
Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening
 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Use Case
2.2. Program Goals
- Engage parents and families living with newborns, children, and adults with SMA to identify LTFU themes to prioritize for SMA;
- Design, implement, and evaluate data collection with input from at least five pediatric neurologists caring for NBS-identified SMA cases;
- Connect the clinical site with their respective state NBS program to foster LTFU collaboration;
- Design, implement, and evaluate data dashboards designed for clinical sites and state NBS programs;
- Design and disseminate LTFU data points that are important for the LTFU of SMA to all state NBS programs in the US;
- Increase the number of infants, children, and families who receive coordinated LTFU care through a medical home by 20 percent from baseline.
2.3. Workflow
- Recruitment of Sites
- Website
- Clinical Sites
- State NBS Programs
- 2.
- Tool Design
- Literature Review
- Family Prioritization of Data Points
- Consultation with Clinicians
- LTFU-Cares Using REDCap®
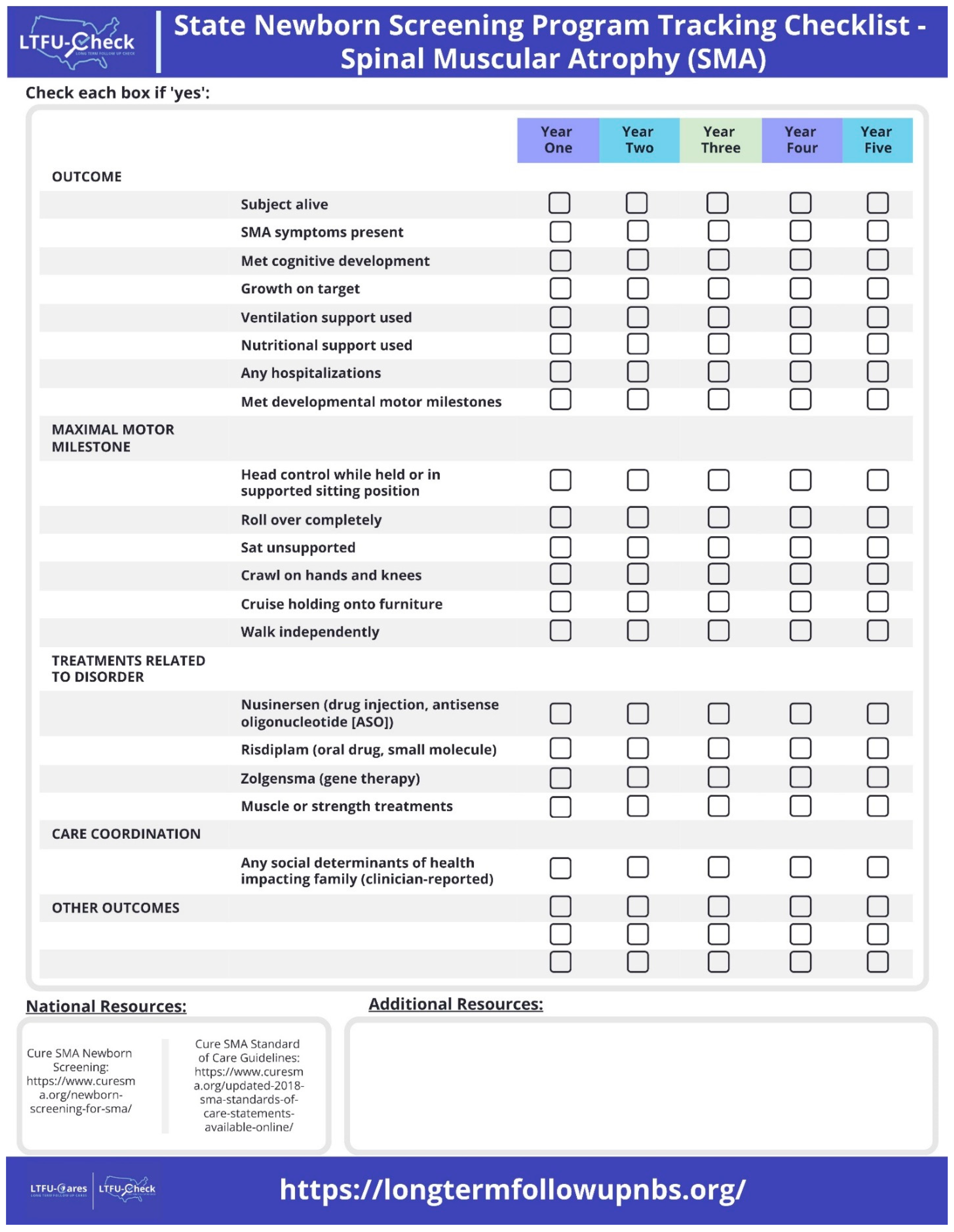
- LTFU-Check
- 3.
- Data Collection using LTFU-Cares
- 4.
- Data Dissemination with LTFU-Cares Dashboard
- 5.
