
Neonatal Jaundice Detection Using a Computer Vision System



1
Department of Medical Instrumentation Techniques Engineering, Electrical Engineering Technical College, Middle Technical University, Baghdad 10022, Iraq
2
UniSA STEM, University of South Australia, Mawson Lakes, SA 5095, Australia
3
Medical Laboratory Technology, College of Health and Medical Technology, Middle Technical University, Baghdad 10022, Iraq
4
Informatics and Telecommunication Public Company, Ministry of Communication, Baghdad 10022, Iraq
5
Joint and Operations Analysis Division, Defence Science and Technology Group, Melbourne, VIC 3207, Australia
*
Author to whom correspondence should be addressed.
Designs 2021, 5(4), 63; https://doi.org/10.3390/designs5040063
Submission received: 20 September 2021
/
Revised: 29 September 2021
/
Accepted: 29 September 2021
/
Published: 8 October 2021
(This article belongs to the Section Bioengineering Design)
Abstract
:Jaundice or Hyperbilirubinemia is a very common condition that affects newborns in their first few weeks of life. The main cause of jaundice is the high level of the bilirubin substance in the blood. As bilirubin is toxic to brain cells, acute bilirubin encephalopathy can occur in cases of extreme jaundice. This condition can result in brain trauma and lead to kernicterus, which causes repetitive and uncontrolled movements, a permanent upward look, and hearing loss. Thus, a timely diagnosis and treatment can help in preventing long-term damage. In this paper, a developed system based on a digital camera was proposed to diagnose and treat jaundice in newborns. The system detects jaundice and determines if the neonate needs treatment based on the analysis obtained from the real-time captured images. The treatment was achieved by using an Arduino Uno microcontroller to drive phototherapy lighting, which has proven to be an efficient treatment method for jaundice. In addition, the proposed system has the ability to send the diagnostic results to the mobile phone of the care provider. The obtained results from 20 infants inside the intensive care unit showed that the proposed system was accurate in terms of detecting jaundice, easy to implement, and affordable.
1. Introduction
The yellow discoloration of a newborn’s skin and eyes is known as infant jaundice. Infant jaundice is a common issue, particularly in premature babies and those who are breastfed [1]. It usually happens when the baby’s liver is not mature enough to get rid of the extra bilirubin in the bloodstream. In addition, baby jaundice may sometimes be caused by an underlying disease [2].
In 2010, the inability to treat jaundice resulted in 114,000 avoidable infant deaths. Moreover, 75,000 children around the world are suffering from brain dysfunction due to jaundice complications. Hyperbilirubinemia is one of the top three causes of death among newborns, according to studies [3].
As bilirubin is toxic to the brain cells, acute bilirubin encephalopathy can occur in cases of extreme jaundice. This condition can result in brain trauma and lead to kernicterus, which causes repetitive and uncontrolled movements, a permanent upward look, and hearing loss. However, timely treatment can help in preventing long-term damage [4].
According to statistics, the poorest parts of the world have the highest rates of morbidity and death from neonatal jaundice complications, such as acute bilirubin encephalopathy and kernicterus [5]. A blood test for Total Serum Bilirubin (TSB) is used to recognize newborns that are at high risk of developing bilirubin encephalopathy [6]. Spectrophotometry techniques that analyze serum and plasma are widely used to assess TSB [7]. Such a procedure entails the collection of blood samples from patients; thus, it is a painful and stressful procedure. Instead, Transcutaneous Bilirubin (TcB), which is a non-invasive test for the detection of jaundice, is used [8]. Yet TcB is not always accessible in places with limited healthcare services, including hospitals sometimes [9].
One of the most effective treatment methods of neonatal jaundice is phototherapy. More than 20 years ago, the first study on the use of phototherapy was published [10]. The key justification for using phototherapy is to avoid the need for exchange transfusions. As the use of exchange transfusions has become very uncommon, it can be now assumed that phototherapy is the leading treatment method. Contemporary phototherapy was discovered in England when it was noticed that the skin of babies who were exposed to sunlight on a daily basis was less jaundiced than unexposed ones. Phototherapy has been commonly used in the treatment of jaundice since then [11].
The ultimate purpose of phototherapy is to lower or stop the current level of circulating bilirubin from increasing. This can be accomplished by using light energy to alter the form and structure of bilirubin, allowing it to be transformed into molecules that can be excreted even when regular conjugation is inadequate [12]. Light absorption by dermal and subcutaneous bilirubin causes a fraction of the pigment to undergo a series of photochemical reactions, each of which occurs at a different rate. As shown in Figure 1, bilirubin absorbs light most significantly in the blue region of the spectrum (near 460 nm). Light penetration through tissue in this region increases dramatically as the wavelength increases [13]. Only the wavelengths that are absorbed by bilirubin and penetrate through tissue have a phototherapeutic effect, so the intensity and wavelengths of used light have a significant impact on the rate of bilirubin photoproducts development. Considering these factors, the most efficient light source for treating hyperbilirubinemia is one that emits light in the 460 to 490 nm range of the spectrum (blue) [14].
Phototherapy as a treatment method for jaundice is safe, comfortable, and reliable. However, jaundiced children who do not respond to phototherapy or have extreme hyperbilirubinemia at the time of diagnosis are treated with more invasive and serious methods, such as exchange transfusion, to eliminate or mitigate bilirubin-induced brain trauma [15]. Computer vision technologies have advanced to the point that they can now undertake more complex functions and communicate with other electronic systems more effectively. Assistive technologies (ATs) are examples of using computer vision in improving the quality of life of people with disabilities. Assistive technology is any item, piece of equipment, software program, or product system that is used to increase, maintain, or improve the functional capabilities of persons with disabilities [16]. Assistive technologies aim to enable people to live healthy, productive, independent, and dignified lives, and to participate in education, the labor market and civic life. Moreover, assistive technologies reduce the need for formal health and support services, long-term care and the work of caregivers. In the last few decades, there has been a tremendous increase in demand for assistive technologies. As a consequence, many research papers addressing the development of assistive technologies have appeared in the literature. We refer the readers to reference [16] for more information about the use of computer vision in assistive technologies.
In addition to assistive technologies, computer vision has been extensively used in the medical field. The emerging new technologies, including digital cameras and smartphones, have become an option for tackling the need for more affordable, portable, and cost-effective methods to screen newborns for jaundice. These new technologies have proved to perform as well as or even better than the current screening tools. Predicting bilirubin concentration by observing the color of the outer skin layer that is visible to the human eye is one of the common methods that can be used to detect jaundice. This can be achieved by finding a direct relationship between skin color and bilirubin concentration through examining the visual features of the skin using a camera and image processing techniques [17].
