
Artificial Intelligence in Pharmaceutical and Healthcare Research
by
 , ,
, ,
Subrat Kumar Bhattamisra
1,*,
Priyanka Banerjee
2,
Pratibha Gupta
2,
Jayashree Mayuren
3,
Susmita Patra
2 and
Mayuren Candasamy
4 1
Department of Pharmacology, GITAM School of Pharmacy, GITAM (Deemed to Be University), Visakhapatnam 530045, Andhra Pradesh, India
2
Department of Pharmaceutical Technology, School of Medical Sciences, Adamas University, Kolkata 700126, West Bengal, India
3
Department of Pharmaceutical Technology, School of Pharmacy, International Medical University, Kuala Lumpur 57000, Malaysia
4
Department of Life Sciences, School of Pharmacy, International Medical University, Kuala Lumpur 57000, Malaysia
*
Author to whom correspondence should be addressed.
Big Data Cogn. Comput. 2023, 7(1), 10; https://doi.org/10.3390/bdcc7010010
Submission received: 15 December 2022
/
Revised: 5 January 2023
/
Accepted: 9 January 2023
/
Published: 11 January 2023
Abstract
:Artificial intelligence (AI) is a branch of computer science that allows machines to work efficiently, can analyze complex data. The research focused on AI has increased tremendously, and its role in healthcare service and research is emerging at a greater pace. This review elaborates on the opportunities and challenges of AI in healthcare and pharmaceutical research. The literature was collected from domains such as PubMed, Science Direct and Google scholar using specific keywords and phrases such as ‘Artificial intelligence’, ‘Pharmaceutical research’, ‘drug discovery’, ‘clinical trial’, ‘disease diagnosis’, etc. to select the research and review articles published within the last five years. The application of AI in disease diagnosis, digital therapy, personalized treatment, drug discovery and forecasting epidemics or pandemics was extensively reviewed in this article. Deep learning and neural networks are the most used AI technologies; Bayesian nonparametric models are the potential technologies for clinical trial design; natural language processing and wearable devices are used in patient identification and clinical trial monitoring. Deep learning and neural networks were applied in predicting the outbreak of seasonal influenza, Zika, Ebola, Tuberculosis and COVID-19. With the advancement of AI technologies, the scientific community may witness rapid and cost-effective healthcare and pharmaceutical research as well as provide improved service to the general public.
1. Introduction
Artificial intelligence (AI) is a combination of various intelligent processes and behavior, developed by computational models, algorithms or a set of rules which supports the machine to mimic the cognitive functions of humans such as learning, problem-solving, etc. [1,2]. AI is expeditiously penetrating the field of the healthcare sector and has a huge impact on clinical decision making, disease diagnosis, and automation [3]. There are opportunities for AI to explore further in the field of pharmaceutical and healthcare research because of its ability to investigate enormous data from various modalities [4]. Some of the current studies elaborate on the utilization of AI in healthcare and other sectors. The AI technologies in the healthcare industry include machine learning (ML), natural language processing (NLP), physical robots, robotic process automation, etc. [5]. In ML, neural network models and deep learning with various features are being applied in imaging data to identify clinically significant elements at the early stages, especially in cancer-related diagnoses [6,7]. NLP uses computational techniques to comprehend human speech and derive its meaning. Lately, ML techniques are being widely incorporated in NLP for exploring unstructured data in the database and records in the form of doctors’ notes, lab reports, etc. by mapping the essential information from various imagery and textual data which helps in decision making in diagnosis and treatment options [8]. The ongoing disruptive innovation creates a pathway for the patients to receive a precise and rapid diagnosis and customized treatment interventions [9]. AI-based solutions have been identified which include platforms that can make use of a variety of data types viz. symptoms reported by the patients, biometrics, imaging, biomarkers, etc. With the advancements in AI, the ability to detect potential illness well ahead is made possible, leading to a greater probability to prevent as an outcome of detection at a very early stage. Physical robots are being used in various healthcare segments including nursing, telemedicine, cleaning, radiology, surgical, rehabilitation, etc. [10,11]. The robotic process automation uses technology, which is inexpensive, easy to program and can perform structured digital tasks for administrative purposes and act like a semi-intelligent user of the systems. This can also be used in combination with image recognition. In the healthcare system, tasks such as preceding authorization, updating patient records and billing, which are repetitive, can utilize this technology [12].
When focusing on the pharmaceutical sector, the role of AI cannot be ignored due to its wider applications across various stages. The influence of AI across all stages of pharmaceutical products from drug discovery to product management is very evident. In drug discovery, AI technologies are used in both the drug screening and drug design; the algorithm includes, to name a few, ML, deep learning, AI-based quantitative structure–activity relationship (QSRL) technologies, QSLRML, virtual screening (VS), support vector machines (SVMs), deep virtual screening, deep neural networks (DNNs), recurrent neural networks (RNNs), etc. Neural networks in AI are inspired by biological neural networks where there is an input and output response after processing the information received. Artificial neural networks (ANN) have several connected units for processing the information. DNNs are similar to ANN wherein there are several layers of data processing units. RNNs process the data in a sequence whereby the output data of the previous analysis is processed as input data for the next phase of analysis. SVMs are used for classification and regression of input data. In pharmaceutical product development, AI is being used to choose the appropriate excipients, selecting the development process, and ensuring the specifications are achieved as per the compliance during the process. The model expert system (MES), ANNs, etc. are used in pharmaceutical product development. In manufacturing, AI is used in automated and personalized manufacturing, matching manufacturing errors to set limits. AI technologies such as meta classifier and tablet classifier are used to achieve the desired quality in the final product [13]. The incorporation of AI in clinical trials helps in selecting subjects and monitoring the trial, the dropouts are reduced because of close monitoring. ML is being used in clinical trials [14]. AI technologies such as ML and NLP tools are used in market analysis, product positioning and product costing [13]. Some of the articles related to AI have been published recently have discussed the AI application in medicinal chemistry, healthcare, pharmaceutical and biomedical studies, especially in target protein identification, computer aided drug design, virtual screening and in silico pharmacokinetic evaluation, disease diagnosis focused on cancer diagnosis and treatment [15,16]. AI has extensively invaded the sectors mentioned above and has led to improvement of the outcome. Owing to the widespread applications of AI in the healthcare and pharmaceutical industries, this review included the articles related to the application of AI in disease diagnosis, drug discovery, clinical trial, personalized treatment, and epidemiological research in the prediction of epidemics or pandemic. The studies related to the application of AI in pharmaceutical manufacturing, education, market analysis, customer service, commercialization, and anything not related to healthcare/pharmaceutical research are excluded in this review. All the studies are searched using domains such as PubMed, Science Direct and Google scholar using specific keywords.
This review discussed the role of artificial intelligence (AI) in the following areas.
- Disease diagnosis;
- Digital therapy/personalized treatment:
- ○
- Radiotherapy;
- ○
- Retina;
- ○
- Cancer;
- ○
- Other chronic disorders.
- Drug discovery:
- ○
- Prediction of bioactivity and toxicity;
- ○
- Clinical trials:
- ▪
- Clinical trial design, patient identification, recruitment and enrolment;
- ▪
- Monitoring trial, patient adherence and endpoint detection.
- Forecasting of an epidemic/pandemic.
2. AI in Disease Diagnosis
Disease analysis becomes pivotal in designing a considerate treatment and safeguarding the wellness of patients. The inaccuracy generated by humans creates a hindrance for accurate diagnosis, as well as the misinterpretation of the generated information creating a dense and demanding task. AI can have varied applications by bringing about proper assurance in accuracy and efficiency. After a vivid literature survey, the applications of various technologies and methodologies for the purpose of disease diagnosis have been reported. With the evolution of the human population, there is always an ever-increasing demand for the healthcare system, according to varied environmental manifestations [17].
A substantial amount of evidence has revealed that though vulnerable, contradictory, non-analyzing incongruities exist, the development of new methods can define the applicability by portraying the current existing scenario that has not been covered [18,19,20]. It is important to categorize the patients based upon whether he/she is severely affected by the diseases, and the AI can gain importance in diagnosis [21]. Diagnosis refers to the state where, upon certain pre-existing problems, one’s condition is designated [22]. It is always advised to maintain every patient’s health report forms, so as to collect the majority of reviews that are obtained via performing examinations and testing. Upon gathering information, the appropriate outcomes are mainly concerning the health care needs for a timely diagnosis. The analysis is the sole discretion of the state of the clinicians and may fluctuate [23]. There is availability of multiple diagnostic strategies which are leading to trust issues and thus, one needs to focus on AI for identification and determination of the early predictive stage of the disease more than the treatment or diagnostic phase. Such diagnosis can help to initiate the early treatment, and initial treatment can bring noticeable changes in the patients as well as improved efficiency in AI modules [24,25]. Nowadays, identification, extraction and catering all the collated data would lead to ample technology usage based on deep learning, neural networking and algorithms [26,27,28,29,30]. Cancer and dementia are the two major diseases where AI has gained importance [31,32]. Algorithms can never be biased if they are not self-generated or have never been associated with any existing data. For statistical supervision, a relevant and specific dataset is required [33,34,35]. The acceptance lies not on the input from the user but the salience of the identified clusters [36]. Hepatitis can be diagnosed through unsupervised learning [37]. However, deep learning correlations can be obtained through various evolutionary changes and adjusting predictions [38,39]. Usually, larger data sets and varied entries can serve the suitability of AI [38,40], but the outcome is incomprehensible [41,42]. Among many examples of deep learning in diagnostic, one is the classification of dermatological diseases [43] and atrial fibrillation detection [44]. The usage of cross-validation can be used for random splitting into multiple sets for algorithms estimation [45]. Accuracy, sensitivity, and specificity are three important aspects where the common measurements of AI focus [46,47].
On the basis of the literature analysis, the clinical aspects which can supervise the deep learning network and neural pathways using support vector machine, nearest neighbor, random forest, decision tree, logistic regression, naive Bayes, discriminate analysis and convolution neural network can generate the results in a more holistic approach. Algorithm-based performance-driven analysis can be performed via origin, sample size, number of features of the training and testing samples. In the diagnosis of liver diseases, decision trees and reasoning were integrated [48]. Many studies were performed for the predictive modeling, which was noticeable for predicting early Parkinson’s disease [49]. Rib segmentation algorithm was developed using the chest X-ray images for diagnosis of lung diseases [50]. Traditional methods are not useful in rib-wise segmentation of X-ray images due to various limitations. In this research, they have developed an algorithm via unpaired sample augmentation of chest X-ray images of pneumonia patients; later, a multi-scale network learns the features of images. The study reports that such algorithm achieves good performance with better rib segmentation which could be useful in diagnosing lung cancers and other lung diseases [50]. Recently, algorithm and machine leaning was used by the researchers in identification and classification of cardiac arrhythmia by processing the electrocardiograms signals. [51]. In another study, tuberculosis was classified and diagnosed by using the optimization genetic algorithm (GA) and support vector machine (SVM) classifier [52].
