; Zhou, M.-L.; Huang, J.-J.; Zhang, J.-J.; Xu, Y.-C.; Hsueh, P.-R. Matrix-Assisted Laser Desorption/Ionization Time of Flight Mass Spectrometry (MALDI-TOF MS) Analysis for the Identification of Pathogenic Microorganisms: A Review. Microorganisms 2021, 9, 1536. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, S.; Tamura, T.; Satoh, K.; Kamewada, H.; Nakano, M.; Shinden, S.; Yamaguchi, H.; Makimura, K. The Molecular Identification and Antifungal Susceptibilities of Aspergillus Species Causing Otomycosis in Tochigi, Japan. Mycopathologia 2019, 184, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Mao, C.; Li, A.; Hu, J.; Wang, P.; Peng, D.; Wang, J.; Sun, Y. Efficient and accurate diagnosis of otomycosis using an ensemble deep-learning model. Front. Mol. Biosci. 2022, 9, 951432. [Google Scholar] [CrossRef] [PubMed]
- Milanović, M.; Milosavljević, A.; Randjelovic, M. Visualization of microscopic morphological characteristics used for determination of infectious molds. In Proceedings of the 65th National Conference on Electronics, Telecommunication, Computing, Automatic Control and Nuclear Engineering (ETRAN 2021), Ethno Village Stanisici, Republic of Srpska, 8–10 September 2021; ETRAN Society: Belgrade, Serbia, 2021; pp. 528–533. [Google Scholar]
- Zhang, J.; Lu, S.; Wang, X.; Du, X.; Ni, G.; Liu, J.; Liu, L.; Liu, Y. Automatic identification of fungi in microscopic leucorrhea images. J. Opt. Soc. Am. A. Opt. Image Sci. Vis. 2017, 34, 1484–1489. [Google Scholar] [CrossRef]
- Chappe, M.; Vrignaud, S.; de Gentile, L.; Legrand, G.; Lagarce, F.; Le Govic, Y. Successful treatment of a recurrent Aspergillus niger otomycosis with local application of voriconazole. J. Mycol. Med. 2018, 28, 396–398. [Google Scholar] [CrossRef]
- Lee, A.; Tysome, J.R.; Saeed, S.R. Topical azole treatments for otomycosis. Cochrane Database Syst. Rev. 2021, 5, Cd009289. [Google Scholar] [CrossRef]
- Chavan, R.P.; Ingole, S.M.; Kanchewad Resident, G.S. Single Topical Application of 1% Clotrimazole Cream in Otomycosis. Indian J. Otolaryngol. Head Neck Surg. 2023, 75, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Antunes, J.; Mendes, N.; Adónis, C.; Freire, F. Treatment of otomycosis with clotrimazole: Results accordingly with the fungus isolated. Acta Otolaryngol. 2022, 142, 664–667. [Google Scholar] [CrossRef]
- Gülüstan, F.; Abakay, M.A.; Demir, E. Efficacy of topical isoconazole nitrate in the treatment of otomycosis. Am. J. Otolaryngol. 2021, 42, 102961. [Google Scholar] [CrossRef] [PubMed]
- Kryukov, A.I.; Kunelskaya, N.L.; Kunel’skaya, V.Y.; Ivoilov, A.Y.; Turovskiy, A.B.; Shadrin, G.B.; Machulin, A.I. Otomycosis: The modern view of etiology and management. Vestn. Otorinolaringol. 2018, 83, 48–51. [Google Scholar] [CrossRef]
- Yang, T.H.; Young, Y.H. Eradicating Otomycosis with Terbinafine Solution: Basic and Clinical Investigation. Audiol. Neurotol. 2019, 24, 183–190. [Google Scholar] [CrossRef]
- Herasym, K.; Bonaparte, J.P.; Kilty, S. A comparison of Locacorten-Vioform and clotrimazole in otomycosis: A systematic review and one-way meta-analysis. Laryngoscope 2016, 126, 1411–1419. [Google Scholar] [CrossRef]
- Koltsidopoulos, P.; Skoulakis, C. Otomycosis With Tympanic Membrane Perforation: A Review of the Literature. Ear Nose Throat J. 2020, 99, 518–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoenigl, M.; Salmanton-García, J.; Walsh, T.J.; Nucci, M.; Neoh, C.F.; Jenks, J.D.; Lackner, M.; Sprute, R.; Al-Hatmi, A.M.S.; Bassetti, M.; et al. Global guideline for the diagnosis and management of rare mould infections: An initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology and the American Society for Microbiology. Lancet Infect. Dis. 2021, 21, e246–e257. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, A.; Majidinia, M.; Jaafari, A.; Ayatollahi Mousavi, S.A.; Zarei Mahmoudabadi, A.; Alikhah, H. Etiologic Agents of Otomycosis in the North-Western Area of Iran. Jundishapur. J. Microbiol. 2015, 8, e21776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, X.; Liang, Q.; Chi, F.; Cao, W. Otomycosis in Shanghai: Aetiology, clinical features and therapy. Mycoses 2012, 55, 404–409. [Google Scholar] [CrossRef]
