
False Positivity of Anti-SARS-CoV-2 Antibodies in Patients with Acute Tropical Diseases in Thailand

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
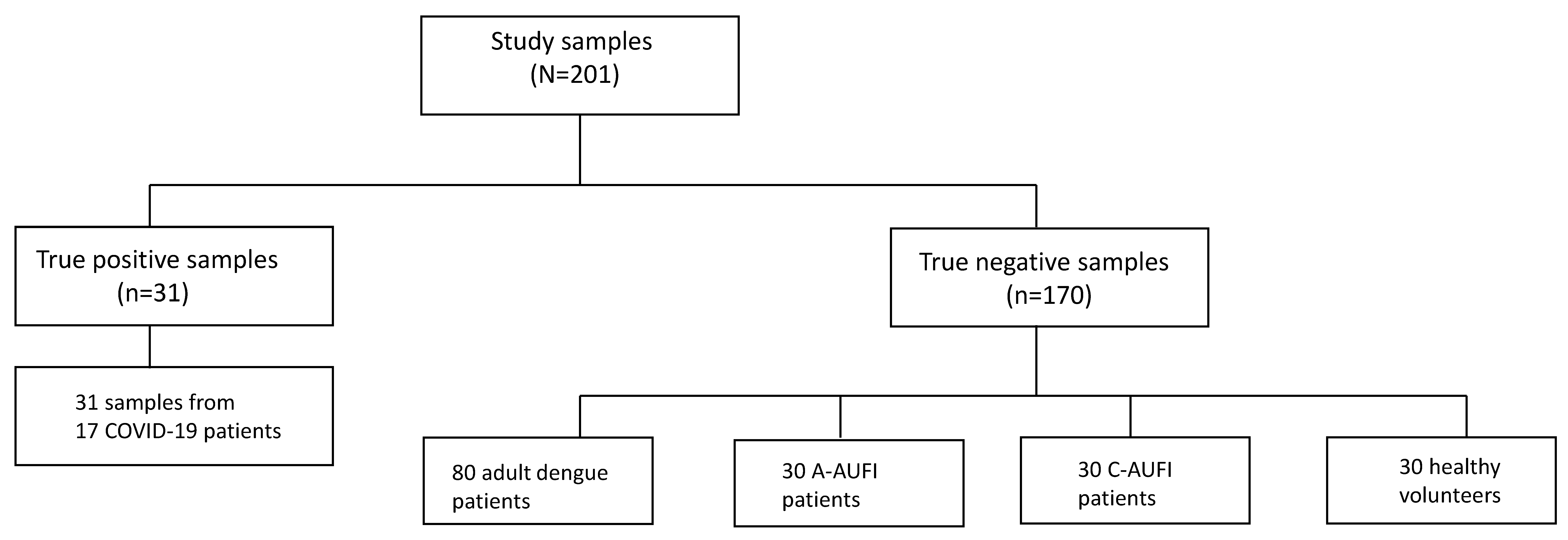
2.1. Serum Samples
2.2. ELISA Assays
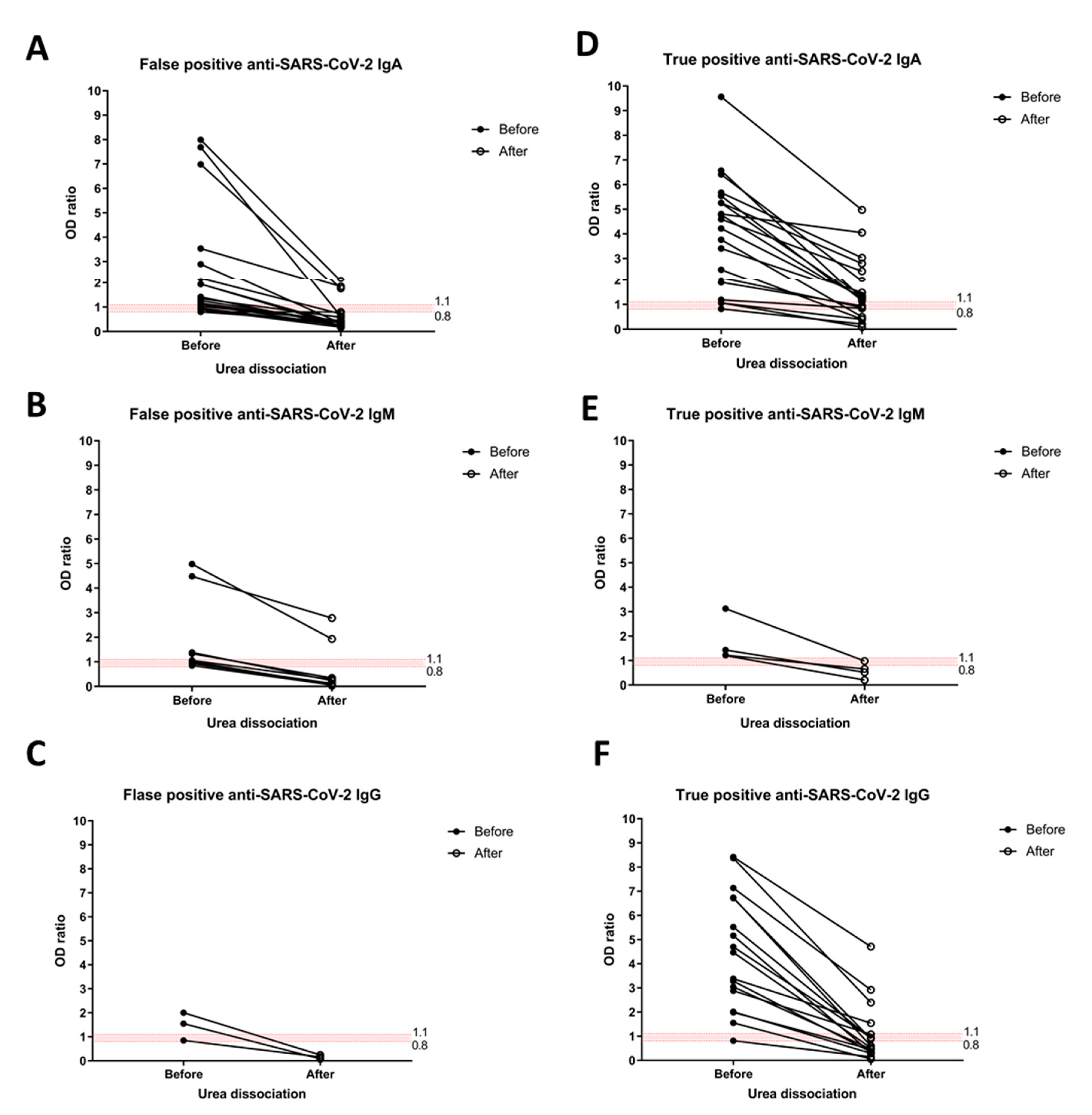
2.3. Urea Dissociation Test
2.4. Ethics Statement
2.5. Statistical Analysis
3. Results
3.1. Characteristics of COVID-19 and Acute Tropical Disease Patients
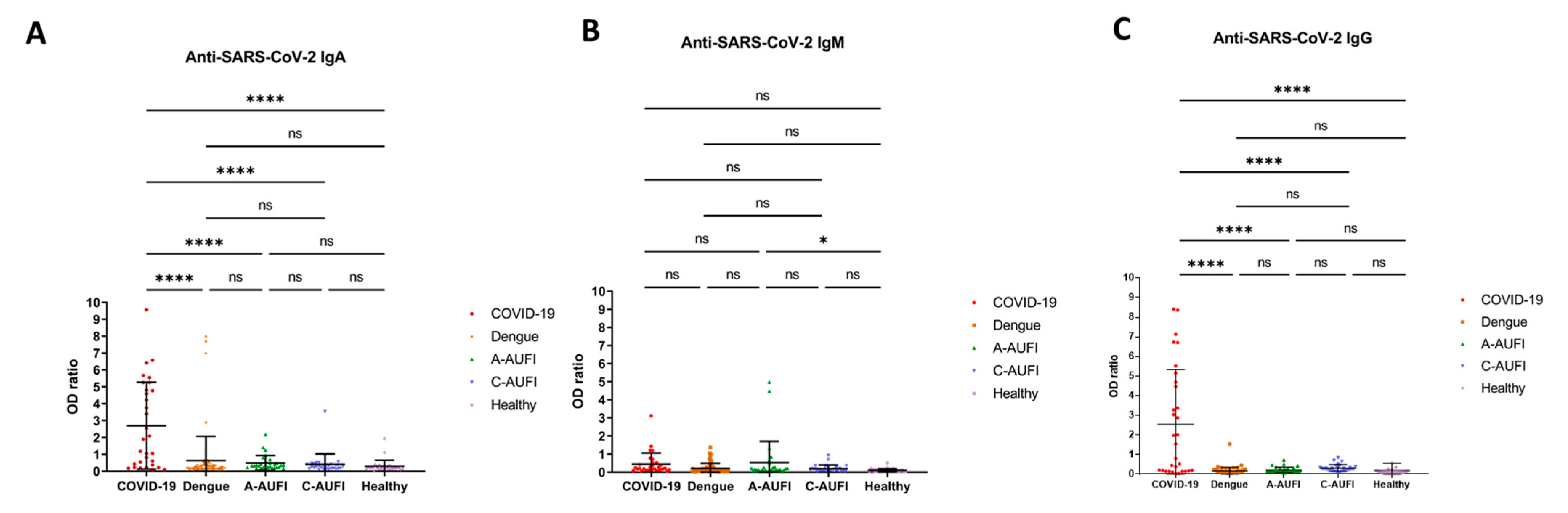
3.2. False Positive, Sensitivity, and Specificity Anti-SARS-CoV-2 Serology
3.3. Anti-SARS-CoV-2 Serology after Urea Dissociation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. The China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Muller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, D.S.Y.; Fragkou, P.C.; Schweitzer, V.A.; Chemaly, R.F.; Moschopoulos, C.D.; Skevaki, C. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Respiratory Viruses (ESGREV). How to interpret and use COVID-19 serology and immunology tests. Clin. Microbiol. Infect. 2021, 27, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Jacot, D.; Moraz, M.; Coste, A.T.; Aubry, C.; Sacks, J.A.; Greub, G.; Croxatto, A. Evaluation of sixteen ELISA SARS-CoV-2 serological tests. J. Clin. Virol. 2021, 142, 104931. [Google Scholar] [CrossRef]
- Lutalo, T.; Nalumansi, A.; Olara, D.; Kayiwa, J.; Ogwang, B.; Odwilo, E.; Watera, C.; Balinandi, S.; Kiconco, J.; Nakaseegu, J.; et al. Evaluation of the performance of 25 SARS-CoV-2 serological rapid diagnostic tests using a reference panel of plasma specimens at the Uganda Virus Research Institute. Int. J. Infect. Dis. 2021, 112, 281–287. [Google Scholar] [CrossRef]
- Shibata, S.; Ishiguro, T.; Kobayashi, Y.; Koike, M.; Numano, T.; Shimizu, Y.; Takayanagi, N. High incidence of false-positive results of IgG antibody against SARS-CoV-2 with rapid immunochromatographic antibody test due to human common cold coronavirus infection. Respir. Med. Case Rep. 2020, 31, 101180. [Google Scholar] [CrossRef]
