
Newborn Screening for Primary Immune Deficiencies with a TREC/KREC/ACTB Triplex Assay—A Three-Year Pilot Study in Sweden

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Method
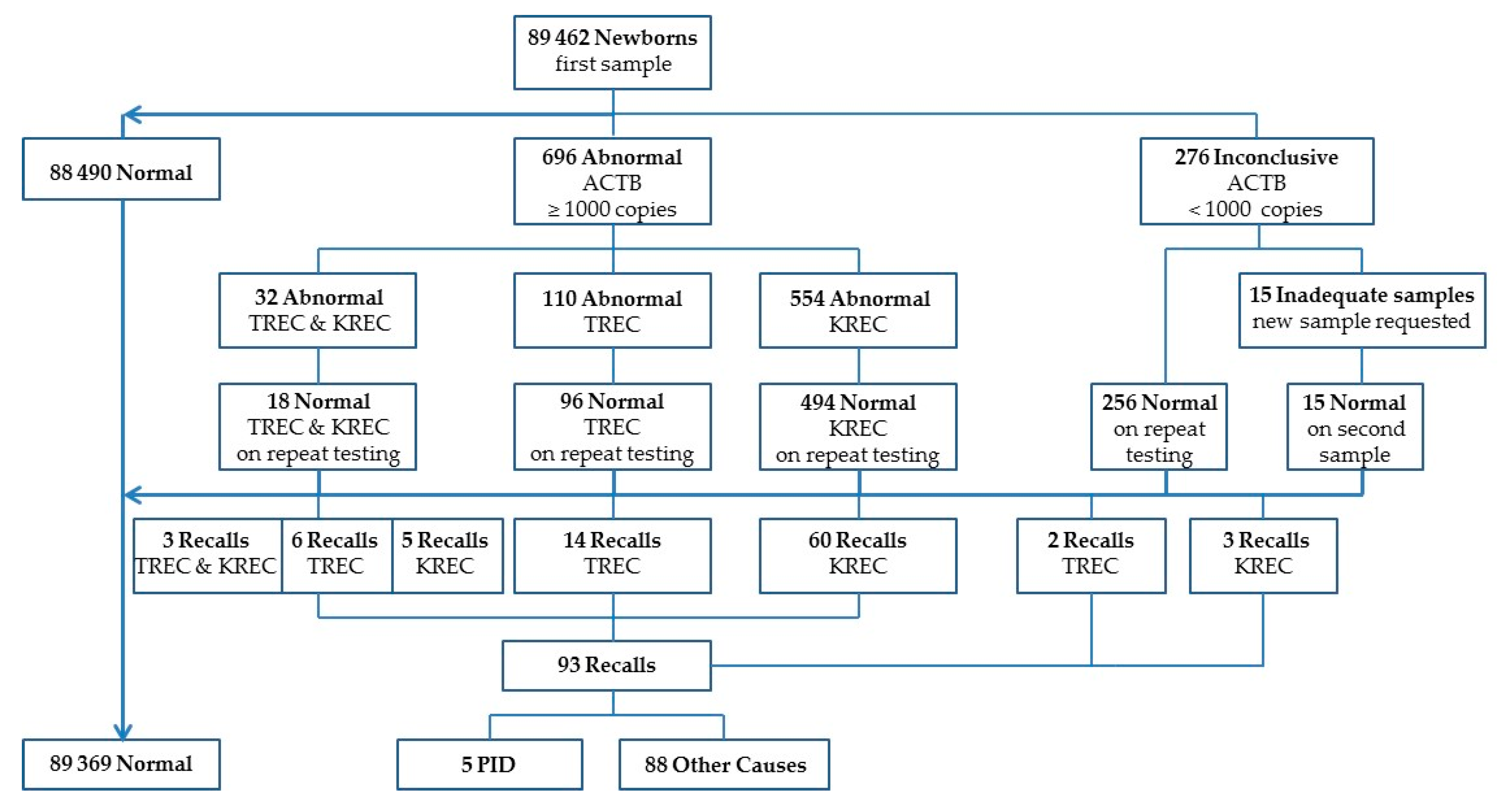
3. Results
3.1. Recalled Patients
3.2. True Positive Patients
3.3. Retrospective Analysis of PID Patients
3.4. Retrospective Analysis of TREC and KREC in Patients with Inborn Errors of Metabolism
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
| Pat | Disorder | Gene 1 | Screening Detected | Comments | TREC Copies | KREC Copies | TREC Recall | KREC Recall |
|---|---|---|---|---|---|---|---|---|
| Cobalamin and Folate Transport and Metabolism Disorders | ||||||||
| 1 | Methylmalonic acidemia, CblA | MMAA | no | Onset at ten months | 184 | 196 | ||
| 2 | Methylmalonic acidemia, CblA | MMAA | yes | 179 | 56 | |||
| 3 | Methylmalonic acidemia, ClbB | MMAB | no | Neonatal onset | 300 | 55 | ||
| 4 | Methylmalonic acidemia and homocystinuria, CblC | MMACHC | no | 167 | 129 | |||
| 5 | Methylmalonic acidemia and homocystinuria, CblC | MMACHC | no | Onset at three months | 64 | 27 | ||
| 6 | Methylmalonic acidemia and homocystinuria, CblC | MMACHC | yes | 61 | 100 | 179 | 181 | |
| 7 | Methylmalonic acidemia and homocystinuria, CblC | MMACHC | yes | 188 | 105 | |||
| 8 | Homocystinuria-megaloblastic anemia, CblG | nd | no | Died at ten months | 33 | 181 | ||
| 9 | Homocystinuria-megaloblastic anemia, CblG | nd | no | Neonatal onset | 76 | 118 | ||
| 10 | Homocystinuria-megaloblastic anemia, CblG | nd | no | 82 | 100 | |||
| 11 | Transcobalamin II deficiency | nd | no | 132 | 147 | |||
| 12 | Homocystinuria due to MTHFR deficiency | MTHFR | 283 | 60 | ||||
| Amino Acid Metabolism | ||||||||
| 13 | Propionic acidemia | PCCB | no | 59 | 47 | |||
| 14 | Propionic acidemia | PCCB | no | Symptoms at day two | 62 | 50 | ||
| 15 | Propionic acidemia | PCCA | yes | Died neonatally | 51 | 4 | ||
| 16 | Propionic acidemia | PCCB | yes | No symptoms | 98 | 157 | 236 | 281 |
| 17 | Propionic acidemia | PCCB | yes | Mild form | 269 | 51 | ||
| 18 | Propionic acidemia | nd | yes | 59 | 11 | 34 | 25 | |
| 19 | Propionic acidemia | PCCA | yes | 220 | 190 | 267 | 91 | |
