Early Detection and Diagnosis of Neonatal Intrahepatic Cholestasis Caused by Citrin Deficiency Missed by Newborn Screening Using Tandem Mass Spectrometry

Abstract
:1. Introduction
2. Materials and Methods
2.1. Newborn Screening Program
2.2. Patients
2.3. Mutation Analysis
2.4. Statistical Analysis
2.5. Ethics
3. Results
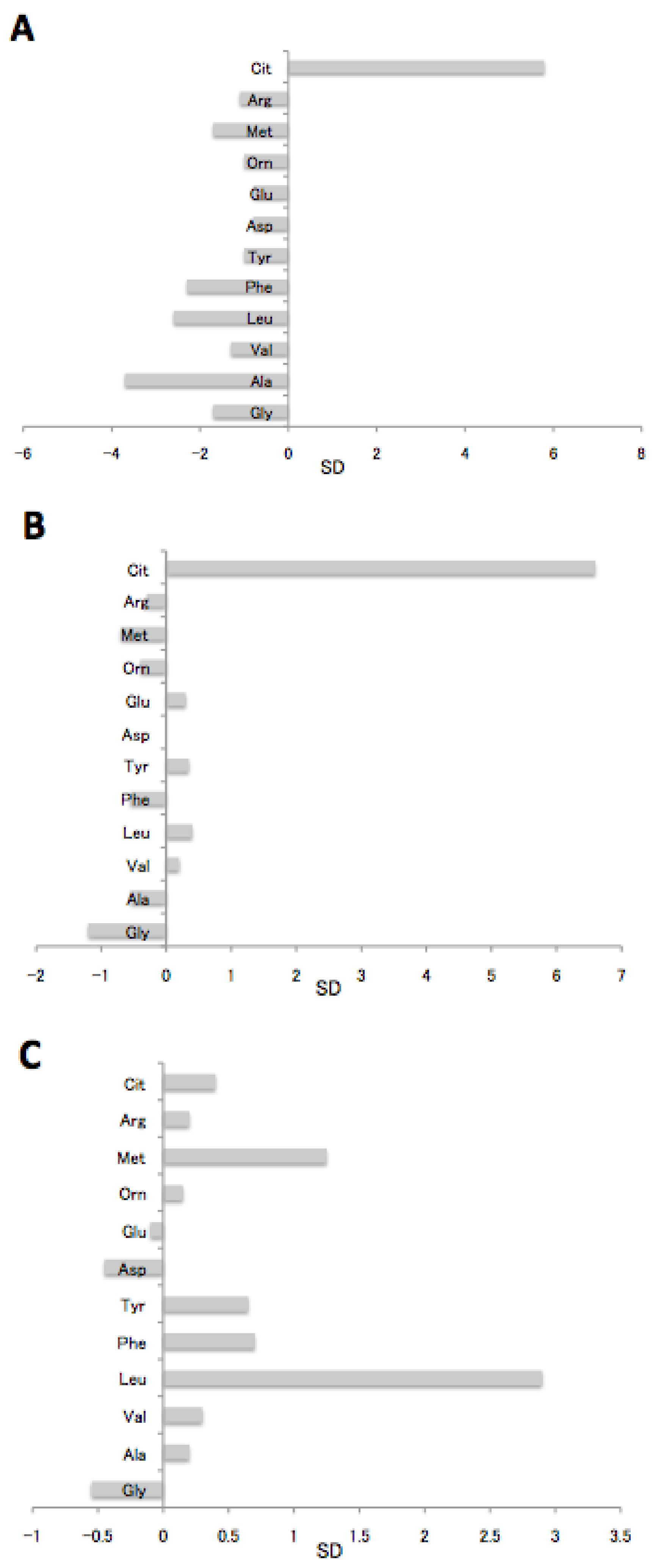
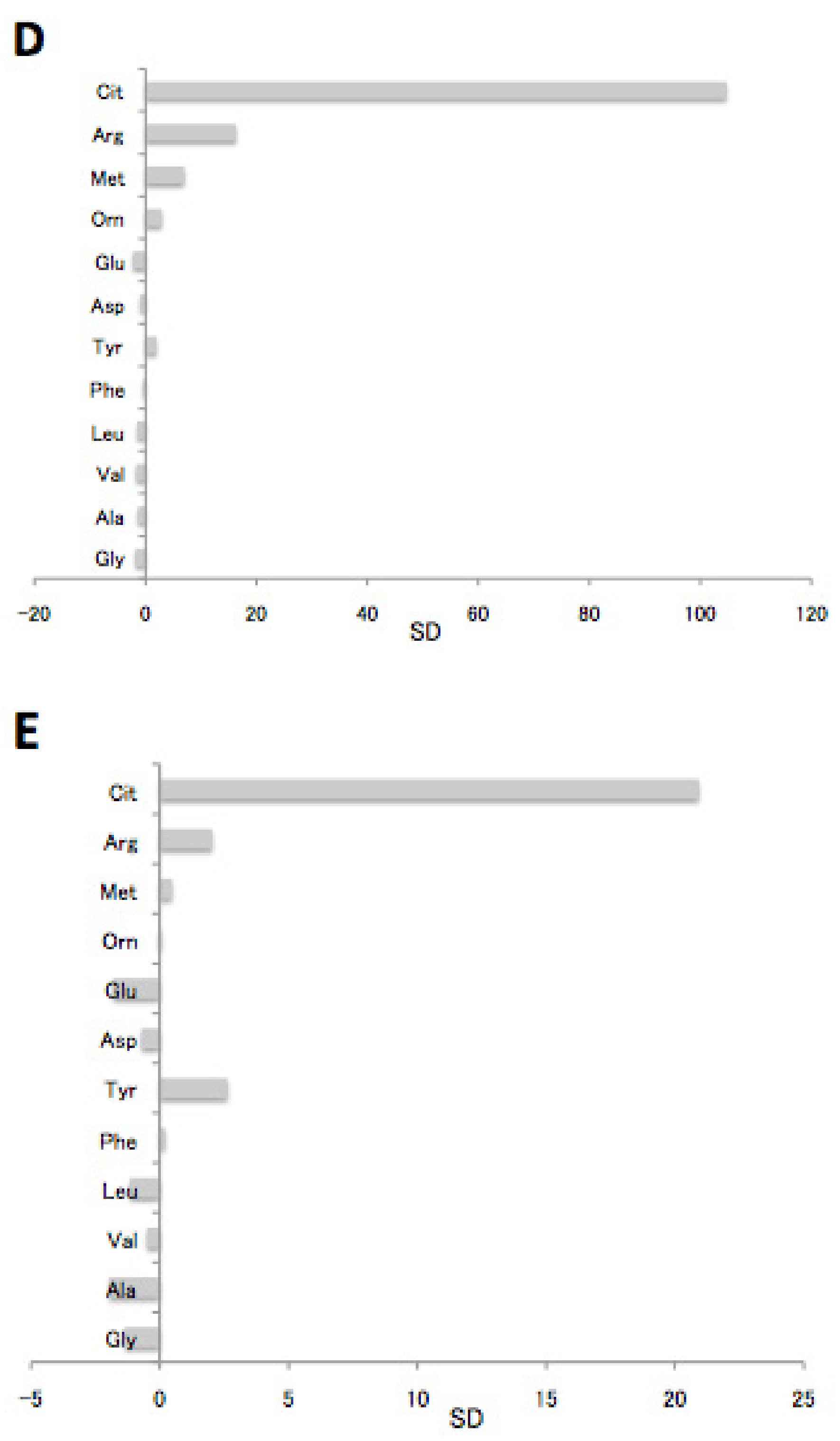
3.1. Amino Acid Analysis at Initial Screening
3.2. Screening for Citrin Deficiency Based on Citrulline Values and Relative Increases
3.3. Estimated NICCD Index
3.4. Mutation Spectrum of Patients with NICCD
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kobayashi, K.; Sinasac, D.S.; Iijima, M.; Boright, A.P.; Begum, L.; Lee, J.R.; Yasuda, T.; Ikeda, S.; Hirano, R.; Terazono, H.; et al. The gene mutated in adult-onset type II citrullinaemia encodes a putative mitochondrial carrier protein. Nat. Genet. 1999, 22, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Tazawa, Y.; Kobayashi, K.; Ohura, T.; Abukawa, D.; Nishinomiya, F.; Hosoda, Y.; Yamashita, M.; Nagata, I.; Kono, Y.; Yasuda, T.; et al. Infantile cholestatic jaundice associated with adult-onset type II citrullinemia. J. Pediatr. 2001, 138, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Tomomasa, T.; Kobayashi, K.; Kaneko, H.; Shimura, H.; Fukusato, T.; Tabata, M.; Inoue, Y.; Ohwada, S.; Kasahara, M.; Morishita, Y.; et al. Possible clinical and histologic manifestations of adult-onset type II citrullinemia in early infancy. J. Pediatr. 2001, 138, 741–743. [Google Scholar] [CrossRef] [PubMed]
- Ohura, T.; Kobayashi, K.; Tazawa, Y.; Nishi, I.; Abukawa, D.; Sakamoto, O.; Iinuma, K.; Saheki, T. Neonatal presentation of adult-onset type II citrullinemia. Hum. Genet. 2001, 108, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Saheki, T.; Kobayashi, K. Mitochondrial aspartate glutamate carrier (citrin) deficiency as the cause of adult-onset type II citrullinemia (CTLN2) and idiopathic neonatal hepatitis (NICCD). J. Hum. Genet. 