3. AI in Digital Therapy/Personalized Treatment
AI has the potential to derive a meaningful relationship within the raw datasheets that can be further used in the diagnosis, treatment, and mitigation of the disease. A variety of newer techniques which are used for computational understanding in this emerging field have the potential to be applied in almost every field of medical science. The complex clinical problems need to be solved with the challenge of acquiring, analyzing, and applying vast knowledge (Figure 1). The development of medical AI has helped clinicians to solve complex clinical problems. The systems such as ANNs, evolutionary computational, fuzzy expert systems and hybrid intelligent systems can assist the healthcare workers to manipulate the data [53]. The ANN is a system that is based upon the principle of the biological nervous system [54]. There is a network of interconnected computer processors called neurons that can perform parallel computations for data processing. The first artificial neuron was developed using a binary threshold function [41]. The multilayer feed-forward perceptron was the most popular model having different layers, such as input layer, middle layer, and output layer. Each neuron is connected through links having numerical weight [55].
Paul Werbos introduced a new technique called “Backpropagation learning” in 1974, which has a suitable learning algorithm [56]. The ANN has been used in diagnosis image analysis, data interpretation and waveform analysis. Fuzzy logic is a science of reasoning, thinking and inference that can recognize and use real-world phenomena. It mainly uses a continuous set of membership from 0 to 1, i.e., 0 for false and 1 for true. Fuzzy controller has also been used for administering vasodilators and anesthetics in the operating room [57]. This evolutionary computation technique is based on the natural evolution process that is focused upon the natural evolution process and survival of the fittest [58]. The most popular algorithm is the genetic algorithm. It finds out many random solutions for one problem and ultimately, one best solution is chosen, while the inferior ones are eliminated [59].
3.1. AI in Radiotherapy
Automated treatment planning is a recent technology, which is highly beneficial in radiotherapy treatment planning. Automated treatment planning is efficiently improving the plan quality, consistency, and error rate. The treatment workflow can be organized into three categories, i.e., automated rule implementation, reasoning modeling of prior knowledge in clinical practice and multi-criteria optimization [60]. A simple automated computer program with structures can implement the clinical guidelines. The treatment planning system can analyze the anatomy and physiology of the patient and can also mimic the reasoning process, which is generally followed in manual treatment planning. Three-dimensional dose distribution and dose models for spatial dose have shown promising accuracy [61]. Radiomics can give in-depth information about tumors with the help of several imaging biomarkers. Radiomics can be implemented for the prediction of outcomes and toxicity for individual patients’ radiation therapy [62].
3.2. AI in Retina
The high-resolution imaging of the retina has given the scope to assess human health remarkably. From a single photograph of the retina, one can extract highly personalized data; with high-definition medicines, the ophthalmologist/retinologist can define a personal therapy and establish a continuously improving learning healthcare system [63].
3.3. AI in Cancer
With the huge applicability of AI, it has gained importance in the fields of diagnosing and treating various cancers. The lymphoma subtypes of non-Hodgkin lymphoma were predicted by using gene expression data in a multilayer perceptron neural network. The neural network has 20,863 genes as the input layer and lymphoma subtypes as the output layer. Lymphoma subtypes includes mantle cell lymphoma (MCL), follicular lymphoma, diffuse large B-cell lymphoma (DLBCL), marginal zone lymphoma and Burkitt. An AI neural network has predicted the lymphoma subtypes with high accuracy [64]. An artificial neural network was used to identify the new prognostic markers of MCL using the gene expression data and reported that 58 genes predicted the survival with high accuracy, and 10 genes were associated with poor survival and 5 genes with favorable survival [65]. The Multilayer perceptron (MLP) with multivariate analysis of gene expressions reported that four genes correlate with favorable survival and three genes with poor survival for DLBCL [66]. MLP and radial basis function (RBF) neural networks were used for prediction of overall survival and prognosis of Follicular lymphoma (FL) patients. After analyzing 22,215 genes, it was reported that 43 genes are associated with the prediction of the overall survival, whereas 18 genes were associated with poor prognosis [67]. Cell-of-origin (COO) classification of DLBCL was carried out by an AI deep learning technique using the genetic and transcriptional data obtained by RNA-Seq in next-generation sequencing (NGS) platform. AI provided reproducible, efficient, and affordable assays for classification and further clinical application [68]. AI is used in cancer diagnosis by minimizing the time with high accuracy. AI-based PET imaging of lymphoma is used in tumor burden evaluation which was later applied in characterization of tumor, quantification of heterogeneity, as well as prediction of treatment response [69].
In gastrointestinal cancer, colorectal cancer (CRC) screening technology is used to analyze the malignancy in patients [70] and prediction of the Helicobacter pylori infection by visual nocturne play a crucial role in predicting the gastric cancer progression [71]. Early diagnosis through proper blood tests, endoscopic imaging and AI can influence the progression of the cancer [70]. However, AI lacks the proper randomization and blindfolded controlled studies, and hence, only retrospective data can be gathered [72]. Further, there have been studies where the prediction models could not justify the prognosis of cancers. Later on, various models such as Multi-task logistic regression algorithm, Cox survival regression algorithm and random survival forest algorithm have gained multiple facets and probable predictive outcomes [73]. With these advancements, automation in diagnosis of malignancy has been achieved via gastroenterology, not only for classification but also for detection and magnification using endocytoscopy, which has not been used in real practice [74].
AI is a versatile clinical aid for lung cancer detection in early stages and screening purposes. Deep learning and machine learning AI techniques give a supportive measure in lung cancer screening due to their ability to maintain a vast amount of data and characterize pulmonary nodules with precision [75,76]. Currently, AI eases the tasks of pathologists and accommodates remote institutes suffering from a shortage of pathologists. Several AI applications are found to be helpful in the field of lung cancer such as the segmentation of carcinoma foci, detection of lymph node metastasis, counting of tumor cells, and prediction of gene mutations [77,78,79,80]. AI has the potential to interpret low-dose computer tomography (LDCT) images of lung cancer screening and thus improved diagnostic accuracy and decreased the false-positive rate [81,82]. AI can also quantify tumor- and non-tumor-related morphological changes, which is important for prognostication on serial imaging. The convolutional neural network (CNN), recurrent neural network (RNN), and combined dual effect of the two algorithms can be utilized to differentiate the classification of benign and malignant nodules [83]. To overcome the limitation of AI in translational research, the tools which are user friendly and do not require computational science background for operation are vital in the progression of this technology in healthcare and pharmaceutical research.
In the last decade, AI has been very promising in the diagnosis of breast cancer. AI-assisted techniques are the combination of both quantitative and qualitative MRI features, which is applicable to predict treatment response in breast cancer patients, even before the start of neoadjuvant chemotherapy (NAC). AI has potential in identification, segmentation and classification of lesions; breast density assessment; and breast cancer risk assessment. AI-based software is able to provide clinical benefit to radiologists in distinguishing between malignant and benign breast lesions and reduce the chances of interpretation of false-negative mammograms [84,85,86,87]. The developments in this direction are preliminary and have many limitations such as absence of large public datasets, requirement of high quality images, ROI annotation dependence, problems in binary classification, inability in handling multiple tasks at the same time. Thus, the developments of AI tools including DL-based CAD are still at a preliminary stage due to the lack of enough public data sets for training the deep convolutional neural networks (DCNNs) [88].
3.4. AI in Other Chronic Diseases
Different computerized therapies are available based on computer programming techniques. The therapies are focused upon the behavioral and cognitive approach, which involves multiple-choice questions or joysticks [89]. Recently, a new computer interaction has been developed, i.e., intelligent computer-assisted instruction, which has the potential to use other AI technologies such as natural language understanding and expert systems [90], and with the use of AI, one can develop a combination therapy based upon the patient’s own biopsy and can adopt n-of-1-medication recommendations. Chronic disease requires monitoring on regular basis, and with the use of AI, this monitoring can be performed using virtual medical assistants. Many companies have installed such assistance, which generally provides virtual coaching through text messages with the use of the mobile applications, and with the use of AI, nutrition recommendations can also be given specifically based upon the gut microbiome. Arterial fibrillation can be predicted with the use of an integrated system based upon deep learning [91], single-lead ECG sensor and physical activity via accelerometer data along with a smart watch. Case-based reasoning, which is designed using AI technique, is being extensively used in the management of diabetes [92]. The automated system can detect problems and memorizes the best effective solution for the individual patient. It is already in use for the optimization of insulin therapy. Other techniques such as the vector regression technique are also in fashion for diabetes care. Machine learning-based different technologies such as clinical decision support can also predict short and long-term HbA1c response after insulin initiation in patients with type 2 diabetes mellitus. AI techniques can also be used to assess the risk of a particular disease. Advanced AI techniques that can work upon the molecular level such as molecular phenotyping, genomics, epigenetic alterations, and the development of digital biomarkers can also be used in the management of different diseased conditions. With the use of newer techniques, patients can manage their diabetes through web-based programs mobile phones and smart phones.
4. AI in Drug Discovery
The possibility of the development of a large number of drug molecules from a chemical space becomes lengthy due to lack of appropriate technologies, which can be improvised by using AI in the drug development process [93,94]. The quantitative structure–activity relationship affects the various parameters’ forecasting activities such as log P or log D, which can foresee the predictions and generation through computations and can justify the biological safety, efficacy and adverse effects, including the pharmacokinetics of the significant molecule [95,96]. The enormous space requires a delocalization of molecules by the three-dimensional distribution of molecules and their properties. It is advisable to collect all prior information regarding the selectivity and the positioning of the molecules for showing the bioactivity using numerous domains including PubChem, ChemBank, DrugBank and ChemDB. Various in silico methods are utilized for virtual screening that generally provides an improved analysis, quicker elimination, and assortment [93]. Drug design algorithms reconsider the physical, chemical, and toxicological profiles while selecting a lead compound to bind with and generate activities [97]. Different physicochemical properties can increase the effectiveness and biological activity [98]. QSAR is geared for the potential application of the drug candidate through AI-based QSAR approaches [99,100,101]. If the traditional approaches are followed for obtaining the statistical differences, the biological activity discovered and developed can take a decade to control [102]. The solubility, partition coefficient, degree of ionization and intrinsic permeability of the drug affect target receptor binding when designing a new drug [103]. Algorithms include molecular descriptors, such as Simplified Molecular Input Line Entry System (SMILES), to forecast the binding properties [104]. A quantitative structure–property relationship (QSPR) is generally used for the determination of the six physicochemical properties, known as the Estimation Program Interface Suite [105]. Deep learning and neural networks based on the ADMET predictor and ALGOPS program have been utilized for the prediction of the lipophilicity and solubility of various compounds [106]. Many undirected graphs are utilized for predicting solubility [107]. The surface area, mass, hydrogen count, refractivity, volume, log P, surface area, sum of the indices, solubility index and rotatable bonds are considered for the prediction of a new chemical entity [108].