- Lv, H.; Wu, N.C.; Tsang, O.T.; Yuan, M.; Perera, R.; Leung, W.S.; So, R.T.Y.; Chan, J.M.C.; Yip, G.K.; Chik, T.S.H.; et al. Cross-reactive Antibody Response between SARS-CoV-2 and SARS-CoV Infections. Cell Rep. 2020, 31, 107725. [Google Scholar] [CrossRef]
- Ye, Q.; Zhang, T.; Lu, D. Potential false-positive reasons for SARS-CoV-2 antibody testing and its solution. J. Med. Virol. 2021, 93, 4242–4246. [Google Scholar] [CrossRef]
- Kharlamova, N.; Dunn, N.; Bedri, S.K.; Jerling, S.; Almgren, M.; Faustini, F.; Gunnarsson, I.; Ronnelid, J.; Pullerits, R.; Gjertsson, I.; et al. False Positive Results in SARS-CoV-2 Serological Tests for Samples from Patients with Chronic Inflammatory Diseases. Front. Immunol. 2021, 12, 666114. [Google Scholar] [CrossRef]
- Liu, W.; Long, X.; Wan, K.; Yin, M.; Yin, Y.; Zhang, B.; Li, L.; Song, Y. The endogenous factors affecting the detection of serum SARS-CoV-2 IgG/IgM antibodies by ELISA. J. Med. Virol. 2022, 94, 1976–1982. [Google Scholar] [CrossRef]
- Marcolino, P.T.; Silva, D.A.; Leser, P.G.; Camargo, M.E.; Mineo, J.R. Molecular markers in acute and chronic phases of human toxoplasmosis: Determination of immunoglobulin G avidity by Western blotting. Clin. Diagn. Lab. Immunol. 2000, 7, 384–389. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Du, Q.; Guo, B.; Mu, D.; Lu, X.; Ma, Q.; Guo, Y.; Fang, L.; Zhang, B.; Zhang, G.; et al. A Method to Prevent SARS-CoV-2 IgM False Positives in Gold Immunochromatography and Enzyme-Linked Immunosorbent Assays. J. Clin. Microbiol. 2020, 58, e00375-20. [Google Scholar] [CrossRef] [Green Version]
- Latiano, A.; Tavano, F.; Panza, A.; Palmieri, O.; Niro, G.A.; Andriulli, N.; Latiano, T.; Corritore, G.; Gioffreda, D.; Gentile, A.; et al. False-positive results of SARS-CoV-2 IgM/IgG antibody tests in sera stored before the 2020 pandemic in Italy. Int. J. Infect. Dis. 2021, 104, 159–163. [Google Scholar] [CrossRef]
- Yan, G.; Lee, C.K.; Lam, L.T.M.; Yan, B.; Chua, Y.X.; Lim, A.Y.N.; Phang, K.F.; Kew, G.S.; Teng, H.; Ngai, C.H.; et al. Covert COVID-19 and false-positive dengue serology in Singapore. Lancet Infect. Dis. 2020, 20, 536. [Google Scholar] [CrossRef] [Green Version]
