1. Introduction
Neonatal hyperbilirubinemia is found in approximately 60% of term and 80% of preterm infants [
1]. Measurement of serum bilirubin is one of the most frequently performed laboratory tests in neonates [
2]. Serial serum bilirubin measurements are used not only to assess the absolute bilirubin concentration but also the rate of change, necessitating the collection of multiple blood samples. Therefore, the possibility of using a noninvasive, painless, and reliable method to determine the bilirubin level and its increment in the first 36 to 72 h after birth has become necessary. This is important in regions where factors such as interruption of power supply, poor maintenance of equipment and shortage of reagents often limit the potential for providing dependable and reliable serum bilirubin measurements. Evaluation of the MBJ20
® transcutaneous bilirubinometer for reliability and accuracy may help reduce repeated blood sampling in a resource-constrained setting such as Anambra State. The availability of MBJ20
®, especially in the primary health centers, will facilitate referrals to tertiary centers once a significant range is determined, thereby reducing unfavorable outcomes. We hypothesized that TcB estimated by MBJ20
® is as good as the Diazo method of measuring the serum bilirubin in jaundiced neonates.
2. Materials and Methods
This study was conducted in the Special Care Baby Unit (SCBU) of Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi, Anambra State, Nigeria. The hospital is the major tertiary health institution in the state. Analysis of the admission records showed that on the average, 60 newborns are admitted monthly and 30%–40% are managed for neonatal jaundice. This was a prospective descriptive cross-sectional hospital based study. Ethical approval for the study was obtained from the Ethical Committee of the Nnamdi Azikiwe University Teaching Hospital Nnewi.
All infants aged less than 28 days presenting to the SCBU with jaundice or who developed jaundice while on admission in the SCBU were assessed for eligibility, and subsequently enrolled for this study following the informed consent obtained from caregivers. Neonates with exfoliative skin infections affecting either the glabellar or midsternum and those who have had exchange blood transfusion or have undergone phototherapy prior to presentation were excluded.
The baseline variables obtained included gestational age, post natal age, sex, birth weight and weight on admission and the socio-demographic factors such as place of birth (delivery at NAUTH, other public hospital, private hospital, maternity, traditional birth home) and predisposing factors. Gestational age was measured in weeks. Babies were grouped into preterm <37 weeks, term ≥37 to 42 weeks and post term >42 weeks [
3]. Postnatal age was recorded in days. The neonates were categorized into extremely low birth weight <1000 g, very low birth weight 1000–1499 g, low birth weight <1500–2499 g, normal birth weight ≥2500–4200 g and macrosomia >4200 g [
3].
2.1. Measurement of Total Serum Bilirubin
Two milliliters (2 mL) of venous blood was collected from the ante cubital fossa into a plain bottle while maintaining asepsis. The sample was labeled and taken to the Chemical Pathology Laboratory within 10 min of collection for immediate analysis. The total serum bilirubin was estimated using a standard laboratory method of Evelyn and Malloy procedure that employed Diazo reagents [
4].
2.2. Estimation of Bilirubin Level Using MBJ20® Transcutaneous Bilirubinometer
Prior to the measurement the instrument was validated (calibration and within-run precision) to confirm repeatability and reproducibility. Four measurements were taken the same time within 10 min of sample collection for serum bilirubin measurement. The transcutaneous jaundice meter was placed gently but firmly on the selected areas. Two measurements were made from the forehead (glabella area) and the other two measurements from the mid sternum (angle of Louis). The bilirubin concentration in mg/dL was clearly displayed on the LED screen. The value of bilirubin measured differently by the device on the glabella and sternum were recorded in mg/dL as the final measurement.
3. Results
Three hundred and eighty-eight (388) neonates were admitted into the SCBU during the period of this study. Out of these, 88 neonates, 53 (60.2%) males and 35 (39.8%) females with a male to female ratio of 1.5:1, were evaluated for hyperbilirubinemia. Forty-eight (54.54%) of the neonates were preterm, 39 (44.32%) were term, and one (1.14%) was post-term. The gestational age range of preterms was 28–36 weeks with a mean (SD) of 31.9 (2.5) weeks, respectively, while the gestational age of term babies was 37–42 weeks with a mean (SD) of 39.5 (1.4) weeks, respectively. A total of 222 paired tests, comprising 102 (45.95%) paired tests for term and post-term (≥37–44 weeks) and 120 (54.05%) paired tests for preterm (<37 weeks) neonates, were generated.