| 20 | Methylmalonic acidemia due to methylmalonyl-CoA mutase deficiency | MUT | no | 73 | 26 | |||
| 21 | Methylmalonic acidemia due to methylmalonyl-CoA mutase deficiency | MUT | no | Neonatal onset | 44 | 6 | ||
| 22 | Methylmalonic acidemia due to methylmalonyl-CoA mutase deficiency | MUT | no | Neonatal onset | 102 | 42 | ||
| 23 | Methylmalonic acidemia due to methylmalonyl-CoA mutase deficiency | MUT | no | Onset at nine months | 75 | 68 | ||
| 24 | Isovaleric acidemia | nd | no | 197 | 53 | |||
| 25 | Isovaleric acidemia | nd | no | |||||
| 26 | Isovaleric acidemia | IVD | yes | No symptoms | 205 | 151 | 187 | 132 |
| 27 | Isovaleric acidemia | IVD | yes | 187 | 150 | 217 | 145 | |
| 28 | Isovaleric acidemia | IVD | yes | 240 | 55 | 431 | 109 | |
| 29 | Isovaleric acidemia | IVD | yes | 196 | 103 | 127 | 61 | |
| 30 | Lysinuric protein intolerance | nd | no | 81 | 92 | |||
| 31 | Lysinuric protein intolerance | nd | no | 36 | 289 | |||
| Mitochondrial Disorders | ||||||||
| 32 | Pearsons syndrome | mtDNA deletion | no | Anemia | 58 | 50 | ||
| 33 | Pearsons syndrome | mtDNA deletion | no | Anemia | 132 | 148 | ||
| 34 | Pearsons syndrome | mtDNA deletion | no | 28 | 12 | |||
| 35 | Leigh syndrome | MTND1 | no | Anemia | 20 | 14 | ||
| 36 | Leigh syndrome | MTND3 | no | 172 | 163 | |||
| 37 | Leigh syndrome | MTND3 | no | 113 | 93 | |||
| 38 | Leigh syndrome | MTND3 | no | 70 | 75 | |||
| 39 | Leigh syndrome | MTND5 | no | Frequent infections | 72 | 77 | ||
| 40 | Leigh syndrome | MTND6 | no | 226 | 78 | |||
| 41 | Leigh syndrome | MTATP6 | no | 100 | 220 | |||
| 42 | Leigh syndrome | MTATP6 | no | 89 | 107 | |||
| 43 | Leigh syndrome | NDUFAF2 | no | 265 | 121 | |||
| 44 | Alpers syndrome | POLG | no | Frequent infections | 208 | 108 | ||
| 45 | Alpers syndrome | POLG | no | 215 | 238 | |||
| 46 | Alpers syndrome | POLG | no | Frequent infections., low IgG, IgA, IgM | 85 | 16 | ||
| 47 | mtDNA depletion syndrome | TK2 | no | 105 | 33 | |||
| 48 | mtDNA depletion syndrome | MPV17 | no | 119 | 108 | |||
| 49 | Mitochondrial encephalopathy | COX10 | no | Anemia, multi organ involvment | 24 | 87 | ||
| 50 | Leigh syndrome | SERAC1 | no | Frequent infections | 3 | 285 | ||