4.1. AI in Prediction of Bioactivity and Toxicity
The efficacy depends on the affinity for the target protein or receptor. In similarity-based interaction, the drug and target are deemed, and it is thought that they will interact with the same target [109]. Chem Mapper and the similarity ensemble approach predict the drug–target interactions [110]. The substructure, connectivity or a combination can also be considered [109]. Deep learning approaches have shown improved performance as deep learning is independent of the 3D protein structure [110]. Deep Affinity, protein, and drug molecules interaction prediction are the approaches [111].
The prediction is necessary to sidestep toxic effects. The in vitro assays are frequent preliminary studies, followed by the preclinical studies where one can distinguish the deadliness, and there is further scope of improvement. Several Web-based technologies are accessible to lower the cost [105]. The Tox21 Data Challenge, organized by the National Institutes of Health, Environmental Protection Agency and US Food and Drug Administration, appraises computational techniques for estimation of the toxicity of the drugs [105]. An algorithm named Deep Tox outstripped all procedures by recognizing static and dynamic features within the chemical descriptors, whereas the eToxPred was applied for estimating the toxicity of small molecules. TargeTox, a biological target-based drug toxicity prediction uses the guilt-by-association principle [112]. A scoring function helps to predict the properties of the novel molecules. PrOCTOR could easily forecast whether a drug would fail in clinical trials owing to its toxicity. It also recognized adverse drug events [113]. AI can feed back by considering computation, geometry and assessment in collaboration with the structure-based drug discovery by predicting the protein structure [114]. The likelihood is necessary to understand its efficacy and effectiveness [114]. Various computational technologies can solve problems encountered with QSPR [115]. Decision-support tools use rule-based choosing systems, depending upon the nature and control of the quantity of the added ingredients for obtaining a positive feedback process [116]. With the increasing complications of better product efficiency and quality, manufacturing systems are trying to grant human knowledge to machines [117]. The amalgamation of technologies in manufacturing can prove to be a boost for the pharmaceutical industry. Chemical Assembly utilizes the novel platform for bringing about automation [97].
4.2. AI in Clinical Trials
In drug discovery, clinical trials are the longest and require a huge amount of investment. Despite the time and capital invested in clinical trials, the success rate is only marginal for those that obtain approval from the Food Drug Administration (FDA) [118,119,120]. There are several bottlenecks in clinical trials, and those can lead to failure of the trial. Those bottlenecks include the insufficient number of participants, drop-outs during the trial, side effects of the test drug, or inconsistent data. If such failure occurs in late phases of clinical trials, such as in phase-III and phase-IV, the sponsor has to absorb an extremely high economic burden [121]. The clinical trials which are associated with high costs also have subsequent effects on therapeutic costs for patients. Due to this reason, biopharma companies tie R&D costs of failed trials into the pricing of approved drugs to hold out the profit [122]. The process of execution and conducting of clinical trials includes clinical trial design, patient recruitment/selection, site selection, monitoring, data collection and analysis. Out of these processes, patient recruitment and selection is the cumbersome process where 80% of the trials overshoot the enrolment timeline, and 30% of phase-III trials are prematurely terminated due to patient enrolment challenges. Trial monitoring in a multi-centered global trial is a very expensive and time-consuming process. Other challenges in clinical trials are the duration from the “last subject last visit” to data submission to regulatory agencies, which are huge data collection and analysis procedures. With the help of AI and digitization, these challenges in the clinical trial have been transforming [123].
4.2.1. Clinical Trial Design, Patient Identification, Recruitment and Enrolment
As per the FDA, AI models are useful in improving the quality of trial design, patient selection by reducing population heterogeneity, prognostic enrichment, and predictive enrichment [124]. Bayesian nonparametric models (BNMs) have emerged as a powerful tool in clinical trial design with many other applications. This model is flexible and uses a nonparametric approach. This model allows us to use infinite-dimensional parameter sets with a finite subset of limited parameters. This approach minimizes the clustering and trial designing duration. Some of the commonly used BNMs are Dirichlet process mixture models and Markov Chain Monte Carlo (MCMC) techniques. There are many applications of such BNMs in clinical trial design, for example, the dose selection in clinical trials involving cancer patients, immuno-oncology and cell therapy trials. Dose selection is complicated due to the heterogeneity of the patients, which may lead to inaccurate dose selection and selection of future target populations. BNMs are an efficient and effective tool for dose selection in such patients because it considers all the variable and heterogeneity of the study subjects [123]. Bayesian nonparametric design is used for adaptive dose selection in multiple populations. This facilitates the borrowing of information across multiple populations while considering the heterogeneity of the populations. Such models help in accurate optimal dose selection, which minimizes the inaccuracy [125]. Other designs such as modified toxicity probability interval (mTPI) designs use the Dirichlet process. This design learns from the emerging data and selects the dose by prior approximation and automatically groups patients into similar clusters [126]. Selection of participants for the trial is the most important step where patients/participants’ health record provides vital information for matching the inclusion or exclusion criteria. Collecting the patients’ data/history or fresh testing would be time-consuming and costly. AI provides an opportunity to combine patient data with the electronic medical record (EMR) including omics data and other patient data, scattered among different locations, owners, and formats. Such analysis using computer vision algorithms such as optical character recognition (OCR) and Natural language processing (NLP) can provide an efficient process in patient identification and characterization [124].
4.2.2. Monitoring Trial, Patient Adherence and Endpoint Detection
Monitoring the trial participants is another challenge in the clinical trial and can be performed by AI-enabled wearable devices. Such monitoring is real-time, individualized and power efficient [124]. Risk-based monitoring (RBM) has recently emerged as the AI-enabled efficient and cost-effective technique alternative to traditional monitoring. An advanced version of RBM may be able to reduce the cost and increase the efficiency and quality of data monitoring in the trial site. AI-assisted “smart monitoring” can use predictive analysis and data visualization in improving the data quality check and trial site performance. Patients’ compliance to adherence criteria of the trial is important to obtain the reliable data and success of the trial. Video monitoring and wearable sensors capture the patient data automatically and continuously making the trial efficient in monitoring patient adherence [124]. Medical image-based endpoint and disease detection become much easier through AI-enabled compared to manual reading, and it is cost effective and fast [124]. Current developments suggest that AI is capable of transforming the traditional way of clinical trial to a cost-effective, safer and faster clinical trial.
5. AI in Forecasting of an Epidemic/Pandemic
Pandemic is boundless and capable of causing morbidity and mortality. Globally, there have been several pandemic outbreaks, to name a few, Black Death, Spanish flu, Cholera, Influenzas, AIDS, COVID-19, and they are capable of causing social and economic interruption [127]. There is intense interdependence between the early detection and successful management of the disease, which reduces the stress on individuals’ health, economic, social, and political systems. To achieve early detection, surveillance plays a major role [128]. Active surveillance demands huge resources, manpower and time. In practice, predicting the epidemic and pandemic is a challenge. However, with the current advancements studying the propagation of dreadful diseases is made possible. AI is the best option to achieve surveillance with the efficient utilization of resources. ML and deep learning are being incorporated in various healthcare segments and are found to be more effective when compared to human resources [129]. Developing epidemiological models is still challenging due to their complexity. Recently, ML has been incorporated to develop outbreak prediction models [130,131,132]. AI is being used in detection, prevention, response, and recovery in pandemics and epidemics. In prevention, it is beginning to be extensively used in prediction, surveillance, and information, especially in the recent COVID-19 outbreak [133]. The prediction of influenza epidemics is always a great challenge due to its shift in epidemic peak, periodic peaking, etc. With the incorporation of the SAAIM (self-adaptive AI model), an accurate forecast is possible even in areas with irregular seasonal influenza [134]. For example, in Taiwan, machine learning and ensemble approaches have been used to predict seasonal influenza, and it is accurate in the prediction forecast [135]. Using machine learning feed-forward propagation neural network model (MSDII-FFNN), the forecasting output precision is 90% for influenza [136]. Machine learning anonymized mobility map (AMM) has been incorporated in predicting influenza in Australia and USA. AMM groups the data from the smart phone and can forecast the epidemics using human mobility even across the state boundaries [137]. In Africa, Ebola is still challenging. To predict Ebola, various techniques have been employed including a hybrid neural network developed by Umang Soni et al. which shows 100% precision when random forest is employed as a classification technique [138]. The use of experimental models involving artificial societies and the integration of machine learning has led to reliable results in predicting the propagation. For example, the spread of Ebola has been studied in a simulated model of Beijing, and the outcome has been predicted [139]. It was very challenging to allocate the surveillance resource during the Zika epidemic in 2015, due to the non-availability of reliable prediction. Later, a dynamic neural network model was used to forecast the spread. This flexible predictive model framework was reliable and added value at the initial phase of the epidemic [140]. Mobile application was used in the Zika project to monitor the mosquito population, and the early detection was performed by incorporating AI neural networks [141]. Vaccine-derived poliovirus (VDPV) observation has gained attention because of its outcomes. Hybrid machine learning is incorporated with the combination of random vector functional link (RVFL) networks with the whale optimization algorithm (WOA), which can predict a VDPV outbreak [142]. In HIV/AIDS prevention measures, ML has the potential to distinguish possible candidates for pre-exposure prophylaxis [143]. Dengue is prevalent in tropical and sub-tropical zones. The ML algorithm support vector regression (SVR) is capable of predicting with negligible error and tracking dengue outbreaks in China [144]. In Malaysia, the ML Support vector model (SVM) using linear kernel performed the best predictor for dengue [145], and Bayesian network ML techniques were employed in dengue outbreak prediction [146]. The ANN is incorporated for rapid diagnosis using TB suspect data, and the overall efficacy is more than 94%. This will help to detect the overall spread of the disease, and swift implantation of some control measure [147]. Using deep learning and machine learning, a CNN model named tuberculosis AI (TB-AI) identified TB bacillus and showed 97.94% sensitivity [148]. Multilayer Perceptron Neural Network Classifier (MPNN) was suggested for the diagnosis of yellow fever, taking seven psychological symptoms of yellow fever, and achieved the prediction precision of 88% [149]. The COVID-19 outbreak shook the entire world [150]. AI-inspired modified stacked auto-encoder modelling was used to predict the COVID-19 [151]. Deep learning Composite Monte Carlo (CMC) in combination with the fuzzy rule was helpful in decision making and predicting the COVID-19 pandemic [152]. A polynomial neural network with corrective feedback (PNN + CF) is used to forecast with negligible error [153]. CNN, a deep neural network used in China, has a precise prediction efficacy [154]. In Switzerland, the AI model (Enerpol) combined with Big Data is used in the prediction of COVID-19 [155]. To investigate the dynamical pattern of COVID-19, statistical and deep learning systems such as autoregressive integrated moving average (ARIMA), multilayer perception (MLP), feed-forward neural network (FNN) and long short-term memory (LSTM) were incorporated. The data produced might be a useful reference for the COVID-19 prediction [156].