Table 1 shows the distribution of bilirubin levels based on the severity of jaundice measured using each of the methods. The mean (SD) bilirubin level was highest using transcutaneous bilirubin (forehead) TcBF 14.1 (5.0) mg/dL, followed by transcutaneous bilirubin (sternum) TcBS 12.9 (5.1) mg/dL, and the lowest was the total serum bilirubin TSB method 10.9 (4.7) mg/dL. The ranges of bilirubin measured by these methods were 1.5–35.9 mg/dL for TSB, and 4.3–33.3 mg/dL and 1.0–33.7 mg/dL for TcBF and TcBS, respectively. The TcBF method over-estimated a higher proportion 73 (32.9%) of neonates with severe jaundice than the TSB method 28 (12.6%) (χ
2 = 53.86,
p = 0.0001). In addition, there was a significant difference in the mean bilirubin level measured using TcBF (
t = 6.95,
p = 0.000) and TcBS (
t = 4.30,
p = 0.000) compared to TSB. Mean TcBS was also significantly lower compared to TcBF (
t = 2.50,
p = 0.013).
Table 2 shows results of the regression analysis between TSB and TcBF, and TSB and TcBS. A linear regression analysis was done to predict the change in TSB for a unit change in TcBF and TcBS. The TcBF level accounted for 81.6% of the explained variability in TSB while the TcBS level accounted for 83.8% of the explained variability in TSB. From the regression analysis it was found that the TcB level for the forehead or sternum could statistically and significantly predict the TSB level,
F(1, 220) = 980.98,
p = 0.000;
F(1, 220) = 1143.86,
p = 0.000, respectively. We applied the linear regression equation
y = α + β
x for both parameters, where
y = TSB; α (intercept) = (−0.93 and 0.102 respectively); β (coefficient of regression) = 0.84/0.83;
x = TcBF or TcBS.
Therefore, the regression equation is: Predicted TSB = −0.93 + 0.84x (TcBF); Predicted TSB = 0.102 + 0.83x (TcBS).
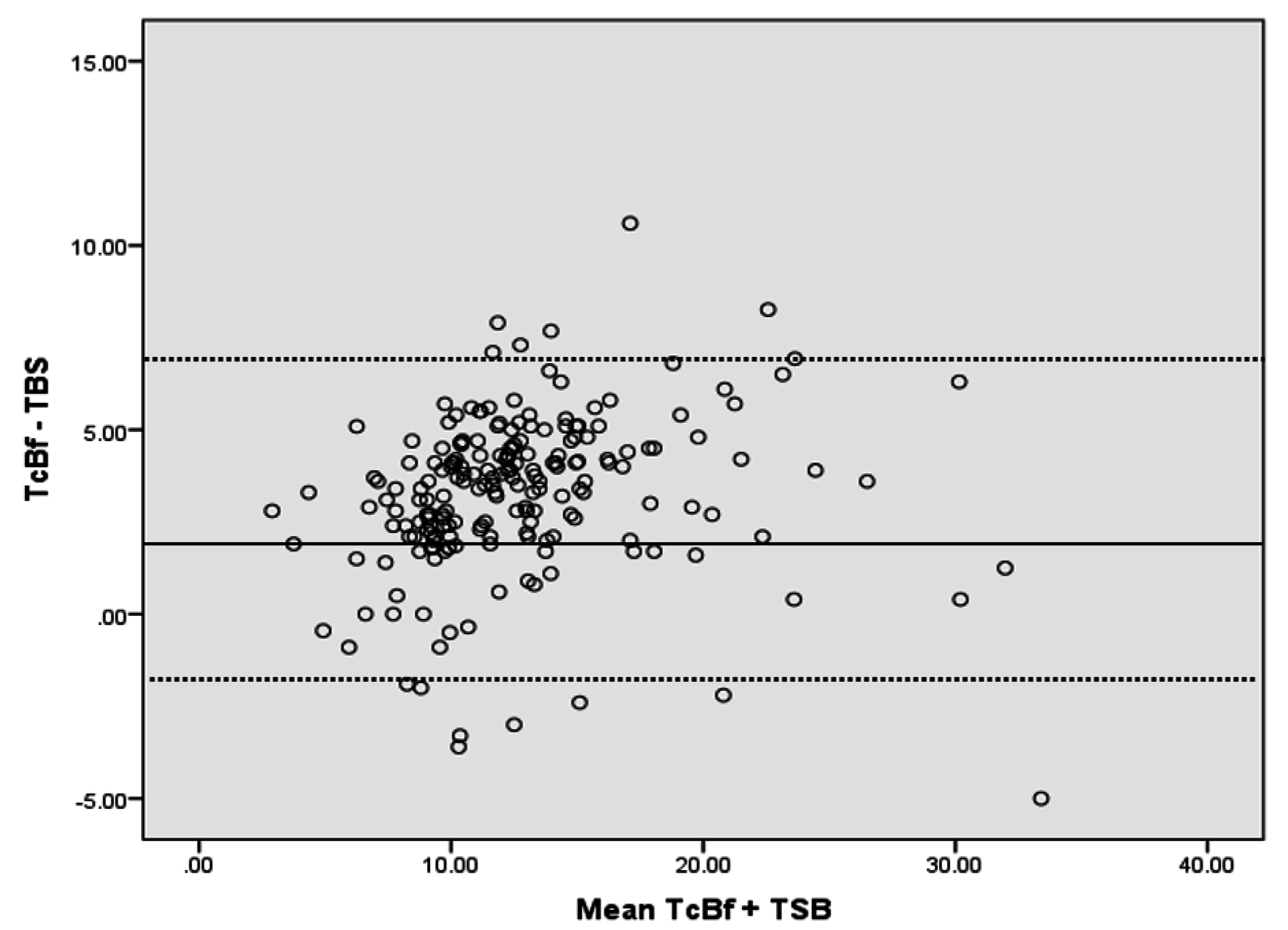
Figure 1 shows a Bland-Altman plot representing the mean difference and limits of agreement of measurement of TSB and TcBF. The mean difference was 3.2 mg/dL (SD = 2.2; CI = −1.1, 7.7). Since the mean difference of 3.2 mg/dL is greater than zero (positive bias), it showed that the TcBF method yielded a higher bilirubin value than the TSB method. It is also noted that 14 of 222 (6%) data points exceeded the limits of agreement; six exceeded the upper limit and eight exceeded the lower limit.
