1. Introduction
Typically, medical devices render alarms to notify staff when they need attention to ensure adequate functioning. However, when too abundant, alarms can result in alarm fatigue and associated desensitization in medical staff [
1]. This is undesirable for both staff and patients, since longer response times to alarms can cause adverse outcomes. In a neonatal intensive care unit (NICU) high alarm pressure is specifically undesirable, since neonates are less tolerant to deviations in vital parameters and early-life noise exposure has an adverse effect on the developing brain [
2,
3]. Furthermore, the high noise level due to the number of alarms in a NICU, in combination with the task of comforting the parents of patients, is associated with a high burnout rate among NICU nurses [
4]. In addition, all alarms are a source of stress for parents, even though alarms from medical devices are often not as urgent as they sound. Therefore, the NICU environment could benefit from solutions to prevent alarms aimed at communicating the status of medical devices.
Currently, nurses get informed about the status of devices when thresholds for alarms are already breached. Earlier warning can prevent alarming by initiating preemptive action. However, earlier warnings should, especially in light of the increasing number of medical devices being used over the last couple of years [
1], be shown in an unobtrusive fashion rather than simply expedite the (intrusive) alarm. One way to achieve this is by employing
Calm technology, which displays warnings, or messages, in a subtle manner to be perceived without explicitly focusing attention on it [
5,
6]. Nurses should be calmly informed about the state of the medical device and or upcoming alarm, so that they can—in the blink of an eye—get an overview of relevant device statuses and act before they reach a critical situation [
7].
To calmly inform nurses, ambient lighting displays could be used [
7]. We expect that, by implementing calm technology, nurses can act in an early stage on the upcoming alarms and, thereby, prevent an alarm. To verify this, we developed a prototype, called CheckMates, to asses if the behavior of nurses could be positively influenced by such ambient lighting displays. Checkmates uses, colored lights to unobtrusively indicate the status of medical devices such as the water level in the incubator and the level of the medication syringes.
Since there is limited research on visualizing device statuses in the NICU department, this study tries to explore the potential of visualizing these statuses by gathering expert opinions and user experiences in a simulation setting. The aim of the research presented in this paper was to answer the following research questions: “What are the potential benefits of the implementation of CheckMates, which show device statuses, in the NICU department?” and “How is the use of Checkmates experienced with regard to nurses’ overview and planning capabilities?”. This brings us to the following hypothesis, which is based on the research questions: “The CheckMates enable nurses to notice the status of medical devices in their periphery and, thereby, help to create a better overview of their upcoming activities.”
To answer the research questions, an expert review and simulation study were performed to gather qualitative data. In addition to related work, the user study setup and data gathering, this paper will discuss data analysis and results. In the end, the paper will discuss and conclude upon the findings of the research.
2. Related Work
CheckMates is based on a design concept of Guerra; the Water Probe [
7]. In his thesis, Guerra focused on less obtrusive ways to communicate critical events detected by NICU devices and on reducing the amount and sound of alarms through better interactions with the alarm system. The Water Probe gives the nurses live feedback on the status of the water tank of the incubator through both peripheral and focused interactions. The Probe consists of a light display and sensor, which measures the water level in the incubator. The sensor is detachable so another sensor could be attached to measure another medical device if this is preferred. The light of the Probe slightly changes from one color to another color as the status of the device changes from completely full to empty. When the device almost runs out of water, the Probe starts pulsing calmly.
Other research groups have also focused on solving similar problems. For instance, other researchers have strived for a calmer atmosphere in adult intensive care units, focusing on the wellbeing of staff and patients. Three examples are CareTunes [
8], UltiMo [
9] and Doplor [
10]. CareTunes transforms patient data, such as heart rate or blood pressure, into a musical piece [
8]. This can result in constant awareness for nurses of their patients’ vitality without having to listen to obtrusive alarms. When thresholds of vital signs are reached or breached, the music will be dissonant, which is impossible for the nurse not to notice. Where CareTunes is focusing on the interaction between alarms and staff, UltiMo is focusing on the recuperation of patients. The intelligent monitoring device only shows the information and alarms according to the needs of the ones present in the room [
9]. If the patient is alone, the UltiMo switches itself into silent mode. When family is present, it will give basic information, whereas when staff are present, it shows all the information. Doplor is an ambient wall painting which measures the noise level of the department and translates this information into a painting [
10]. The shown information makes the medical staff aware of the sounds and behavioral patterns that cause noise.