| 51 | Leigh syndrome | SERAC1 | no | 110 | 105 | |||
| 52* | Mitochondrial encephalopathy | SERAC1 | no | 112 | 161 | |||
| 53* | Mitochondrial encephalopathy | SERAC1 | no | 70 | 60 | |||
| 54 | Leigh syndrome | SERAC1 | no | 191 | 61 | |||
| 55 | Mitochondrial encephalomyopathy | nd | no | 11 | 91 | |||
| Galactosemia | ||||||||
| 56 | Galactosemia | GALT | yes | 102 | 61 | 139 | 133 | |
| 57 | Galactosemia | GALT | yes | 158 | 100 | 182 | 172 | |
| 58 | Galactosemia | GALT | yes | 208 | 76 | 110 | 49 | |
| 59 | Galactosemia | GALT | yes | 56 | 128 | 119 | 197 | |
| 60 | Galactosemia | GALT | yes | 163 | 89 | 228 | 129 | |
| 61 | Galactosemia | GALT | yes | 240 | 104 | 155 | 113 | |
| 62 | Galactosemia | GALT | yes | 412 | 45 | |||
| 63 | Galactosemia | GALT | yes | 169 | 115 | 321 | 261 | |
| Disorders of Nucleic Acid Metabolism | ||||||||
| 64 | Arts syndrome | PRPS1 | no | 93 | 51 | |||
| Congenital Disorders of Glycosylation | ||||||||
| 65 | Congenital disorder of glycosylation, type Ia | ALG13 | no | 330 | 118 | |||
| Lysosomal Storage Disorders | ||||||||
| 66 | Gaucher disease | GBA | no | 123 | 424 | |||
| 67 | Gaucher disease | GBA | no | 302 | 99 | |||
| 68 | Gaucher disease | GBA | no | 229 | 113 | |||
| 69 | Aspartyl glucosaminuria | AGA | no | 246 | 64 | |||
References
- Guthrie, R.; Susi, A. A simple phenylalanine method for detecting phenylketonuria in large populations of newborn infants. Pediatrics 1963, 32, 338–343. [Google Scholar] [PubMed]
- PKU-provet—Karolinska Universitetssjukhuset. Available online: http://www.karolinska.se/PKU (accessed on 14 May 2017).
- Wilson, J.M.G.; Jungner, G. Principles and Practice of Screening for Disease. Available online: http://apps.who.int/iris/bitstream/10665/37650/17/WHO_PHP_34.pdf (accessed on 11 May 2017).
- Andermann, A.; Blancquaert, I.; Beauchamp, S.; Déry, V. Revisiting Wilson and Jungner in the genomic age: A review of screening criteria over the past 40 years. Bull. World Health Org. 2008, 86, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Nationella screeningprogram—modell för bedömning, införande och uppföljning. Available online: http://www.socialstyrelsen.se/publikationer2014/2014-2-16 (accessed on 14 May 2017).