2002, 47, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Yamaguchi, N.; Kobayashi, K.; Nishi, I.; Horinouchi, H.; Jalil, M.A.; Li, M.X.; Ushikai, M.; Iijima, M.; Kondo, I.; et al. Identification of two novel mutations in the SLC25A13 gene and detection of seven mutations in 102 patients with adult-onset type II citrullinemia. Hum. Genet. 2000, 107, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, N.; Kobayashi, K.; Yasuda, T.; Nishi, I.; Iijima, M.; Nakagawa, M.; Osame, M.; Kondo, I.; Saheki, T. Screening of SLC25A13 mutations in early and late onset patients with citrin deficiency and in the Japanese population: Identification of two novel mutations and establishment of multiple DNA diagnosis methods for nine mutations. Hum. Mutat. 2002, 19, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Tabata, A.; Sheng, J.-S.; Ushikai, M.; Song, Y.-Z.; Gao, H.-Z.; Lu, Y.-B.; Okamura, F.; Iijima, M.; Mutoh, M.; Kishida, S.; et al. Identification of 13 novel mutations including a retrotransposal insertion in SLC25A13 gene and frequency of 30 mutations found in patients with citrin deficiency. J. Hum. Genet. 2008, 53, 534–545. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.-Z.; Guo, L.; Yang, Y.-L.; Han, L.-S.; Kobayashi, K.; Saheki, T. Failure to thrive and dyslipidemia caused by citrin deficiency. A novel clinical phenotype. Chin. J. Contemp. Pediatr. 2009, 11, 328–332. [Google Scholar]
- Ikeda, S.; Yazaki, M.; Takei, Y.; Ikegami, T.; Kawasaki, S.; Iwai, M.; Kobayashi, K.; Saheki, T. Type II (adult onset) citrullinemia: Clinical pictures and the therapeutic effect of liver transplantation. J. Neurol. Neurosurg. Psychiatry 2001, 71, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, M.; Yazaki, M.; Tanaka, N.; Sano, K.; Hashimoto, E.; Takei, Y.; Song, Y.-Z.; Tanaka, E.; Kiyosawa, K.; Saheki, T.; et al. Citrin deficiency as a cause of chronic liver disorder mimicking non-alcoholic fatty liver disease. J. Hepatol. 2008, 49, 810–820. [Google Scholar] [CrossRef] [PubMed]
- Saheki, T.; Inoue, K.; Tushima, A.; Mutoh, K.; Kobayashi, K. Citrin deficiency and current treatment concepts. Mol. Genet. Metab. 2010, 100 (Suppl. 1), S59–S64. [Google Scholar] [CrossRef] [PubMed]
