Emerging Roles of Cardiotrophin-1 in the Pathogenesis and Biomarker of Atherosclerosis


Laboratory of Cardiovascular Medicine, Tokyo University of Pharmacy and Life Sciences, Tokyo 192-0392, Japan
*
Author to whom correspondence should be addressed.
J 2018, 1(1), 94-105; https://doi.org/10.3390/j1010010
Submission received: 4 September 2018
/
Revised: 18 September 2018
/
Accepted: 18 September 2018
/
Published: 20 September 2018
(This article belongs to the Special Issue Atherosclerosis: Molecular Mechanisms and Therapeutic Advances)
Abstract
:Cardiotrophin-1 (CT-1), an interleukin-6 family cytokine, is known as an active inducer capable of cardiac hypertrophy and vascular stiffness in hypertensive heart disease. CT-1 is expressed at high levels in the heart, vascular endothelial cells (ECs), and adipocytes. CT-1 stimulates inflammatory and proatherogenic molecule expression in human monocytes and ECs, as well as monocyte-EC adhesion. CT-1 enhances oxidized low-density lipoprotein-induced foam-cell formation in human monocyte-derived macrophages. CT-1 stimulates the migration, proliferation, and colloagen-1 production in human vascular smooth muscle cells. Chronic CT-1 infusion into Apoe−/− mice accelerates the development of aortic atherosclerotic lesions. CT-1 is expressed at high levels in ECs and macrophage foam cells within atheromatous plaques in Apoe−/− mice. A blockade of CT-1 using anti-CT-1 neutralizing antibody results in the prevention of atherogenesis in Apoe−/− mice. Plasma CT-1 concentrations are elevated in patients with hypertensive heart disease, ischemic heart disease, and metabolic syndrome, and are positively associated with the severity of cardiac hypertrophy, heart failure, and atherosclerosis. Increased plasma concentration of CT-1 is a predictor of death and heart failure following acute myocardial infarction. Therefore, CT-1 serves a novel therapeutic target for atherosclerosis and related diseases. Plasma CT-1 may be a reliable biomarker for atherosclerotic cardiovascular diseases.
1. Introduction
Hypertension is regarded as a promotive and risk factor of atherosclerosis [1]. Several lines of evidence have shown that endothelial injury, an initial step of atherosclerosis, is caused by hypertension-induced pressure overload, stretch, or shear stress on the artery wall [2]. As a result, endothelial inflammation characterized as increased expression of inflammatory cytokines and adhesion molecules as well as the migration and proliferation of arterial smooth muscle cells (SMCs) and the production of extracellular matrix production, such as collagen, fibronectin, elastin, and matrix metalloproteinase (MMP), by SMCs [2]. These phenomena are called hypertension-induced arteriosclerosis and remodeling. In addition, a lipid core derived by oxidized low-density lipoprotein (oxLDL)-induced macrophage foam-cell formation is essential for atherosclerosis [3]. The formation of atherosclerosis is caused by several vasoconstrictors increased in hypertension. We have clarified that angiotensin II, endothelin-1, urotensin II, kisspeptin-10, and 5-hydroxytryptamine (serotonin) play important roles in linking hypertension to atherosclerosis [4,5,6,7,8]. In contrast, a variety of novel hypotensive peptides, such as salusin-α, heregulin-β1, urocortin-1, omentin-1, and catestatin contribute to suppress atherosclerosis [9,10,11,12,13]. Recent studies have shown that cariotrophin-1 (CT-1) is an active inducer capable of cardiac hypertrophy and vascular stiffness in hypertensive heart disease [14]. We have provided the first evidence that CT-1 is expressed at high levels in atherosclerotic lesions and shows proatherogenic effects [15]. Other studies have reported that plasma concentrations of CT-1 are increased in patients with coronary artery disease (CAD) [16].
The present review introduces the recent accumulating evidence regarding the roles of CT-1 in the pathophysiology of atherosclerosis and the potential biomarker of cardiovascular and metabolic diseases.
2. Structure, Expression, and Function of CT-1
CT-1 is a new member of the interleukin (IL)-6 cytokine family that was originally cloned from a mouse embryoid body cDNA library based on its ability to induce hypertrophy in neonatal cardiomyocytes [17]. cDNA clones of human CT-1 were isolated by screening a heart cDNA library with a mouse CT-1 probe [17]. The DNA sequence of these clones encodes a protein of 201 amino acids that is 80% identical with the 203 amino acid residue of mouse CT-1 [18]. CT-1 has a molecular weight of 21.5 kDa. Human and mouse CT-1 lack a conventional, hydrophobic, N-terminal amino acid sequence indicative of a secretion signal [18]. The amino acid sequence of rat CT-1 is 80% and 94% identical to those of human CT-1 and mouse CT-1, respectively [19]. The coding region of CT-1 is contained on 3 exons and is located on human chromosome 16p11.1–16p11.2 [18].
