1. Introduction
The Perkin Elmer Genetic Screening Processor (GSP)™ is a fully automated system for the processing of immunoassays for TSH, 17-OHP, IRT, biotinidase, and total T4, as well as enzymatic assays for total galactose and galactose-1-phosphate uridyltransferase (GALT) from dried blood spots (DBS) [
1,
2]. In Switzerland GALT activity is measured with the GSP since 2011. In the central newborn screening laboratory in Zurich there are 2 instruments available. The principle of the assay is still the same as the classical beutler test [
3,
4]. The GSP however, has one drawback: it cannot transfer samples from one microtiterplate to another. While this is not a problem with immunoassays, it makes enzymatic assays more problematic, because the blood spots have to remain in the wells and can cause significant signal quenching, thereby reducing sensitivity, or they can increase fluorescence intensity, when the extracted spots are floating on the surface of the reaction mixture. The later can cause false negative results, when GALT activity is measured for galactosaemia screening [
1]. To overcome this problem, the GSP includes an additional measurement step to check for floating disks, leading to prevention of the affected measurements. However, this causes a secondary problem in this totally closed system. We detected floating disk signals in approx. 0.7% of all samples, screening samples as well as quality control samples, so that these measurements had to be repeated. In some cases even a second sample had to be requested, because floating disks were detected again in the 2nd, 3rd, and 4th repeat assays. We describe a simple method, which is just a re-measurement on a victor fluorescence reader, or any other plate fluorimeter, with filters for excitation wavelength 340 nm, and emission wavelength 405 nm. Using this re-measurement approach made all repeat measurements unnecessary.
2. Methods
2.1. Routine Measurement of GALT Activity
GALT activity was measured using the Perkin Elmer GSP Neonatal GALT kit. 3.2 mm circles of calibrators, controls, and samples from newborns were punched into the respective microtiterplates of the test kits, which were placed afterwards into the GSP where they were processed and measured according to the test protocol of the instrument and test kit. After the measurement, the microtiterplates of the GALT assay are collected in the output magazine of the GSP without removal of the reagents.
2.2. Remeasurement of GALT Activity
In case the GSP detected a “floating disc”, the respective microtiterplates were removed from the GSP. All floating discs were removed from the respective wells using a sharp pair of tweezers. After removal of all floating discs, the fluorescence of the respective microtiterplates were measured together with calibrators and controls on Victor2™ D fluorimeter from Perkin Elmer, with excitation wavelength 340 nm, and emission wavelength 405 nm, within 1 h.
3. Result
Since January 1
st 2011 we have measured 517,372 samples. The utilization ratio of both instruments was quite equal, with the ratio GSP-1/GSP-2 = 1.05. In total we found a “floating disc” signal in 0.66% of all measurements. The floating disc problem was seen equally in screening and QC samples. The ratio of floating disc signals in QC samples compared to screening samples was 2.42% which quite well resembles the frequency of QC samples compared to routine samples in total. On every microtiter plate we had 2–3 control samples. During the evaluation of the frequency of floating disc signals it became clear that despite an equal utilization of the 2 GSPs, the number of floating disc signals on GSP-1 was nearly twice as high as the one on GSP-2, with a ratio of 1.97 (
Figure 1). A correlation of floating disc signals to different batches of filterpaper could not be observed.
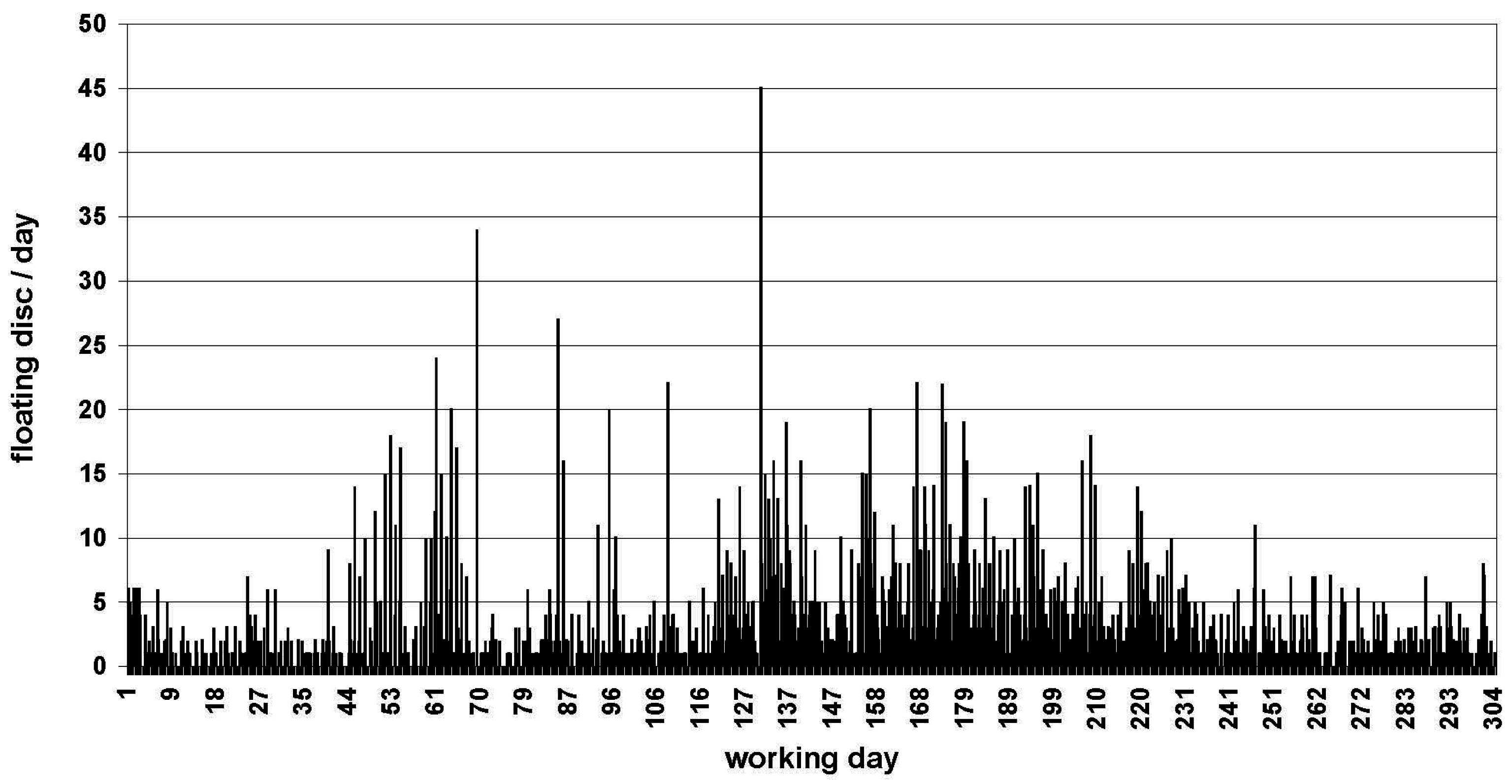
In the chronological sequence, certain clusters could be anticipated (
