Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mak, C.M.; Lee, H.C.; Chan, A.Y.; Lam, C.W. Inborn errors of metabolism and expanded newborn screening: Review and update. Crit. Rev. Clin. Lab. Sci. 2013, 50, 142–162. [Google Scholar] [CrossRef]
- Gurian, E.A.; Kinnamon, D.D.; Henry, J.J.; Waisbren, S.E. Expanded newborn screening for biochemical disorders: The effect of a false-positive result. Pediatrics 2006, 117, 1915–1921. [Google Scholar] [CrossRef]
- Yamada, K.; Osawa, Y.; Kobayashi, H.; Hasegawa, Y.; Fukuda, S.; Yamaguchi, S.; Taketani, T. Serum C14:1/C12:1 ratio is a useful marker for differentiating affected patients with very long-chain acyl-CoA dehydrogenase deficiency from heterozygous carriers. Mol. Genet. Metab. Rep. 2019, 21, 100535. [Google Scholar] [CrossRef] [PubMed]
- Gavrilov, D.K.; Piazza, A.L.; Pino, G.; Turgeon, C.; Matern, D.; Oglesbee, D.; Raymond, K.; Tortorelli, S.; Rinaldo, P. The Combined Impact of CLIR Post-Analytical Tools and Second Tier Testing on the Performance of Newborn Screening for Disorders of Propionate, Methionine, and Cobalamin Metabolism. Int. J. Neonatal Screen. 2020, 6, 33. [Google Scholar] [CrossRef]
- Yeung, M.C.W.; Chan, T.C.H.; Mak, C.M. Clinical Utility of Second-tier Testing in Newborn Screening for Congenital Adrenal Hyperplasia: The Hong Kong Experience. HK J. Paediatr. New Ser. 2020, 25, 3–7. [Google Scholar]
- Chen, H.A.; Hsu, R.H.; Chang, K.L.; Huang, Y.C.; Chiang, Y.C.; Lee, N.C.; Hwu, W.L.; Chiu, P.C.; Chien, Y.H. Asymptomatic ASS1 carriers with high blood citrulline levels. Mol. Genet. Genom. Med. 2022, 10, e2007. [Google Scholar] [CrossRef]
- Siri, B.; Olivieri, G.; Angeloni, A.; Cairoli, S.; Carducci, C.; Cotugno, G.; Di Michele, S.; Giovanniello, T.; La Marca, G.; Lepri, F.R.; et al. The diagnostic challenge of mild citrulline elevation at newborn screening. Mol. Genet. Metab. 2022, 135, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Spiekerkoetter, U.; Bick, D.; Scott, R.; Hopkins, H.; Krones, T.; Gross, E.S.; Bonham, J.R. Genomic newborn screening: Are we entering a new era of screening? J. Inherit. Metab. Dis. 2023, 46, 778–795. [Google Scholar] [CrossRef]
- Ferlini, A.; Gross, E.S.; Garnier, N.; on behalf of the Screen4Care consortium. Rare diseases’ genetic newborn screening as the gateway to future genomic medicine: The Screen4Care EU-IMI project. Orphanet J. Rare Dis. 2023, 18, 310. [Google Scholar] [CrossRef]
- Holm, I.A.; Agrawal, P.B.; Ceyhan-Birsoy, O.; Christensen, K.D.; Fayer, S.; Frankel, L.A.; Genetti, C.A.; Krier, J.B.; LaMay, R.C.; Levy, H.L.; et al. The BabySeq project: Implementing genomic sequencing in newborns. BMC Pediatr. 2018, 18, 225. [Google Scholar] [CrossRef]