CT-1 is expressed in the cardiovascular system as well as the brain, thymus, lungs, kidneys, liver, intestine, testes, prostate, skeletal muscles, and adipose tissue [18,19,20,21,22,23]. In cardiovascular cells, cardiomyocytes, cardiac fibroblasts, vascular endothelial cells (ECs), vascular SMCs, and macrophages abundantly express CT-1 [15,24,25,26,27]. Expression of CT-1 is upregulated by mechanical stretching, hypoxia, and hormonal substances such as angiotensin II, aldosterone, noradrenaline, urocortin-1, fibroblast growth factor-2, heparin-binding epidermal growth factor-like growth factor, insulin, glucose, and reactive oxygen species [28,29,30,31,32,33,34,35,36,37]. CT-1 is produced in the heart and secreted via the coronary sinus into peripheral circulation [38]. The concentrations of CT-1 in the circulating blood are directly correlated with the expression levels of CT-1 in the myocardium [39]. Plasma CT-1 concentration is transiently increased by cardiopulmonary exercise in healthy subjects [40]. It may be involved in a mechanism that exercise-induced noradrenaline release and hypoxia increase plasma CT-1 concentration. Adipocytes participate as an important source of plasma CT-1 under hyperglycemic conditions [23]. Therefore, CT-1 could act not only in a paracrine manner, but also as a hormone or adipocytokine involved in the regulation of several physiological/pathophysiological functions.
CT-1 plays a crucial role in cardiac development [41]. CT-1 has a great number of different functions, such as providing myocardial protection, predisposing the heart to pathological conditions, and producing hemodynamic effects and endocrine properties (secreting atrial natriuretic peptide and brain natriuretic peptide) [20,21,22,42,43]. CT-1 participates in cardiovascular remodeling induced by hypertensive heart disease, ischemic heart disease, and heart failure [20,42]. Other than the heart, CT-1 induces the growth of the liver, kidneys, spleen, and airway SMCs, and the atrophy of the thymus, and increases the number of platelets and red blood cells [44,45]. CT-1 has the regulatory effects on glucose and lipid metabolism [46], as well as survival-promoting effects on the nervous system [20].
3. Receptor and Signaling of CT-1
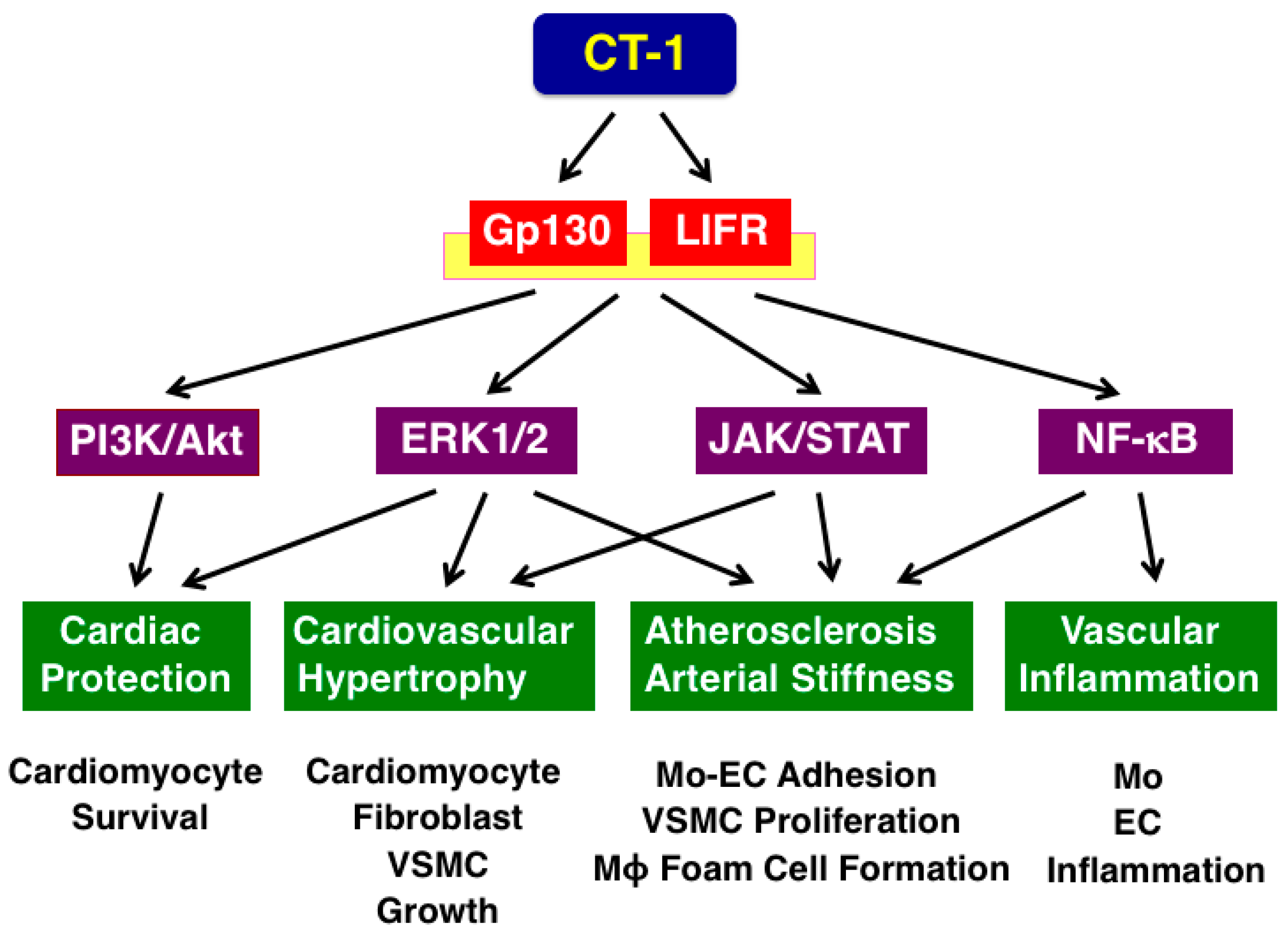
CT-1 binds to glycoprotein 130 (gp130) and leukemia inhibitory factor receptor (LIFR) heterodimer [22,47]. It has been recently reported to recruit an uncharacterized α receptor (CT-1Rα) [48], which confers CT-1 high-potency trophic signaling for motor neurons [49]. Subsequently, CT-1 activates the phosphatidylinositol 3-kinase (PI3K)/Akt, c-Src tyrosine kinase/extracellular signal-regulated kinase (ERK) 1/2, Janus kinase (JAK)/signal transducers and activators of transcription (STAT), and nuclear factor-κB (NF-κB) pathways [22,42]. Thereby, CT-1 exerts a variety of biological responses via these signaling pathways. The cardiovascular outcomes for each of the pathways are summarized in Figure 1.