6. Discussion and Conclusions
Researchers are fascinated by the recent developments in AI, especially its application in healthcare and pharmaceutical research and service. Smart hospitals and healthcare facilities enabled with AI, ML and Big Data will be shaping the future healthcare sector. Pharmaceutical industries are in constant advancement with their technologies and AI will be an opportunity for minimizing the cost and time for drug development. Various applications of AI in healthcare and pharmaceutical research as well as the limitations/challenges of these technologies have been presented in Table 1. The role of AI in disease diagnosis is well demonstrated by using deep learning, neural networking and unsupervised learning. These AI tools have the ability to process unstructured data and correlate with the learned data to predict an accurate outcome, which is useful in predicting a particular disease diagnosis. AI has been proven a vital technology such as intelligent computer-assisted instruction (ICAI), Case-based reasoning, vector regression technique, clinical decision support for monitoring chronic disease progress and optimizing the therapy for those diseases. Vector regression technique is useful in identifying the connections between variables; ICAI is useful in computer assisted instruction to patients to obtain an informative answer from the patients; case-based reasoning helps in solving a problem from its past similar experience and clinical decision support provides patient-specific information and knowledge to healthcare team to help in monitoring and treating a disease. These technologies are useful in developing a personalized treatment, which is always a challenge. Other techniques such as Radiomics, which is the prediction of the outcomes and toxicity for individual patients’ radiation therapy, and high-resolution imaging of the retina give scope to examine human health. Drug discovery and bringing a new drug to the market is the prime objective of Pharmaceutical R&D, which is a very lengthy and costly affair. AI has the potential to ease the process, from target selection through to clinical trials of a drug. Drug discovery starts with the identification of target biological molecules that interfere in modifying the disease. In the drug discovery process, thousands of synthetic molecules are generated that could bind to the target and modify its activity for managing a particular disease. In this process, computer-aided drug design and quantitative structure–activity relationship (QSAR) or quantitative structure–property relationships (QSPR) are used to determine the physicochemical and pharmacokinetic properties. Deep learning and neural networks based on the ADMET predictor and ALGOPS program are used in the prediction of lipophilicity and solubility of an NCE. Chem Mapper and similarity ensemble approach are the AI technologies that predict the drug–target interactions. In toxicity testing, Deep Tox, eToxPred, TargeTox and PrOCTOR are the tools used in predicting the toxicity of a small molecule. Such predictions can exclude plausible toxic molecules and help industries to save time and money in preclinical or clinical studies. Clinical trials of a new molecule consume most of the time and budget of the drug discovery process, and AI has been used in improving the quality of trial design, patient selection, dose selection, patient adherence, trial monitoring and endpoint analysis. BNMs have potential application in clinical trial design and dose selection, whereas OCR and NLP provide an efficient method in patient identification and characterization. RBM, video monitoring and wearable sensors are cost-effective techniques in patient monitoring and patient adherence. AI can play a key role in clinical trials in reducing the total duration and cost of launching a drug to market. The world often witnesses several epidemic and pandemic outbreaks causing tremendous human suffering and death. Currently, the world is witnessing the COVID-19 pandemic, with nearly six million deaths. Historically, there have been many deadly outbreaks, which include Cholera, Spanish Flu, AIDS, etc. AI is an effective technology in detection, prevention, response, and recovery in epidemics or pandemics. Deep learning is found to be more effective in tracking the pandemic or epidemic. Other effective AI technologies include neural networks, AMM, and the ML algorithm SVR for predicting an epidemic or pandemic. Besides its applications and advantages over traditional methods, AI possesses some limitations or challenges. The major challenges are the requirement of huge amounts of data to feed the system for training, logistical difficulties in implementation, expense, and dependence on the hardware or computational facilities. Sometimes, AI technologies such as QSPR and Chem Mapper are unreliable due to epistemic uncertainty, errors and lack of flexibility. The progressions in AI technologies are constantly evolving, and these technologies will be useful when the advantages over the limitations will be higher. Thus, AI-enabled techniques will be opening up many opportunities in various sectors of healthcare and pharmaceutical research, and this could be a game-changer in futuristic research.
Author Contributions
Conceptualization, S.K.B.; methodology, S.K.B., P.B. and P.G.; writing—original draft preparation, S.K.B., P.B., P.G., S.P., M.C. and J.M.; writing—review and editing, S.K.B. and M.C.; supervision, S.K.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen, M.; Decary, M. Artificial intelligence in healthcare: An essential guide for health leaders. In Healthcare Management Forum; SAGE Publications: Los Angeles, CA, USA, 2020. [Google Scholar]
- Bajwa, J.; Munir, U.; Nori, A.; Williams, B. Artificial intelligence in healthcare: Transforming the practice of medicine. Futur. Healthc. J. 2021, 8, e188–e194. [Google Scholar] [CrossRef] [PubMed]
- Sunarti, S.; Rahman, F.F.; Naufal, M.; Risky, M.; Febriyanto, K.; Masnina, R. Artificial intelligence in healthcare: Opportunities and risk for future. Gac. Sanit. 2021, 35, S67–S70. [Google Scholar] [CrossRef]
- Toepper, M. Dissociating Normal Aging from Alzheimer’s Disease: A View from Cognitive Neuroscience. J. Alzheimer’s Dis. 2017, 57, 331–352. [Google Scholar] [CrossRef] [Green Version]
- Davenport, T.; Kalakota, R. The potential for artificial intelligence in healthcare. Futur. Healthc. J. 2019, 6, 94–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fakoor, R.; Ladhak, F.; Nazi, A.; Huber, M. Using deep learning to enhance cancer diagnosis and classification. In Proceedings of the International Conference on Machine Learning, Atlanta, GA, USA, 16–21 June 2013; ACM: New York, NY, USA, 2013; Volume 28, pp. 3937–3949. [Google Scholar]
- Vial, A.; Stirling, D.; Field, M.; Ros, M.; Ritz, C.; Carolan, M.; Holloway, L.; Miller, A.A. The role of deep learning and radiomic feature extraction in cancer-specific predictive modelling: A review. Transl. Cancer Res. 2018, 7, 803–816. [Google Scholar] [CrossRef]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; Depristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]
- Horgan, D.; Romao, M.; Morré, S.A.; Kalra, D. Artificial Intelligence: Power for Civilisation—And for Better Healthcare. Public Health Genom. 2019, 22, 145–161. [Google Scholar] [CrossRef]
- Hussain, A.; Malik, A.; Halim, M.U.; Ali, A.M. The use of robotics in surgery: A review. Int. J. Clin. Pract. 2014, 68, 1376–1382. [Google Scholar] [CrossRef]
- Khan, Z.H.; Siddique, A.; Lee, C.W. Robotics Utilization for Healthcare Digitization in Global COVID-19 Management. Int. J. Environ. Res. Public Health 2020, 17, 3819. [Google Scholar] [CrossRef]
- Ribeiro, J.; Lima, R.; Eckhardt, T.; Paiva, S. Robotic Process Automation and Artificial Intelligence in Industry 4.0—A Literature review. Procedia Comput. Sci. 2021, 181, 51–58. [Google Scholar] [CrossRef]
- Paul, D.; Sanap, G.; Shenoy, S.; Kalyane, D.; Kalia, K.; Tekade, R.K. Artificial intelligence in drug discovery and development. Drug Discov. Today 2021, 26, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A. Artificial intelligence in managing clinical trial design and conduct: Man and machine still on the learning curve? Perspect. Clin. Res. 2021, 12, 1. [Google Scholar] [CrossRef]
- Sahu, A.; Mishra, J.; Kushwaha, N. Artificial Intelligence (AI) in Drugs and Pharmaceuticals. Comb. Chem. High Throughput Screen. 2022, 25, 1818–1837. [Google Scholar] [CrossRef] [PubMed]
- Thakur, A.; Mishra, A.P.; Panda, B.; Rodríguez, C.S.; Gaurav, I.; Majhi, B. Application of Artificial Intelligence in Pharmaceutical and Biomedical Studies. Curr. Pharm. Des. 2020, 26, 3569–3578. [Google Scholar] [CrossRef] [PubMed]
- Menschner, P.; Prinz, A.; Koene, P.; Köbler, F.; Altmann, M.; Krcmar, H.; Leimeister, J.M. Reaching into patients’ homes—Participatory designed AAL services: The case of a patient-centered nutrition tracking service. Electron. Mark. 2011, 21, 63–76. [Google Scholar] [CrossRef] [Green Version]
- Okoli, C. A Guide to Conducting a Standalone Systematic Literature Review. Commun. Assoc. Inf. Syst. 2015, 37, 879–910. [Google Scholar] [CrossRef] [Green Version]
- Paré, G.; Trudel, M.-C.; Jaana, M.; Kitsiou, S. Synthesizing information systems knowledge: A typology of literature reviews. Inf. Manag. 2015, 52, 183–199. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Ransohoff, D.F.; Feinstein, A.R. Problems of Spectrum and Bias in Evaluating the Efficacy of Diagnostic Tests. N. Engl. J. Med. 1978, 299, 926–930. [Google Scholar] [CrossRef]
- Jutel, A. Sociology of diagnosis: A preliminary review. Sociol. Health Illn. 2009, 31, 278–299. [Google Scholar] [CrossRef]
- Chang, C.L.; Hsu, M.Y. The study that applies artificial intelligence and logistic regression for assistance in differential diagnostic of pancreatic cancer. Expert Syst. Appl. 2009, 36, 10663–10672. [Google Scholar] [CrossRef]