- Al-Herz, W.; Bousfiha, A.; Casanove, J.-L.; Chatila, T.; Conley, M.E.; Cunningham-Rundles, C.; Etzioni, A.; France, J.L.; Gaspar, H.B.; Holland, S.M.; et al. Primary immunodeficiency diseases: An update on the classification from the international union of immunological societies expert committee for primary immunodeficiency. Proc. ICI Milan 2014, 5, 162. [Google Scholar]
- Chan, K.; Puck, J.M. Development of population-based newborn screening for severe combined immunodeficiency. J. Allergy Clin. Immunol. 2005, 115, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Verbsky, J.W.; Chatila, T.A. T-regulatory cells in primary immune deficiencies. Curr. Opin. Allergy Clin. Immunol. 2011, 11, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Kwan, A.; Church, J.A.; Cowan, M.J.; Agarwal, R.; Kapoor, N.; Kohn, D.B.; Lewis, D.B.; McGhee, S.A.; Moore, T.B.; Porteus, M.; et al. Newborn screening for severe combined immunodeficiency and T-cell lymphopenia in California: Results of the first 2 years. J. Allergy Clin. Immunol. 2013, 132, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Therrell, B.L.; Padilla, C.D.; Loeber, J.G.; Kneisser, I.; Saadallah, A.; Borrajo, G.J.; Adams, J. Current status of newborn screening worldwide: 2015. Semin. Perinatol. 2015, 39, 171–187. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, N.; Imai, K.; Kanegane, H.; Sato, H.; Yamada, M.; Kondoh, K.; Okada, S.; Kobayashi, M.; Agematsu, K.; Takada, H.; et al. Quantification of κ-deleting recombination excision circles in Guthrie cards for the identification of early B-cell maturation defects. J. Allergy Clin. Immunol. 2011, 128, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Borte, S.; von Döbeln, U.; Fasth, A.; Wang, N.; Janzi, M.; Winiarski, J.; Sack, U.; Pan-Hammarström, Q.; Borte, M.; Hammarström, L. Neonatal screening for severe primary immunodeficiency diseases using high-throughput triplex real-time PCR. Blood 2012, 119, 2552–2555. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, M.; Ohlsson, A.; Borte, S.; Jonsson, S.; Zetterström, R.H.; King, J.; Winiarski, J.; von Döbeln, U.; Hammarström, L. Newborn Screening for Severe Primary Immunodeficiency Diseases in Sweden—A 2-Year Pilot TREC and KREC Screening Study. J. Clin. Immunol. 2017, 37, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Yokota, M.; Tatsumi, N.; Nathalang, O.; Yamada, T.; Tsuda, I. Effects of heparin on polymerase chain reaction for blood white cells. J. Clin. Lab. Anal. 1999, 13, 133–140. [Google Scholar] [CrossRef]
- Holodniy, M.; Kim, S.; Katzenstein, D.; Konrad, M.; Groves, E.; Merigan, T.C. Inhibition of human immunodeficiency virus gene amplification by heparin. J. Clin. Microbiol. 1991, 29, 676–679. [Google Scholar] [PubMed]
- Routes, J.M.; Grossman, W.J.; Verbsky, J.; Laessig, R.H.; Hoffman, G.L.; Brokopp, C.D.; Baker, M.W. Statewide newborn screening for severe T-cell lymphopenia. Jama 2009, 302, 2465–2470. [Google Scholar] [CrossRef] [PubMed]
- Kwan, A.; Abraham, R.S.; Currier, R.; Brower, A.; Andruszewski, K.; Abbott, J.K.; Baker, M.; Ballow, M.; Bartoshesky, L.E.; Bonagura, V.R.; Bonilla, F.A. Newborn screening for severe combined immunodeficiency in 11 screening programs in the United States. Jama 2014, 312, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Buelow, B.J.; Verbsky, J.W.; Routes, J.M. Newborn screening for SCID: Lessons learned. Expert Rev. Hematol. 2016, 9, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Felipe, B.; Olbrich, P.; Lucenas, J.M.; Delgado-Pecellin, C.; Pavon-Delgado, A.; Marquez, J.; Salamanca, C.; Soler-Palacin, P.; Gonzalez-Granado, L.I.; Antolin, L.F.; et al. Prospective neonatal screening for severe T- and B-lymphocyte deficiencies in Seville. Pediatric Allergy Immunol. 