4. Roles of CT-1 in Hypertension
Plasma CT-1 concentrations are positively correlated with systolic blood pressure and pulse-wave velocity (PWV), an index of arterial stiffness, and are significantly elevated in untreated and treated patients with hypertension [28,50] (Table 1). Plasma CT-1 concentrations have been demonstrated to be associated with hypertensive heart disease [51]. Plasma CT-1 concentrations are correlated positively with left ventricular hypertrophy, and negatively with ejection fraction in hypertensive patients [52,53]. Plasma CT-1 concentration further increases in the presence of left ventricular hypertrophy and heart failure in hypertensive patients [53] (Table 1). Overexpression of CT-1 is associated with myocardial fibrosis with increased collagen expression in hypertensive patients with heart failure [54].
In spontaneously hypertensive rats compared with Wistar normotensive rats, CT-1 expression in ventricular tissue is increased, and vascular smooth muscle cell (VSMC) proliferation and collagen-1, collagen-3, fibronectin, and elastin production in VSMCs are enhanced by CT-1 [27,28]. These findings indicate that CT-1 plays important roles in hypertension-induced cardiac and vascular hypertrophy, fibrosis, and remodeling.
5. Roles of CT-1 in Metabolic Syndrome
CT-1 reduces fatty acid synthesis and insulin receptor substrate-1 expression, and induces insulin resistance in adipocytes in vitro [55]. Exogenous CT-1 administration into mice increases energy expenditure, fatty acid oxidation, and glucose cellular uptake [56]. Chronic administration of CT-1 increases lipolysis, fatty acid oxidation, mitochondrial biogenesis, and adipocyte shrinkage [56]. However, the relationship between the in vitro and in vivo effects of CT-1 and its plasma concentrations in human metabolic diseases remains unknown so far.
Adipocytes participate as an important source of CT-1 under hyperglycemic conditions [23]. A 24 h circadian rhythm of plasma CT-1 concentrations was observed in normal-weight subjects, which was altered in overweight patients [57]. Plasma CT-1 concentrations are positively correlated with diastolic blood pressure or triglyceride concentration in women with polycystic ovary syndrome [58]. Plasma CT-1 concentrations are increased in patients with metabolic syndrome, diabetes, or obesity [23,59,60] (Table 1). In addition, common genetic variation in the human CTF1 locus, encoding CT-1, contributes to insulin sensitivity in humans, indicating the insulin-desensitizing effect of CT-1 [61].
