Rickettsial Infections and Q Fever Amongst Febrile Patients in Bhutan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
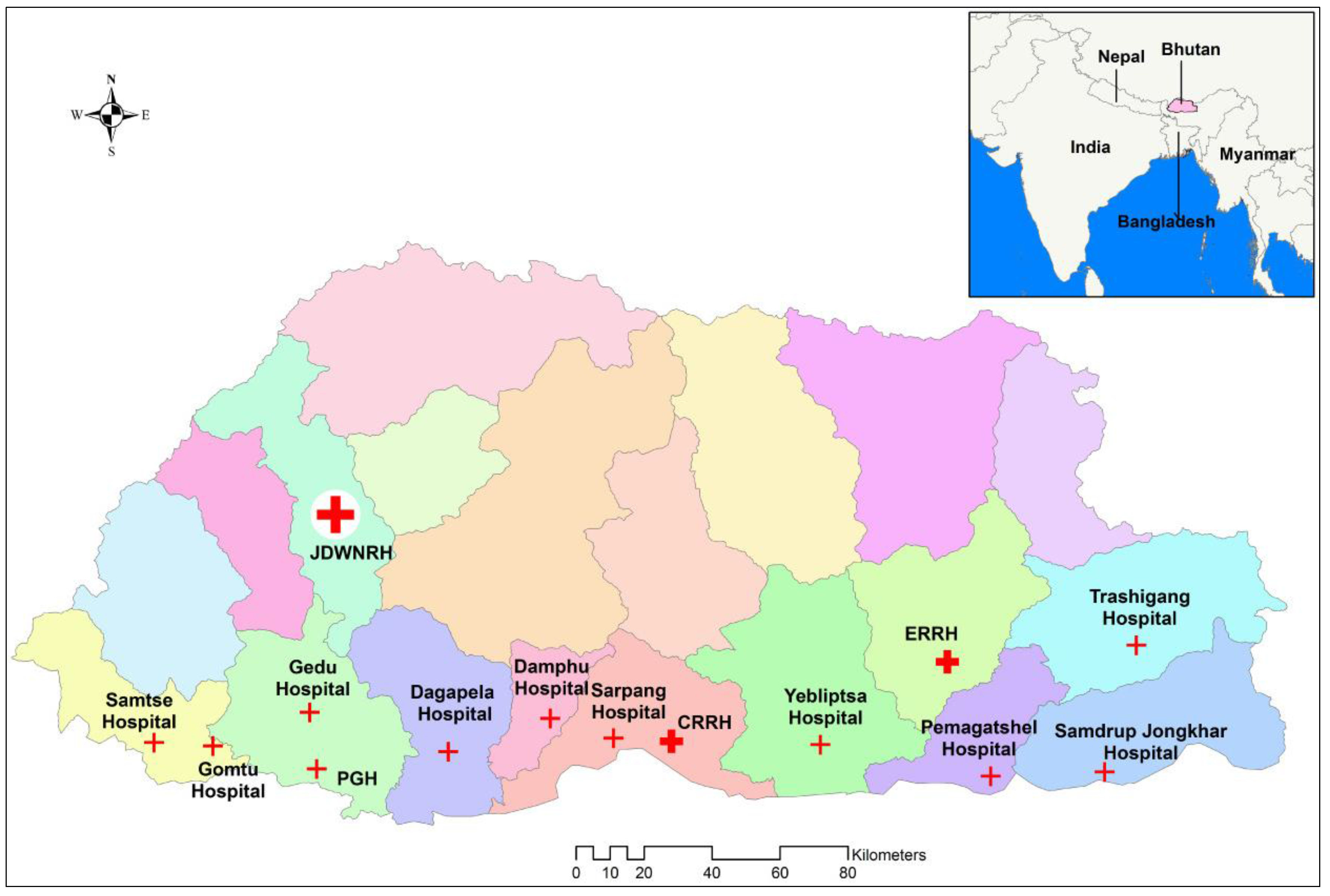
2.1. Setting and Study Sites
2.2. Study Design and Participants
2.3. Laboratory Testing
2.4. Defining Current Infections
2.5. Statistical Analysis and Determination of Associations
2.6. Ethics, Consent and Confidentiality
3. Results
3.1. Demography
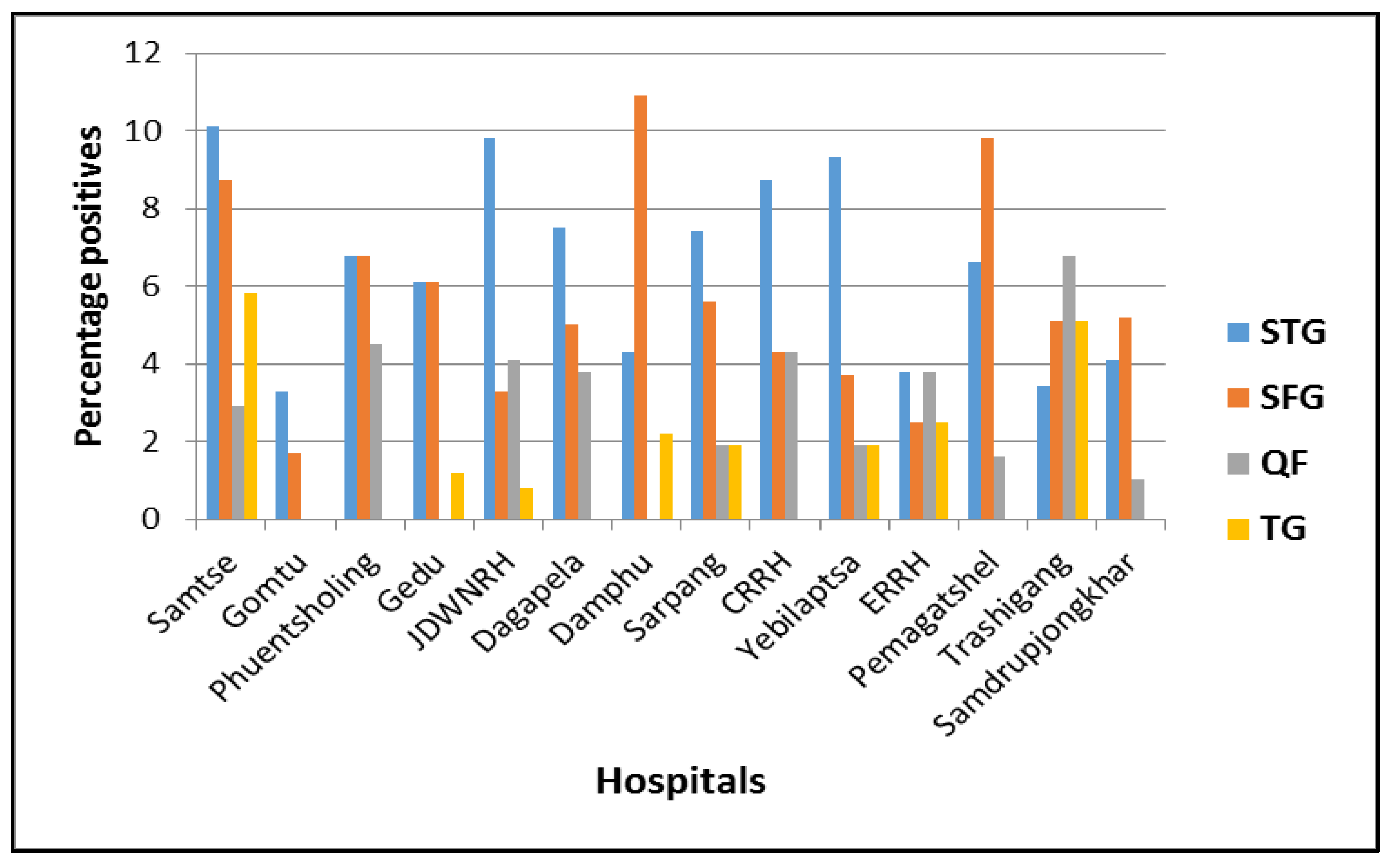
3.2. Laboratory Findings
3.3. Clinical Presentations
3.4. Environmental Factors and Association with Rickettsial Infection
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mahajan, S.K. Rickettsial diseases. J. Assoc. Physicians India 2012, 60, 37–44. [Google Scholar] [PubMed]
- Walker, D.H. Rickettsiae and rickettsial infections: The current state of knowledge. Clin. Infect. Dis. 2007, 45 (Suppl. S1), S39–S44. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Dutta, P.; Khan, A.M.; Topno, R.; Borah, J.; Chowdhury, P.; Mahanta, J. Re-emergence of scrub typhus in northeast India. Int. J. Infect. Dis. 2012, 16, e889–e890. [Google Scholar] [CrossRef] [PubMed]