One of the first attempts to implement an alternative diagnosis approach was made by a group of researchers in 2009, in which they designed a non-invasive method to measure the bilirubin level in 61 newborns. In the proposed method, images of the chests of the newborn were taken using a digital camera, and the authors manually inspected and adjusted them in Photoshop. Then the images were analyzed, and the values of Y and M components of the CMYK system were measured. By subtracting the value of M from Y, the real value of serum bilirubin was found. The correlation between total serum bilirubin and the value of Y-M was assessed by Pearson’s product-moment correlation and linear regression. The authors found a significant correlation between serum bilirubin level and bilirubin estimated values obtained from the images. Although the method was considered imprecise, it was the beginning of the other non-invasive methods [18].
A study by Mansor et al. [19] monitored jaundice in newborns by using a color detection method. The detection method relied on images selected from a database. The images used differ from each other in terms of illumination level, distance, and the angle of capturing. The images were then processed with Matlab using the Image Acquisition Toolbox. The skin detection was based on YCrCb color space applied to the input images. This color space has the advantage that Chroma (CrCb) and luminance (Y) information are stored in different channels, which is suitable for the used images as they were taken under different lighting conditions. The authors discarded the luminance component (Y) because lighting information could easily lead to false detection. Then they used certain features such as mean, standard deviation, skewness, kurtosis, energy, and entropy to compare the color of normal skin and the color of skin with jaundice. The authors found that Kurtosis gives a higher value compared to other features; thus it was used to detect jaundice. In 2013, the authors developed their work further and used the k-NN algorithm as a classifier for discriminating infant image textures. The experimental results published in [20] revealed that the proposed method could act as a supplement to support earlier detection and more effective treatment due to improved jaundice recognition.
In another study, Munkholm et al. [21] proposed a method for transcutaneous bilirubin measurement that uses the camera of an iPhone 6 as the primary tool for data collection. A dermatoscope (which is a device that consists of a magnifier, a light source, and a transparent plate that is used for inspection of skin lesions unobstructed by skin surface reflections) was attached to the iPhone 6. Between the iPhone 6 and the dermatoscope, a Wratten No. 11 filter was used to minimize hemoglobin reflectance, allowing the wavelengths emitted by bilirubin to be sensed. After that, Matlab was used to calculate the average intensity of the red, green, and blue channels for each pixel. The Pearson’s correlation coefficient was used to assess the relationship between channel intensity and TSB levels. The results showed that photographs taken with a smartphone connected to a dermatoscope and applied to a neonate’s glabella provided good evidence that could be used to test for neonatal hyperbilirubinemia. Nevertheless, it did not reach a degree of validity appropriate for clinical use.
Kawano et al. [22] proposed a non-invasive method for neonatal jaundice detection that uses image processing techniques. The researcher used the normalized RGB color and a threshold value to extract the face area and then extract the eye map and mouth map. To detect jaundice, two image features were used: the first was the measurement of the average value of skin hue information. The second was to check the color spread, as skin color remains the same in normal cases but varies in cases of jaundice. The eigenvalues of the variance–covariance matrix were then found to see if skin color was spread or not. The method suggested in [22] is simple and can be improved to achieve better results; however, it was unable to extract skin area clearly because eyebrows and eyes could not be removed using an eye chart, resulting in failed cases.
Endang et al. [23] proposed a risk-zone estimation system. The system uses a digital camera to take images of newborns, uses a median filter to delete grains from the images, and uses color correction to reduce color saturation by using a color card of three main colors: red, green, and blue. The images were then transformed into three different color spaces: RGB, HSV, and YCbCr, with statistical parameters computed from the histograms of each channel. These parameters were used as input parameters for the validation and modeling of linear regression with an approximate bilirubin level as an output variable. Even though the proposed system was simple and had a strong correlation category, it had an error percentage of 17% and its accuracy was only 67%.
The authors of [24] developed a system for measuring bilirubin levels in newborn infants. The system combines color analysis of digital images with physics-based modeling of light transport in the skin. Using a mathematical model based on diffusion theory, the authors built a library of simulated reflectance spectra of newborn skin. The authors also took digital images with a mobile camera that only used three colors: red, green, and blue. Colors on the reference card used with each image were used to calibrate the colors. A color spectrometer was used to measure each card, and the results were saved and compared to a large database of color and bilirubin. The database could be downloaded to the phone and used even when the phone was not connected to the internet. The findings in [24] were shown to be strongly correlated.
In [25], Rong et al. introduced an image-based system named AIB that used a colored calibration card and an automated smartphone to predict jaundice and compare the results with TcB and TSB for preterm and term neonates. The skin images captured by the smartphone were uploaded to a cloud server that employed machine learning-based software to provide an individualized and immediate predicted bilirubin index. The t-test was utilized to determine if AIB and total serum bilirubin (TSB) were significantly different. Moreover, Bland–Altman analysis was used to measure the agreement of AIB with TcB. The results revealed a strong relevance between AIB and TSB and good correlation was found; however, the sensitivity and specificity of the system were not high.
Another study by Taylor et al. [26] captured images for 530 newborns (African American, Hispanic, and Asian American) using an iPhone 5s. The authors used a colored calibration card that was placed on the newborn’s sternum and fitted by using a small amount of adhesive. The images were sent to a computer server for processing over the Internet. Pixel RGB values from various regions of the colored calibration card, as well as an area of the newborn’s skin in the hollow section of the card, were measured on the server. After that, the measurements were converted to additional color representations for feature extraction and fed into a 10-fold cross-validation process, a machine-learning algorithm that was used to predict bilirubin levels. The proposed approach had many benefits, including the use of low-cost, easily accessible technology to test newborns for jaundice, relatively reliable estimates of TSB values in newborn babies, and high specificity for detecting newborns with TSB levels in the high-risk zone. Furthermore, the results revealed that while BiliCam is not precise enough to be used as a standalone tool for assessing jaundice in newborns, it can be used as a screening tool to help determine which babies need blood collection for TSB. On the other hand, the proposed system has a disadvantage, which is: if there is no internet, there is no connection to the server, and therefore the system was inoperable.
The approach suggested by Aydin et al. [27] was used to analyze photographs of 40 healthy and 40 jaundiced babies taken with a Samsung Galaxy Alpha smartphone’s 12 MP camera. In the proposed approach, an eight-color calibration card was placed on the abdomen of the baby. Color balance was the first stage of the proposed system, which was accomplished by an image segmentation technique. Important regions and their data were retained, while unused regions were reorganized in black. As a result, the photographs are not affected by ambient light, reflections, or shadows. The details about the baby’s skin and the colors of the calibration card were collected in RGB, YCbCr, and Lab color spaces in the second stage, which was feature extraction. This was achieved by using colormap transformations and features calculation. Machine learning regressions are the proposed approach’s third stage. The dataset collected in the second stage was used in this stage to apply the kNN (k-Nearest Neighbor) and SVR (Support Vector Regression) algorithms. The final stage of the proposed approach involved estimating bilirubin levels using the regression process data. The results indicate that the suggested approach was of good quality and took a small period to process.