2016, 27, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Verbsky, J.W.; Baker, M.W.; Grossman, W.J.; Hintermeyer, M.; Dasu, T.; Bonacci, B.; Reddy, S.; Margolis, D.; Casper, J.; Gries, M.; DeSantes, K. Newborn screening for severe combined immunodeficiency; the Wisconsin experience (2008–2011). J. Clin. Immunol. 2012, 32, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.Y.; Garcia-Lloret, M.I.; Slev, P.; Bohnsack, J.F.; Chen, K. Profound T-cell lymphopenia associated with prenatal exposure to purine antagonists detected by TREC newborn screening. J. Allergy Clin. Immunol. Practice 2017, 5, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Parvaneh, N.; Quartier, P.; Rostami, P.; Casanova, J.L.; de Lonlay, P. Inborn errors of metabolism underlying primary immunodeficiencies. J. Clin. Immunol. 2014, 34, 753–771. [Google Scholar] [CrossRef] [PubMed]
- Ozand, P.T.; Gascon, G.G. Topical Review Article: Organic Acidurias: A Review. Part 1. J. Child Neurol. 1991, 6, 196–219. [Google Scholar] [CrossRef] [PubMed]
- Waggoner, D.; Buist, N.; Donnell, G. Long-term prognosis in galactosaemia: Results of a survey of 350 cases. J. Inherit. Metab. Dis. 1990, 13, 802–818. [Google Scholar] [CrossRef] [PubMed]
- Muraki, K.; Nishimura, S.; Goto, Y.; Nonaka, I.; Sakura, N.; Ueda, K. The association between haematological manifestation and mtDNA deletions in Pearson syndrome. J. Inherit. Metab. Dis. 1997, 20, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Reichenbach, J.; Schubert, R.; Horvàth, R.; Petersen, J.; Fütterer, N.; Malle, E.; Stumpf, A.; Gebhardt, B.R.; Koehl, U.; Schraven, B.; Zielen, S. Fatal neonatal-onset mitochondrial respiratory chain disease with T cell immunodeficiency. Pediatric Res. 2006, 60, 321–326. [Google Scholar] [CrossRef] [PubMed]

| Period | Screened Infants | Recall Values | Number of Recalls | |||
|---|---|---|---|---|---|---|
| TREC * | KREC * | TREC | KREC | TREC/KREC | ||
| 1 | 16,582 | 15 | 10 | 6 | 29 | 0 |
| 2 | 28,298 | 8 | 4 | 3 | 7 | 1 |
| 3 | 44,582 | 10 | 6 | 13 | 32 | 2 |
| Total | 89,462 | - | - | 22 ** | 68 | 3 *** |
| Pat | Gender | Weeks | Grams | TREC * | KREC * | Phenotype | Genetic Diagnosis |
|---|---|---|---|---|---|---|---|
| 1 | M | 34 | 1800 | 0 | 0 | SCID | Artemis deficiency |
| 2 | M | 39 | 3110 | 5 | 7 | CID | Ataxia Telangiectasia |
| 3 | M | 36 | 2770 | 7 | 205 | CID | Unknown |
| 4 | M | 38 | 3250 | 0 | 0 | SCID | ADA deficiency |
| 5 | M | 40 | 3445 | 8 | 180 | CID | Unknown |
| Pat | Gender | Weeks | Grams | TREC * | KREC * | Phenotype | Genetic Diagnosis |
|---|---|---|---|---|---|---|---|
| 1 | M | 38 | 2875 | 48 | 0 | Agammaglobulinemia | nd |
| 2 | F | 41 | 3185 | 0 | 0 | SCID | Artemis deficiency |
| 3 | M | 39 | 3200 | 0 | 86 | SCID | IL2RG |
| 4 | M | 35 | un | 7 | 17 | Severe lymphopenia | UBE2A ** |
| 5 | M | 41 | 3500 | 0 | 0 | SCID | Artemis deficiency |
| 6 | F | 41 | 3655 | 0 | 0 | SCID | RAG1 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zetterström, R.H.; Barbaro, M.; Ohlsson, A.; Borte, S.; Jonsson, S.; Winiarski, J.; Von Döbeln, U.; Hammarström, L. Newborn Screening for Primary Immune Deficiencies with a TREC/KREC/ACTB Triplex Assay—A Three-Year Pilot Study in Sweden. Int. J. Neonatal Screen. 2017, 3, 11. https://doi.org/10.3390/ijns3020011
Zetterström RH, Barbaro M, Ohlsson A, Borte S, Jonsson S, Winiarski J, Von Döbeln U, Hammarström L. Newborn Screening for Primary Immune Deficiencies with a TREC/KREC/ACTB Triplex Assay—A Three-Year Pilot Study in Sweden. International Journal of Neonatal Screening. 2017; 3(2):11. https://doi.org/10.3390/ijns3020011
Chicago/Turabian StyleZetterström, Rolf H., Michela Barbaro, Annika Ohlsson, Stephan Borte, Susanne Jonsson, Jacek Winiarski, Ulrika Von Döbeln, and Lennart Hammarström. 2017. "Newborn Screening for Primary Immune Deficiencies with a TREC/KREC/ACTB Triplex Assay—A Three-Year Pilot Study in Sweden" International Journal of Neonatal Screening 3, no. 2: 11. https://doi.org/10.3390/ijns3020011