6. Atheroprone Effects of CT-1
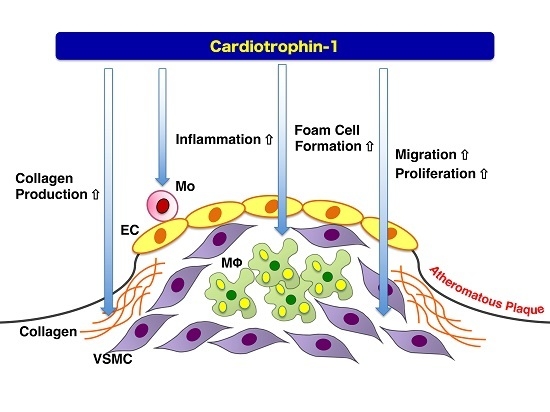
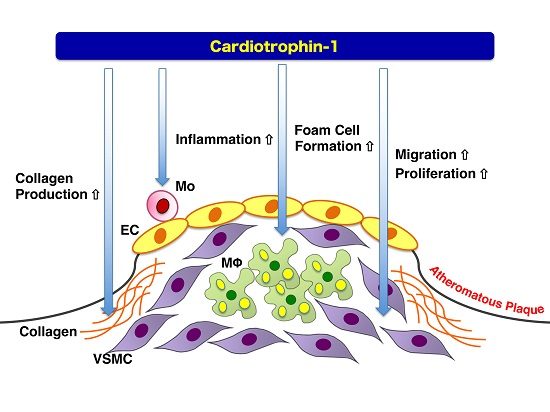
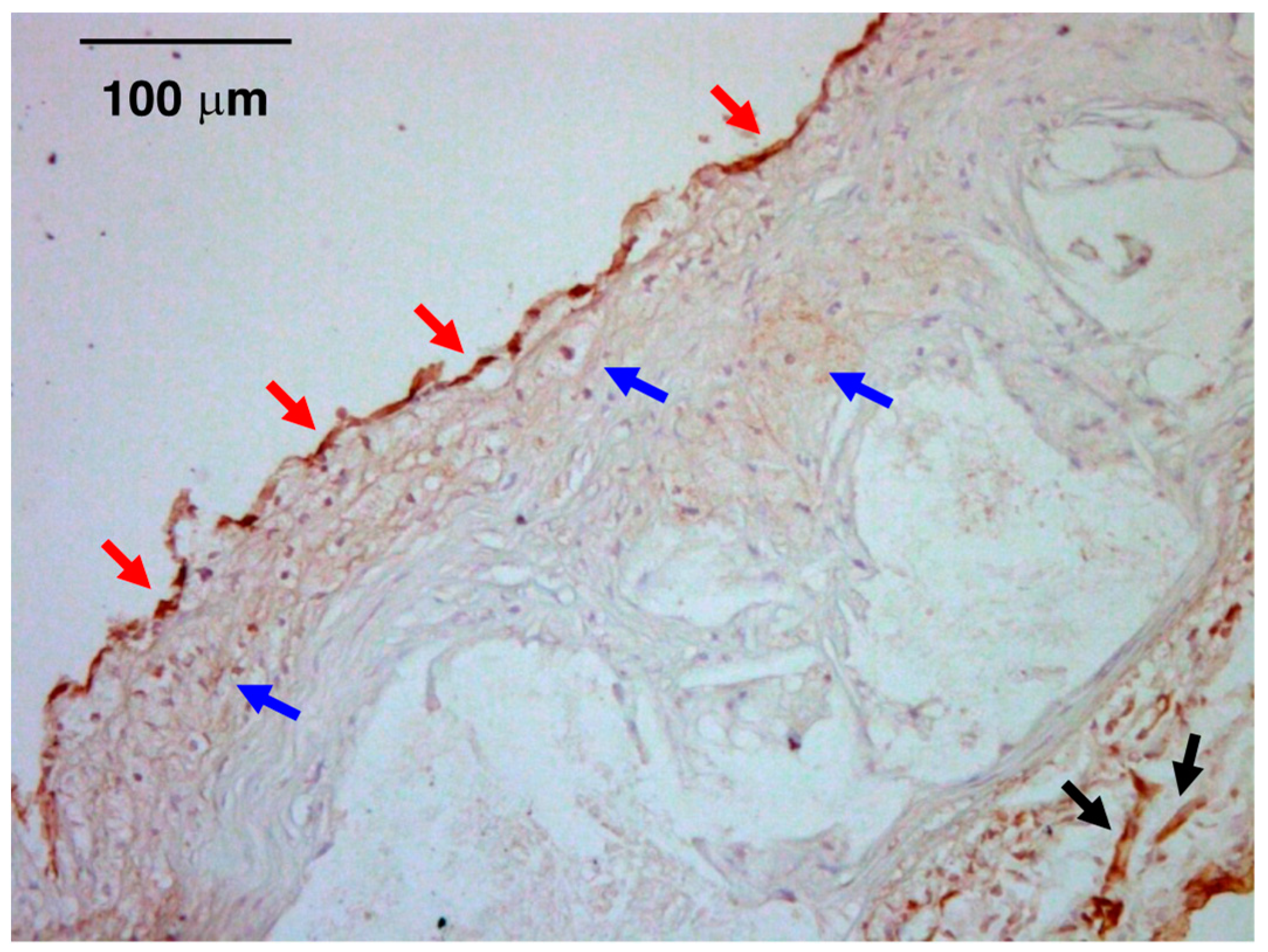
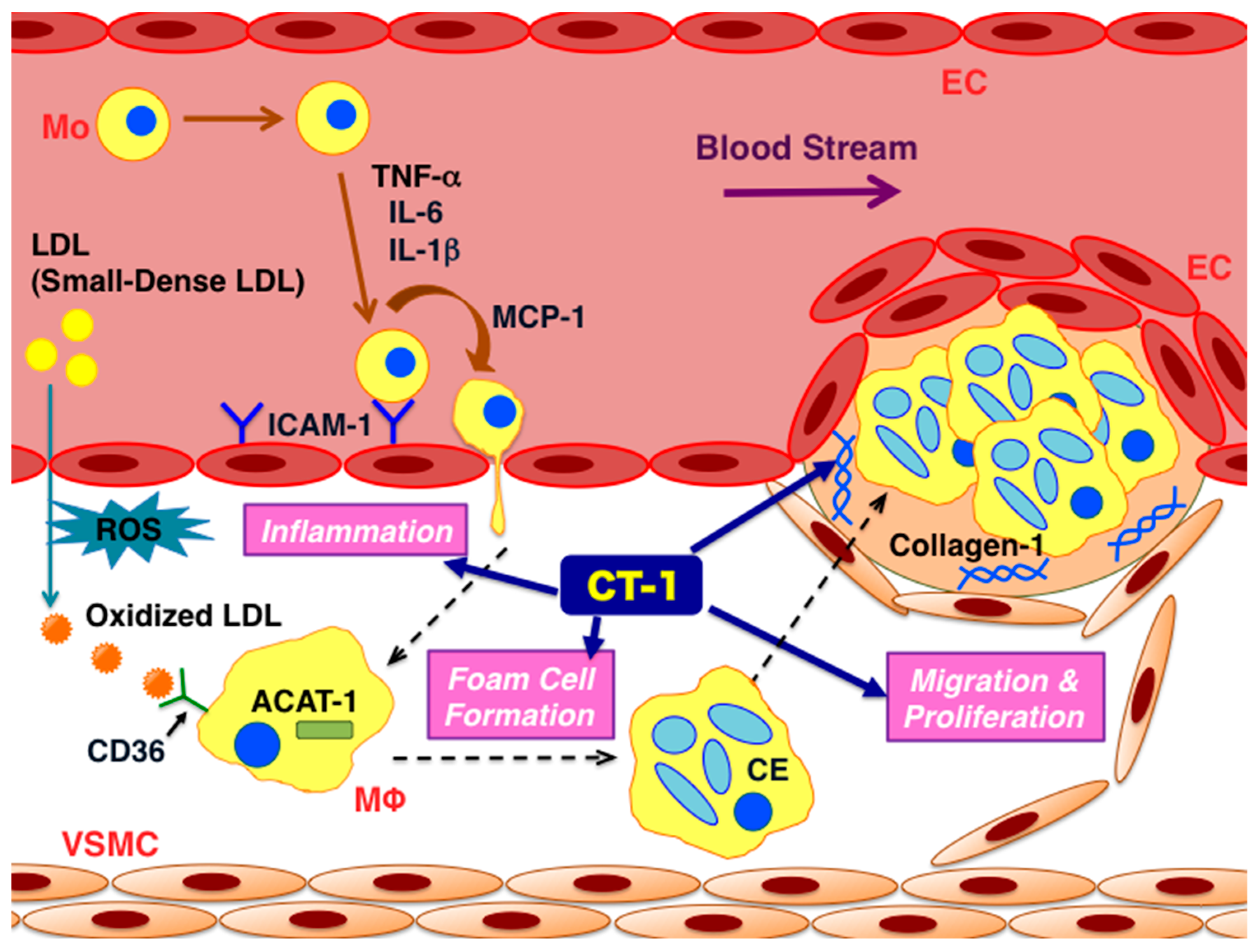
Our previous study has shown the abundant expression of CT-1 in ECs, macrophages, and SMCs within atherosclerotic lesions (Figure 2) [15]. The relationship between CT-1 and the formation of atherosclerosis has been clarified. The direct atherogenic effects of CT-1 on vascular wall cells are shown in Figure 3. CT-1 stimulates the migration and proliferation of human umbilical vein ECs [64], which contributes to atherogenesis as well as angiogenesis. CT-1 stimulates the synthesis of inflammatory cytokines and proatherogenic molecules, such as IL-6, monocyte chemoattractant protein-1, intercellular adhesion molecule-1, and MMP-1, in human ECs [26,65,66,67]. CT-1 stimulates the synthesis of IL-6, IL-1β, and tumor necrosis factor-α (TNF-α) in human monocytes [68,69,70]. Thereby, CT-1 induces human monocyte–EC adhesion and monocyte migration [26]. CT-1 also stimulates superoxide production via activating nicotinamide adenine dinucleotide phosphate (NADPH) oxidase in human monocytes [71]. CT-1 enhances oxLDL-induced foam-cell formation via acyl-coenzyme A: cholesterol acyltransferase-1 and CD36 upregulation in human monocyte-derived macrophages [15]. CT-1 increases the migration, proliferation, and collagen-1 production via activating ERK1/2, JAK/STAT, and NF-κB pathways in human aortic SMCs [15]. CT-1 also induces apoptosis via caspase-3, p53, p21, p16, and NF-κB upregulation in rat aortic SMCs [72]. However, CT-1 has no effects on the production of plasminogen activator inhibitor-1 in the human coronary artery and aortic SMCs [73].