Momo Medical strives for patient safety through technology [
11]. The Pressure Ulcer Prevention helps the nurse to take preventive action at the right time. At first, it was meant to notify the nurse directly when action was needed, but the company discovered that this would be annoying for the staff since there is already significant alarm pressure [
12]. Therefore, a display ring was implemented, which visualizes the data from the sensor plate and gives the nurse insights into how much time is left until the next repositioning action. To visualize the information, the ring slowly fills up, and after three quarters, the ring turns yellow.
Except for related work within the hospital, there is also relevant work in other professional contexts. A good example is the case study which was designed in the context of peripheral interaction and focused on the workflow of school teachers; ClassBeacons [
13]. The ClassBeacons, ambient lighting devices, are distributed over the classroom and show the teacher’s proximity and, thus, interaction time with each student, based on data of the teacher’s positioning and heading in the classroom. Lighting from the ClassBeacons goes from yellow, which indicates the teacher spent less time around the device, to green, which indicates the teacher spent more time around the device. The system visualizes the complex information in a simple way so it will not distract the teacher too much. During the study, the potential benefits of tracking, visualizing teacher proximity, and the user experiences of ClassBeacons were explored.
In conclusion, compared to the related work, we will be focusing on the interaction between nurses and the alarm system as inspired by Guerra’s Water Probe.
3. User Study Setup
This study consisted of two parts. In the first part, an expert review was performed to gather opinions about potential benefits and hazards of CheckMates. Three independent experts with different specialities in the field of neonatology were interviewed. In the second part of the study, four simulation sessions were held in which eight NICU nurses experienced using the CheckMates. Before presenting further details of the study methodology, we first describe the functioning of CheckMates.
3.1. CheckMates
The CheckMates are small LED displays which visualize the status of medical devices by using a color transition, see
Figure 1. We hypothesize that the transition between the two primary colors will subtly inform the nurses of relevant information, without disturbing their work.
The CheckMates used in the simulation sessions were preprogrammed to reflect device statuses using different colors as follows:
Color—a green light represents that the device is full of supplies, while blue light represents that the device is running out of supplies. A medium contrast visualization is chosen to ensure that users think about the level of green/blue. A red color might upset a parent and will fill in too much information for the nurse.
Color transition—based on the usage of the device, the green color slowly turns into blue an hour before the device runs out of supplies, see
Figure 2.
Pulsing blue—three minutes before the device runs out of supplies and the alarm will go off, the blue light starts pulsing at a low-rate to attract the nurse’s attention less calmly. Furthermore, the pulsing will stop when the water level is filled.
Placement—the CheckMates are placed on the stock of the medical device itself, so the nurse immediately know which status belonged to which device, see
Figure 1. In addition, the CheckMates will be positioned so that the pulsing is not visible to the infant.
Brightness—an appropriate amount of brightness is chosen to have a noticeable, but not distracting display. During the transition, the brightness stays the same.
3.2. Expert Review
An expert review on the CheckMates was conducted through the use of the co-constructing stories method [
14]. Three experts with a background in neonatology were involved in this review (E1 male, E2 female, E3 female). E1 is a pediatrician with a speciality in neonatology and cardiology at a Neonatal Post IC. E2 works as a nurse and implements new technologies with a speciality in alarms at a NICU department. E3 works as a nurse with a speciality in Newborn Individualized Development Care and Assessment Program (NIDCAP) and implements development-oriented care at a NICU department. All experts have between 23 and 25 years of work experience in the field of neonatology. All the interviews were held in an office setting and took about 45 minutes.