- Project Evaluation
3. Preliminary Results
3.1. Recruitment of Sites
3.1.1. Website
3.1.2. Clinical Sites
3.1.3. State NBS Programs
3.2. Tool Design
3.2.1. Parent and Family Engagement
3.2.2. LTFU-Cares Data Collection
3.2.3. LTFU-Cares Data Dashboard
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Motyl, A.A.L.; Gillingwater, T.H. Timing Is Everything: Clinical Evidence Supports Pre-Symptomatic Treatment for Spinal Muscular Atrophy. Cell Rep. Med. 2022, 3, 100725. [Google Scholar] [CrossRef] [PubMed]
- Brower, A.; Chan, K.; Williams, M.; Berry, S.; Currier, R.; Rinaldo, P.; Caggana, M.; Gaviglio, A.; Wilcox, W.; Steiner, R.; et al. Population-Based Screening of Newborns: Findings from the NBS Expansion Study (Part One). Front. Genet. 2022, 13, 867337. [Google Scholar] [CrossRef] [PubMed]
- The United Nations. Convention on the Rights of the Child; UN General Assembly: New York, NY, USA, 1989. [Google Scholar]
- Describing SMA—Cure SMA. Available online: https://www.curesma.org/describing-sma/ (accessed on 1 February 2024).
- Lee, B.H.; Waldrop, M.A.; Connolly, A.M.; Ciafaloni, E. Time Is Muscle: A Recommendation for Early Treatment for Preterm Infants with Spinal Muscular Atrophy. Muscle Nerve 2021, 64, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Osterman, M.; Hamilton, B.; Martin, J.; Driscoll, A.; Valenzuela, C. Births: Final Data for 2020; National Center for Health Statistics (U.S.): Hyattsville, MA, USA, 2021. [CrossRef]
- Al-Zaidy, S.; Pickard, A.S.; Kotha, K.; Alfano, L.N.; Lowes, L.; Paul, G.; Church, K.; Lehman, K.; Sproule, D.M.; Dabbous, O.; et al. Health Outcomes in Spinal Muscular Atrophy Type 1 Following AVXS-101 Gene Replacement Therapy. Pediatr. Pulmonol. 2019, 54, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Aslesh, T.; Yokota, T. Restoring SMN Expression: An Overview of the Therapeutic Developments for the Treatment of Spinal Muscular Atrophy. Cells 2022, 11, 417. [Google Scholar] [CrossRef] [PubMed]
- Butterfield, R.J. Spinal Muscular Atrophy Treatments, Newborn Screening, and the Creation of a Neurogenetics Urgency. Semin. Pediatr. Neurol. 2021, 38, 100899. [Google Scholar] [CrossRef] [PubMed]
- Corsello, A.; Scatigno, L.; Pascuzzi, M.C.; Calcaterra, V.; Dilillo, D.; Vizzuso, S.; Pelizzo, G.; Zoia, E.; Mandelli, A.; Govoni, A.; et al. Nutritional, Gastrointestinal and Endo-Metabolic Challenges in the Management of Children with Spinal Muscular Atrophy Type 1. Nutrients 2021, 13, 2400. [Google Scholar] [CrossRef] [PubMed]
- Dangouloff, T.; Botty, C.; Beaudart, C.; Servais, L.; Hiligsmann, M. Systematic Literature Review of the Economic Burden of Spinal Muscular Atrophy and Economic Evaluations of Treatments. Orphanet J. Rare Dis. 2021, 16, 47. [Google Scholar] [CrossRef] [PubMed]
- Van Der Heul, A.M.B.; Cuppen, I.; Wadman, R.I.; Asselman, F.; Schoenmakers, M.A.G.C.; Van De Woude, D.R.; Gerrits, E.; Van Der Pol, W.L.; Van Den Engel-Hoek, L. Feeding and Swallowing Problems in Infants with Spinal Muscular Atrophy Type 1: An Observational Study. J. Neuromuscul. Dis. 2020, 7, 323–330. [Google Scholar] [CrossRef]
- De Holanda Mendonça, R.; Jorge Polido, G.; Ciro, M.; Jorge Fontoura Solla, D.; Conti Reed, U.; Zanoteli, E. Clinical Outcomes in Patients with Spinal Muscular Atrophy Type 1 Treated with Nusinersen. J. Neuromuscul. Dis. 2021, 8, 217–224. [Google Scholar] [CrossRef]
- Kennedy, R.A.; Carroll, K.; McGinley, J.L.; Paterson, K.L. Walking and Weakness in Children: A Narrative Review of Gait and Functional Ambulation in Paediatric Neuromuscular Disease. J. Foot Ankle Res. 2020, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.H.; Collins, E.; Lewis, L.; Guntrum, D.; Eichinger, K.; Voter, K.; Abdel-Hamid, H.Z.; Ciafaloni, E. Combination Therapy with Nusinersen and AVXS-101 in SMA Type 1. Neurology 2019, 93, 640–641. [Google Scholar] [CrossRef] [PubMed]
- Markati, T.; Fisher, G.; Ramdas, S.; Servais, L. Risdiplam: An Investigational Survival Motor Neuron 2 (SMN2) Splicing Modifier for Spinal Muscular Atrophy (SMA). Expert. Opin. Investig. Drugs 2022, 31, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Matesanz, S.E.; Curry, C.; Gross, B.; Rubin, A.I.; Linn, R.; Yum, S.W.; Kichula, E.A. Clinical Course in a Patient with Spinal Muscular Atrophy Type 0 Treated with Nusinersen and Onasemnogene Abeparvovec. J. Child. Neurol. 2020, 35, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Salmin, F.; Albamonte, E.; Morettini, V.; Gagliano, N.; Mercuri, E.; Sansone, V.A. Resolution of Skin Necrosis after Nusinersen Treatment in an Infant with Spinal Muscular Atrophy. Muscle Nerve 2019, 59, E42–E44. [Google Scholar] [CrossRef] [PubMed]