Administration of CT-1 into Wistar rats increases vascular fibrosis by increasing collagen-1, collagen-3, fibronectin, MMP-2, MMP-9, and MMP-13 production in carotid arteries [27,74]. Chronic CT-1 infusion into Apoe−/− mice accelerates the development of aortic atherosclerotic lesions with inflammatory responses in infiltrated monocytes/macrophages [15]. Neutralization of endogenous CT-1 with chronic infusion of anti-CT-1 antibody prevents the development of atherosclerotic lesions with reduced intraplaque monocyte/macrophage infiltration in Apoe−/− mice [15]. Deficiency of CT-1 results in the decrease in arterial stiffness and myocardial and arterial fibrosis with suppressing collagen-1, collagen-3, fibronectin, MMP-2, MMP-9, and MMP-13 production in mice [72,75].
7. Plasma/Tissue Levels of CT-1 in Atherosclerotic Cardiovascular Disease
Plasma concentrations of CT-1 are elevated in various diseases that are associated with endothelial dysfunction, such as hypertension, diabetes, metabolic syndrome, acute coronary syndrome, heart failure, and chronic renal disease [14,16,23,59,76,77,78,79] (Table 1). Circulating CT-1 concentrations are positively related to arterial stiffness assessed by brachial-ankle PWV independent of traditional cardiometabolic risk factors (diabetes, insulin resistance, lipid profile, high-sensitivity C-reactive protein, creatinine, etc.) [80]. Plasma CT-1 is a predictor of hypertension- and diabetes-induced target organ damage and cardiovascular risk [60]. CT-1 is a reliable biomarker of heart failure (area under the curve: 0.831) in hypertensive patients [81]. Plasma CT-1 concentrations are increased in the accordance with the severity of heart failure, and are helpful in predicting mortality in patients with heart failure [82]. Plasma CT-1 concentrations are also elevated in patients with aortic stenosis or hypertrophic cardiomyopathy [61,62]. Expression of CT-1 is increased in the right atrial and ventricular myocardium in patients with Tetralogy of Fallot, which is associated with hypoxemia-induced activation of the JAK/STAT pathway [83].
Plasma CT-1 concentrations are further increased following the onset of acute myocardial infarction [75]. In a postinfarcted heart, CT-1 expression is increased in the infarcted myocardium in the early phase (24 h to eight weeks), and in the viable myocardium in the chronic phase of wound healing (eight weeks) [84]. The early expression of CT-1 in the infarcted myocardium may represent adaptive and protective phenomena that are beneficial in reducing cardiomyocyte loss and inducing hypertrophy of the remaining cardiomyocytes so that overall ventricular function is remained [85]. CT-1 expression in the late phase of wound healing and the onset of heart failure may contribute to ventricular dilation by inducing hypertrophy of cardiomyocytes with increased cell length [86]. CT-1 stimulates the differentiation of human cardiac fibroblast to myofibroblasts [54]. CT-1 is released from myocardium after coronary artery bypass grafting [87].
Further, increased plasma concentration of CT-1 is a predictor of death and heart failure following acute myocardial infarction [88]. These findings suggest that plasma CT-1 also may be beneficial as a possible biomarker for major adverse cardiac events after acute myocardial infarction.
8. Pharmacological Intervention Against CT-1
Recent studies have shed some light on pharmacological intervention against CT-1. As described above, chronic infusion of an anti-CT-1 neutralizing antibody into Apoe−/− mice prevents the development of atherosclerosis [15]. However, to our knowledge, neither the anti-CT-1 neutralizing antibody nor antagonists/blockers for the CT-1 receptor (gp130 and LIFR complex) have been developed as a medical procedure so far. CT-1 transcript levels in peripheral blood mononuclear cells are reduced after lifestyle intervention in obese children [89]. Oral administration of baicalin, a major bioactive ingredient of the traditional Chinese medicine, decreases circulating CT-1 levels in patients with CAD and rheumatoid arthritis [90]. Zhibital, a traditional Chinese medicine used for treating blood lipid disorders, and atorvastatin also reduce circulating CT-1 levels in CAD patients [91]. Simvastatin attenuates CT-1-induced cardiac hypertrophy via JAK/STAT pathway in vitro and in vivo [92,93]. A liver X receptor agonist (TO901317) inhibits oxLDL-induced mitogenic effects of CT-1 [94]. Etanercept, a TNF-α inhibitor, decreases CT-1 levels secreted from neonatal rat cardiomyocytes [95]. These interventions against CT-1 may provide therapeutic advances for atherosclerotic cardiovascular diseases.