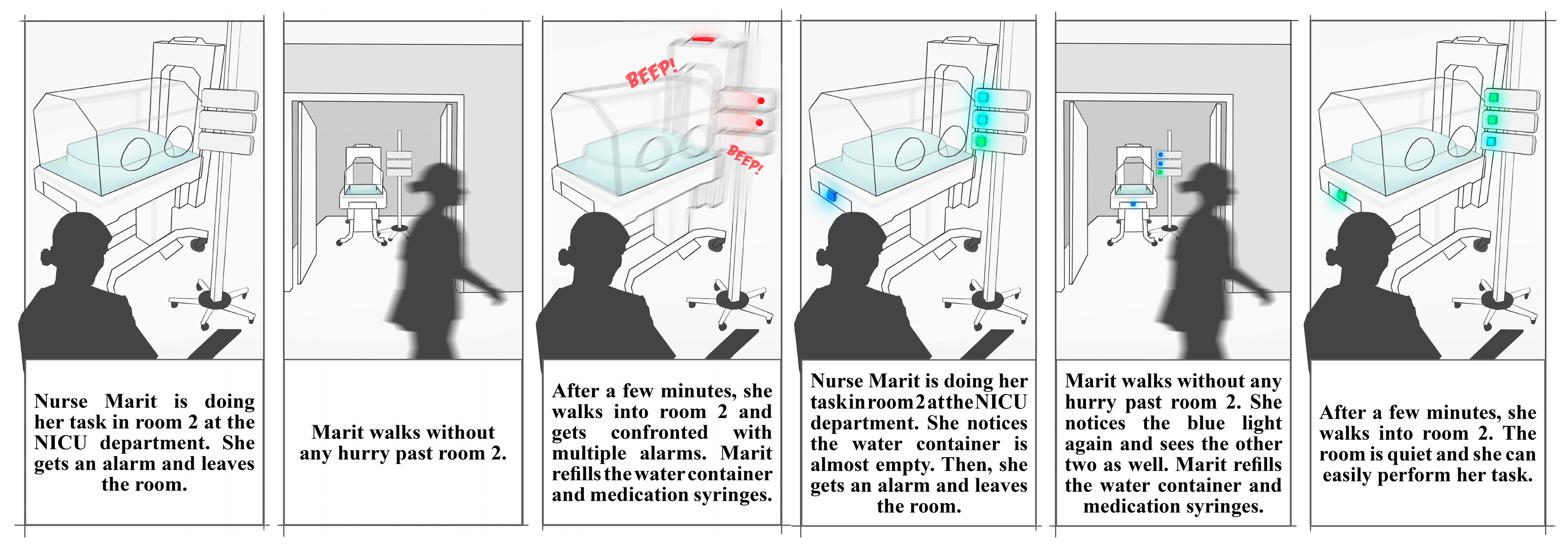
Confirming the co-constructing stories approach. In the first part of the interview a ‘sensitizing storyboard’ was shown, containing a story that had a connection with the experiences of the expert on alarms in their daily lives (see
Figure 3). They were asked if they could recognize the situation and if they could give any related examples from their own experience. In the second part of the interview, a ‘visionary storyboard’ was shown where CheckMates was implemented in the same context as the sensitizing story (see
Figure 1). Following the co-constructing stories approach, they were asked this time if they could see a potential benefit of CheckMates and how they would use the visible information in their own routines. In addition, the described experiences in the first storyboard were compared to the second storyboard.
The interviews were recorded and transcribed. A thematic analysis [
15] was conducted to the gathered textual data. Codes or keywords were defined during data analysis. This approach was chosen to gain a rich understanding of involved phenomena.
3.3. Simulation Study
A simulation study was performed to gather users’ experiences of CheckMates. As
Table 1 shows, eight nurses participated in the sessions. We recruited a diverse group of participants in terms of years of work experience. They were all employees of the NICU department of the same hospital. Nurses who worked either the day or evening shift on the day of the simulation study were able to subscribe. Per session, two nurses participated. Each session lasted about an hour. The participants were assigned to the sessions based on availability. The research took place in a twin room within the NICU department. To separate the two incubators in the twin room, a cover screen was implemented in the middle of the room. In both of the separated areas, one incubator with associated equipment and an infant-doll was placed.
Throughout the session, three different clinical scenarios were being played out by the participants. To create realistic scenarios based on actual NICU workflows, a nurse was shadowed one shift before the study “
to record behavior with a view to discovering patterns in it” [
16]. The female nurse had over 30 years of work experience in the field of neonatology. Information like time, location, interactions, and activities were noted. During the shift, questions about what she was doing, if she could tell which activities she was going to do, and if she could plan these activities ahead were asked. Afterwards, an interview was held with the nurse to get a better understanding of the workflow of the shift and how this flow was compared to other shifts. In this interview, examples of the notes were presented.