- Ji, C.; Farrar, M.A.; Norris, S.; Bhattacharya, K.; Bennetts, B.; Newson, A.J.; Healy, L.; Millis, N.; Kariyawasam, D.S. The Australian landscape of newborn screening in the genomics. Rare Dis. Orphan Drugs J. 2023, 2, 26. [Google Scholar] [CrossRef]
- Tsang, K.; Chan, T.; Yeung, M.; Wong, T.; Lau, W.; Mak, C. Validation of amplicon-based next generation sequencing panel for second-tier test in newborn screening for inborn errors of metabolism. J. Lab. Med. 2021, 45, 267–274. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Lin, Y.; Liu, Y.; Zhu, L.; Le, K.; Shen, Y.; Yang, C.; Chen, X.; Hu, H.; Ma, Q.; Shi, X.; et al. Combining newborn metabolic and genetic screening for neonatal intrahepatic cholestasis caused by citrin deficiency. J. Inherit. Metab. Dis. 2020, 43, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Turgeon, C.T.; Magera, M.J.; Cuthbert, C.D.; Loken, P.R.; Gavrilov, D.K.; Tortorelli, S.; Raymond, K.M.; Oglesbee, D.; Rinaldo, P.; Matern, D. Determination of total homocysteine, methylmalonic acid, and 2-methylcitric acid in dried blood spots by tandem mass spectrometry. Clin. Chem. 2010, 56, 1686–1695. [Google Scholar] [CrossRef] [PubMed]
- Currier, R.J.; Sciortino, S.; Liu, R.; Bishop, T.; Alikhani Koupaei, R.; Feuchtbaum, L. Genomic sequencing in cystic fibrosis newborn screening: What works best, two-tier predefined CFTR mutation panels or second-tier CFTR panel followed by third-tier sequencing? Genet. Med. 2017, 19, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.H.; Gong, J.Y.; Wang, J.S. Citrin deficiency presenting as acute liver failure in an eight-month-old infant. World J. Gastroenterol. 2015, 21, 7331–7334. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Zhu, S.; Miao, H.; Yang, J.; Shi, Y.; Yue, Y.; Zhang, Y.; Yang, R.; Wu, B.; Huang, X. Dynamic changes of metabolic characteristics in neonatal intrahepatic cholestasis caused by citrin deficiency. Front. Mol. Biosci. 2022, 9, 939837. [Google Scholar] [CrossRef] [PubMed]
- Shigetomi, H.; Tanaka, T.; Nagao, M.; Tsutsumi, H. Early Detection and Diagnosis of Neonatal Intrahepatic Cholestasis Caused by Citrin Deficiency Missed by Newborn Screening Using Tandem Mass Spectrometry. Int. J. Neonatal Screen. 2018, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Lund, A.M.; Wibrand, F.; Skogstrand, K.; Bækvad-Hansen, M.; Gregersen, N.; Andresen, B.S.; Hougaard, D.M.; Dunø, M.; Olsen, R.K.J. Use of Molecular Genetic Analyses in Danish Routine Newborn Screening. Int. J. Neonatal Screen. 2021, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.T.; Hsiao, K.J.; Chen, C.Y.; Wu, C.C.; Lin, S.J.; Chou, Y.Y.; Shiesh, S.C. High resolution melting analysis for the detection of SLC25A13 gene mutations in Taiwan. Clin. Chim. Acta 2011, 412, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.W.; Atkins, A.E.; Cordovado, S.K.; Hendrix, M.; Earley, M.C.; Farrell, P.M. Improving newborn screening for cystic fibrosis using next-generation sequencing technology: A technical feasibility study. Genet. Med. 2016, 18, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Sicko, R.J.; Stevens, C.F.; Hughes, E.E.; Leisner, M.; Ling, H.; Saavedra-Matiz, C.A.; Caggana, M.; Kay, D.M. Validation of a Custom Next-Generation Sequencing Assay for Cystic Fibrosis Newborn Screening. Int. J. Neonatal Screen. 