- Valbuena, G. Rickettsioses: Pathogenesis, immunity, and vaccine development. Acta Méd. Costarric. 2013, 55, 48–59. [Google Scholar]
- Izzard, L.; Fuller, A.; Blacksell, S.D.; Paris, D.H.; Richards, A.L.; Aukkanit, N.; Nguyen, C.; Jiang, J.; Fenwick, S.; Day, N.P.; et al. Isolation of a novel Orientia species (O. chuto sp. nov.) from a patient infected in Dubai. J. Clin. Microbiol. 2010, 48, 4404–4409. [Google Scholar] [CrossRef] [PubMed]
- Porter, S.R.; Czaplicki, G.; Mainil, J.; Guattéo, R.; Saegerman, C. Q Fever: Current state of knowledge and perspectives of research of a neglected zoonosis. Int. J. Microbiol. 2011, 2011, 248418. [Google Scholar] [CrossRef] [PubMed]
- Hilbink, F.; Penrose, M.; Kovacova, E.; Kazar, J. Q fever is absent from New Zealand. Int. J. Epidemiol. 1993, 22, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Luce-Fedrow, A.; Mullins, K.; Kostik, A.P.; St John, H.K.; Jiang, J.; Richards, A.L. Strategies for detecting rickettsiae and diagnosing rickettsial diseases. Future Microbiol. 2015, 10, 537–564. [Google Scholar] [CrossRef] [PubMed]