- Naito, E.; Ito, M.; Matsuura, S.; Yokota, I.; Saijo, T.; Ogawa, Y.; Kitamura, S.; Kobayashi, K.; Saheki, T.; Nishimura, Y.; et al. Type II citrullinaemia (citrin deficiency) in a neonate with hypergalactosaemia detected by mass screening. J. Inherit. Metab. Dis. 2002, 25, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Ohura, T.; Kobayashi, K.; Tazawa, Y.; Abukawa, D.; Sakamoto, O.; Tsuchiya, S.; Saheki, T. Clinical pictures of 75 patients with neonatal intrahepatic cholestasis caused by citrin deficiency (NICCD). J. Inherit. Metab. Dis. 2007, 30, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Tamamori, A.; Fujimoto, A.; Okano, Y.; Kobayashi, K.; Saheki, T.; Tagami, Y.; Takei, H.; Shigematsu, Y.; Hata, I.; Ozaki, H.; et al. Effects of Citrin Deficiency in the Perinatal Period: Feasibility of Newborn Mass Screening for Citrin Deficiency. Pediatr. Res. 2004, 56, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, A.; Arai-Ichinoi, N.; Sakamoto, O.; Matsubara, Y.; Saheki, T.; Kobayashi, K.; Ohura, T.; Kure, S. Simple and rapid genetic testing for citrin deficiency by screening 11 prevalent mutations in SLC25A13. Mol. Genet. Metab. 2012, 105, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Ohura, T.; Kobayashi, K.; Abukawa, D.; Tazawa, T.; Aikawa, J.; Salamoto, O.; Saheki, T.; Imamura, K. A novel inborn error of metabolism detected by elevated methionine and/or galactose in newborn screening: Neonatal intrahepatic cholestasis caused by citrin deficiency. Eur. J. Pediatr. 2003, 162, 317–322. [Google Scholar] [PubMed]
- Shigematsu, Y.; Hirano, S.; Hata, Y.; Tanaka, M.; Sudo, M.; Sakura, N.; Tajima, T.; Yamaguchi, S. Newborn mass screening and selective screening using electrospray tandem mass spectrometry in Japan. J. Chromatogr. B 2002, 776, 39–48. [Google Scholar] [CrossRef]
- Wang, L.Y.; Chen, N.I.; Chen, P.W.; Chiang, S.C.; Hwu, W.L.; Lee, N.C.; Chien, Y.H. Newborn screening for citrin deficiency and carnitine uptake defect using second-tier molecular tests. BMC Med. Genet. 2013, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.B.; Kobayashi, K.; Ushikai, M.; Tabata, A.; Iijima, M.; Li, M.X.; Lei, L.; Kawabe, K.; Taura, S.; Yang, Y.; et al. Frequency and distribution in East Asia of 12 mutations identified in the SLC25A13 gene of Japanese patients with citrin deficiency. J. Hum. Genet. 2005, 50, 338–346. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient No. | Sex | Cit (nmol/mL) * | Onset (Month) | Allele 1 | Allele 2 | Initial Symptoms |