2021, 7, 73. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.L.; Qian, G.L.; Wu, D.W.; Miao, J.K.; Yang, X.; Wu, B.Q.; Yan, Y.Q.; Li, H.B.; Mao, X.M.; He, J.; et al. A multicenter prospective study of next-generation sequencing-based newborn screening for monogenic genetic diseases in China. World J. Pediatr. 2023, 19, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Ceyhan-Birsoy, O.; Murry, J.B.; Machini, K.; Lebo, M.S.; Timothy, W.Y.; Fayer, S.; Genetti, C.A.; Schwartz, T.S.; Agrawal, P.B.; Parad, R.B.; et al. Interpretation of Genomic Sequencing Results in Healthy and Ill Newborns: Results from the BabySeq Project. Am. J. Hum. Genet. 2019, 104, 76–93. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Fan, C.; Huang, Y.; Feng, J.; Zhang, Y.; Miao, J.; Wang, X.; Li, Y.; Huang, C.; Jin, W.; et al. Genomic Sequencing as a First-Tier Screening Test and Outcomes of Newborn Screening. JAMA Netw. Open 2023, 6, e2331162. [Google Scholar] [CrossRef]
- Kingsmore, S.F.; Smith, L.D.; Kunard, C.M.; Bainbridge, M.; Batalov, S.; Benson, W.; Blincow, E.; Caylor, S.; Chambers, C.; Del Angel, G.; et al. A genome sequencing system for universal newborn screening, diagnosis, and precision medicine for severe genetic diseases. Am. J. Hum. Genet. 2022, 109, 1605–1619. [Google Scholar] [CrossRef]
- Wojcik, M.H.; Zhang, T.; Ceyhan-Birsoy, O.; Genetti, C.A.; Lebo, M.S.; Yu, T.W.; Parad, R.B.; Holm, I.A.; Rehm, H.L.; Beggs, A.H.; et al. Discordant results between conventional newborn screening and genomic sequencing in the BabySeq Project. Genet. Med. 2021, 23, 1372–1375. [Google Scholar] [CrossRef]
- Kilgore, M.B.; Platis, D.; Lim, T.; Isenberg, S.; Pickens, C.A.; Cuthbert, C.; Petritis, K. Development of a Universal Second-Tier Newborn Screening LC-MS/MS Method for Amino Acids, Lysophosphatidylcholines, and Organic Acids. Anal. Chem. 2023, 95, 3187–3194. [Google Scholar] [CrossRef]
- Mak, J.; Peng, G.; Le, A.; Gandotra, N.; Enns, G.M.; Scharfe, C.; Cowan, T.M. Validation of a targeted metabolomics panel for improved second-tier newborn screening. J. Inherit. Metab. Dis. 2023, 46, 194–205. [Google Scholar] [CrossRef]
- Stenton, S.L.; Campagna, M.; Philippakis, A.; O’Donnell-Luria, A.; Gelb, M.H. First-tier next-generation sequencing for newborn screening: An important role for biochemical second-tier testing. Genet. Med. Open 2023, 1, 100821. [Google Scholar] [CrossRef]