- Obeng, O.; Paul, S. Understanding HIPAA compliance practice in healthcare organizations in a cultural context. In Proceedings of the 25th Americas Conference on Information Systems 2019, Cancún, Mexico, 15–17 August 2019. [Google Scholar]
- Spohrer, J.; Banavar, G. Cognition as a Service: An Industry Perspective. AI Mag. 2017, 36, 71–86. [Google Scholar] [CrossRef] [Green Version]
- Nasirian, F.; Ahmadian, M.; Lee, O. AI-Based Voice Assistant Systems: Evaluating from the Interaction and Trust Perspectives. In Proceedings of the 23rd Americas Conference on Information Systems 2017, Boston, MA, USA, 10–12 August 2017. [Google Scholar]
- Dellermann, D.; Lipusch, N.; Ebel, P.; Leimeister, J.M. Design principles for a hybrid intelligence decision support system for business model validation. Electron. Mark. 2019, 29, 423–441. [Google Scholar] [CrossRef] [Green Version]
- Kersting, K. Machine Learning and Artificial Intelligence: Two Fellow Travelers on the Quest for Intelligent Behaviour in Machines. Front. Big Data 2018, 1, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauschert, S.; Raubenheimer, K.; Melton, P.E.; Huang, R.C. Machine learning and clinical epigenetics: A review of challenges for diagnosis and classification. Clin. Epigenetics 2020, 12, 51. [Google Scholar] [CrossRef] [Green Version]
- Bosse, S.; Maniry, D.; Muller, K.R.; Wiegand, T.; Samek, W. Deep Neural Networks for No-Reference and Full-Reference Image Quality Assessment. IEEE Trans. Image Process. 2018, 27, 206–219. [Google Scholar] [CrossRef] [Green Version]
- Mazzocco, T.; Hussain, A. Novel logistic regression models to aid the diagnosis of dementia. Expert Syst. Appl. 2012, 39, 3356–3361. [Google Scholar] [CrossRef]
- Lu, J.; Song, E.; Ghoneim, A.; Alrashoud, M. Machine learning for assisting cervical cancer diagnosis: An ensemble approach. Futur. Gener. Comput. Syst. 2020, 106, 199–205. [Google Scholar] [CrossRef]
- Solan, Z.; Horn, D.; Ruppin, E.; Edelman, S. Unsupervised learning of natural languages. Proc. Natl. Acad. Sci. USA 2005, 102, 11629–11634. [Google Scholar] [CrossRef] [Green Version]
- Karpischek, S.; Michahelles, F.; Fleisch, E. Detecting incorrect product names in online sources for product master data. Electron. Mark. 2014, 24, 151–160. [Google Scholar] [CrossRef]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alanazi, H.O.; Abdullah, A.H.; Qureshi, K.N. A Critical Review for Developing Accurate and Dynamic Predictive Models Using Machine Learning Methods in Medicine and Health Care. J. Med. Syst. 2017, 41, 69. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Mehta, J.C.; Anand, D.; Nath, P.; Pandey, B.; Khamparia, A. An intelligent hybrid approach for hepatitis disease diagnosis: Combining enhanced k -means clustering and improved ensemble learning. Expert Syst. 2020, 38, e12526. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning, 1st ed.; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Fogassi, L.; Ferrari, P.F.; Gesierich, B.; Rozzi, S.; Chersi, F.; Rizzolotti, G. Neuroscience: Parietal lobe: From action organization to intention understanding. Science 2005, 308, 662–667. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Mao, J.; Mohiuddin, K. Artificial neural networks: A tutorial. Computer 1996, 29, 31–44. [Google Scholar] [CrossRef] [Green Version]
- Rudin, C. Stop explaining black box machine learning models for high stakes decisions and use interpretable models instead. Nat. Mach. Intell. 2019, 1, 206–215. [Google Scholar] [CrossRef] [Green Version]
- Mishra, S.; Yamasaki, T.; Imaizumi, H. Supervised classification of Dermatological diseases by Deep learning. arXiv 2018, arXiv:1802.03752. [Google Scholar]
- Jin, Y.; Qin, C.; Huang, Y.; Zhao, W.; Liu, C. Multi-domain modeling of atrial fibrillation detection with twin attentional convo-lutional long short-term memory neural networks. Knowl.-Based Syst. 2020, 193, 105460. [Google Scholar] [CrossRef]
- Wong, T.T. Performance evaluation of classification algorithms by k-fold and leave-one-out cross validation. Pattern Recognit. 2015, 48, 2839–2846. [Google Scholar] [CrossRef]
- Ben-David, A. Comparison of classification accuracy using Cohen’s Weighted Kappa. Expert Syst. Appl. 2008, 34, 825–832. [Google Scholar] [CrossRef]
- Sokolova, M.; Lapalme, G. A systematic analysis of performance measures for classification tasks. Inf. Process. Manag. 2009, 45, 427–437. [Google Scholar] [CrossRef]
- Lin, R.H. An intelligent model for liver disease diagnosis. Artif. Intell. Med. 2009, 47, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Prashanth, R.; Roy, S.D.; Mandal, P.K.; Ghosh, S. High-Accuracy Detection of Early Parkinson’s Disease through Multimodal Features and Machine Learning. Int. J. Med. Inform. 2016, 90, 13–21. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, D.; Ding, S.; Gao, Z.; Feng, J.; Wan, S. Rib segmentation algorithm for X-ray image based on unpaired sample augmentation and multi-scale network. Neural Comput. Appl. 2021, 1–15. [Google Scholar] [CrossRef]
- Qaisar, S.M.; Khan, S.I.; Srinivasan, K.; Krichen, M. Arrhythmia classification using multirate processing metaheuristic optimization and variational mode decomposition. J. King Saud Univ.—Comput. Inf. Sci. 2022; in press. [Google Scholar]
- Hrizi, O.; Gasmi, K.; Ben Ltaifa, I.; Alshammari, H.; Karamti, H.; Krichen, M.; Ben Ammar, L.; Mahmood, M.A. Tuberculosis Disease Diagnosis Based on an Optimized Machine Learning Model. J. Heal. Eng. 2022, 2022, 8950243. [Google Scholar] [CrossRef]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.; Drew, P.J. Artificial intelligence in medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334. [Google Scholar] [CrossRef] [Green Version]
- Albu, A.; Ungureanu, L. Artificial neural network in medicine. Telemed. J. e-Health 2012, 18, 446–453. [Google Scholar]
- Hopfield, J.J. Artificial neural networks. IEEE Circuits Syst. Mag. 1988, 4, 3–10. [Google Scholar] [CrossRef]
- Mandal, L.; Jana, N.D. Prediction of Active Drug Molecule using Back-Propagation Neural Network. In Proceedings of the 8th International Conference System Modeling and Advancement in Research Trends (SMART) 2019, Moradabad, India, 22–23 November 2019; pp. 22–26. [Google Scholar]
- Hanson III, C.W.; Marshall, B.E. Artificial intelligence applications in the intensive care unit. Crit. Care Med. 2001, 29, 427–435. [Google Scholar] [CrossRef] [Green Version]
- Fogel, D.B. What is evolutionary computation? IEEE Spectr. 2000, 37, 26–32. [Google Scholar] [CrossRef]
- Whitley, D. A genetic algorithm tutorial. Stat. Comput. 1994, 4, 65–85. [Google Scholar] [CrossRef]
- Moore, K.L. Automated radiotherapy treatment planning. In Seminars in Radiation Oncology; WB Saunders: Philadelphia, PA, USA, 2019; Volume 29, pp. 209–218. [Google Scholar]
- Troulis, M.; Everett, P.; Seldin, E.; Kikinis, R.; Kaban, L. Development of a three-dimensional treatment planning system based on computed tomographic data. Int. J. Oral Maxillofac. Surg. 2002, 31, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Arimura, H.; Soufi, M.; Kamezawa, H.; Ninomiya, K.; Yamada, M. Radiomics with artificial intelligence for precision medicine in radiation therapy. J. Radiat. Res. 2019, 60, 150–157. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Sadeghipour, A.; Gerendas, B.S.; Waldstein, S.M.; Bogunović, H. Artificial intelligence in retina. Prog. Retin. Eye Res. 2018, 67, 1–29. [Google Scholar] [CrossRef]
- Carreras, J.; Hamoudi, R. Artificial Neural Network Analysis of Gene Expression Data Predicted Non-Hodgkin Lymphoma Subtypes with High Accuracy. Mach. Learn. Knowl. Extr. 2021, 3, 720–739. [Google Scholar] [CrossRef]
- Carreras, J.; Nakamura, N.; Hamoudi, R. Artificial Intelligence Analysis of Gene Expression Predicted the Overall Survival of Mantle Cell Lymphoma and a Large Pan-Cancer Series. Healthcare 2022, 10, 155. [Google Scholar] [CrossRef]
- Carreras, J.; Hiraiwa, S.; Kikuti, Y.Y.; Miyaoka, M.; Tomita, S.; Ikoma, H.; Ito, A.; Kondo, Y.; Roncador, G.; Garcia, J.F.; et al. Artificial Neural Networks Predicted the Overall Survival and Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using a Pancancer Immune-Oncology Panel. Cancers 2021, 13, 6384. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Nakamura, N.; Hamoudi, R. Artificial Intelligence Analysis of the Gene Expression of Follicular Lymphoma Predicted the Overall Survival and Correlated with the Immune Microenvironment Response Sig-natures. Mach. Learn. Knowl. Extr. 2020, 2, 647–671. [Google Scholar] [CrossRef]
- Xu-Monette, Z.Y.; Zhang, H.; Zhu, F.; Tzankov, A.; Bhagat, G.; Visco, C.; Dybkaer, K.; Chiu, A.; Tam, W.; Zu, Y.; et al. A refined cell-of-origin classifier with targeted NGS and artificial intelligence shows robust predictive value in DLBCL. Blood Adv. 2020, 4, 3391–3404. [Google Scholar] [CrossRef]
- Hasani, N.; Paravastu, S.; Farhadi, F.; Yousefirizi, F.; Morris, M.; Rahmim, A.; Roschewski, M.; Summers, R.; Saboury, B. Artificial Intelligence in Lymphoma PET Imaging: A Scoping Review (Current Trends and Future Directions). PET Clin. 2022, 17, 145–174. [Google Scholar] [CrossRef] [PubMed]
- Mitsala, A.; Tsalikidis, C.; Pitiakoudis, M.; Simopoulos, C.; Tsaroucha, A. Artificial Intelligence in Colorectal Cancer Screening, Diagnosis and Treatment. A New Era. Curr. Oncol. 2021, 28, 1581–1607. [Google Scholar] [CrossRef] [PubMed]
- Bang, C.S.; Lee, J.J.; Baik, G.H. Artificial Intelligence for the Prediction of Helicobacter Pylori Infection in Endoscopic Images: Systematic Review and Meta-Analysis Of Diagnostic Test Accuracy. J. Med. Internet Res. 2020, 22, e21983. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y. Artificial intelligence-assisted endoscopic detection of esophageal neoplasia in early stage: The next step? World J. Gastroenterol. 2021, 27, 1392–1405. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; He, T.; Huang, L.; Li, J.; Wang, P. Immune gene prognostic signature for disease free survival of gastric cancer: Translational research of an artificial intelligence survival predictive system. Comput. Struct. Biotechnol. J. 2021, 19, 2329–2346. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Cho, B.-J.; Lee, M.-J.; Kim, J.H.; Lim, H.; Bang, C.S.; Jeong, H.M.; Hong, J.T.; Baik, G.H. Automated Classification of Colorectal Neoplasms in White-Light Colonoscopy Images via Deep Learning. J. Clin. Med. 2020, 9, 1593. [Google Scholar] [CrossRef]