- Richards, A.L. Worldwide detection and identification of new and old rickettsiae and rickettsial diseases. FEMS Immunol. Med. Microbiol. 2012, 64, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Aung, A.K.; Spelman, D.W.; Murray, R.J.; Graves, S. Rickettsial infections in Southeast Asia: Implications for local populace and febrile returned travelers. Am. J. Trop. Med. Hyg. 2014, 91, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wei, Y.H.; Yang, Y.; Ma, Y.; de Vlas, S.J.; Yao, H.W.; Huang, Y.; Ma, M.J.; Liu, K.; Li, X.N.; et al. Rapid increase of scrub typhus incidence in Guangzhou, Southern China, 2006–2014. BMC Infect. Dis. 2017, 17, 13. [Google Scholar] [CrossRef] [PubMed]
- Siraj, A.K.; Trishna, B.; Basanta, L.; Abdul, M.K.; Prafulla, D. Scrub typhus leading to acute encephalitis syndrome, Assam, India. Emerg. Infect. Dis. 2017, 23, 148–150. [Google Scholar] [CrossRef]
- Upadhyaya, B.P.; Shakya, G.; Adhikari, S.; Rijal, N.; Acharya, J.; Maharjan, L.; Marasini, B.R. Scrub typhus: An emerging neglected tropical disease in Nepal. J. Nepal Health Res. Counc. 2016, 14, 122–127. [Google Scholar] [PubMed]
- Lhazeen, K.; Department of Public Health, Thimphu, Bhutan; Tshokey, T.; University of Newcastle, Callaghan, NSW, Australia. Personal communication, 2016.