Padidar et al. [28] proposed an application based on Android OS for detecting jaundice in 113 neonates. A mobile, a zoom microscope clip, and a colored calibration card were needed for this app-based bilirubin level estimator. The average RGB values of the images of the calibration card and the forehead skin were measured and then translated to hue, saturation, and intensity (HSI) parameters. To calculate bilirubin levels, the authors used machine learning and its subcategories, such as supervised learning and regressive methods. The proposed application is a promising screening method for neonatal jaundice since all of the earlier mentioned procedures were implemented without the use of an internet connection. Furthermore, if used by parents at home to screen for neonatal jaundice, the app could significantly reduce morbidity and mortality, particularly due to its low cost. However, the app’s sensitivity and precision are insufficient to assess whether a newborn requires medical care such as phototherapy and exchange transfusion.
Angelico et al. [29] developed an intuitive application for Android smartphones. Machine learning was used in the application to generate an algorithm for stool color recognition based on the seven grades of the infant stool color card, which was considered as the reference model. Consecutive images of stool were taken by the smartphone’s camera and the application classified the images as “normal”, and “acholic”. The sensitivity, specificity, and accuracy of the application were evaluated based on the analysis of 165 images and were 100, 99.0, and 99.4%, respectively.
The authors of [30] presented a technique for jaundice detection by processing images of the sclera. A webcam camera and a controllable LED flashlight mounted on the webcam were used to capture the images. The flashlight was optimized to maintain a steady level of illumination regardless of outside lighting conditions. The individual was asked to wear specially made goggles during the image capture process, which blocked ambient light and increased the efficiency of the region of interest extraction. After that, the images were exposed to a 3D median filter to eliminate noise. The proposed technique depends on images of the sclera; therefore, sclera extraction must be performed by using a bounding box algorithm and color thresholding to suppress the skin around the eye. The authors also used RGB, HSV histogram, and a random forest regression algorithm to determine the level of bilirubin. The technique proposed in [30] was able to assess the intensity of jaundice and provide results in a matter of minutes. Furthermore, it did not require exceptionally trained personnel to operate; however, it was only suitable for adults.
Another study by Outlaw et al. [31] suggested a neonatal jaundice screening method that involved taking photographs of 51 neonates’ sclera using a smartphone. The RGB values were derived directly from the color filter output data using the proposed method. After that, the median RGB values within the region of interest (ROI) (manually selected) for flash and no-flash images were determined, and the RGB values without ambient lighting were estimated by subtracting the output RGB values of images without flash from the images with flash. The RGB values were then converted to XYZ values to obtain chromaticity, which was used to measure the bilirubin rate. The suggested method’s key benefits included eliminating the need for color cards in any image’s frame for calibration and ensuring that the ambient light falling on the ROI does not change in intensity or chromaticity. On the other hand, there are some limitations, including that capturing photographs for an infant’s eyes was difficult owing to erratic movements and the amount of time spent sleeping, many neonates’ sclera has a blue hue because it is thinner than adults, and all flash and no-flash images must be taken for the same exposure; otherwise, it may produce unusable images.
With the evidence-based need for globally affordable jaundice detection technologies, the main contribution is the design of an inexpensive and reliable jaundice screening and treatment system that is based on computer vision and color analysis. The proposed solution can significantly reduce brain dysfunction and mortalities related to jaundice. In addition, it neither uses color calibration cards, which can cause infection to neonates and incur an additional cost, nor does it use any accessories that are usually used in the sclera color analysis. Moreover, the system controls the operation of the blue LED light (that is more effective at reducing the time spent under phototherapy) compared with conventional phototherapy that uses a compact fluorescent lamp (CFL) or halogen illumination [32] by the use of a microcontroller and sends the neonate’s status over GSM to the mobile phone of the concerned person. Another advantage of the proposed system over the other existing systems is the response time, which is only 1 s. This response time is considerably much shorter than the time needed by other tests such as TSB.
2. Materials and Methods
2.1. Data Collection
The functionality of the proposed system was tested on three different sets of data. The first data set was collected in Ibn Al-Atheer teaching hospital of pediatrics in Mosul, Iraq. The examination was performed in real-time on a group of twenty infants with a known TSB rate. All of these infants were over 48 h old and with a birth weight of 2500 g or above. The study was conducted according to the guidelines of the Declaration of Helsinki (Finland 1964), and written informed consent has been obtained from the parents after a full explanation of the experimental procedures. Ethical clearance was granted by the Human Research Ethics Committee at the Ministry of Health and Environment, Training and Human Development Centre, Iraq (Protocol number: 84/21). The second data set contains 16 photos of infants that were downloaded from the internet; 5 of these photos are for healthy babies, and the other 11 photos are for jaundiced babies. The third set of data was obtained by using four manikins. The dimensions of the manikins are 56 × 25 × 12 cm (LWH). These manikins were used as a replacement for real infants to investigate four different cases. The first case is for a manikin that has a normal light skin which represents the case of an infant without jaundice, while the second case is for a manikin that has a yellowish light skin which represents an infant with jaundice. The third case is for a manikin that has normal brown skin which is the case of a brown skin infant without jaundice, and the fourth case is for a manikin that has a yellowish-brown skin color which represents the case of a brown skin infant with jaundice.