9. Conclusions
CT-1 is known to be a mediator capable of hypertension-induced cardiovascular hypertrophy and remodeling. CT-1 plays a key role in the pathophysiology of atherogenesis in the presence or absence of influence of hypertension. A blockade of CT-1 is expected to emerge as a new line of therapy against atherosclerosis and related diseases. In addition, CT in the circulating blood is a promising biomarker for estimating the presence, severity, and prognosis of atherosclerotic cardiovascular diseases.
Author Contributions
T.W. wrote the manuscript, H.K. drew the figures, and K.S. performed CT-1 immunostaining.
Acknowledgments
This work was supported in part by a Grant-in-Aid for Scientific Research © (26460659 and 17K08993 to T.W.) from the Japan Society for the Promotion of Science.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Watanabe, T.; Kanome, T.; Miyazaki, A. Relationship between hypertension and atherosclerosis: From a viewpoint of the most potent vasoconstrictor human urotensin II. Curr. Hypertens. Rev. 2006, 2, 237–246. [Google Scholar] [CrossRef]
- Dzau, V.J. Atherosclerosis and hypertension: Mechanisms and interrelationships. J. Cardiovasc. Pharmacol. 1990, 15, S59–S64. [Google Scholar] [CrossRef] [PubMed]
- Maiolino, G.; Rossitto, G.; Caielli, P.; Bisogni, V.; Rossi, G.P.; Calò, L.A. The role of oxidized low-density lipoproteins in atherosclerosis: The myths and the facts. Mediat. Inflamm 2013, 2013, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Sato, K.; Itoh, F.; Noguchi, Y.; Fujimoto, K.; Koyama, T.; Shichiri, M. Emerging roles for vasoactive peptides in diagnostic and therapeutic strategies against atherosclerotic cardiovascular diseases. Curr. Protein Pept. Sci. 2013, 14, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Pakala, R.; Katagiri, T.; Benedict, CR. Angiotensin II and serotonin potentiate endothelin-1-induced vascular smooth muscle cell proliferation. J. Hypertens. 2001, 19, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Arita, S.; Shiraishi, Y.; Suguro, T.; Sakai, T.; Hongo, S.; Miyazaki, A. Human urotensin II promotes hypertension and atherosclerotic cardiovascular diseases. Curr. Med. Chem. 2009, 16, 550–563. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Shirai, R.; Hontani, M.; Shinooka, R.; Hasegawa, A.; Kichise, T.; Yamashita, T.; Yoshizawa, H.; Watanabe, R.; Matsuyama, T.; et al. Potent vasoconstrictor kisspeptin-10 induces atherosclerotic plaque progression and instability: Reversal by its receptor GPR54 antagonist. J. Am. Heart Assoc. 2017, 6, e005790. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Koba, S. Roles of serotonin in atherothrombosis and related diseases. In Traditional and Novel Risk Factors in Atherothrombosis; Efrain Gaxiola, Ed.; INTECH: Rijeka, Croatia, 2012; pp. 57–70. [Google Scholar]
- Watanabe, T.; Sato, K.; Itoh, F.; Iso, Y.; Nagashima, M.; Hirano, T.; Shichiri, M. The roles of salusins in atherosclerosis and related cardiovascular diseases. J. Am. Soc. Hypertens. 2011, 5, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Watanabe, T.; Iso, Y.; Koba, S.; Sakai, T.; Nagashima, M.; Arita, S.; Hongo, S.; Ota, H.; Kobayashi, Y.; et al. Preventive effects of heregulin-β1 on macrophage foam cell formation and atherosclerosis. Circ. Res. 2009, 105, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, A.; Sato, K.; Shirai, R.; Watanabe, R.; Yamamoto, K.; Watanabe, K.; Nohtomi, K.; Hirano, T.; Watanabe, T. Vasoprotective effects of urocortin 1 against atherosclerosis in vitro and in vivo. PLoS ONE 2014, 9, e110866. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Watanabe, R.; Konii, H.; Shirai, R.; Sato, K.; Matsuyama, T.; Ishibashi-Ueda, H.; Koba, S.; Kobayashi, Y.; Hirano, T.; et al. Counteractive effects of omentin-1 against atherogenesis. Cardiovasc. Res. 2016, 110, 118–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, M.; Ozawa, N.; Mori, Y.; Takahashi, Y.; Watanabe-Kominato, K.; Shirai, R.; Watanabe, R.; Sato, K.; Matsuyama, T.; Ishibashi-Ueda, H.; et al. Catestatin prevents macrophage-driven atherosclerosis but not arterial injury-induced neointimal hyperplasia. Thromb. Haemost. 2018, 118, 182–194. [Google Scholar] [CrossRef] [PubMed]