- Sonam, W.; Karma, L.; Tandin, D. Clinical Characteristics of Scrub Typhus in Gedu and Mongar (Bhutan); Public Health Laboratory: Thimphu, Bhutan, 2012. [Google Scholar]
- Tshokey, T.; Choden, T.; Sharma, R. Scrub typhus in Bhutan: A synthesis of data from 2009 to 2014. WHO South East Asia J. Public Health 2016, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Tshokey, T.; Graves, S.; Tshering, D.; Phuntsho, K.; Tshering, K.; Stenos, J. Scrub typhus outbreak in a remote primary school, Bhutan, 2014. Emerg. Infect. Dis. 2017, 23, 1412–1414. [Google Scholar] [CrossRef] [PubMed]
- Health Management and Information System. Annual Health Bulletin 2016; Minstry of Health: Thimphu, Bhutan, 2016. [Google Scholar]
- Tshokey, T.; Stenos, J.; Durrheim, D.N.; Eastwood, K.; Nguyen, C.; Graves, S.R. Seroprevalence of rickettsial infections and Q fever in Bhutan. PLoS Negl. Trop. Dis. 2017, 11, e0006107. [Google Scholar] [CrossRef] [PubMed]
- National Statistics Bureau. Bhutan at a Glance; National Statistics Bureau: Thimphu, Bhutan, 2016. [Google Scholar]
- National Statistics Bureau. Annual Dzongkhag Statistics; National Statistics Bureau: Thimphu, Bhutan, 2014. [Google Scholar]
- Armed Forces Pest Management Board. Regional Disease Vector Ecology Profile. South Central Asia; Defense Pest Management Information Analysis Centre: Washington, DC, USA, 2001; p. 219. [Google Scholar]
- Australian Rickettsial Reference Laboratory: Unlocking the Science of Rickettsiology. Available online: https://www.rickettsialab.org.au/ (accessed on 20 May 2017).
- Graves, S.; Dwyer, B.; McColl, D.; McDade, J. Flinders Island spotted fever: A newly recognised endemic focus of tick typhus in Bass Strait. Part 2. Serological investigations. Med. J. Aust. 1991, 154, 99–104. [Google Scholar] [PubMed]
- Paris, D.H.; Blacksell, S.D.; Stenos, J.; Graves, S.R.; Unsworth, N.B.; Phetsouvanh, R.; Newton, P.N.; Day, N.P. Real-time multiplex PCR assay for detection and differentiation of rickettsiae and orientiae. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Stenos, J.; Graves, S.R.; Unsworth, N.B. A highly sensitive and specific real-time PCR assay for the detection of spotted fever and typhus group Rickettsiae. Am. J. Trop. Med. Hyg. 2005, 73, 1083–1085. [Google Scholar] [PubMed]
- Stenos, J.; Graves, S.; Izzard, L. Rickettsia. In PCR for Clinical Microbiology—An Australian and International Perspective; Schuller, M., Sloots, T., James, G., Halliday, C., Carter, I., Eds.; Springer: Dordrecht, The Netherlands, 2010. [Google Scholar]
- Walker, D.H. Scrub typhus—Scientific neglect, ever-widening impact. N. Engl. J. Med. 2016, 375, 913–915. [Google Scholar] [CrossRef] [PubMed]
- Canty and Associates LLC. Bhutan—Weather Averages, 2016. Available online: http://www.weatherbase.com/weather/city.php3?c=BT# (accessed on 13 May 2017).