|---|---|---|---|---|---|---|
| 1 | F | 19.4 | 3 | IVS11+1G>A | IVS13+1G>A | Poor weight gain, icterus, white stool, developmental delay |
| 2 | F | 29.2 | 1 | IVS11+1G>A | S225X | Poor weight gain, icterus, white stool |
| 3 | M | 31.1 | 1 | IVS11+1G>A | IVS11+1G>A | Icterus, white stool |
| 4 | M | 23.2 | 4 | 851del4 | IVS11+1G>A | Icterus, hepatomegaly |
| 5 | F | 29 | 4 | IVS11+1G>A | Y504C | Hepatomegaly |
| 6 | M | 26.8 | 1 | 851del4 | IVS11+1G>A | Icterus, anemia |
| 7 | M | 18.9 | 1 | 851del4 | IVS11+1G>A | Poor weight gain, icterus, white stool |
| 8 | F | 26 | 1 | IVS11+1G>A | IVS11+1G>A | Poor weight gain |
| 9 | M | 13 | 1 | IVS11+1G>A | E601X | Poor weight gain, icterus |
| 10 | M | 29.7 | 2 | 851del4 | 851del4 | White stool |
| 11 | M | 12.6 | 4 | IVS11+1G>A | IVS11+1G>A | Poor weight gain, icterus |
| 12 | F | 19.7 | 2 | 851del4 | IVS13+1G>A | Icterus |
| 13 | M | 74.5 | 0 (NBS+) | 851del4 | IVS11+1G>A | None |
| AA (nmol/mL) | NICCD (n = 12) | Neonatal Population | p a | |||
|---|---|---|---|---|---|---|
| (n = 16,360) | ||||||
| Mean | SD | Range | Mean | SD | ||
| Glycine | 324.1 | 125.8 | 170.3–644 | 362.3 | 107.3 | 0.581 |
| Alanine | 282.7 | 118.1 | 123–508 | 280.8 | 82.7 | 0.938 |
| Valine | 102.7 | 33.4 | 56.5–140.6 | 108 | 27.1 | 0.497 |
| Leucine+Isoleucine | 193.2 | 62.9 | 97.6–294.6 | 182.8 | 35.2 | 0.281 |
| Phenylalanine | 46.9 | 10.5 | 29.5–70.8 | 48.1 | 8.9 | 0.64 |
| Tyrosine | 129.4 | 51.2 | 59.4–233.3 | 103.4 | 37.3 | 0.016 |
| Aspartic acid | 53.2 | 19.7 | 26.8–83.5 | 41.7 | 17.3 | 0.021 |
| Glutamic acid | 352.2 | 90.8 | 239.9–519.5 | 296.5 | 60.9 | 0.001 |
| Ornithine | 119.5 | 51.8 | 56.3–231.8 | 109.9 | 43.3 | 0.443 |
| Methionine | 17.7 | 5.3 | 11.6–28.2 | 21.5 | 4.5 | 0.004 |
| Arginine | 14.8 | 6.6 | 7.7–25.9 | 12.6 | 5.6 | 0.173 |
| Citrulline | 23.2 | 6.4 | 12.6–31.1 | 11.7 | 3 | <0.001 |