- Joy Mathew, C.; David, A.M.; Joy Mathew, C.M. Artificial Intelligence and its future potential in lung cancer screening. EXCLI J. 2020, 19, 1552–1562. [Google Scholar]
- Hunter, B.; Hindocha, S.; Lee, R.W. The Role of Artificial Intelligence in Early Cancer Diagnosis. Cancers 2022, 14, 1524. [Google Scholar] [CrossRef]
- Arlova, A.; Jin, C.; Wong-Rolle, A.; Chen, E.S.; Lisle, C.; Brown, G.T.; Lay, N.; Choyke, P.L.; Turkbey, B.; Harmon, S.; et al. Artificial Intelligence-based Tumor Segmentation in Mouse Models of Lung Adenocarcinoma. J. Pathol. Inform. 2022, 13, 100007. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, T.; Furukawa, T.; Lami, K.; Pham, H.H.N.; Uegami, W.; Kuroda, K.; Kawai, M.; Sakanashi, H.; Cooper, L.A.D.; Bychkov, A.; et al. A narrative review of digital pathology and artificial intelligence: Focusing on lung cancer. Transl. Lung Cancer Res. 2020, 9, 2255–2276. [Google Scholar] [CrossRef]
- Espinoza, J.L.; Dong, L.T. Artificial Intelligence Tools for Refining Lung Cancer Screening. J. Clin. Med. 2020, 9, 3860. [Google Scholar] [CrossRef]
- Ye, M.; Tong, L.; Zheng, X.; Wang, H.; Zhou, H.; Zhu, X.; Zhou, C.; Zhao, P.; Wang, Y.; Wang, Q.; et al. A Classifier for Improving Early Lung Cancer Diagnosis Incorpo-rating Artificial Intelligence and Liquid Biopsy. Front. Oncol. 2022, 12, 853801. [Google Scholar] [CrossRef] [PubMed]
- Trebeschi, S.; Bodalal, Z.; Boellaard, T.N.; Bucho, T.M.T.; Drago, S.G.; Kurilova, I.; Calin-Vainak, A.M.; Pizzi, A.D.; Muller, M.; Hummelink, K.; et al. Prognostic Value of Deep Learning-Mediated Treatment Monitoring in Lung Cancer Patients Receiving Immunotherapy. Front. Oncol. 2021, 11, 609054. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.Y.; Chao, H.S.; Chen, Y.M. Application of Artificial Intelligence in Lung Cancer. Cancers 2022, 14, 1370. [Google Scholar] [CrossRef]
- Chen, S. Models of Artificial Intelligence-Assisted Diagnosis of Lung Cancer Pathology Based on Deep Learning Algorithms. J. Healthc. Eng. 2022, 2022, 3972298. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.M.; Yin, M.; Yu, M.H.; Yu, J.; Zeng, S.E.; Lv, W.Z.; Li, J.; Ye, H.R.; Cui, X.W.; Dietrich, C.F. Artificial Intelligence in Medical Imaging of the Breast. Front. Oncol. 2021, 11, 2892. [Google Scholar] [CrossRef]
- Poortmans, P.M.; Takanen, S.; Marta, G.N.; Meattini, I.; Kaidar-Person, O. Winter is over: The use of Artificial Intelligence to individualise radiation therapy for breast cancer. Breast 2020, 49, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Li, H.; Edwards, A.V.; Papaioannou, J.; Ma, W.; Liu, P.; Giger, M.L. Independent validation of machine learning in diagnosing breast Cancer on magnetic resonance imaging within a single institution. Cancer Imaging 2019, 19, 64. [Google Scholar] [CrossRef] [Green Version]
- Lo Gullo, R.; Eskreis-Winkler, S.; Morris, E.A.; Pinker, K. Machine learning with multiparametric magnetic resonance imaging of the breast for early prediction of response to neoadjuvant chemotherapy. Breast 2020, 49, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.P.; Samala, R.K.; Hadjiiski, L.M. CAD and AI for breast cancer—Recent development and challenges. Br. J. Radiol. 2020, 93, 20190580. [Google Scholar] [CrossRef]
- Posner, M.I.; Rothbart, M.K. Research on Attention Networks as a Model for the Integration of Psychological Science. Annu. Rev. Psychol. 2007, 58, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haag, M.; Maylein, L.; Leven, F.J.; Tönshoff, B.; Haux, R. Web-based training: A new paradigm in computer-assisted instruction in medicine. Int. J. Med. Inform. 1999, 53, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, H.; Du, X.; Zhang, P.; Hu, G.; Xie, G.; Guo, S.; Xu, M.; Xie, X. Integrated Machine Learning Approaches for Predicting Ischemic Stroke and Thromboembolism in Atrial Fibrillation. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Chicago, IL, USA, 2016; Volume 2016, p. 799. [Google Scholar]
- Ellahham, S. Artificial Intelligence: The Future for Diabetes Care. Am. J. Med. 2020, 133, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.K.; Pichika, M.R. Artificial intelligence in drug development: Present status and future prospects. Drug Discov. Today 2019, 24, 773–780. [Google Scholar] [CrossRef]
- Vyas, M. Artificial intelligence: The beginning of a new era in pharmacy profession. Asian J. Pharm. 2018, 12, 72–76. [Google Scholar]
- Zhu, H. Big Data and Artificial Intelligence Modeling for Drug Discovery. Annu. Rev. Pharmacol. Toxicol. 2020, 60, 573–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciallella, H.L.; Zhu, H. Advancing Computational Toxicology in the Big Data Era by Artificial Intelligence: Data-Driven and Mechanism-Driven Modeling for Chemical Toxicity. Chem. Res. Toxicol. 2019, 32, 536–547. [Google Scholar] [CrossRef]
- Chan, H.C.S.; Shan, H.; Dahoun, T.; Vogel, H.; Yuan, S. Advancing Drug Discovery via Artificial Intelligence. Trends Pharmacol. Sci. 2019, 40, 592–604. [Google Scholar] [CrossRef]
- Firth, N.C.; Atrash, B.; Brown, N.; Blagg, J. MOARF, an Integrated Workflow for Multiobjective Optimization: Implementation, Synthesis, and Biological Evaluation. J. Chem. Inf. Model. 2015, 55, 1169–1180. [Google Scholar] [CrossRef]
- Zhang, L.; Tan, J.; Han, D.; Zhu, H. From machine learning to deep learning: Progress in machine intelligence for rational drug discovery. Drug Discov. Today 2017, 22, 1680–1685. [Google Scholar] [CrossRef]
- Jain, N.; Gupta, S.; Sapre, N.; Sapre, N.S. In silico de novo design of novel NNRTIs: A bio-molecular modelling approach. RSC Adv. 2015, 5, 14814–14827. [Google Scholar] [CrossRef]
- Wang, Y.; Guo, Y.; Kuang, Q.; Pu, X.; Ji, Y.; Zhang, Z.; Li, M. A comparative study of family-specific protein–ligand complex affinity prediction based on random forest approach. J. Comput. Mol. Des. 2014, 29, 349–360. [Google Scholar] [CrossRef] [PubMed]
- King, R.D.; Hirst, J.; Sternberg, M. Comparison of Artificial Intelligence Methods for Modeling Pharmaceutical QSARs. Appl. Artif. Intell. 1995, 9, 213–233. [Google Scholar] [CrossRef]
- Zang, Q.; Mansouri, K.; Williams, A.J.; Judson, R.S.; Allen, D.G.; Casey, W.M.; Kleinstreuer, N.C. In Silico Prediction of Physicochemical Properties of Environmental Chemicals Using Molecular Fingerprints and Machine Learning. J. Chem. Inf. Model. 2017, 57, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Hessler, G.; Baringhaus, K.-H. Artificial Intelligence in Drug Design. Molecules 2018, 23, 2520. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Wang, Y.; Byrne, R.; Schneider, G.; Yang, S. Concepts of Artificial Intelligence for Computer-Assisted Drug Discovery. Chem. Rev. 2019, 119, 10520–10594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lusci, A.; Pollastri, G.; Baldi, P. Deep Architectures and Deep Learning in Chemoinformatics: The Prediction of Aqueous Solubility for Drug-Like Molecules. J. Chem. Inf. Model. 2013, 53, 1563–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, R.; Sharma, A.; Siddiqui, M.H.; Tiwari, R.K. Prediction of human intestinal absorption of compounds using artificial in-telligence techniques. Curr. Drug Discov. Technol. 2017, 14, 244–254. [Google Scholar] [CrossRef]
- Chai, S.; Liu, Q.; Liang, X.; Guo, Y.; Zhang, S.; Xu, C.; Du, J.; Yuan, Z.; Zhang, L.; Gani, R. A grand product design model for crystallization solvent design. Comput. Chem. Eng. 2020, 135, 106764. [Google Scholar] [CrossRef]
- Öztürk, H.; Özgür, A.; Ozkirimli, E. Deep DTA: Deep drug–target binding affinity prediction. Bioinformatics 2018, 34, i821–i829. [Google Scholar] [CrossRef] [Green Version]
- Lounkine, E.; Keiser, M.J.; Whitebread, S.; Mikhailov, D.; Hamon, J.; Jenkins, J.L.; Lavan, P.; Weber, E.; Doak, A.K.; Côté, S.; et al. Large-scale prediction and testing of drug activity on side-effect targets. Nature 2012, 486, 361–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Q.; Dueva, E.; Cherkasov, A.; Ester, M. Padme: A deep learning-based framework for drug-target interaction prediction. arXiv 2018, arXiv:1807.09741. [Google Scholar]
- Lysenko, A.; Sharma, A.; A Boroevich, K.; Tsunoda, T. An integrative machine learning approach for prediction of toxicity-related drug safety. Life Sci. Alliance 2018, 1, e201800098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gayvert, K.M.; Madhukar, N.S.; Elemento, O. A Data-Driven Approach to Predicting Successes and Failures of Clinical Trials. Cell Chem. Biol. 2016, 23, 1294–1301. [Google Scholar] [CrossRef]
- Wan, F.; Zeng, J. Deep learning with feature embedding for compound—Protein interaction prediction. bioRxiv 2016, 086033. [Google Scholar]
- Mehta, C.H.; Narayan, R.; Nayak, U.Y. Computational modeling for formulation design. Drug Discov. Today 2018, 24, 781–788. [Google Scholar] [CrossRef]
- Zhao, C.; Jain, A.; Hailemariam, L.; Suresh, P.; Akkisetty, P.; Joglekar, G.; Venkatasubramanian, V.; Reklaitis, G.V.; Morris, K.; Basu, P. Toward intelligent decision support for pharma-ceutical product development. J. Pharm. Innov. 2006, 1, 23–35. [Google Scholar] [CrossRef]
- Meziane, F.; Vadera, S.; Kobbacy, K.; Proudlove, N. Intelligent systems in manufacturing: Current developments and future prospects. Integr. Manuf. Syst. 2000, 11, 218–238. [Google Scholar] [CrossRef]
- Huss, R. The high price of failed clinical trials: Time to rethink the model. Clinical Leader, 3 October 2016. Available online: https://www.clinicalleader.com/doc/the-high-price-of-failed-clinical-trials-time-to-rethink-the-model-0001 (accessed on 10 November 2022).