- Varghese, G.M.; Trowbridge, P.; Janardhanan, J.; Thomas, K.; Peter, J.V.; Mathews, P.; Abraham, O.C.; Kavitha, M.L. Clinical profile and improving mortality trend of scrub typhus in South India. Int. J. Infect. Dis. 2014, 23, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Udayan, U.; Dias, M.; Machado, S. A hospital based study of rickettsial diseases evidenced by Weil Felix test in a tertiary care hospital. CHRISMED J. Health Res. 2014, 1, 150–153. [Google Scholar] [CrossRef]
- Lai, C.-H.; Chen, Y.-H.; Lin, J.-N.; Chang, L.-L.; Chen, W.-F.; Lin, H.-H. Acute Q fever and scrub typhus, southern Taiwan. Emerg. Infect. Dis. 2009, 15, e61. [Google Scholar] [CrossRef] [PubMed]
- Thipmontree, W.; Tantibhedhyangkul, W.; Silpasakorn, S.; Wongsawat, E.; Waywa, D.; Suputtamongkol, Y. Scrub typhus in northeastern Thailand: eschar distribution, abnormal electrocardiographic findings, and predictors of fatal outcome. Am. J. Trop. Med. Hyg. 2016, 95, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, M.; Nicholson, W.L.; Roche, A.J.; Kersh, G.J.; Fitzpatrick, K.A.; Oliver, L.D.; Massung, R.F.; Morrissey, A.B.; Bartlett, J.A.; Onyango, J.J.; et al. Q fever, spotted fever group, and typhus group rickettsioses among hospitalized febrile patients in northern Tanzania. Clin. Infect. Dis. 2011, 53, e8–e15. [Google Scholar] [CrossRef] [PubMed]
- Narvencar, K.P.; Rodrigues, S.; Nevrekar, R.P.; Dias, L.; Dias, A.; Vaz, M.; Gomes, E. Scrub typhus in patients reporting with acute febrile illness at a tertiary health care institution in Goa. Indian J. Med. Res. 2012, 136, 1020–1024. [Google Scholar] [PubMed]
- Premaratna, R.; Ariyaratna, N.; Attanayake, C.; Bandara, W.; Chandrasena, N.; de Silva, H.J. Rickettsial infection among military personnel deployed in Northern Sri Lanka. BMC Infect. Dis. 2014, 14, 3864. [Google Scholar] [CrossRef] [PubMed]
- Kalal, B.S.; Puranik, P.; Nagaraj, S.; Rego, S.; Shet, A. Scrub typhus and spotted fever among hospitalised children in South India: Clinical profile and serological epidemiology. Indian J. Med. Microbiol. 2016, 34, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Su, T.-H.; Liu, C.-J.; Chen, D.-S.; Kao, J.-H. Milder clinical manifestation of scrub typhus in Kinmen, Taiwan. J. Formos. Med. Assoc. 2013, 112, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.K.; Rolain, J.-M.; Kashyap, R.; Bakshi, D.; Sharma, V.; Prasher, B.S.; Pal, L.S.; Raoult, D. Scrub typhus in Himalayas. Emerg. Infect. Dis. 2006, 12, 1590–1592. [Google Scholar] [CrossRef] [PubMed]
- Rathi, N.B.; Rathi, A.N.; Goodman, M.H.; Aghai, Z.H. Rickettsial diseases in Central India: Proposed clinical scoring system for early detection of spotted fever. Indian Pediatr. 2011, 48, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Maina, A.N.; Farris, C.M.; Odhiambo, A.; Jiang, J.; Laktabai, J.; Armstrong, J.; Holland, T.; Richards, A.L.; O’Meara, W.P. Q fever, scrub typhus, and rickettsial diseases in children, Kenya, 2011–2012. Emerg. Infect. Dis. 2016, 22, 883. [Google Scholar] [CrossRef] [PubMed]