- Peng, G.; Shen, P.; Gandotra, N.; Le, A.; Fung, E.; Jelliffe-Pawlowski, L.; Davis, R.W.; Enns, G.M.; Zhao, H.; Cowan, T.M.; et al. Combining newborn metabolic and DNA analysis for second-tier testing of methylmalonic acidemia. Genet. Med. 2019, 21, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, Y.Y.; Hong, D.Y.; Zhang, Z.L.; Li, Y.H.; Yang, P.Y.; Sun, Y.; Jiang, T.; Xu, Z.F. Combined genetic screening and traditional biochemical screening to optimize newborn screening systems. Clin. Chim. Acta 2022, 528, 44–51. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
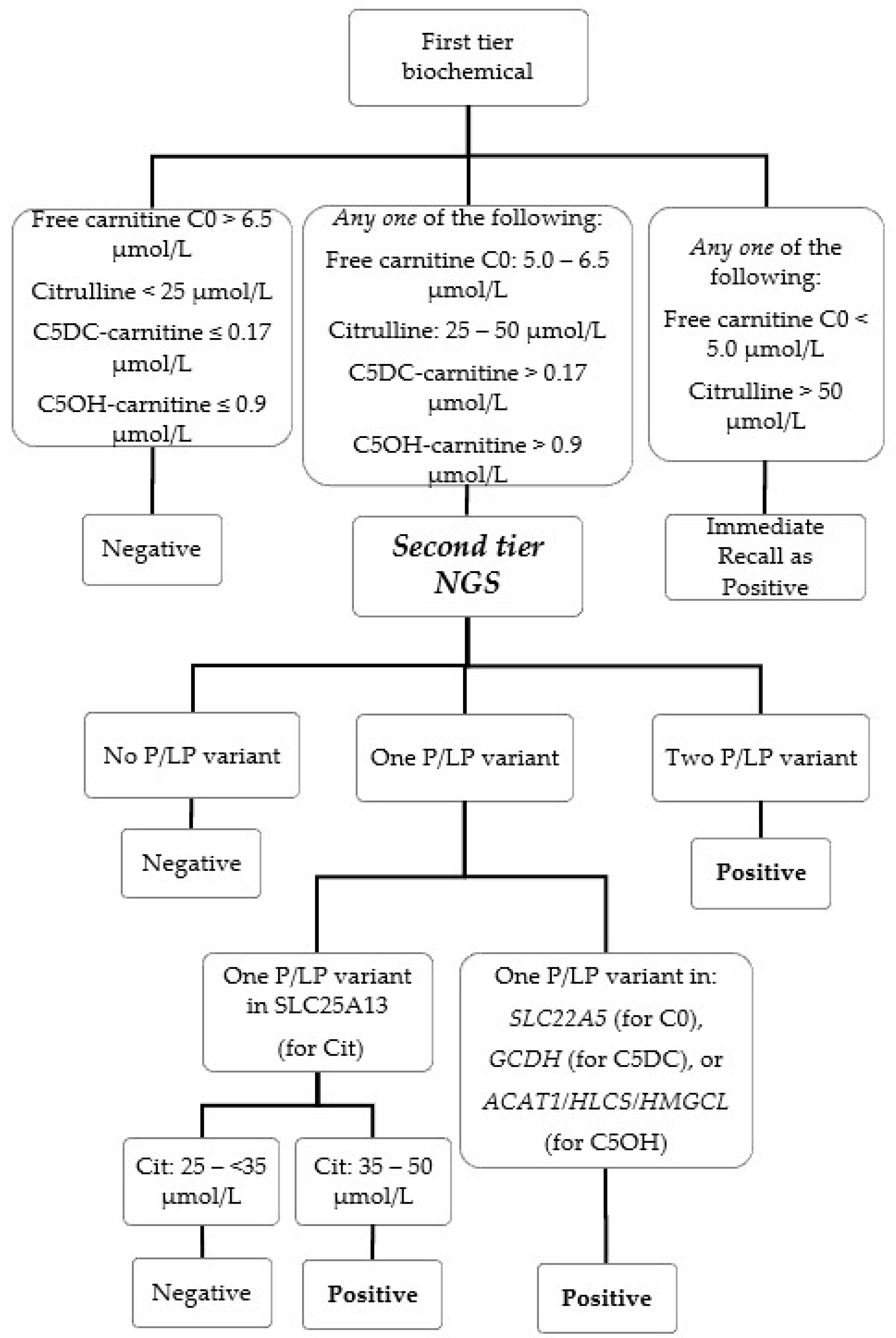
| First-Tier Biochemical | Second-Tier Genetic | Target Condition | Historical Biochemical Cutoff for Recall without 2nd Tier (μmol/L) | ||
|---|---|---|---|---|---|
| Biochemical Marker | Cutoff (μmol/L) | Genotyping Marker | Cutoff | ||
| Free carnitine-C0 | 5.0–6.5 n/c * | Sequence variant in SLC22A5 gene | ≥one P/LP variant | Carnitine uptake defect (CUD, MIM #212140, also known as systemic primary carnitine deficiency) | ≤6.2 c |
| Citrulline | 25–50 n/c ^ | Sequence variant and target screening for IVS16ins3kb in SLC25A13 gene $ | 1. ≥one P/LP variant and citrulline ≥ 35 μmol/L, or 2. ≥two P/LP variant and citrulline ≥25 and <35 μmol/L @ | Citrin deficiency (CD, MIM #605814, also known as citrullinemia type II) | ≥35 c |
| C5DC-carnitine | >0.17 n >0.35 c | Sequence variant in GCDH gene | ≥one P/LP variant | Glutaric acidemia type I (MIM #231670) | ≥0.35 c |
| C5OH-carnitine | >0.9 n >0.7 c | Sequence variant in ACAT1, HLCS and HMGCL gene | ≥one P/LP variant | Beta-ketothiolase deficiency (#203750) Holocarboxylase synthetase deficiency (MIM #253270) 3-Hydroxy-3-methylglutaryl-CoA lyase deficiency (MIM #246450). | ≥0.78 c |
| Case Number | Newborn Screening Result | Confirmatory Genetic Test Result | Clinical Summary | |
|---|---|---|---|---|
| First-Tier Biochemical | Second-Tier Genetic | |||
| Cit-1 (TP) | Citrulline: 27 μmol/L | Homozygous for the pathogenic variant: c.852_855del in SLC25A13 gene | Genetically confirmed as CD, both parents were heterozygote carrier. | 21 months old during latest clinic visit with satisfactory growth and development, on lactose-free formula, uneventful clinical course. |
| Cit-2 (TP) | Citrulline: 26 μmol/L | Heterozygous for the pathogenic variant, c.1311+1G>A, and Target screening positive for heterozygous IVS16ins3kb variant, in SLC25A13 gene | Genetically confirmed as CD, both parents were heterozygote carrier. | 19 months old during latest visit, now with satisfactory growth and development, on lactose-free MCT-enriched formula. Initially screened negative with sequence analysis alone. Presented with conjugated hyperbilirubinemia and failure to thrive at 2 months while on breastfeeding, with no definitive diagnosis despite extensive investigation performed including plasma amino acids and liver biopsy. Jaundice resolved spontaneously at 3 months. Recalled and eventually diagnosed as citrin deficiency at 13 months of age after implementation of target screening for IVS16ins3kb variant. Catch-up growth with appropriate dietary management. |