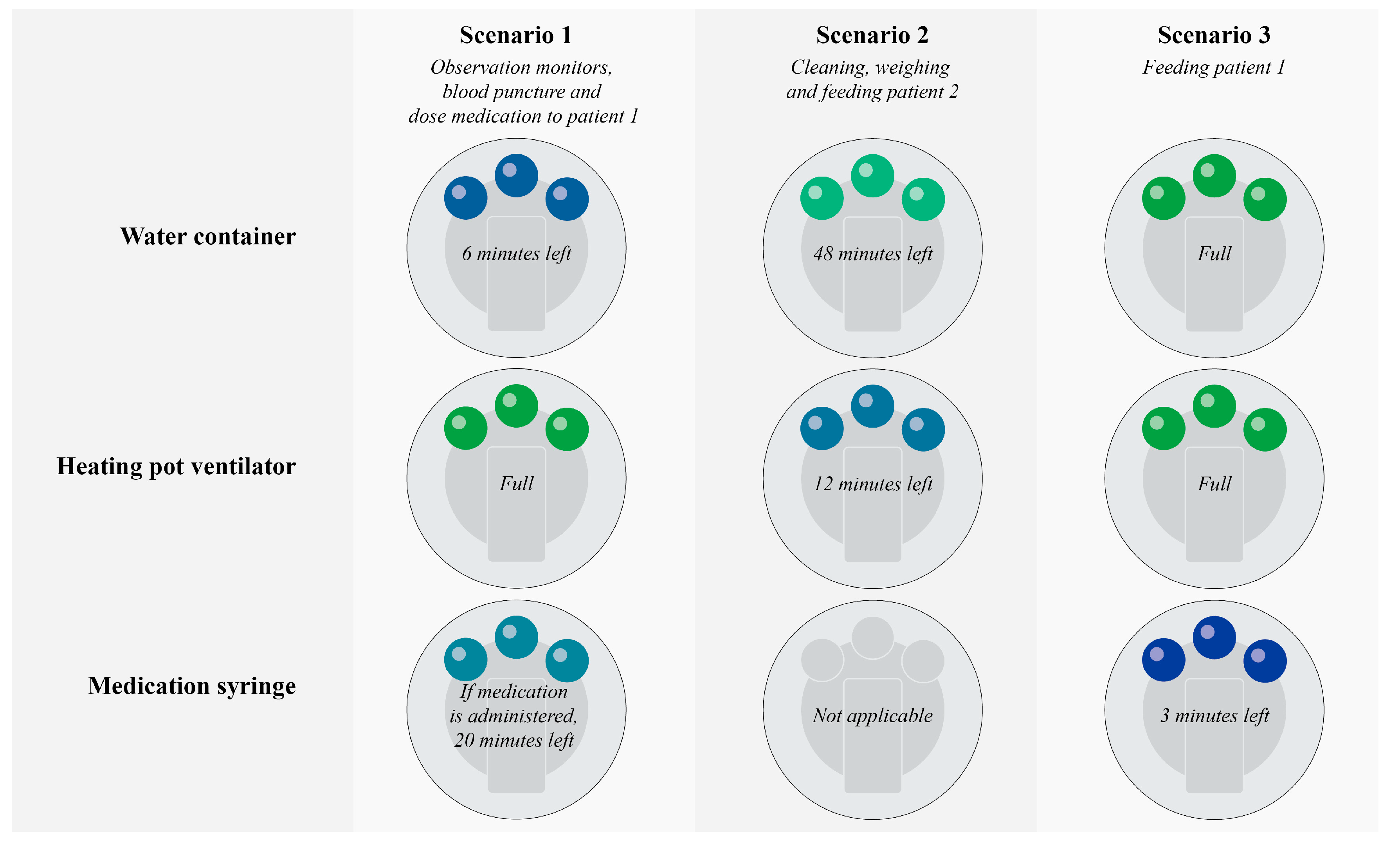
During the scenarios, four medical devices were running out of supplies (2x water container, 1x humidifying chamber of the ventilator, 1x medication syringe). The statuses were shown for each device with the use of the created CheckMates. See
Figure 4 for the scenarios.