2.2. Experimental Setup
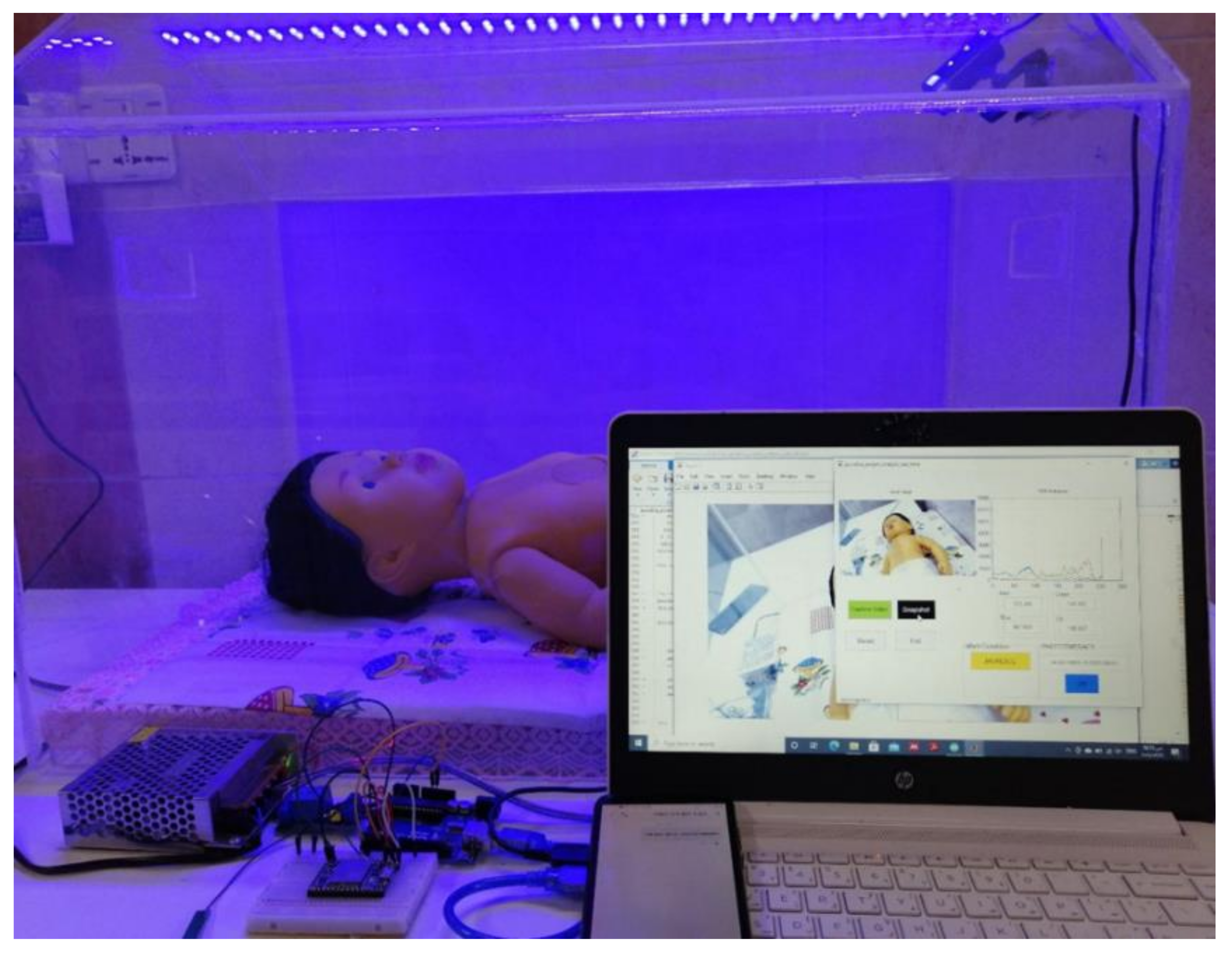
In the proposed system, a full-HD Webcam is used, which offers smooth video recording and high-quality rich-color image capturing. The video resolution is up to 1080 × 1920 pixels, and the still image resolution is up to 16 megapixels. To capture images of manikins and infants, the camera was fitted at 30 cm away from the subject, at an angle of 45 degrees and under ambient lighting conditions of 200 lux, using fluorescent lamps as a source of lighting. Matlab 2020 was used for image processing as well as signal processing. Additionally, an Arduino Uno Microcontroller was used to control the operation of the blue LED light, and a GSM A9 module was used to send an SMS message to the care provider’s mobile phone regarding the infant’s condition. Figure 2 shows the system’s setup including the camera and the blue LED light, which was switched ON when a manikin that has a yellowish light skin was used.
2.3. System Design
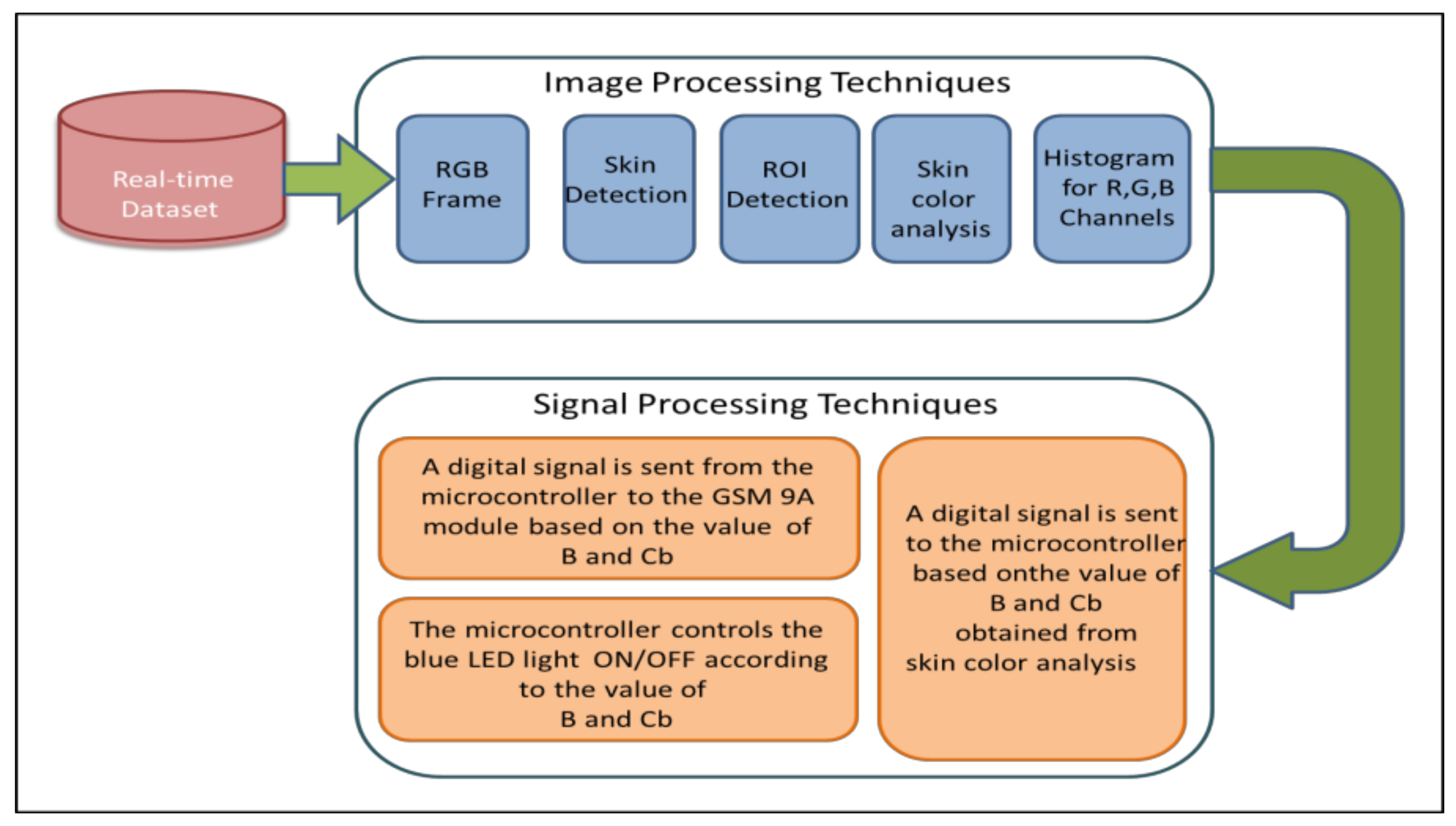
Different image processing techniques were applied in this system for extracting and analyzing useful features of interest in real-time. These techniques include skin detection, Region of Interest (ROI) selection, skin color analysis, color space transformation. Figure 3 shows the general design of the proposed system.