Figure 2), for example around batch No. 2011-201, 2012-195, between 2013-141 and 2013-191, between 2014-139 and 2014-189, between 2015-036 and 2015-086, and around 2015-136. However, they could not be significantly related to a particular season (
Figure 3). In addition, we could observe that samples which did not elute properly very often showed a floating disc signal at the same time. Therefore, we punched 61 white filterpaper discs into subsequent routine assays. These “white” samples persistently gave an “elution failed” signal and a “floating disc” signal.
The mean difference of re-measured samples on the Victor was 6.1%, QC-samples are always in the expected range, and true positive samples from patients with classical galactosaemia and QC-samples with 0%–10% residual activity (or less than 2 U, according to the GSP-GALT test kit) were always positive when re-measured. To test the stability of the signal intensity a whole daily routine (n = 188) was re-measured after 1 h, 16 h, and 24 h. The standard deviation and coefficient of variation of the mean GALT activity of all 4 measurements (including the measurement on the GSP) were 1.8% and 13.5% respectively.
4. Discussion
By measuring completely processed microtiterplates of the GALT-assays on a Victor, we could easily prevent unnecessary work from repunching samples and in particular we could prevent unnecessary second heelpricks in healthy newborns. The re-measurement can be made with any plate fluorimeter that is able to measure NADP/NADPH (excitation 340 nm; emission 405 nm). The reason for this significant difference of the frequency of floating disc signals on 2 equally utilized GSPs over a time course of 5 years is yet unknown. However, besides sample dependent causes for floating discs, there must also be device related causes of “floating disc” signals. Unfortunately, due to the totally closed architecture of the GSPs we had no chance to elucidate these device related causes.
5. Conclusions
Fully automated systems are principally fast, reliable, and accurate platforms for high throughput screening processes, as newborn screening in centralized laboratories normally is. However, if a system is as closed as the GSP is, there is nearly no room for interaction or manipulation by the operator. While this normally prevents errors and increases accuracy, in some cases, like floating discs, it produces unnecessary workload in the laboratory, and even worse, in single cases it causes an unnecessary second healprick in otherwise healthy babies.
The problem of floating disks also shows a principle problem of closed systems like the GSP, where no other procedures are possible, but running the manufactures test-kits, according to the kit protocol. Without stand-alone devices, screening laboratories are totally committed to the manufacturer. Therefore, it seems advisable to recommend that newborn screening laboratories do not totally rely on fully automated systems, but keep the ability for manual performance of screening tests in case of failure, malfunctions, or down time of the automated systems.
Author Contributions
All authors have participated in the concept and design, analysis and interpretation of data, drafting or revising of the manuscript; and they have approved the manuscript as submitted.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fingerhut, R.; Torresani, T. Evaluation of the genetic screening processor (GSPTM) for newborn screening. Anal. Methods 2013, 5, 4769–4776. [Google Scholar] [CrossRef]
- Fingerhut, R.; Torresani, T. Determination of Total Galactose from Dried Blood Spots—Extensive Assay Evaluation of a CE-Marked Test-Kit. J. Anal. Sci. Methods Instrum. 2013, 3, 163–166. [Google Scholar] [CrossRef]
- Beutler, E.; Baluda, M.C. A simple spot screening test for galactosemia. J. Lab. Clin. Med. 1966, 68, 137–141. [Google Scholar] [PubMed]
- Beutler, E.; Baluda, M.C. New rapid method for the estimation of red cell galactose-1-phosphate uridyltransferase activity. J. Lab. Clin. Med. 1968, 72, 527–532. [Google Scholar] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).




{kind=link}
{kind=link}
{kind=link}