| Cit-3 (FP) | Citrulline: 26 μmol/L | Heterozygous for the pathogenic variant, c.615+5G>A | Genetically confirmed as CD carrier. | Case closed at 7 months old during latest clinic visit after extensive biochemical and genetic investigations, normal growth and development. |
| Cit-4 (FP) | Citrulline: 26 μmol/L | Heterozygous for the pathogenic variant, c.615 + 5G>A | Genetically confirmed as CD carrier. | Case closed at 7 months old during latest clinic visit after extensive biochemical and genetic investigations, normal growth and development. |
| C0-1 (TP) | Free carnitine C0: 6.9 μmol/L Citrulline: 26 μmol/L | Heterozygous for the pathogenic variant, c.51C>G, and Heterozygous for the pathogenic variant, c.1400C>G in the SLC22A5 gene No P/LP variants in the SLC25A13 gene | Genetically confirmed as CUD, both parents were heterozygote carrier. | 12 months old during latest clinic visit with satisfactory growth and development, on levocarnitine, uneventful clinical course |
| C0-2 (FP) | Free carnitine C0: 6.3 μmol/L | Heterozygous for the pathogenic variant, c.1400C>G in the SLC22A5 gene | Genetically confirmed as CUD carrier | Case closed at 3 months old during latest clinic visit after full biochemical and genetic investigations, normal growth and development. |
| C5DC-1 (FP) | C5DC-carnitine: 0.18 μmol/L | Heterozygous for the pathogenic variant, c.1156C>T in the GCDH gene | Genetically confirmed as GA1 carrier | Case closed at 7 months old during latest clinic visit after full biochemical and genetic investigations, normal growth and development. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, T.C.H.; Mak, C.M.; Yeung, M.C.W.; Law, E.C.-Y.; Cheung, J.; Wong, T.K.; Cheng, V.W.-S.; Lee, J.K.H.; Wong, J.C.L.; Fung, C.W.; et al. Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism. Int. J. Neonatal Screen. 2024, 10, 19. https://doi.org/10.3390/ijns10010019
Chan TCH, Mak CM, Yeung MCW, Law EC-Y, Cheung J, Wong TK, Cheng VW-S, Lee JKH, Wong JCL, Fung CW, et al. Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism. International Journal of Neonatal Screening. 2024; 10(1):19. https://doi.org/10.3390/ijns10010019
Chicago/Turabian StyleChan, Toby Chun Hei, Chloe Miu Mak, Matthew Chun Wing Yeung, Eric Chun-Yiu Law, Jana Cheung, Tsz Ki Wong, Vincent Wing-Sang Cheng, Jacky Kwan Ho Lee, Jimmy Chi Lap Wong, Cheuk Wing Fung, and et al. 2024. "Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism" International Journal of Neonatal Screening 10, no. 1: 19. https://doi.org/10.3390/ijns10010019