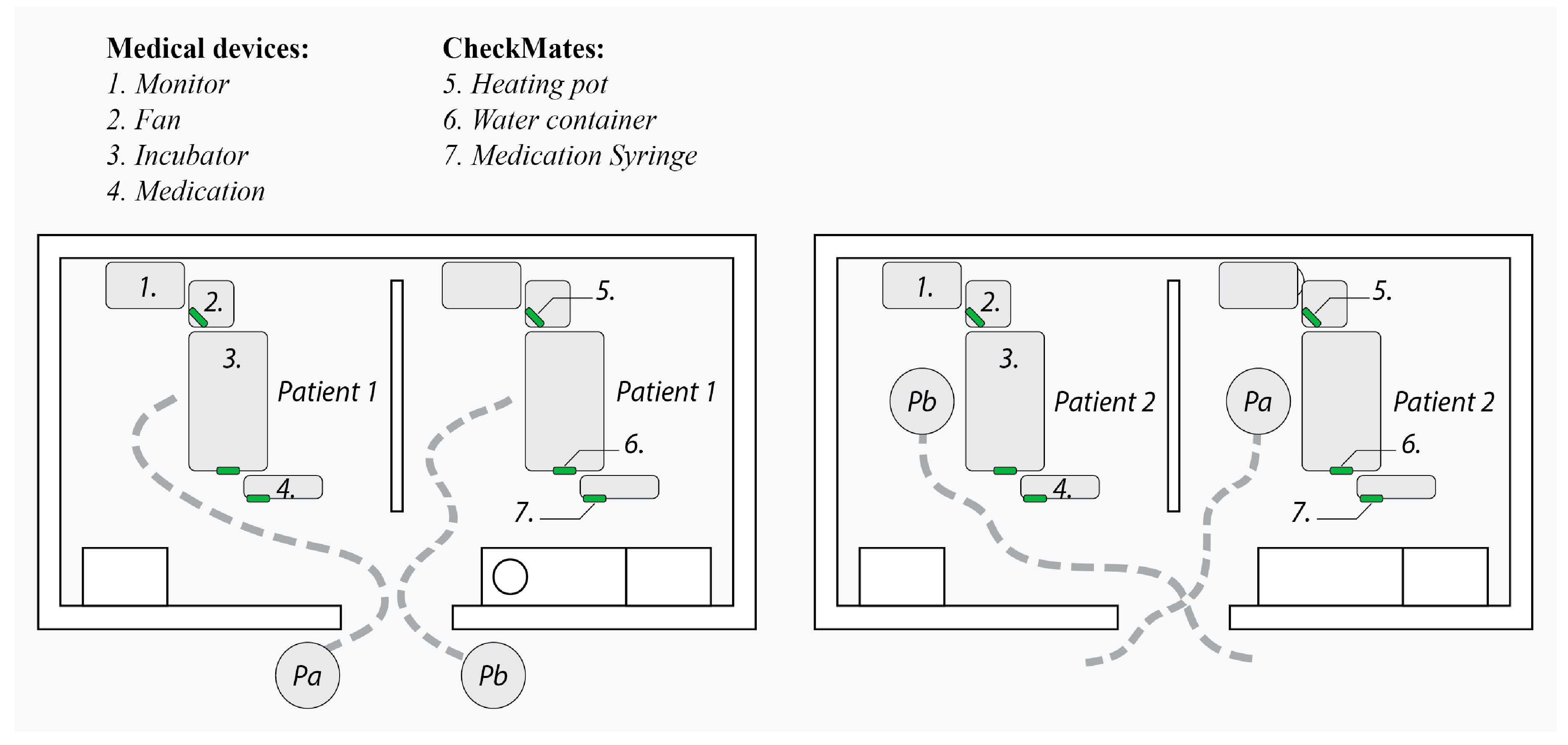
The simulation session started with a brief explanation of the research and a detailed explanation of the scenarios. Thereafter, the two participants would start each in a different part of the room, so P1a started in area 1 and P1b in area 2, see
Figure 5. Both participants were asked to perform the tasks from scenario 1, observing monitors, performing a blood puncture on the (doll-)patient and dosing medication on the patient, as described in
Figure 4. The participants were allowed to take as long as they needed.
After both nurses had enacted scenario 1, they were called to attend another patient and were asked to leave the room by the researcher. The two participants then swapped rooms and both enacted scenario 2 on fictional patient 2 for 5 to 10 minutes, which involved cleaning, weighing, and feeding the (doll-)patient. After scenario 2, they were called back to attend to patient 1 and again swapped rooms to enact scenario 3, in which they fed the patient (see
Figure 5).
Finally, we conducted a 15-minute semi-structured interview with both participants together. The interview gave insights into the experiences in the field of overview and planning for the nurses (RQ). The list of interview questions is provided in
Appendix A. The interviewer used follow-up questions (e.g., ‘why?’ and ‘Can you explain that further?’) to go into more detail when considered relevant.
Just as the expert review, the simulation interviews were recorded and transcribed verbatim. A thematic analysis [
15] was applied to the gathered textual data. Codes or keywords were generated. This approach was chosen to gain a richer understanding of phenomena.
4. Results
To answer the research questions, an expert review and simulation study were held to gather qualitative data. In the following part, we will present and discuss our findings. While the interviews were carried out in Dutch (the native language of both interviewer and interviewees), quotes presented in this section have been translated to English.
4.1. Expert Review
The expert review aimed to answer the following research question: What are the potential benefits of the implementation of CheckMates, which show device statuses, in the NICU department? After analyzing the data, we came up with two different topics; Potential benefits of the CheckMates and Perception of information.