- Wong, C.H.; Siah, K.W.; Lo, A.W. Estimation of clinical trial success rates and related parameters. Biostatistics 2019, 20, 273–286. [Google Scholar] [CrossRef]
- Thorlund, K.; Haggstrom, J.; Park, J.J.; Mills, E.J. Key design considerations for adaptive clinical trials: A primer for clinicians. BMJ 2018, 360, k698. [Google Scholar] [CrossRef] [Green Version]
- Goldsack, J. Synthetic Control Arms Can Save Time and Money in Clinical Trials. 2019. Available online: https://www.statnews.com/2019/02/05/synthetic-control-arms-clinical-trials/ (accessed on 5 November 2021).
- Unger, J.M.; Vaidya, R.; Hershman, D.L.; Minasian, L.M.; E Fleury, M. Systematic Review and Meta-Analysis of the Magnitude of Structural, Clinical, and Physician and Patient Barriers to Cancer Clinical Trial Participation. Gynecol. Oncol. 2019, 111, 245–255. [Google Scholar] [CrossRef]
- Kolluri, S.; Lin, J.; Liu, R.; Zhang, Y.; Zhang, W. Machine Learning and Artificial Intelligence in Pharmaceutical Research and Development: A Review. AAPS J. 2022, 24, 19. [Google Scholar] [CrossRef] [PubMed]
- Harrer, S.; Shah, P.; Antony, B.; Hu, J. Artificial Intelligence for Clinical Trial Design. Trends Pharmacol. Sci. 2019, 40, 577–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Liu, R.; Lin, J.; Bunn, V.; Zhao, H. Bayesian Semi-parametric Design (BSD) for adaptive dose-finding with multiple strata. J. Biopharm. Stat. 2020, 30, 806–820. [Google Scholar] [CrossRef]
- Liu, R.; Lin, J.; Li, P. Design considerations for phase I/II dose finding clinical trials in Immuno-oncology and cell therapy. Contemp. Clin. Trials 2020, 96, 106083. [Google Scholar] [CrossRef] [PubMed]
- Madhav, N.; Oppenheim, B.; Gallivan, M.; Mulembakani, P.; Rubin, E.; Wolfe, N. Pandemics: Risks, Impacts, and Mitigation. Disease Control Priorities: Improving Health and Reducing Poverty, 3rd ed.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017; Volume 9, pp. 315–345. [Google Scholar]
- Steele, L.; Orefuwa, E.; Bino, S.; Singer, S.R.; Lutwama, J.; Dickmann, P. Earlier Outbreak Detection—A Generic Model and Novel Methodology to Guide Earlier Detection Supported by Data from Low- and Mid-Income Countries. Front. Public Health 2020, 8, 452. [Google Scholar] [CrossRef]
- Gopinath, N. Artificial intelligence: Potential tool to subside SARS-CoV-2 pandemic. Process Biochem. 2021, 110, 94–99. [Google Scholar] [CrossRef]
- Burke, R.M.; Shah, M.P.; E Wikswo, M.; Barclay, L.; Kambhampati, A.; Marsh, Z.; Cannon, J.L.; Parashar, U.D.; Vinjé, J.; Hall, A.J. The Norovirus Epidemiologic Triad: Predictors of Severe Outcomes in US Norovirus Outbreaks, 2009–2016. J. Infect. Dis. 2018, 219, 1364–1372. [Google Scholar] [CrossRef] [Green Version]
- Carlson, C.J.; Dougherty, E.; Boots, M.; Getz, W.; Ryan, S.J. Consensus and conflict among ecological forecasts of Zika virus out-breaks in the United States. Sci. Rep. 2018, 8, 4921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleiven, E.F.; Henden, J.-A.; Ims, R.A.; Yoccoz, N.G. Seasonal difference in temporal transferability of an ecological model: Near-term predictions of lemming outbreak abundances. Sci. Rep. 2018, 8, 15252. [Google Scholar] [CrossRef] [Green Version]
- OECD. Artificial Intelligence in Society; OECD: Paris, France, 2019. [Google Scholar]
- Su, K.; Xu, L.; Li, G.; Ruan, X.; Li, X.; Deng, P.; Li, X.; Li, Q.; Chen, X.; Xiong, Y.; et al. Forecasting influenza activity using self-adaptive AI model and multi-source data in Chongqing, China. Ebiomedicine 2019, 47, 284–292. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.-Y.; Wu, Y.-C.; Lin, M.-H.; Liu, Y.-L.; Tsai, Y.-Y.; Wu, J.-H.; Pan, K.-H.; Ke, C.-J.; Chen, C.-M.; Liu, D.-P.; et al. Applying Machine Learning Models with An Ensemble Approach for Accurate Real-Time Influenza Forecasting in Taiwan: Development and Validation Study. J. Med. Internet Res. 2020, 22, e15394. [Google Scholar] [CrossRef]
- Khan, M.A.; Abidi, W.U.H.; Al Ghamdi, M.A.; Almotiri, S.H.; Saqib, S.; Alyas, T.; Khan, K.M.; Mahmood, N. Forecast the influenza pandemic using machine learning. Comput. Mater. Contin. 2021, 66, 331–340. [Google Scholar]
- Venkatramanan, S.; Sadilek, A.; Fadikar, A.; Barrett, C.L.; Biggerstaff, M.; Chen, J.; Dotiwalla, X.; Eastham, P.; Gipson, B.; Higdon, D.; et al. Forecasting Influenza Activity Using Machine-Learned Mobility Map. Nat. Commun. 2021, 12, 726. [Google Scholar] [CrossRef] [PubMed]
- Soni, U.; Gupta, N.; Sakshi. An Artificial Intelligence Approach for Forecasting Ebola Disease. J. Physics: Conf. Ser. 2021, 1950, 012038. [Google Scholar] [CrossRef]
- Zhang, P.; Chen, B.; Ma, L.; Li, Z.; Song, Z.; Duan, W.; Qiu, X. The Large Scale Machine Learning in an Artificial Society: Prediction of the Ebola Outbreak in Beijing. Comput. Intell. Neurosci. 2015, 2015, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhtar, M.; Kraemer, M.U.G.; Gardner, L.M. A dynamic neural network model for predicting risk of Zika in real time. BMC Med. 2019, 17, 171. [Google Scholar] [CrossRef] [PubMed]
- Kostkova, P.; Pinheiro dos Santos, W.; Massoni, T. ZIKA: Improved surveillance and forecast of Zika virus in Brazil. Eur. J. Public Health 2019, 29 (Suppl. 4), ckz186-085. [Google Scholar] [CrossRef]
- Hemedan, A.A.; Abd Elaziz, M.; Jiao, P.; Alavi, A.H.; Bahgat, M.; Ostaszewski, M.; Schneider, R.; Ghazy, H.A.; Ewees, A.A.; Lu, S. Prediction of the Vaccine-derived Poliovirus Outbreak Incidence: A Hybrid Machine Learning Approach. Sci. Rep. 2020, 10, 5058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, J.L.; Sewell, W.C.; Balzer, L.B.; Krakower, D.S. Artificial Intelligence and Machine Learning for HIV Prevention: Emerging Approaches to Ending the Epidemic. Curr. HIV/AIDS Rep. 2020, 17, 171–179. [Google Scholar] [CrossRef]
- Guo, P.; Liu, T.; Zhang, Q.; Wang, L.; Xiao, J.; Zhang, Q.; Luo, G.; Li, Z.; He, J.; Zhang, Y.; et al. Developing a dengue forecast model using machine learning: A case study in China. PLOS Neglected Trop. Dis. 2017, 11, e0005973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salim, N.A.M.; Wah, Y.B.; Reeves, C.; Smith, M.; Yaacob, W.F.W.; Mudin, R.N.; Dapari, R.; Sapri, N.N.F.F.; Haque, U. Prediction of dengue outbreak in Selangor Malaysia using machine learning techniques. Sci. Rep. 2021, 11, 939. [Google Scholar] [CrossRef]
- Raja, D.B.; Mallol, R.; Ting, C.Y.; Kamaludin, F.; Ahmad, R.; Ismail, S.; Jayaraj, V.J.; Sundram, B.M. Artificial Intelligence Model as Predictor for Dengue Outbreaks. Malays. J. Public Health Med. 2019, 19, 103–108. [Google Scholar] [CrossRef]
- Khan, M.T.; Kaushik, A.C.; Ji, L.; Malik, S.I.; Ali, S.; Wei, D.-Q. Artificial Neural Networks for Prediction of Tuberculosis Disease. Front. Microbiol. 2019, 10, 395. [Google Scholar] [CrossRef]
- Xiong, Y.; Ba, X.; Hou, A.; Zhang, K.; Chen, L.; Li, T. Automatic detection of mycobacterium tuberculosis using artificial intelligence. J. Thorac. Dis. 2018, 10, 1936–1940. [Google Scholar] [CrossRef] [Green Version]
- Amadin, F.I.; Bello, M.E. Prediction of yellow fever using multilayer perceptron neural network classifier. J. Emerg. Trends Eng. Appl. Sci. 2018, 9, 282–286. [Google Scholar]
- Sinha, A.; Rathi, M. COVID-19 prediction using AI analytics for South Korea. Appl. Intell. 2021, 51, 8579–8597. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Ge, Q.; Li, S.; Jin, S.; Xiong, M. Artificial Intelligence Forecasting of COVID-19 in China. arXiv 2020, arXiv:2002.07112. [Google Scholar] [CrossRef]
- Fong, S.J.; Li, G.; Dey, N.; Crespo, R.G.; Herrera-Viedma, E. Composite Monte Carlo decision making under high uncertainty of novel coronavirus epidemic using hybridized deep learning and fuzzy rule induction. Appl. Soft Comput. 2020, 93, 106282. [Google Scholar] [CrossRef]
- Fong, S.J.; Li, G.; Dey, N.; Gonzalez-Crespo, R.; Herrera-Viedma, E. Finding an Accurate Early Forecasting Model from Small Dataset: A Case of 2019-nCoV Novel Coronavirus Outbreak. Int. J. Interact. Multimedia Artif. Intell. 2020, 6, 132. [Google Scholar] [CrossRef]
- Huang, C.J.; Chen, Y.H.; Ma, Y.; Kuo, P.H. Multiple-Input Deep Convolutional Neural Network Model for COVID-19 Forecasting in China. medRxiv 2020. medRxiv:2020.03.23.20041608. [Google Scholar]
- Marini, M.; Chokani, N.; Abhari, R.S. COVID-19 Epidemic in Switzerland: Growth Prediction and Containment Strategy Using Artificial Intelligence and Big Data. medRxiv 2020. medRxiv:2020.03.30.20047472. [Google Scholar]
- Yu, C.S.; Chang, S.S.; Chang, T.H.; Wu, J.L.; Lin, Y.J.; Chien, H.F.; Chen, R.J. A COVID-19 Pandemic Artificial Intelligence–Based System with Deep Learning Forecasting and Automatic Statistical Data Acquisition: Development and Implementation Study. J. Med. Internet Res. 2021, 23, e27806. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
AI in acquiring and analyzing data of a patient in personalizing the treatment.