- Thiga, J.W.; Mutai, B.K.; Eyako, W.K.; Ng’ang’a, Z.; Jiang, J.; Richards, A.L.; Waitumbi, J.N. High seroprevalence of antibodies against spotted fever and scrub typhus bacteria in patients with febrile Illness, Kenya. Emerg. Infect. Dis. 2015, 21, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Bora, T.; Chattopadhyay, S.; Jiang, J.; Richards, A.L.; Dutta, P. Seroepidemiology of rickettsial infections in Northeast India. Trans. R. Soc. Trop. Med. Hyg. 2016. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.N.; Blacksell, S.D.; Paris, D.H.; Arjyal, A.; Karkey, A.; Dongol, S.; Giri, A.; Dolecek, C.; Day, N.; Baker, S.; et al. Undifferentiated febrile illness in Kathmandu, Nepal. Am. J. Trop. Med. Hyg. 2015, 92, 875–878. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S. Scrub typhus. J. Assoc. Physicians India 2005, 53, 269. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Occupation | Age Groups in Years | |||||
|---|---|---|---|---|---|---|
| <13 | 13–24 | 25–36 | 37–48 | >48 | Overall (%) | |
| Farmer | 0 | 20 | 55 | 71 | 128 | 274 (26) |
| Office worker | 0 | 22 | 134 | 82 | 31 | 269 (26) |
| Student | 114 | 165 | 7 | 0 | 0 | 286 (27) |
| Housewife | 0 | 17 | 62 | 33 | 37 | 149 (14) |
| Unemployed | 0 | 5 | 5 | 4 | 2 | 16 (2) |
| Pre-school | 50 | 0 | 0 | 0 | 0 | 50 (5) |
| Total (%) | 164 (16) | 229 (22) | 263 (25) | 190 (18) | 198 (19) | 1044 (100) |
| Variable | No. of Positives (%) | ||||
|---|---|---|---|---|---|
| Age Group (yrs.) | STG (n = 70) | SFG (n = 46) | TG (n = 4) | SFG + TG (n = 10) | QF (n = 29) |
| <13 | 10 (14.2) | 7 (15.2) | 0 (0.0) | 1 (10.0) | 0 (0.0) |
| 13–24 | 14 (20.0) | 10 (21.7) | 1 (25.0) | 4 (40.0) | 7 (24.1) |
| 25–36 | 13 (18.6) | 16 (34.8) | 0 (0.0) | 3 (30.0) | 7 (24.1) |
| 37–48 | 20 (28.6) | 8 (17.4) | 1 (25.0) | 0 (0.0) | 6 (20.7) |
| >48 | 13 (18.6) | 5 (10.9) | 2 (50.0) | 2 (20.0) | 9 (31.1) |
| Occupation | |||||
| Farmer | 23 (32.9) | 11 (23.9) | 1 (25.0) | 6 (60.0) | 11 (37.9) |
| Office worker | 21 (30.0) | 9 (19.6) | 2 (50.0) | 1 (10.0) | 8 (27.6) |
| Student | 10 (14.3) | 14 (30.4) | 1 (25.0) | 1 (10.0) | 5 (17.2) |
| Housewife | 10 (14.3) | 8 (17.4) | 0 (0.0) | 1 (10.0) | 3 (10.4) |
| Unemployed | 1 (1.4) | 3 (6.5) | 0 (0.0) | 0 (0.0) | 2 (6.9) |
| Pre-school | 5 (7.1) | 1 (2.2) | 0 (0.0) | 1 (10.0) | 0 (0.0) |
| Signs and Symptoms | STG (n = 70) | SFG (n = 56) | TG (n = 14) | QF (n = 29) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pos | Neg | p Value | Pos | Neg | p Value | Pos | Neg | p Value | Pos | Neg | p Value | ||
| Rash | Yes | 23 | 240 | 0.126 | 11 | 252 | 0.325 | 4 | 259 | 0.769 | 8 | 255 | 0.763 |
| No | 47 | 734 | 45 | 736 | 10 | 771 | 21 | 760 | |||||
| Eschar | Yes | 31 | 9 | <0.001 * | 0 | 40 | 0.125 | 0 | 40 | 0.452 | 0 | 40 | 0.276 |
| No | 39 | 965 | 56 | 948 | 14 | 990 | 29 | 975 | |||||
| Headache | Yes | 55 | 750 | 0.763 | 48 | 757 | 0.115 | 13 | 792 | 0.158 | 22 | 783 | 0.871 |
| No | 15 | 224 | 8 | 231 | 1 | 238 | 7 | 232 | |||||