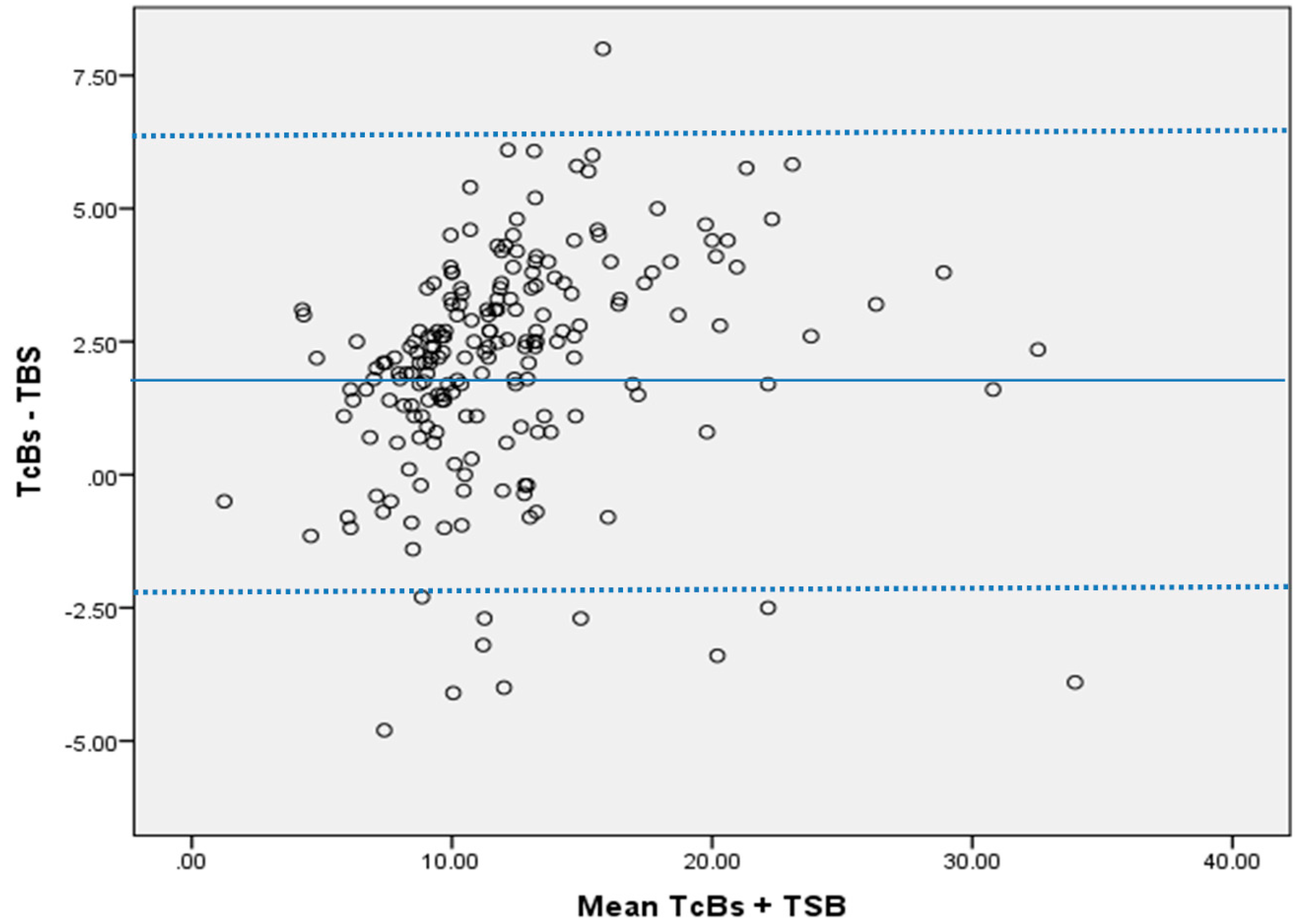
Figure 2 shows a Bland-Altman plot representing the mean difference and limit of agreement of the measurements of TSB and TcBS. The mean difference was 2.0 mg/dL (SD = 2.1; CI = −2.1, 6.3). Since the mean difference is 2.0 mg/dL, which is greater than zero (positive bias), it showed that the TcBS method yielded higher bilirubin values than the TSB method. It is also noted that 10 of 222 (5%) data points exceeded the limits of agreement; one exceeded the upper limit and nine exceeded the lower limit.