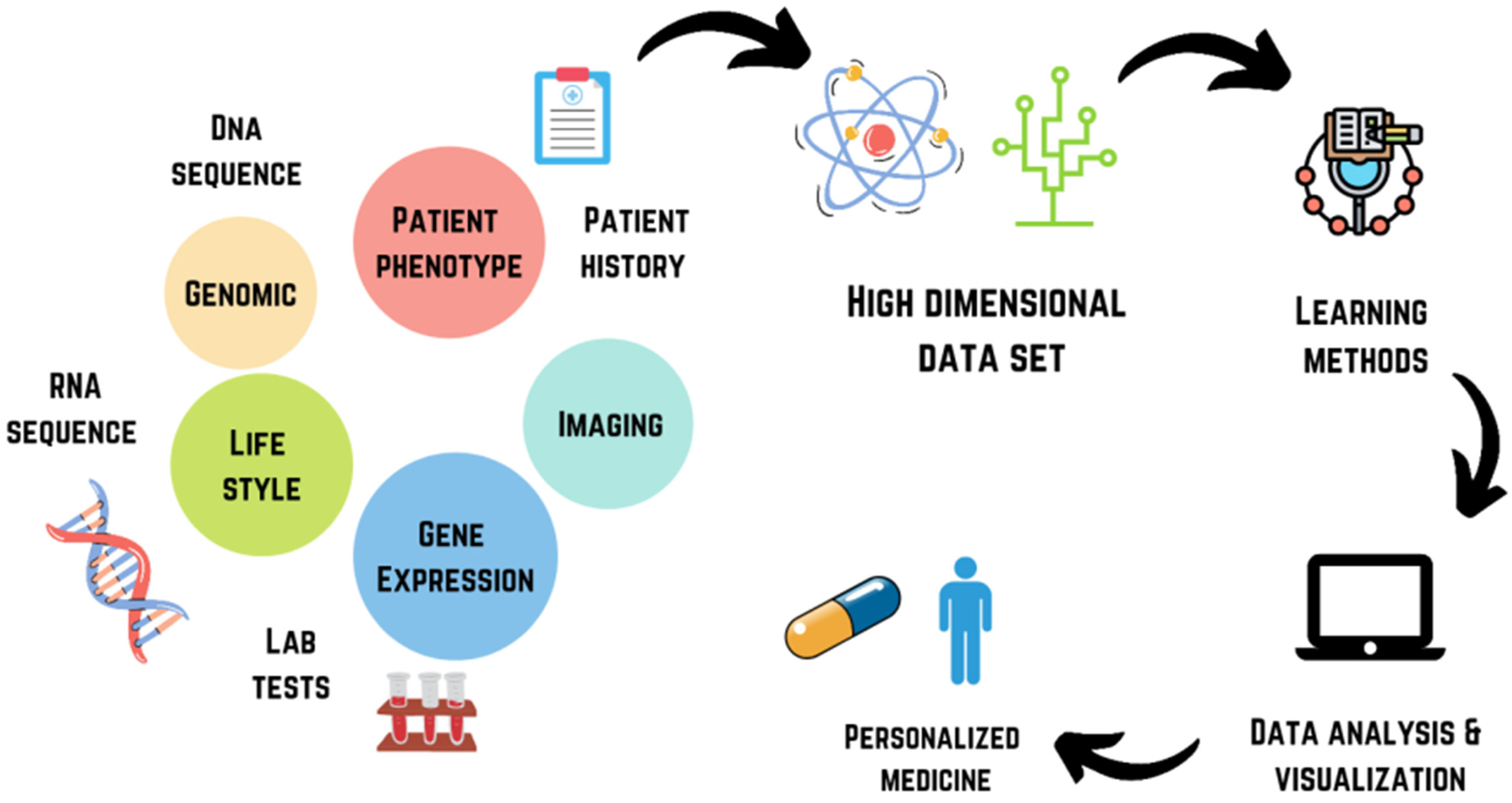{kind=link}
Table 1.
A comprehensive detail of AI applications and their limitations/challenges in healthcare and pharmaceutical research.
Table 1.
A comprehensive detail of AI applications and their limitations/challenges in healthcare and pharmaceutical research.
| Sectors | AI Technologies | Applications | Limitations/Challenges |
|---|---|---|---|
| Disease diagnosis [43,44,48,50] | Deep learning Neural networking Unsupervised learning | Cancer, Dementia, Dermatological diseases, Arial fibrillation |
|
| Digital therapy and personalized treatment [53,57,62,63,91,92] | ANN Evolutionary computational Fuzzy expert systems Hybrid intelligent system Automated treatment planning Radiomics | Image analysis, Data interpretation Administration of vasodilator and anesthesia Radiotherapy Prediction of outcomes and toxicity of radiation therapy |
|
| Virtual medical assistants Case-based reasoning Vector regression technique | Monitoring chronic diseases | ||
| Clinical decision support Intelligent computer-assisted instruction | Management of Diabetes | ||
| Drug discovery [105,106,110,112,113,123,124] | QSPR (Estimation program interface suite) | Determination of physicochemical properties of small molecules |
|
| SMILES | Forecast drug-receptor binding | ||
| Deep learning Neural networks with ADMET predictor and ALGOPS programme | Lipophilicity and solubility prediction | ||
| Chem Mapper Deep learning | Drug-target interaction |
| |
| Deep Tox, eTOXPred, Targe Tox | Drug toxicity prediction | ||
| PrOCTOR | Predict if drug would fail in clinical trial due to toxicity | ||
| BNMs Dirichlet process mixture model mTPI, MCMC | CT design, dose selection |
| |
| OCR, NLP | Patient identification and characterization for CT |
| |
| RBM, AI-enabled wearable device | CT monitoring |
| |
| Video monitoring Wearable sensors | Patient adherence | ||
| Forecasting epidemic/pandemic [135,136,137,140,153,154,155,156] | Deep learning SAAIM MSDII-FFNN ML-AMM | Forecast of seasonal influenza |
|
| HNN | Prediction of Ebola | ||
| DNN | Prediction of Zika |
| |
| RVFL networks with WOA | Prediction of VDPV outbreak | ||
| SVR BNM | Prediction and tracking of dengue outbreak | ||
| ANN, CNN TB-AI | Rapid diagnosis of TB suspects Identify TB bacillus | ||
| MPNN | Diagnosis of yellow fever | ||
| Deep learning CMC in combination with Fuzzy rule PNN + CF CNN Deep neural networks Enterpol combined with bigdata | COVID-19 prediction | ||
| ARIMA | Investigate the dynamic pattern of COVID-19 |
| |
| MLP | Investigate the dynamic pattern of COVID-19 |
| |
| FNN | Investigate the dynamic pattern of COVID-19 |
| |
| LSTM | Investigate the dynamic pattern of COVID-19 |
AI: artificial intelligence; ANN: artificial neural networks; BNMs: Bayesian nonparametric models (BNMs); CT: clinical trial; mTPI: modified toxicity probability interval; MCMC: Markov Chain Monte Carlo; OCR: optical character recognition; NLP: natural language processing; RBM: risk-based monitoring; MSDII-FFNN: machine learning feed-forward propagation neural network model; ML-AMM: machine learning anonymized mobility map; SAAIM: self-adaptive AI model; HNN: hybrid neural network; DNN: dynamic neural network; RVFL: random vector functional link; WOA: whale optimization algorithm; SVR: support vector regression; CNN: convolutional neural network; TB-AI: tuberculosis-AI; MPNN: multilayer perceptron neural network classifiers; CMC: composite Monte Carlo; PNN + CF: polynomial neural network with corrective feedback; ARIMA: autoRegressive integrated moving average; MLP: multilayer perceptron; FNN: feed-forward neural network; LSTM: long short-term memory networks.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bhattamisra, S.K.; Banerjee, P.; Gupta, P.; Mayuren, J.; Patra, S.; Candasamy, M. Artificial Intelligence in Pharmaceutical and Healthcare Research. Big Data Cogn. Comput. 2023, 7, 10. https://doi.org/10.3390/bdcc7010010
AMA Style
Bhattamisra SK, Banerjee P, Gupta P, Mayuren J, Patra S, Candasamy M. Artificial Intelligence in Pharmaceutical and Healthcare Research. Big Data and Cognitive Computing. 2023; 7(1):10. https://doi.org/10.3390/bdcc7010010
Chicago/Turabian StyleBhattamisra, Subrat Kumar, Priyanka Banerjee, Pratibha Gupta, Jayashree Mayuren, Susmita Patra, and Mayuren Candasamy. 2023. "Artificial Intelligence in Pharmaceutical and Healthcare Research" Big Data and Cognitive Computing 7, no. 1: 10. https://doi.org/10.3390/bdcc7010010