| Arthralgia | Yes | 48 | 575 | 0.116 | 37 | 586 | 0.316 | 11 | 612 | 0.147 | 19 | 604 | 0.515 |
| No | 22 | 399 | 19 | 402 | 3 | 418 | 10 | 411 | |||||
| Myalgia | Yes | 31 | 267 | 0.003 * | 17 | 281 | 0.761 | 3 | 295 | 0.551 | 5 | 293 | 0.171 |
| No | 39 | 706 | 39 | 706 | 11 | 734 | 24 | 721 | |||||
| Lymphadenopathy | Yes | 5 | 28 | 0.049 * | 2 | 31 | 0.859 | 0 | 33 | 0.496 | 1 | 32 | 0.930 |
| No | 65 | 944 | 54 | 955 | 14 | 995 | 28 | 981 | |||||
| Others | Yes | 8 | 99 | 0.736 | 10 | 97 | 0.054 | 1 | 106 | 0.700 | 1 | 106 | 0.221 |
| No | 62 | 875 | 46 | 891 | 13 | 924 | 28 | 909 | |||||
| Signs and Symptoms | Diagnosis | p Value | ||
|---|---|---|---|---|
| Rickettsioses | Non-Rickettsioses | |||
| Rash | Yes | 43 | 220 | 0.559 |
| No | 116 | 665 | ||
| Eschar | Yes | 31 | 9 | <0.001 * |
| No | 128 | 876 | ||
| Headache | Yes | 129 | 676 | 0.190 |
| No | 30 | 209 | ||
| Arthralgia | Yes | 106 | 517 | 0.051 |
| No | 53 | 368 | ||
| Myalgia | Yes | 53 | 245 | 0.149 |
| No | 106 | 639 | ||
| Lymphadenopathy | Yes | 8 | 25 | 0.145 |
| No | 151 | 858 | ||
| Others | Yes | 19 | 140 | 0.443 |
| No | 140 | 797 | ||
| Variables | OR | 95% CI | p Value | |
|---|---|---|---|---|
| Age group (yrs.) | ||||
| Children | Ref. | |||
| 13–24 | 1.00 | 0.43 | 2.32 | 0.995 |
| 25–36 | 0.80 | 0.34 | 1.87 | 0.608 |
| 37–48 | 1.81 | 0.82 | 3.99 | 0.140 |
| Above 48 | 1.08 | 0.46 | 2.54 | 0.856 |
| Gender | ||||
| Male | Ref. | |||
| Female | 0.88 | 0.54 | 1.42 | 0.596 |
| Occupation | ||||
| Farmer | Ref. | |||
| Office worker | 1.08 | 0.58 | 2.00 | 0.802 |
| Student | 0.43 | 0.20 | 0.93 | 0.031 * |
| Housewife | 0.85 | 0.39 | 1.86 | 0.683 |
| Unemployed | 0.79 | 0.20 | 6.26 | 0.821 |
| Pre-school | 1.31 | 0.47 | 3.66 | 0.604 |
| District | ||||
| Samtse | Ref. | |||
| Chukha | 0.92 | 0.37 | 2.30 | 0.862 |
| Thimphu | 1.45 | 0.59 | 3.59 | 0.416 |
| Dagana | 1.08 | 0.37 | 3.16 | 0.887 |
| Tsirang | 0.61 | 0.13 | 2.91 | 0.532 |
| Sarpang | 1.19 | 0.49 | 2.93 | 0.699 |
| Zhemgang | 1.36 | 0.43 | 4.27 | 0.597 |
| Mongar | 0.52 | 0.14 | 1.98 | 0.337 |
| Pemagatshel | 0.94 | 0.28 | 3.17 | 0.915 |
| Trashigang | 0.47 | 0.10 | 2.24 | 0.341 |
| Samdrupjongkhar | 0.57 | 0.17 | 1.92 | 0.367 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tshokey, T.; Stenos, J.; Durrheim, D.N.; Eastwood, K.; Nguyen, C.; Vincent, G.; Graves, S.R. Rickettsial Infections and Q Fever Amongst Febrile Patients in Bhutan. Trop. Med. Infect. Dis. 2018, 3, 12. https://doi.org/10.3390/tropicalmed3010012
Tshokey T, Stenos J, Durrheim DN, Eastwood K, Nguyen C, Vincent G, Graves SR. Rickettsial Infections and Q Fever Amongst Febrile Patients in Bhutan. Tropical Medicine and Infectious Disease. 2018; 3(1):12. https://doi.org/10.3390/tropicalmed3010012
Chicago/Turabian StyleTshokey, Tshokey, John Stenos, David N. Durrheim, Keith Eastwood, Chelsea Nguyen, Gemma Vincent, and Stephen R. Graves. 2018. "Rickettsial Infections and Q Fever Amongst Febrile Patients in Bhutan" Tropical Medicine and Infectious Disease 3, no. 1: 12. https://doi.org/10.3390/tropicalmed3010012