The process of finding skin-colored pixels in an image or video is known as skin detection. Skin color is the primary key for skin detection as it is a useful feature to detect skin pixels. However, it is not the only deciding factor due to the variation in skin tone according to race or the light conditions. Several techniques that can be used to detect skin in an image, but color-based techniques are the most common ones as they do not require a long processing time [33].
In the proposed system, a Matlab program was used to detect the skin from the captured images. It is based on color space transformation, thresholding, and image processing techniques. The proposed system starts the diagnosis by converting the image of the neonate from the RGB color space to the “Lab” color space (The Lab color space expresses colors mathematically as three values, “L” for lightness, “a” for green–red colors, and “b” for the blue–yellow colors). Converting an image to “Lab” is the easiest conversion to do, as there are no settings that the conversion depends on, and there are no decisions to be made. The Lab color space is the most exact method of representing colors, and it defines colors independently of how they are created or displayed. This property makes the Lab color space very useful in skin detection as results are comparable regardless of the image capturing device. Afterward, a threshold is applied in gray level and binary to the “Lab” channels individually (Image thresholding is a technique for binarizing an image based on the intensity of the pixels). The threshold value and the grayscale image are typically the inputs to such thresholding algorithms, and the output is a binary image. If a pixel in the input image has a higher intensity than the threshold, the resulting output pixel is white (foreground); otherwise, the output pixel is black (background). The reason behind using thresholding is to classify each pixel independently of its neighboring pixels and to obtain a binary image [34]. It is worth mentioning that in the proposed system, Otsu’s Thresholding method was used.
Morphology operations are used to enhance the image and segment the skin from the output of the previous part. The morphological operations were performed on a binary image that has only two values: zero and one. As a result, it can effectively deal with the ROI in terms of object extraction, image noise reduction, and image enhancement. The output image from the previous operations is further processed using an erosion filter to remove the unwanted pixels. While the pixels of skin are set to one, every other pixel near the border is set to zero and erased. Therefore, the resulting image has smooth edges, and any area other than the skin is removed. The resulting image after the aforementioned operations represents the desired ROI which contains only the skin. The technique used in detecting the skin and identifying the region of interest is very efficient for jaundice detection, especially for the cases when the neonate is moving, crying, lying on his belly, or on one side. Figure 4 shows how to determine the ROI in different postures.
Skin color is a highly informative aspect in various human-related image processing applications. Skin color analysis deals with analyzing each pixel of skin in ROI based on the following main color models: RGB (red, green, and blue), and YCbCr (Luminance, Chrominance). The main advantage of using the YCbCr color space is that the chroma (CrCb) and luminance (Y) components are stored in different channels. Thus, it is easy to remove the luminance component as it can easily lead to false detection. Therefore, the performance and results of the skin color analysis methods that use the YCbCr color space is quite promising. It is already known in the literature that the blue component is the most prominent channel for yellowness detection compared to other channels [35]. This conclusion is based on the results of tests conducted on many pictures of neonates that have jaundice. Thus, the B and Cb channels were used in the proposed system as the main components in detecting jaundice. A threshold value for B and Cb is used in this system to diagnose infants with jaundice in real-time; if the value of B or Cb exceeds this threshold value, the infant is diagnosed as jaundice-free and does not require phototherapy. The methodology followed in this paper can be described in the following steps:
- Capturing real-time images using a full HD digital camera.
- Using color transformation and Otsu thresholding techniques to detect the skin in the captured images.
- Specify the ROI (skin) by using image processing techniques.
- Finding the values of the B channel and Cb channel for the ROI from the RGB and YCbCr color spaces, respectively.
- Comparing the values of the B and Cb channels with the predefined threshold value.
- If the value of either B or Cb channel is less than the threshold, the diagnosis result is “Jaundice” and the infant needs phototherapy. Otherwise, the diagnosis result is “Normal”.
- If phototherapy is needed, the system will switch ON the blue LED light. Otherwise, the blue LED will be switched OFF. In both cases, an SMS message is sent to the care provider informing him/her whether the infant needs phototherapy or not.
3. Results
As mentioned earlier, a threshold value was used to determine if the infant has jaundice or not. The threshold value was set to 100 in all the experiments that were conducted to check the functionality and accuracy of the proposed system. We consider three different scenarios based on the subjects used, these scenarios are:
3.1. Scenario 1
In this scenario, four manikins were used as a substitute for real infants to cover different skin tone cases. The tests were conducted under the same ambient lighting conditions and for the same camera–manikin distance in all cases. The first case considered is for a manikin that has a light skin color, which resembles a jaundice-free infant. As shown in Figure 5, the system detects the infant condition as normal and does not need phototherapy because the mean values of b and Cb channels are higher than the threshold value.
Figure 6 shows the behavior of the proposed system when a manikin that has a yellowish light skin color is used. Since the values of the B and Cb channels are less than the threshold value, then the system diagnoses the condition as jaundice and indicates that the infant needs phototherapy. Based on this diagnosis, the computer sends out a digital signal to the Arduino microcontroller which in turn switches ON the blue LED in the incubator and also sends a digital signal to the GSM module as shown in Figure 7. After receiving the digital signal, the GSM module sends out an SMS message to the mobile phone of the care providers informing them about the test result. Figure 8 shows an example of the SMS message that is sent to the mobile phone of the care provider when an infant is detected with jaundice.
Figure 9 illustrates the case when a manikin with a brown complexion is used. It can be noted that the mean values of the B and Cb channels of the manikin’s image that are calculated by the system are higher than the threshold value. Thus, the system considers the manikin condition is normal (jaundice-free) and does not need phototherapy.