- Lustig, Y.; Keler, S.; Kolodny, R.; Ben-Tal, N.; Atias-Varon, D.; Shlush, E.; Gerlic, M.; Munitz, A.; Doolman, R.; Asraf, K.; et al. Potential Antigenic Cross-reactivity Between Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Dengue Viruses. Clin. Infect. Dis. 2021, 73, e2444–e2449. [Google Scholar] [CrossRef]
- Spinicci, M.; Bartoloni, A.; Mantella, A.; Zammarchi, L.; Rossolini, G.M.; Antonelli, A. Low risk of serological cross-reactivity between dengue and COVID-19. Mem. Inst. Oswaldo Cruz. 2020, 115, e200225. [Google Scholar] [CrossRef]
- Santoso, M.S.; Masyeni, S.; Haryanto, S.; Yohan, B.; Hibberd, M.L.; Sasmono, R.T. Assessment of dengue and COVID-19 antibody rapid diagnostic tests cross-reactivity in Indonesia. Virol. J. 2021, 18, 54. [Google Scholar] [CrossRef]
- Nath, H.; Mallick, A.; Roy, S.; Sukla, S.; Basu, K.; De, A.; Biswas, S. Archived dengue serum samples produced false-positive results in SARS-CoV-2 lateral flow-based rapid antibody tests. J. Med. Microbiol. 2021, 70, 001369. [Google Scholar] [CrossRef]
- Faccini-Martinez, A.A.; Rivero, R.; Garay, E.; Garcia, A.; Mattar, S.; Botero, Y.; Galeano, K.; Miranda, J.; Martinez, C.; Guzman, C.; et al. Serological cross-reactivity using a SARS-CoV-2 ELISA test in acute Zika virus infection, Colombia. Int. J. Infect. Dis. 2020, 101, 191–193. [Google Scholar] [CrossRef]
- Navarro, J.C.; Arrivillaga-Henriquez, J.; Salazar-Loor, J.; Rodriguez-Morales, A.J. COVID-19 and dengue, co-epidemics in Ecuador and other countries in Latin America: Pushing strained health care systems over the edge. Travel Med. Infect. Dis. 2020, 37, 101656. [Google Scholar] [CrossRef]
- Lorenz, C.; Azevedo, T.S.; Chiaravalloti-Neto, F. COVID-19 and dengue fever: A dangerous combination for the health system in Brazil. Travel Med. Infect. Dis. 2020, 35, 101659. [Google Scholar] [CrossRef]
- Luvira, V.; Silachamroon, U.; Piyaphanee, W.; Lawpoolsri, S.; Chierakul, W.; Leaungwutiwong, P.; Thawornkuno, C.; Wattanagoon, Y. Etiologies of Acute Undifferentiated Febrile Illness in Bangkok, Thailand. Am. J. Trop. Med. Hyg. 2019, 100, 622–629. [Google Scholar] [CrossRef] [Green Version]