- Pontes, Z.B.; Silva, A.D.; Lima Ede, O.; Guerra Mde, H.; Oliveira, N.M.; Carvalho Mde, F.; Guerra, F.S. Otomycosis: A retrospective study. Braz. J. Otorhinolaryngol. 2009, 75, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.T.; Al-Kafri, A.; Ismail, M. Otomycosis in Damascus, Syria: Etiology and clinical features. Curr. Med. Mycol. 2017, 3, 27–30. [Google Scholar] [CrossRef] [Green Version]
- Ozcan, K.M.; Ozcan, M.; Karaarslan, A.; Karaarslan, F. Otomycosis in Turkey: Predisposing factors, aetiology and therapy. J. Laryngol. Otol. 2003, 117, 39–42. [Google Scholar] [CrossRef]
- Kurnatowski, P.; Filipiak, A. Otomycosis: Prevalence, clinical symptoms, therapeutic procedure. Mycoses 2001, 44, 472–479. [Google Scholar] [CrossRef]
- Dorko, E.; Jenca, A.; Orencák, M.; Virágová, S.; Pilipcinec, E. Otomycoses of candidal origin in eastern Slovakia. Folia Microbiol. 2004, 49, 601–604. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Country (Sample Size *) | Identified Fungal Species ** | Reported Signs and Symptoms *** | Predisposing Factors *** | References |
|---|---|---|---|---|
| Asia | ||||
| Japan (29 patients) | A. niger, A. terreus, A. fumigatus | N/A | N/A | Hagiwara, S. et al. [43] |
| China (108 patients) | A. niger, C. albicans, A. terreus, A. flavus, C. lustaniae, A. fumigatus, C. parapsilosis, C. famata, Cryptococcus laurentii, C. guilliermondii, A. versicolor, Fusarium solani | Pruritus, Otorrhea, Ear fullness, Hearing loss, Otalgia, Tinnitus | N/A | Jia, X. et al. [58] |
| India (30 patients) | A. niger, A. flavus, C. tropicalis | Pruritus, Otalgia, Ear fullness, Hearing loss, Otorrhea | Ear pricking with hard objects, Use of oil ear drops, Swimming or pond baths, Diabetes, Immunodeficiency | Panigrahi, M. et al. [36] |
| India (350 patients) | A. niger, A. flavus, A. fumigatus, C. albicans, C. krusei, C. tropicalis, Penicillium spp., Mucor spp., Trichophyton mentagrophyte | Hearing loss, Ear fullness, Pruritus, Otalgia, Otorrhea, Tinnitus | Ear pricking with hard objects, Use of oil ear drops | Agarwal, P. et al. [2] |
| India (100 patients) | A. niger, A. flavus, A. fumigatus, C. albicans, C. tropicalis, C. glabrata,C. kefyr, Penicilium spp., Geotrichum spp., Scopulariopsis spp. | Pruritus, Otalgia, Ear blockage, Tinnitus, Hearing loss, Otorrhea | Use of oil ear drops, Use of antibiotic or wax-dissolving ear drops, Ear pricking with hard objects, Diabetes, Swimming | Rawat, S. et al. [15] |
| India (100 patients) | A. niger, A. fumigatus, A. flavus, Penicillium spp., C. albicans, Rhizospus spp., Chrysosporium spp. | Pruritus, Ear fullness, Otorrhea, Otalgia, Tinnitus | Use of oil ear drops, Ear pricking with hard objects, Use of antibiotic ear drops | Prasad, S.C. et al. [11] |
| Pakistan (180 patients) | N/A | Hearing loss, Pruritus, Otalgia, Otorrhea, Tinnitus | N/A | Anwar, K. et al. [25] |
| Iran (129 patients) | A. niger, A. flavus, A. fumigatus, C. albicans, Penicillium spp., Dermatophytes, C. tropicalis, Fusarium spp., Rhizopus spp., Eurotium spp. | Pruritus, Ear fullness, Otorrhea, Otalgia | Ear pricking with hard objects, Diabetes | Kazemi, A. et al. [57] |
| Syria (70 patients) | A. niger, C. albicans,A. versicolor, A. fumigatus, A. flavus, Penicillium spp. | Otorrhea, Otalgia, Hearing loss | N/A | Ismail, M.T. et al. [60] |
| Turkey (87 patients) | A. niger, A. fumigatus, A. flavus, A. terreus, C. albicans, C. tropicalis, C. kefyr | Pruritus, Otalgia, Hearing loss, Tinnitus, Otorrhea | Wearing a traditional head covering, Swimming in the pool/sea, Spa baths, Itching on other body parts, Long-term antibiotic treatment, Rainy weather season | Ozcan, K.M. et al. [61] |
| Turkey (544 patients) | A. niger, C. tropicalis, A. fumigatus, C. albicans, A. terreus, A. flavus, C. parapsilosis, C. glabrata, Penicillium spp., C. kefyr, C. guilliermondii, C. krusei, Trichophyton spp., Geotrichum candidum | N/A | N/A | Değerli, K. et al. [8] |
| Africa | ||||