In the last case, a manikin with yellowish brown skin was used, which represents the case of a jaundiced brown skinned infant. Figure 10 depicts how the proposed system detects that the manikin has jaundice and needs phototherapy. This diagnosis is based on the mean values of the B and Cb channels which are higher than the threshold value specified by the system. As clarified earlier, the blue LED inside the incubator is switched ON and an SMS message is sent to the care provider.
Table 1 summarizes the four different cases considered in Scenario 1.
3.2. Scenario 2
In this scenario, 16 images of infants (11 images of diagnosis with jaundice skins and 5 images for babies with normal skin color) from the internet were used with different skin tone colors, under different lighting conditions, using different cameras, and with different camera–infant distance. As shown in Table 2, the proposed system successfully diagnosed all the infants without jaundice as normal infants not needing phototherapy. In addition, all the images of the infants with jaundice were diagnosed as “jaundice” and needing phototherapy.
3.3. Scenario 3
Images of twenty infants who were kept in the care unit of Ibn Al-atheer hospital are used in this scenario. The TSB for these infants is pre-known and is used to compare and investigate the validity of the results produced by the proposed system. As shown in Table 3, the proposed system diagnoses infants that have a TSB level less than 14 mg/dl as normal (jaundice-free) and do not need phototherapy. On the other hand, if the TSB level of an infant is higher than 14 mg/dl, then the system diagnoses the infant as jaundiced and needing phototherapy.
4. Discussion
Jaundice is a very common and serious illness that affects newborns in the first week of life. It is a source of fear for parents and a source of worry for the physician. Thus, many previous researchers tried to find a way to detect jaundice to bypass the faults of the TSB and TCB tests. However, most of this research cannot be considered as a completely reliable substitute for the TSB test in detecting jaundice for many reasons, such as: the accuracy of the methods used to determine the ROI, the efficiency in mitigating the effect of lighting, the need for using a colored calibration card which can be a source of infection and allergy and adds extra cost. In addition, the research that proposed the use of the sclera of the eye as a ROI are not suitable for neonates as their eyes are closed most of the time, and also this requires extra accessories. Moreover, the use of stool images is only suitable to detect jaundice that is caused by biliary atresia. In contrast with the previous research, the proposed system overcomes the aforementioned obstacles by: (1) using an efficient skin detection technique rather than choosing a specific ROI such as face or sclera; (2) using the Cb channel of the YCbCr color space in analyzing the skin color to eliminate the effect of ambient lighting on the results; (3) using a threshold value to diagnose jaundice, which can be adjusted easily to control the desired bilirubin level at which the phototherapy is provided; (4) high diagnostic accuracy at a relatively low cost. However, there is a limitation: in the absence of lighting, the result of the diagnosis was inaccurate, but by using a night vision and Infrared camera a jaundice detection system can be developed to work even in the absence of adequate lighting.
5. Conclusions
Neonatal jaundice is a very common condition that affects infants in their first few days of life. Prompt diagnosis and treatment of jaundice are essential to prevent infant brain damage and its complications. In this paper, a developed imaging system based on computer vision (digital camera) was proposed to diagnose and treat jaundice in neonates. Several image processing techniques were applied to the captured images to detect the skin of the neonate and automatically determine the ROI. Afterwards, color space transformation techniques were applied to the ROI and based on the output of these techniques. The proposed system decides efficiently whether the neonate has jaundice or not. If jaundice is detected, the system starts the phototherapy by switching a blue LED light ON. The functionality and reliability of the proposed system were investigated and tested in three different scenarios. Moreover, the effect of skin color, camera distance, and ambient lighting on the system’s performance were also considered. The proposed system has several advantages over the other proposed system found in literature, including that it is effective in detecting jaundice at a TSB level of 14 mg/dL and above, the detection time is only 1 s, and it can be used in hospitals and medical centers where laboratory facilities and trained medical staff are not available, due to its low cost.
Author Contributions
Conceptualization, A.A.-N.; methodology, W.H., A.A.-N., I.A.A.-R. and M.A.; software, A.A.-N. and W.H.; validation, W.H., I.A.A.-R. and M.A.; formal analysis, W.H., A.A.-N., and I.A.A.-R.; investigation, W.H., A.A.-N. and M.A.; resources, W.H., A.A.-N., and M.A.; data curation, W.H., A.A.-N. and M.A.; writing—original draft preparation, W.H.; writing—review and editing, A.A.-N., I.A.A.-R., M.A. and J.C.; visualization, W.H., A.A.-N., I.A.A.-R. and J.C.; project administration, A.A.-N. and J.C.; funding acquisition, A.A.-N. and J.C.; supervision, A.A.-N. and I.A.A.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ministry of Health and Environment, Training and Human Development Centre, Iraq (Protocol number: 84/21).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dzulkifli, F.A.; Mashor, M.Y.; Khalid, K. Methods for determining bilirubin level in neonatal jaundice screening and monitoring: A literature review. J. Eng. Res. Educ. 2018, 10, 1–10. [Google Scholar]
- Brits, H.; Adendorff, J.; Huisamen, D.; Beukes, D.; Botha, K.; Herbst, H.; Joubert, G. The prevalence of neonatal jaundice and risk factors in healthy term neonates at National District Hospital in Bloemfontein. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhutani, V.K.; Zipursky, A.; Blencowe, H.; Khanna, R.; Sgro, M.; Ebbesen, F.; Bell, J.; Mori, R.; Slusher, T.M.; Fahmy, N. Neonatal hyperbilirubinemia and Rhesus disease of the newborn: Incidence and impairment estimates for 2010 at regional and global levels. Pediatric Res. 2013, 74, 86–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vodret, S. Neonatal Hyperbilirubinemia: In Vivo Characterization of Mechanisms of Bilirubin Neurotoxicity and Pharmacological Treatments; International Centre for Genetic Engineering and Biotechnology: New Delhi, India, 2016. [Google Scholar]
- Mishra, S.; Agarwal, R.; Deorari, A.K.; Paul, V.K. Jaundice in the newborns. Indian J. Pediatrics 2008, 75, 157–163. [Google Scholar] [CrossRef]