- Kavirayani, V.; Madiyal, M.; Aroor, S.; Chhabra, S. Clinical profile and role of serology in pediatric acute febrile illness: Experience from a tertiary care hospital in South India. Clin. Epidemiol. Glob. Health 2021, 12, 100898. [Google Scholar] [CrossRef]
- Wayne, W.D. Biostatistics—A Foundations for Analysis in the Health Sciences, 6th ed.; Wiley & Sons: New York, NY, USA, 1995. [Google Scholar]
- Tandhavanant, S.; Koosakunirand, S.; Kaewarpai, T.; Piyaphanee, W.; Leaungwutiwong, P.; Luvira, V.; Chantratita, N. Longitudinal analysis to characterize classes and subclasses of antibody responses to recombinant receptor-binding protein (RBD) of SARS-CoV-2 in COVID-19 patients in Thailand. PLoS ONE 2021, 16, e0255796. [Google Scholar] [CrossRef]
- Sabchareon, A.; Sirivichayakul, C.; Limkittikul, K.; Chanthavanich, P.; Suvannadabba, S.; Jiwariyavej, V.; Dulyachai, W.; Pengsaa, K.; Margolis, H.S.; Letson, G.W. Dengue infection in children in Ratchaburi, Thailand: A cohort study. I. Epidemiology of symptomatic acute dengue infection in children, 2006-2009. PLoS ONE Negl. Trop. Dis. 2012, 6, e1732. [Google Scholar] [CrossRef] [Green Version]
- Beavis, K.G.; Matushek, S.M.; Abeleda, A.P.F.; Bethel, C.; Hunt, C.; Gillen, S.; Moran, A.; Tesic, V. Evaluation of the EUROIMMUN Anti-SARS-CoV-2 ELISA Assay for detection of IgA and IgG antibodies. J. Clin. Virol. 2020, 129, 104468. [Google Scholar] [CrossRef]
- Gaddis, M.L. Statistical methodology: IV. Analysis of variance, analysis of covariance, and multivariate analysis of variance. Acad. Emerg. Med. 1998, 5, 258–265. [Google Scholar] [CrossRef]
- Vongpunsawad, S.; Intharasongkroh, D.; Thongmee, T.; Poovorawan, Y. Seroprevalence of antibodies to dengue and chikungunya viruses in Thailand. PLoS ONE 2017, 12, e0180560. [Google Scholar] [CrossRef] [Green Version]
- El-Qushayri, A.E.; Kamel, A.M.A.; Reda, A.; Ghozy, S. Does dengue and COVID-19 co-infection have worse outcomes? A systematic review of current evidence. Rev. Med. Virol. 2022, 2022, e2339. [Google Scholar] [CrossRef]