| Marker | NICCD (n = 12) | Controls (n = 16360) | p * | |||
|---|---|---|---|---|---|---|
| Mean | SD | Range | Mean | SD | ||
| tAA | 1667 | 464 | 990–2686 | 1587 | 308 | 0.18 |
| Cit/tAA | 0.015 | 0.006 | 0.008–0.029 | 0.007 | 0.001 | <0.001 |
| Patient | Cit (nmol/mL) | Cit/tAA | Score |
|---|---|---|---|
| 1 | 19.4 | 0.009 | 0 |
| 2 | 29.2 | 0.029 | 3 |
| 3 | 31.1 | 0.021 | 3 |
| 4 | 23.2 | 0.015 | 1 |
| 5 | 29 | 0.011 | 3 |
| 6 | 26.8 | 0.016 | 3 |
| 7 | 18.9 | 0.018 | 1 |
| 8 | 26 | 0.015 | 1 |
| 9 | 13 | 0.008 | 0 |
| 10 | 29.7 | 0.015 | 3 |
| 11 | 12.6 | 0.011 | 1 |
| 12 | 19.7 | 0.011 | 1 |
| 13 (NBS+) | 74.5 | 0.059 | 4 |
| Cit (Screening Cutoff) | Cit | Cit/tAA | |
| Cutoff | 40 (+9.4 SD) | 26.7 (+5 SD) | 0.01 (+3 SD) |
| Score | 3 | 2 | 1 |
| Judgement | Definitive | 4 | |
| Probable | 3 | ||
| Possible | 1–2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shigetomi, H.; Tanaka, T.; Nagao, M.; Tsutsumi, H. Early Detection and Diagnosis of Neonatal Intrahepatic Cholestasis Caused by Citrin Deficiency Missed by Newborn Screening Using Tandem Mass Spectrometry. Int. J. Neonatal Screen. 2018, 4, 5. https://doi.org/10.3390/ijns4010005
Shigetomi H, Tanaka T, Nagao M, Tsutsumi H. Early Detection and Diagnosis of Neonatal Intrahepatic Cholestasis Caused by Citrin Deficiency Missed by Newborn Screening Using Tandem Mass Spectrometry. International Journal of Neonatal Screening. 2018; 4(1):5. https://doi.org/10.3390/ijns4010005
Chicago/Turabian StyleShigetomi, Hiroko, Toju Tanaka, Masayoshi Nagao, and Hiroyuki Tsutsumi. 2018. "Early Detection and Diagnosis of Neonatal Intrahepatic Cholestasis Caused by Citrin Deficiency Missed by Newborn Screening Using Tandem Mass Spectrometry" International Journal of Neonatal Screening 4, no. 1: 5. https://doi.org/10.3390/ijns4010005
APA StyleShigetomi, H., Tanaka, T., Nagao, M., & Tsutsumi, H. (2018). Early Detection and Diagnosis of Neonatal Intrahepatic Cholestasis Caused by Citrin Deficiency Missed by Newborn Screening Using Tandem Mass Spectrometry. International Journal of Neonatal Screening, 4(1), 5. https://doi.org/10.3390/ijns4010005