| Egypt (110 patients) | A. niger, A. flavus | Pruritus, Otalgia, Hearing loss, Otorrhea | Ear canal trauma, Swimming, Use of antibiotic ear drops, Absent cerumen, Summer season | Abdelazeem, M. et al. [24] |
| Egypt (102 patients) | A. niger, A. flavus, C. famata, A. terreus, C. parapsilosis, C. utiliz, Rhizopus stolonifer, C. guilliermondii, C. krusei, Cryptococcus laurentii, Penicillium duclauxi | Pruritus, Otalgia, Otorrhea, Hearing loss, Tinnitus | N/A | Ali, K. et al. [10] |
| Nigeria (378 patients) | A. niger, A. fumigatus, C. albicans, A. flavus | Pruritus, Otalgia, Tinnitus, Ear fullness, Hearing loss, Otorrhea | Ear pricking with hard objects, Long-term use of oral antibiotics, Use of antibiotic ear drops, Diabetes, Sino-nasal and nasopharyngeal malignancy, Retroviral infection | Fasunla, J. et al. [1] |
| Central America | ||||
| Mexico (40 patients) | A. niger, C. albicans, C. glabrata, Fusarium spp., A. terreus, A. flavus, Alternaria spp. | Pruritus, Hearing loss, Otorrhea, Otalgia | N/A | Alarid-Coronel, J. et al. [12] |
| North America | ||||
| USA (132 patients) | Aspergillus spp. Candida spp. Aureobasidium spp. Acremonium spp. | Otalgia, Otorrhea, Hearing loss, Ear fullness, Pruritus, Tinnitus | Diabetes, History of otologic procedures, Mastoid cavity after surgical procedure | Ho, T. et al. [14] |
| South America | ||||
| Brasil (20 patients) | C. albicans, C. parapsilosis, A. niger, A. flavus, A. fumigatus, C. tropicalis, Trichosporon asahii, Scedosporium apiospermum | Pruritus, Otalgia, Otorrhea, Hearing loss | Chronic otitis, Long-term antibiotic treatment, Absent cerumen, Ear pricking with hard objects | Pontes, Z.B. et al. [59] |
| Europe | ||||
| Poland (96 patients) | C. parapsilosis, C. albicans, A. niger, A. flavus, Penicillium spp., C. guilliermondii, C. tropicalis, C. glabrata, C. humicola, C. krusei, A. candidus, Geotrichum candidum, Rhodotorula rubra | Pruritus, Otorrhea, Ear fullness, Hearing loss, Tinnitus, Otalgia, EAC swelling and redness, Headache | N/A | Kurnatowski, P. et al. [62] |
| Slovakia (40 patients) | C. albicans, C. parapsilosis, C. tropicalis, C. krusei, C. gulliermondii | Burning sensation in the ear, Pruritus, Ear fullness, Hearing loss, Otalgia, Otorrhea, Tinnitus, Headache, Nausea | Swimming pool and sauna usage, Diabetes, Immunosuppressive therapy, Long-term antibiotic treatment | Dorko, E. et al. [63] |
| Spain (390 patients) | C. parapsilosis, A. flavus, C. albicans, A. niger, A. fumigatus, A. candidus, A. terreus, C. glabrata, C. tropicalis, Paecilomyces variotii | Pruritus, Otalgia, Hearing loss | N/A | García-Agudo, L. et al. [13] |
| Russia (331 patients) | A. niger, A. flavus, A. fumigatus, Candida spp. | N/A | N/A | Kryukov, A.I. et al. [52] |
| Serbia (292 patients) | A. niger, C. albicans, C. parapsilosis, A. flavus, A. fumigatus, C. krusei, C. guilliermondii, C. glabrata, C. tropicalis | N/A | N/A | Tasić-Otašević, S. et al. [4] |
| Serbia (30 patients) | A. niger, A. flavus | N/A | Use of antibiotic ear drops, Use of EAC hygiene pro-ducts, Headphone usage, Frequent ORL examinations and rinsing of EAC, Corticosteroid ear drop usage, Predisposing diseases | Bojanović, M. et al. [40] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bojanović, M.; Stalević, M.; Arsić-Arsenijević, V.; Ignjatović, A.; Ranđelović, M.; Golubović, M.; Živković-Marinkov, E.; Koraćević, G.; Stamenković, B.; Otašević, S. Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review. J. Fungi 2023, 9, 662. https://doi.org/10.3390/jof9060662
Bojanović M, Stalević M, Arsić-Arsenijević V, Ignjatović A, Ranđelović M, Golubović M, Živković-Marinkov E, Koraćević G, Stamenković B, Otašević S. Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review. Journal of Fungi. 2023; 9(6):662. https://doi.org/10.3390/jof9060662
Chicago/Turabian StyleBojanović, Mila, Marko Stalević, Valentina Arsić-Arsenijević, Aleksandra Ignjatović, Marina Ranđelović, Milan Golubović, Emilija Živković-Marinkov, Goran Koraćević, Bojana Stamenković, and Suzana Otašević. 2023. "Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review" Journal of Fungi 9, no. 6: 662. https://doi.org/10.3390/jof9060662