- Indini, A.; Cattaneo, M.; Ghidini, M.; Rijavec, E.; Bareggi, C.; Galassi, B.; Gambini, D.; Ceriani, R.; Ceriotti, F.; Berti, E.; et al. Triage process for the assessment of coronavirus disease 2019-positive patients with cancer: The ONCOVID prospective study. Cancer 2021, 127, 1091–1101. [Google Scholar] [CrossRef]
- Candoni, A.; Petruzzellis, G.; Sperotto, A.; Andreotti, V.; Giavarra, M.; Corvaja, C.; Minisini, A.; Comuzzi, C.; Tascini, C.; Fanin, R.; et al. Detection of SARS-CoV-2 infection prevalence in 860 cancer patients with a combined screening procedure including triage, molecular nasopharyngeal swabs and rapid serological test. A report from the first epidemic wave. PLoS ONE 2022, 17, e0262784. [Google Scholar] [CrossRef] [PubMed]
- Shurrab, F.M.; Al-Sadeq, D.W.; Amanullah, F.H.; Al-Absi, E.S.; Qotba, H.; Yassine, H.M.; Abu-Raddad, L.J.; Nasrallah, G.K. Low risk of serological cross-reactivity between the dengue virus and SARS-CoV-2 IgG antibodies using advanced detection assays. Intervirology 2022, 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Silvestre, O.M.; Costa, L.R.; Lopes, B.V.R.; Barbosa, M.R.; Botelho, K.K.P.; Albuquerque, K.L.C.; Souza, A.G.S.; Coelho, L.A.; de Oliveira, A.J.; Barantini, C.B.; et al. Previous Dengue Infection and Mortality in Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 73, e1219–e1221. [Google Scholar] [CrossRef] [PubMed]
- Nath, H.; Mallick, A.; Roy, S.; Sukla, S.; Biswas, S. Computational modelling supports that dengue virus envelope antibodies can bind to SARS-CoV-2 receptor binding sites: Is pre-exposure to dengue virus protective against COVID-19 severity? Comput. Struct. Biotechnol. J. 2021, 19, 459–466. [Google Scholar] [CrossRef]
- Emmerich, P.; Murawski, C.; Ehmen, C.; von Possel, R.; Pekarek, N.; Oestereich, L.; Duraffour, S.; Pahlmann, M.; Struck, N.; Eibach, D.; et al. Limited specificity of commercially available SARS-CoV-2 IgG ELISAs in serum samples of African origin. Trop. Med. Int. Health 2021, 26, 621–631. [Google Scholar] [CrossRef]
- Prapinjumrune, C.; Prucktrakul, C.; Sooktonglarng, T.; Thongprasom, K. Serum antinuclear antibody in adult Thais. Gerodontology 2017, 34, 86–89. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Group | N | False Positive Anti-SARS-CoV-2 | ||