- Vega, P.; Glisser, C.; Castiglioni, C.; Amézquita, M.V.; Quirola, M.; Barja Yañez, S. Calidad de Vida En Niños y Adolescentes Con Atrofia Muscular Espinal. Rev. Chil. Pediatr. 2020, 91, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Waldrop, M.A.; Elsheikh, B.H. Spinal Muscular Atrophy in the Treatment Era. Neurol. Clin. 2020, 38, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Wurster, C.; Petri, S. Progress in Spinal Muscular Atrophy Research. Curr. Opin. Neurol. 2022, 35, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Brower, A.; Chan, K.; Hartnett, M.; Taylor, J. The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts. Int. J. Neonatal. Screen. 2021, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.; Hu, Z.; Bush, L.W.; Cope, H.; Holm, I.A.; Kingsmore, S.F.; Wilhelm, K.; Scharfe, C.; Brower, A. NBSTRN Tools to Advance Newborn Screening Research and Support Newborn Screening Stakeholders. Int. J. Neonatal. Screen. 2023, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.A.; Leslie, N.D.; Edick, M.J.; Hiner, S.; Justice, K.; Cameron, C. Inborn Errors of Metabolism Collaborative: Large-Scale Collection of Data on Long-Term Follow-up for Newborn-Screened Conditions. Genet. Med. 2016, 18, 1276–1281. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, N.; Howell, S.; Davis, S.; Kowal, K.; Tanda, T.; Brown, M.; Boada, C.; Alston, A.; Crawford, L.; Thompson, T.; et al. Early neurodevelopmental and medical profile in children with sex chromosome trisomies: Background for the prospective eXtraordinarY babies study to identify early risk factors and targets for intervention. Am. J. Med. Genet. C 2020, 184, 428–443. [Google Scholar] [CrossRef] [PubMed]
- Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity|KFF. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/ (accessed on 26 October 2023).
- Newborn Screening for SMA—Cure SMA. Available online: https://www.curesma.org/newborn-screening-for-sma/ (accessed on 21 February 2024).
- Updated 2018 SMA Standards of Care Statements Available Online—Cure SMA. Available online: https://www.curesma.org/updated-2018-sma-standards-of-care-statements-available-online/ (accessed on 21 February 2024).
- Kemper, A.; Lam, K.; Comeau, A.; Kwon, J.; Green, N.; Ojodu, J.; Grosse, S.; Prosser, L.; Jones, E.; Tanksley, S. Evidence-Based Review of Newborn Screening for Spinal Muscular Atrophy (SMA): Final Report (v5.2); Maternal and Child Health Bureau. 2018. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/reports-recommendations/sma-final-report.pdf (accessed on 26 February 2024).
- AAP Motor Delay Tool. Available online: https://www.healthychildren.org/English/MotorDelay/Pages/default.aspx (accessed on 9 July 2019).
- CDC. What Is a Developmental Milestone? Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://www.cdc.gov/ncbddd/actearly/milestones/index.html (accessed on 26 February 2024).




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lietsch, M.; Chan, K.; Taylor, J.; Lee, B.H.; Ciafaloni, E.; Kwon, J.M.; Waldrop, M.A.; Butterfield, R.J.; Rathore, G.; Veerapandiyan, A.; et al. Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening. Int. J. Neonatal Screen. 2024, 10, 34. https://doi.org/10.3390/ijns10020034
Lietsch M, Chan K, Taylor J, Lee BH, Ciafaloni E, Kwon JM, Waldrop MA, Butterfield RJ, Rathore G, Veerapandiyan A, et al. Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening. International Journal of Neonatal Screening. 2024; 10(2):34. https://doi.org/10.3390/ijns10020034
Chicago/Turabian StyleLietsch, Mei, Kee Chan, Jennifer Taylor, Bo Hoon Lee, Emma Ciafaloni, Jennifer M. Kwon, Megan A. Waldrop, Russell J. Butterfield, Geetanjali Rathore, Aravindhan Veerapandiyan, and et al. 2024. "Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening" International Journal of Neonatal Screening 10, no. 2: 34. https://doi.org/10.3390/ijns10020034