- Hyperbilirubinemia, A.A.o.P.S.o. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics 2004, 114, 297–316. [Google Scholar] [CrossRef] [Green Version]
- Mantagou, L.; Fouzas, S.; Skylogianni, E.; Giannakopoulos, I.; Karatza, A.; Varvarigou, A. Trends of transcutaneous bilirubin in neonates who develop significant hyperbilirubinemia. Pediatrics 2012, 130, e898–e904. [Google Scholar] [CrossRef] [Green Version]
- Mansouri, M.; Mahmoodnejad, A.; Taghizadeh Sarvestani, R.; Gharibi, F. A comparison between transcutaneous bilirubin (TcB) and total serum bilirubin (TSB) measurements in term neonates. Int. J. Pediatrics 2015, 3, 633–641. [Google Scholar]
- Alsaedi, S.A. Transcutaneous bilirubin measurements can be used to measure bilirubin levels during phototherapy. Int. J. Pediatrics 2018, 2018, 4856390. [Google Scholar] [CrossRef] [Green Version]
- Mreihil, K.; Nakstad, B.; Stensvold, H.J.; Benth, J.Š.; Hansen, T.W.R.; Group, N.N.P.S.; Network, N.N.; Scheck, O.; Nordin, S.; Prytz, A. Uniform national guidelines do not prevent wide variations in the clinical application of phototherapy for neonatal jaundice. Acta Paediatr. 2018, 107, 620–627. [Google Scholar] [CrossRef] [Green Version]
- Maisels, M.J.; McDonagh, A.F. Phototherapy for neonatal jaundice. N. Engl. J. Med. 2008, 358, 920–928. [Google Scholar] [CrossRef] [Green Version]
- Mreihil, K.; Benth, J.Š.; Stensvold, H.J.; Nakstad, B.; Hansen, T.W.R.; Group, N.N.P.S.; Network, N.N.; Scheck, O.; Nordin, S.; Prytz, A. Phototherapy is commonly used for neonatal jaundice but greater control is needed to avoid toxicity in the most vulnerable infants. Acta Paediatr. 2018, 107, 611–619. [Google Scholar] [CrossRef] [Green Version]
- Woodgate, P.; Jardine, L.A. Neonatal jaundice: Phototherapy. BMJ Clin. Evid. 2015, 2015. [Google Scholar]
- Donel, J. Bili blanket phototherapy. Int. J. Contemp. Pediatr. 2019, 6, 2231–2234. [Google Scholar] [CrossRef]
- Maisels, M.; Watchko, J.; Bhutani, V.; Stevenson, D. An approach to the management of hyperbilirubinemia in the preterm infant less than 35 weeks of gestation. J. Perinatol. 2012, 32, 660–664. [Google Scholar] [CrossRef]
- Marco, L.; Giovanni, M.F. Computer Vision For Assistive Healthcare; Academic Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Hashim, W.; Al-Naji, A.; Al-Rayahi, I.A.; Oudah, M. Computer Vision for Jaundice Detection in Neonates Using Graphic User Interface. IOP Conf. Ser. Mater. Sci. Eng. 2021, 1105, 012076. [Google Scholar] [CrossRef]
- Leartveravat, S. Transcutaneous bilirubin measurement in full term neonate by digital camera. Med J. Srisaket Surin Buriram Hosp. 2009, 24, 105–118. [Google Scholar]
- Mansor, M.; Yaacob, S.; Hariharan, M.; Basah, S.; Jamil, S.A.; Khidir, M.M.; Rejab, M.; Ibrahim, K.K.; Jamil, A.A.; Junoh, A. Jaundice in newborn monitoring using color detection method. Procedia Eng. 2012, 29, 1631–1635. [Google Scholar] [CrossRef] [Green Version]
- Mansor, M.; Hariharan, M.; Basah, S.; Yaacob, S. New newborn jaundice monitoring scheme based on combination of pre-processing and color detection method. Neurocomputing 2013, 120, 258–261. [Google Scholar] [CrossRef]
- Munkholm, S.B.; Krøgholt, T.; Ebbesen, F.; Szecsi, P.B.; Kristensen, S.R. The smartphone camera as a potential method for transcutaneous bilirubin measurement. PLoS ONE 2018, 13, e0197938. [Google Scholar]
- Kawano, S.; Zin, T.T.; Kodama, Y. A Study on Non-contact and Non-invasive Neonatal Jaundice Detection and Bilirubin Value Prediction. In Proceedings of the 2018 IEEE 7th Global Conference on Consumer Electronics (GCCE), Nara, Japan, 9–12 October 2018; pp. 401–402. [Google Scholar]
- Juliastuti, E.; Nadhira, V.; Satwika, Y.W.; Aziz, N.A.; Zahra, N. Risk Zone Estimation of Newborn Jaundice Based on Skin Color Image Analysis. In Proceedings of the 2019 6th International Conference on Instrumentation, Control and Automation (ICA), Bandung, Indonesia, 31 July–2 August 2019; pp. 176–181. [Google Scholar]
- Aune, A.; Vartdal, G.; Bergseng, H.; Randeberg, L.L.; Darj, E. Bilirubin estimates from smartphone images of newborn infants’ skin correlated highly to serum bilirubin levels. Acta Paediatr. 2020, 109, 2532–2538. [Google Scholar] [CrossRef] [Green Version]
- Rong, Z.; Luo, F.; Ma, L.; Chen, L.; Wu, L.; Liu, W.; Du, L.; Luo, X. Evaluation of an automatic image-based screening technique for neonatal hyperbilirubinemia. Zhonghua Er Ke Za Zhi / Chin. J. Pediatrics 2016, 54, 597–600. [Google Scholar]
- Taylor, J.A.; Stout, J.W.; de Greef, L.; Goel, M.; Patel, S.; Chung, E.K.; Koduri, A.; McMahon, S.; Dickerson, J.; Simpson, E.A. Use of a smartphone app to assess neonatal jaundice. Pediatrics 2017, 140, e20170312. [Google Scholar] [CrossRef] [Green Version]
- Aydın, M.; Hardalaç, F.; Ural, B.; Karap, S. Neonatal jaundice detection system. J. Med Syst. 2016, 40, 166. [Google Scholar] [CrossRef]
- Padidar, P.; Shaker, M.; Amoozgar, H.; Khorraminejad-Shirazi, M.; Hemmati, F.; Najib, K.S.; Pourarian, S. Detection of neonatal jaundice by using an android OS-based smartphone application. Iran. J. Pediatrics 2019, 29, e84397. [Google Scholar] [CrossRef] [Green Version]
- Angelico, R.; Liccardo, D.; Paoletti, M.; Pietrobattista, A.; Basso, M.S.; Mosca, A.; Safarikia, S. A Novel Mobile Phone Application for Infant Stool Color Recognition: An Easy and Effective Tool to Identify Acholic Stools in Newborns. J. Med Screen. 2020, 26, 230–237. [Google Scholar]
- Miah, M.M. Non-Invasive Bilirubin Level Quantification and Jaundice Detection by Sclera Image Processing. In Proceedings of the 2019 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 17–20 October 2019; pp. 1–7. [Google Scholar]
- Outlaw, I.d.; Nixon, M.; Odeyemi, O.; Macdonald, L.W.; Meek, J.; Leung, T.S. Smartphone Screening for Neonatal Jaundice via Ambient-Subtracted Sclera Chromaticity. PLoS ONE 2020, 15, e0216970. [Google Scholar] [CrossRef] [Green Version]
- Viau Colindres, J.; Rountree, C.; Destarac, M.A.; Cui, Y.; Pérez Valdez, M.; Herrera Castellanos, M.; Mirabal, Y.; Spiegel, G.; Richards-Kortum, R.; Oden, M. Prospective randomized controlled study comparing low-cost LED and conventional phototherapy for treatment of neonatal hyperbilirubinemia. J. Trop. Pediatrics 2012, 58, 178–183. [Google Scholar] [CrossRef] [Green Version]
- Kolkur, S.; Kalbande, D.; Shimpi, P.; Bapat, C.; Jatakia, J. Human skin detection using RGB, HSV and YCbCr color models. arXiv 2017, arXiv:1708.02694. [Google Scholar]
- Bangare, S.L.; Dubal, A.; Bangare, P.S.; Patil, S. Reviewing otsu’s method for image thresholding. Int. J. Appl. Eng. Res. 2015, 10, 21777–21783. [Google Scholar] [CrossRef]
- Chowdhary, A.; Dutta, S.; Ghosh, R. Neonatal Jaundice Detection using Colour Detection Method. Int. Adv. Res. J. Sci. Eng. Technol. 2017, 4, 197–203. [Google Scholar]
Figure 1.