|---|---|---|---|---|
| IgA (%) | IgM (%) | IgG (%) | ||
| Adult tropical diseases | 110 | 14 (12.7%) | 8 (7.3%) | 1 (0.9%) |
| -Dengue | 80 | 9 (11.3%) | 4 (5%) | 1 (1.3%) |
| -Adult-AUFI | 30 | 5 (16.7%) | 4 (13.3%) | 0 |
| Children with non-dengue AUFI | 30 | 2 (6.7%) | 1 (3.3%) | 1 (3.3%) |
| Healthy | 30 | 2 (6.7%) | 0 | 1 (3.3%) |
| No. | Group | Diagnosis | Anti-Dengue | Anti-SARS-CoV-2 | |||
|---|---|---|---|---|---|---|---|
| IgM | IgG | IgA | IgM | IgG | |||
| 6 | Adult AUFI | Dengue | positive | positive | borderline | negative | negative |
| 19 | Adult AUFI | Leptospirosis | negative | positive | negative | positive | negative |
| 22 | Adult AUFI | Influenza | negative | positive | positive | negative | negative |
| 26 | Adult AUFI | Dengue | positive | positive | negative | borderline | negative |
| 32 | Adult AUFI | Murine typhus | negative | positive | borderline | negative | negative |
| 41 | Adult AUFI | Dengue | negative | positive | positive | negative | negative |
| 48 | Adult AUFI | Dengue | negative | positive | negative | positive | negative |
| 51 | Adult AUFI | Dengue | positive | positive | positive | negative | negative |
| 54 | Adult AUFI | Leptospirosis | negative | positive | negative | positive | negative |
| 59 | Adult AUFI | Murine typhus | negative | positive | borderline | negative | negative |
| 72 | Adult AUFI | Dengue | positive | positive | positive | negative | negative |
| 84 | Adult AUFI | Dengue | negative | positive | positive | negative | negative |
| 87 | Adult AUFI | Dengue | positive | positive | positive | negative | negative |
| 88 | Adult AUFI | Murine typhus | negative | positive | negative | positive | negative |
| 93 | Adult AUFI | Dengue | positive | positive | negative | borderline | negative |
| 94 | Adult AUFI | Murine typhus | negative | positive | positive | borderline | negative |
| 95 | Adult AUFI | Dengue | positive | positive | negative | borderline | negative |
| 97 | Adult AUFI | Dengue | positive | positive | borderline | negative | negative |
| 104 | Adult AUFI | Dengue | positive | positive | positive | negative | positive |