4.1.1. Potential benefits of CheckMates
Overview and Planning: When discussing the sensitizing storyboard, which depicts the current usage of alarms in the NICU, experts recognized that when a nurse walks into a patient’s room and gets confronted with an alarm, the nurse experiences it as “very annoying and would have liked to get informed, because it is very disturbing for the patient” (E2). In addition, E3 sai:, “It is disturbing because I have to immediately quit the task I was working on. I’m walking by and had some other tasks in mind”. It is not only disturbing for nurse and patient it is also “bad for the patients’ health. The incubator will cooldown if you ignore the alarm of the water container for more than half an hour”. E2 explained why it is difficult for a nurse to keep track of the device statuses: “You will try to do it right at the beginning of your shift, but you will immediately forget about it because you start doing so many things at once … A nurse has a hundred tasks to do and refilling a device is the first task she will forget”. When introducing the visionary story, which showed the CheckMates, E1 replied by saying: “With the current system you will suddenly run out of water, and the alarm will go off, the nurse is clearing up after the alarm. With the new system, the nurse can start anticipating, e.g., I can see there is a blue light, if I wait 10 more minutes, the alarm will go off, so I have to act on it right now”. E2 thougt it is “always good to make a nurse more alert”. E3 could see how the CheckMates could help the nurse anticipate on the visualized information and what positive consequences might appear. “The nurse is already working ahead, so I don’t see any disadvantages. You do not have to rush … It will give you more space to calmly take care of your patients”. For E2, the potential benefit is that “nurses will prevent alarms and especially the ones which are not connected to a portable beeper”. She also saw how CheckMates could contribute to a better overview from activities in the past, “it may be difficult to figure out what you were doing before an alarm … the blue lights can be a mnemonic to a nurse, who already needs to remember so much” (E2).
E3 told us that “there are moments when a mother is performing kangaroo care, which means nurses do not enter the room for two hours. At that moment, we cannot see the CheckMates”. At the same time, E2 and E3 wondered if the different measurements from the whole NICU department could be overviewed at the team post, so nurses could act without being present in the room. E3: “Then it will be possible to coordinate from a distance”. A different environment than the NICU department might be interesting as well, E2 said: “The system also has a lot of potential at the Medium Care Unit. They have fewer alarms, but more patients per nurse”.
Developmental care and Empathizing: E1 indicates that developmental care is an important concept within the NICU environment. This is one of the reasons why NICU departments switch from open room care to suite care. E1 is active in both environments and said the following: “Suite care is the future for developmental care in neonatology, but the downside is that nurses cannot notice the alarms from a distance as they could with open room care”. So even though suite care is better for long term development, it will make it more difficult for nurses to react to these type of alarms. E3 confirmed this by saying: “If you miss an alarm, it could take a while before you notice it, which means the child will get exposed to the alarm all this time”. Such an alarm that indicates an empty medical device is “an extra stimulus that a premature infant actually cannot handle” (E3). That was why E1 thinks “the CheckMates fit very well within the concept of developmental care, in which we try to avoid incentives towards the child as much as possible”. E3, specialized in developmental care, saw the visionary story and replied immediately: “This will be the ideal situation! The room will be quiet and comfortable for the child, and you don’t have to quit your tasks to solve an alarm, which will be the biggest potential benefit”. These alarms are not only disturbing for the patient but also for parents. “We never thought the alarm of the water container would be so disturbing for parents. As a nurse, you do not experience this alarm as urgent, but parents do” explained E2. The nurses always tried to avoid these situations, but “nurses do not always succeed at preventing the alarms, and in our opinion, the alarm is not critical, so it could be very frustrating, and that produces stress”.
4.1.2. Perception of Information
None of the experts thought the blue lights could cause any extra stress for nurses when the visionary story was shown. E2 said: “You don’t get forced to act on the blue lights like an alarm does so you can let it slip for a while if you want to”. E3 shared a similar answer and said: “The blue lights don’t indicate it is acute, so you still have some time in which you can adapt the task into your planning”.
E1 also gave a suggestion about the design of the CheckMates. He indicated that the color transition of the CheckMates should flow at the same pace: “Every light with exactly the same color should have the same amount of time left. Otherwise, the nurse won’t know if the alarm still takes 30 minutes or 10 minutes before it goes off and she will ignore the signal”. If CheckMates share the same pace in color transition and the nurse sees “a blue light, which indicates that the alarm will go off in 10 minutes, she will understand that nobody else will get it and that she will be responsible at that moment”. Since the expert evaluation was performed before the simulation study, this suggestion was implemented in the implementation evaluated in the NICU.