The effective range of wavelengths for phototherapy.

Figure 2.
The system’s camera and blue LED when using manikin that has a yellowish light skin.

Figure 3.
The general design of the proposed system.

Figure 4.
The region of interest in different positions.

Figure 5.
A manikin with light skin color (jaundice-free).

Figure 6.
A manikin with a yellowish light skin color and jaundice.

Figure 7.
The blue LED inside the incubator is switched ON when jaundice is detected.

Figure 8.
An example of the SMS sent by the proposed system to the care provider.

Figure 9.
A manikin with brown skin color and jaundice-free.

Figure 10.
A manikin that has yellowish brown skin.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The summary of all cases considered in scenario 1.
| Manikin Skin Color | B Channel | Cb Channel | Infant Condition | Blue LED Status |
|---|---|---|---|---|
| light complexion | 150.272 | 116.807 | Normal | OFF |
| light and yellow complexion | 46.666 | 99.427 | Jaundice | ON |
| brown complexion | 127.764 | 113.391 | Normal | OFF |
| brown and yellow complexion | 85.245 | 97.537 | Jaundice | ON |
Table 2.
The summary of all images considered in scenario 2.
| B Channel | Cb Channel | System Diagnosis | BLUE LED State | Detection Rate | |
|---|---|---|---|---|---|
| Image 1 | 153.689 | 107.847 | Normal | OFF | 100% |
| Image 2 | 82.243 | 71.472 | Jaundice | ON | 100% |
| Image 3 | 78.390 | 93.892 | Jaundice | ON | 100% |
| Image 4 | 96.535 | 94.734 | Jaundice | ON | 100% |
| Image 5 | 139.922 | 105.819 | Normal | OFF | 100% |
| Image 6 | 72.2273 | 87.396 | Jaundice | ON | 100% |
| Image 7 | 74.297 | 86.833 | Jaundice | ON | 100% |
| Image 8 | 174.604 | 122.421 | Normal | OFF | 100% |
| Image 9 | 149.787 | 106.868 | Normal | OFF | 100% |
| Image 10 | 71.236 | 89.514 | Jaundice | ON | 100% |
| Image 11 | 91.926 | 90.523 | Jaundice | ON | 100% |
| Image 12 | 81.257 | 70.999 | Jaundice | ON | 100% |
| Image 13 | 73.113 | 91.935 | Jaundice | ON | 100% |
| Image 14 | 71.236 | 89.514 | Jaundice | ON | 100% |
| Image 15 | 83.224 | 85.680 | Jaundice | ON | 100% |
| Image 16 | 113.996 | 109.049 | Normal | OFF | 100% |
Table 3.
A comparison between the TSB and diagnosis results of the proposed system.
| TSB mg/dl | B Channel | Cb Channel | Diagnosis | Blue LED Status | |
|---|---|---|---|---|---|
 | 7 | 172.586 | 122.225 | Normal | OFF |
 | 8.6 | 165.272 | 112.581 | Normal | OFF |
 | 9.5 | 158.541 | 119.198 | Normal | OFF |
 | 9.7 | 159.115 | 113.239 | Normal | OFF |
 | 11 | 142.738 | 120.761 | Normal | OFF |
 | 12 | 132.405 | 108.44 | Normal | OFF |
 | 12.3 | 128.241 | 101.419 | Normal | OFF |
 | 12.5 | 123.8 | 124.007 | Normal | OFF |
 | 13.3 | 111.418 | 120.743 | Normal | OFF |
 | 13.8 | 108.689 | 107.645 | Normal | OFF |
 | 14.2 | 99.702 | 119.679 | Jaundice | ON |
 | 14.8 | 93.178 | 118.437 | Jaundice | ON |
 | 15.1 | 91.688 | 107.441 | Jaundice | ON |
 | 16.5 | 86.435 | 94.539 | Jaundice | ON |
 | 16.7 | 83.36 | 93.043 | Jaundice | ON |
 | 17 | 80.576 | 92.693 | Jaundice | ON |
 | 18 | 73.741 | 88.060 | Jaundice | ON |
 | 18.2 | 70.382 | 89.123 | Jaundice | ON |
 | 20.1 | 65.555 | 70.467 | Jaundice | ON |
 | 26 | 48.240 | 67.465 | Jaundice | ON |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hashim, W.; Al-Naji, A.; Al-Rayahi, I.A.; Alkhaled, M.; Chahl, J. Neonatal Jaundice Detection Using a Computer Vision System. Designs 2021, 5, 63. https://doi.org/10.3390/designs5040063
AMA Style
Hashim W, Al-Naji A, Al-Rayahi IA, Alkhaled M, Chahl J. Neonatal Jaundice Detection Using a Computer Vision System. Designs. 2021; 5(4):63. https://doi.org/10.3390/designs5040063
Chicago/Turabian StyleHashim, Warqaa, Ali Al-Naji, Izzat A. Al-Rayahi, Makram Alkhaled, and Javaan Chahl. 2021. "Neonatal Jaundice Detection Using a Computer Vision System" Designs 5, no. 4: 63. https://doi.org/10.3390/designs5040063