| 106 | Adult AUFI | Murine typhus | negative | positive | positive | negative | negative |
| 109 | Adult AUFI | Dengue | positive | positive | positive | negative | negative |
| 113 | Children with AUFI | Bronchitis | negative | negative | negative | negative | borderline |
| 115 | Children with AUFI | Acute tonsillitis | negative | negative | negative | borderline | negative |
| 130 | Children with AUFI | Acute pharyngitis | negative | negative | borderline | negative | negative |
| 132 | Children with AUFI | Pharyngitis | negative | negative | positive | negative | negative |
| 184 | Healthy | Healthy | negative | positive | positive | negative | positive |
| 187 | Healthy | Healthy | negative | positive | positive | negative | negative |
| Anti-SARS-CoV-2 ELISA | Sensitivity (%) | Specificity (%) |
|---|---|---|
| IgA | 64.5 | 89.4 |
| IgM | 12.9 | 94.7 |
| IgG | 54.8 | 98.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luvira, V.; Leaungwutiwong, P.; Thippornchai, N.; Thawornkuno, C.; Chatchen, S.; Chancharoenthana, W.; Tandhavanant, S.; Muangnoicharoen, S.; Piyaphanee, W.; Chantratita, N. False Positivity of Anti-SARS-CoV-2 Antibodies in Patients with Acute Tropical Diseases in Thailand. Trop. Med. Infect. Dis. 2022, 7, 132. https://doi.org/10.3390/tropicalmed7070132
Luvira V, Leaungwutiwong P, Thippornchai N, Thawornkuno C, Chatchen S, Chancharoenthana W, Tandhavanant S, Muangnoicharoen S, Piyaphanee W, Chantratita N. False Positivity of Anti-SARS-CoV-2 Antibodies in Patients with Acute Tropical Diseases in Thailand. Tropical Medicine and Infectious Disease. 2022; 7(7):132. https://doi.org/10.3390/tropicalmed7070132
Chicago/Turabian StyleLuvira, Viravarn, Pornsawan Leaungwutiwong, Narin Thippornchai, Charin Thawornkuno, Supawat Chatchen, Wiwat Chancharoenthana, Sarunporn Tandhavanant, Sant Muangnoicharoen, Watcharapong Piyaphanee, and Narisara Chantratita. 2022. "False Positivity of Anti-SARS-CoV-2 Antibodies in Patients with Acute Tropical Diseases in Thailand" Tropical Medicine and Infectious Disease 7, no. 7: 132. https://doi.org/10.3390/tropicalmed7070132