4.2. Simulation Study
The simulation study aimed to answer the following research question: How is the use of Checkmates experienced with regard to nurses’ overview and planning capabilities? After analyzing the data, we came up with three different topics; Creating overview and better planning capabilities, Perception of information, and Empathizing.
4.2.1. Creating Overview and Planning Capabilities
During the interviews, seven participants said that the CheckMates could help with creating a better overview. For instance, as P1a reported: “You will have an overview in no time, which means that you can start your shift prepared”. In addition, planning capabilities were involved, for example, P1b said: “it increases the amount of time for consideration”. Some participants referred to their own experiences in the NICU and could see how the CheckMates would influence their overview: “Sometimes, when I look at the water container of the incubator, I think there is still plenty of water, and then it turns out that there was not enough water. So, I get surprised by an alarm. It will be nice if I can avoid these situations” (P3a). Some nurses mentioned that the CheckMate of the water container and medical syringe were placed in such a way, you could see the statuses by only walking through the hallway, for example P4a said: “I can see the syringe and water container from a distance, so I only have to walk by to see them. I will only notice the one on the humidifying chamber of the ventilator when I observe my devices in the room itself because it is hidden”. P1b mentioned how the information on CheckMates influenced her overview and planning. “I think I’m going to act faster before the alarms go off”. P4b had a similar opinion. “I think, as a nurse, you will fill up the water container before it is empty and that will make you avoid an alarm”. In addition, P3a said: “I will definitely use the CheckMates, because you can see the statuses in one glance”. For P3b the visualized information on the CheckMates would not contribute to a better overview or planning. She said, “I always check the statuses at the beginning of a shift, which is the way I learned it … I have an eye for detail, so it also has something to do with a personal characteristic”. However, she noticed that her colleagues often struggled with these tasks. “Sometimes, I walk into someone else’s room and notice that the syringe is almost empty. When I ask about it, the nurse in question had not seen it yet, and I will get her a new one”.
4.2.2. Perception of Information
The transition from focus to periphery and back: All participants thought the CheckMates were not annoying or bothering their work, as P4a said: “
No, it does not bother me, but it grabs my attention”. For all the participants where the CheckMates helped create a better overview, it grabbed their attention at certain moments. The CheckMates were not eye-catching when nurses were focused on certain clinical tasks, but when they took some distance or stopped performing a task, the CheckMates would attract their attention again. P1a said the following: “
When we are working in the incubator, the CheckMates do not stand out … but at a certain point, we will observe the whole environment, and at that moment, the CheckMates will catch our eye”. P4a and P4b can confirm this argument. P4b said: “
I don’t see it when I’m focused on the patient”, on which P4a said: “
The CheckMates stand out when you are observing the room”. Performing a task, like feeding a patient, is a kind of task where not a lot of attention is required. During the recording of one session, a participant was feeding patient 1 in scenario 3, when she suddenly saw the blue light of the medication syringe (see
Figure 6). In addition to this example in which the CheckMates really stood out, P3a gave another example: “
When I walk into the room, I immediately see whether the water container is running out of water or not”. However, P2a had her doubts about the CheckMates standing out or not: “
We also have other visual ways to anticipate the alarms. Will we see a CheckMate sooner? I don’t know”. P1a mentioned the color transition is too hard to read: “
It is hard to notice a difference in light blue or dark blue”, which means it was hard to see how much time was left.
Not all participants saw benefits in the CheckMates being attached to the medication syringes since in this NICU nurses receive a notification on a portable beeper 15 minutes before the medication syringe is empty. However, P1a said she did not want an extra notification: “I think that alarm would then be unnecessary, we have already so many alarms”.
Habituate: P1b said the following about the implementation of CheckMates: “I think when I’m used to the CheckMates, it could be nice. Right now, I cannot say that I’m already used to it, but I think when it will be implemented in my routine, it will be very nice”. Another participant came up with a similar statement: “It was not bothering me, I get used to it really quickly. Right now, I still have to adapt to the CheckMates, but that is not a problem” (P3a). Even though the CheckMates did not help P2a and P2b during the simulation session, P2a said the following about habituation: “We look at so many things when we walk into the room and right now the lights are new for us, so we do not see it … I think a lot of us are used to acoustic incentives and only focused on acoustic alarms, but it will be a matter of training”. On which P2b replied: “After a couple of confronting moments, you get used to it”.