4. Discussion
In the evaluation of MBJ20
®, this present study showed that the mean bilirubin concentration determined by the Diazo method was lower. The value for TSB was (10.87 ± 4.66) mg/dL compared to TcBF (14.05 ± 5.00) mg/dL and TcBS (12.92 ± 5.11) mg/dL. This indicated that the transcutaneous bilirubinometric method overestimated the serum bilirubin level. This finding is similar to that of Slusher, Angyo, Bode-Thomas et al. [
5], who demonstrated that the mean bilirubin level of TSB (11.9 ± 6.5) was lower than TcB (13.1 ± 5.5) mg/dL as determined by Bilicheck. Raimondi, Lama, Landolfo and colleagues [
6] found that the mean TSB (9.5 mg/dL) was lower when compared to the mean bilirubin level obtained from three different transcutaneous devices: 9.8 mg/dL by Bilicheck
®, 9.8 mg/dL from JM103
® and 10.4 mg/dL by Bilimed
®. For the reason of inter-laboratory variations [
7,
8] in total serum bilirubin measurements and non-routine use of HPLC, which is the “gold standard” for serum bilirubin measurement, notwithstanding, the reasons for differences in TcB and TSB in various studies are not clear.
The degree of correlation demonstrated by MBJ20
® and the Diazo method in this study was high. A strong positive linear relationship with TSB was observed with the correlation coefficients of 0.904 (TSB and TcB forehead) and 0.917 (TSB and TcB sternum). This correlation coefficient is similar to those obtained from other transcutaneous bilirubinometers. Maisels, Ostrea, Touch and co-workers [
9] evaluated JM103
® and found a correlation of 0.915 between TSB and TcB values estimated on the sternum. Similarly, Slusher, Angyo, Bode-Thomas and their colleagues [
5] who evaluated Bilicheck
® found a correlation of 0.904 and 0.917 for measurements performed on the forehead and sternum, respectively. The present study corroborated the findings of the earlier studies [
5,
9]. Nevertheless the findings of this present study were at variance with the observation by Ajay and Savitha [
10] who evaluated MBJ20
® and got a positive but weak correlation of 0.342 for the measurements obtained from TcBF and the Diazo method. Though Liu, Yang and Zhang [
11] did not make use of the correlation coefficient, their study demonstrated good consistency between MBJ20
®, JM103
® and serum bilirubin estimation by a standard laboratory method. The strong positive relationship from the present study indicates that estimation of the bilirubin level by MBJ20
® was consistent with the corresponding TSB. Therefore, MBJ20
® can serve as a valuable device even in patients with high bilirubin values that may require phototherapy or exchange blood transfusion.
In contradistinction to findings from other studies [
5,
12] that bilirubin estimates from TcB forehead are lower than bilirubin values from TcB sternum, this study found bilirubin levels from TcB forehead to be higher than those of TcB sternum. The reason for this is unclear; however, a possible explanation for this observation could be the cephalocadual progression of jaundice which could make bilirubin values on the forehead be expectedly higher than levels at the sternum.
The Bland-Altman plot which showed that the majority of the measurements fell within a 95% confidence interval, signifying strong agreement between the standard laboratory method and the MBJ20 transcutaneous bilirubinometer, also highlighted that the level of imprecision was great with an overestimation of 3.2 mg/dL for TcBF and 2.0 mg/dL for TcBS. Though similar to the study conducted by Liu,Yang and Zhang [
11], who found a mean difference of 2.5 mg/dL for TcBF and 3.5 mg/dL for TcBS using the same device, this is not in keeping with the recommended guideline of American Academy of Pediatrics (AAP) which allows for a difference of 1 mg/dL between the transcutaneous device and TSB. The clinical implication is that the MBJ20
® cannot totally replace TSB measurements in the evaluation of jaundiced neonates but can only serve as a surrogate.


 ,
, 


{kind=link}
{kind=link}