4.2.3. Empathizing
When P1b compared her experiences from the simulation sessions to her daily experiences in the NICU, she replied: “In the end, it does not matter if the incubator is out of water for a few minutes, so we do not care about that, but you can avoid noise for the patients”. When P2b was asked if the CheckMates were useful for the NICU environment, she replied: “Yes! For the children, this will be very nice”. P3a involved the parents and says: “Yes, I think this will be a positive improvement because you will avoid parents who get shocked by some alarms”.
5. Discussion
This study was performed to find out what the potential benefits of the CheckMates were and if they contributed to better overview and planning capabilities.
The expert reviews showed that the CheckMates have a lot of potential when it comes to developmental care. The participants confirmed that it positively influences the situation for patient and parents during the simulation study. We noticed that the nurses showed a lot of sympathy and want to strive for a better environment for their patients. However, E3 mentioned that the light of the displays could have an impact on the premature infants. The visual system of the infants are still developing [
2] and, therefore, we should be careful with using additional light exposure in the environment.
During the study, it became clear that in a NICU environment, nurses need to be flexible. Planning ahead is difficult. The CheckMates can help the nurse anticipate on certain activities and, thus, have the ability to distribute their workload. All the experts and most of the participants during the simulation study confirmed this statement. It became clear that there are certain moments in a nurse’s shift were the CheckMates caught the nurse’s attention at the right moment. For example, every two hours a nurse will observe and take notes of the condition of the patient. During this observation, they may also observe the different statuses from the medical devices. In addition to this example, the displays also stand out when a nurse walks into the room or when she is at a distance from the incubator and observes the environment. On the other hand, the displays seem to disappear into the background when a nurse is focusing on a task, such as cleaning the patient. During such moments, the CheckMates will not attract any attention. In the results of the simulation study, multiple nurses said the CheckMates could even be seen from the hallway, except the one on the humidifying chamber of the ventilator. E3 also indicated that sometimes the curtains are closed for some more privacy or that a screen separates two families in a twin room. In those instances, none of the CheckMates will be noticeable from the hallway. An opportunity could be to make the CheckMates flexible in placement, so nurses can adjust the placement for a better overview during tasks or walking through the hallway. Or, as E2 and E3 mentioned, the different statuses could be overviewed from the whole NICU department at the team posts, so nurses could act without being present in the room.
Multiple participants mentioned that they find it was not useful to be informed about the status of the medication syringe because in the current situation nurses also get an alarm 15 minutes before the syringe is empty. However, such notifications are experienced as disturbing since there are already numerous audible notifications as P1a said. The CheckMates could alert the nurses in the periphery of their attention that they should prepare a new medication syringe, so the audible notification will be prevented, and they do not have to quit any other task they are performing directly, due to taking preemptive action.
It appeared the less experienced nurses expected to adapt to the system better than the experienced nurses. This could be because the less experienced nurses are better at adapting to new technologies or that the more experienced nurses have such ingrained routines that it might be harder for them to adapt to new technologies. However, all participants who did not notice the CheckMates during the session said it will be a matter of practice and that after an initial phase of getting accustomed to the system, it could blend in their routine easily.
We believe that the way of calmly informing the staff, as we did in this study, can also be applicable for other interactions within the field of neonatology. For example, during the shadowing study, the nurse constantly looked at the monitor while taking care of the patient. The reason behind this is to keep track of the condition of the patient and to ensure that the patient will not deteriorate. At the moment, the nurse is constantly shifting her attention from the monitor to the patient and back. This interaction could be simplified by implementing calm technology. In this way, the nurse only has to focus on the patient and receives the information from the monitor in her periphery. Not only for the field of neonatology but calm technology could also be a solution for other (medical) contexts. However, some limitations of this study need to be considered.
Limitations
While leading to new insights, the work presented in this paper naturally also had a number of limitations. First, when showing a novel design to potential users, people often tend to report positively about it. This could have caused biased responses in both studies. During the expert review, we asked if they could also discuss the hazards, but they could not find any at that moment. The simulation study indeed showed some negative responses, but they were followed up with solutions.
In this study, the concept of Checkmates was introduced in a simulation setting, rather than in the real everyday routine of NICU nurses. The actual technology should be tested in a field study, to quantify benefits for both staff and patients with regard to reduced alarm pressure and noise exposure respectively. In addition, while our work focused on the experience of nurses, future field research should have outcomes measuring the effect of showing device statuses on overview and planning capabilities.
6. Conclusions
In this paper, we presented expert opinions and simulation study of CheckMates, ambient displays visualizing the status of medical devices in a neonatal intensive care unit (NICU). Our findings show that CheckMates can help nurses to distribute their workload. This could result in the prevention of alarms and a more developmental-care oriented environment for premature infants.

 and
and 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}