- González, A.; López, B.; Ravassa, S.; Beaumont, J.; Zudaire, A.; Gallego, I.; Brugnolaro, C.; Díez, J. Cardiotrophin-1 in hypertensive heart disease. Endocrine 2012, 42, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Konii, H.; Sato, K.; Kikuchi, S.; Okiyama, H.; Watanabe, R.; Hasegawa, A.; Yamamoto, K.; Itoh, F.; Hirano, T.; Watanabe, T. Stimulatory effects of cardiotrophin 1 on atherosclerosis. Hypertension 2013, 62, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Talwar, S.; Squire, I.B.; Downie, P.F.; Davies, J.E.; Ng, L.L. Plasma N terminal pro-brain natriuretic peptide and cardiotrophin 1 are raised in unstable angina. Heart 2000, 84, 421–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennica, D.; King, K.L.; Shaw, K.J.; Luis, E.; Rullamas, J.; Luoh, S.M.; Darbonne, W.C.; Knutzon, D.S.; Yen, R.; Chien, K.R.; et al. Expression cloning of cardiotrophin 1, a cytokine that induces cardiac myocyte hypertrophy. Proc. Natl. Acad. Sci. USA 1995, 92, 1142–1146. [Google Scholar] [CrossRef] [PubMed]
- Pennica, D.; Swanson, T.A.; Shaw, K.J.; Kuang, W.J.; Gray, C.L.; Beatty, B.G.; Wood, W.I. Human cardiotrophin-1: Protein and gene structure, biological and binding activities, and chromosomal localization. Cytokine 1996, 8, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, M.; Saito, Y.; Miyamoto, Y.; Kuwahara, K.; Ogawa, E.; Nakagawa, O.; Harada, M.; Masuda, I.; Nakao, K. cDNA cloning of rat cardiotrophin-1 (CT-1): Augmented expression of ct-1 gene in ventricle of genetically hypertensive rats. Biochem. Biophys. Res. Commun. 1996, 219, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Latchman, D.S. Cardiotrophin-1: A novel cytokine and its effects in the heart and other tissues. Pharmacol. Ther. 2000, 85, 29–37. [Google Scholar] [CrossRef]
- Jougasaki, M. Cardiotrophin-1 in cardiovascular regulation. Adv. Clin. Chem. 2010, 52, 41–76. [Google Scholar] [PubMed]
- Stejskal, D.; Ruzicka, V. Cardiotrophin-1 review. Biomed. Pap Med. Fac. Univ. Palacky Olomuc Czechsolv. Repub. 2008, 152, 9–19. [Google Scholar] [CrossRef]
- Natal, C.; Fortuño, M.A.; Restituto, P.; Bazán, A.; Colina, I.; Díez, J.; Varo, N. Cardiotrophin-1 is expressed in adipose tissue and upregulated in the metabolic syndrome. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E52–E60. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Z.; Pennica, D.; Wood, W.I.; Chien, K.R. Cardiotrophin-1 displays early expression in the murine heart tube and promotes cardiac myocyte survival. Development 1996, 122, 419–428. [Google Scholar] [PubMed]
- Tsuruda, T.; Jougasaki, M.; Boerrigter, G.; Huntley, B.K.; Chen, H.H.; D’Assoro, A.B.; Lee, S.C.; Larsen, A.M.; Cataliotti, A.; Burnett, J.C., Jr. Cardiotrophin-1 stimulation of cardiac fibroblast growth: Roles for glycoprotein 130/leukemia inhibitory factor receptor and the endothelin type A receptor. Circ. Res. 2002, 90, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Ichiki, T.; Jougasaki, M.; Setoguchi, M.; Imamura, J.; Nakashima, H.; Matsuoka, T.; Sonoda, M.; Nakamura, K.; Minagoe, S.; Tei, C. Cardiotrophin-1 stimulates intercellular adhesion molecule-1 and monocyte chemoattractant protein-1 in human aortic endothelial cells. Am. J. Physiol. Heart Circ. Physiol. 2008, 294, H750–H763. [Google Scholar] [CrossRef] [PubMed]
- López-Andrés, N.; Fortuño, M.A.; Diez, J.; Zannad, F.; Lacolley, P.; Rossignol, P. Vascular effects of cardiotrophin-1: A role in hypertension? J. Hypertens. 2010, 28, 1261–1272. [Google Scholar] [CrossRef] [PubMed]
- Pemberton, C.J.; Raudsepp, S.D.; Yandle, T.G.; Cameron, V.A.; Richards, A.M. Plasma cardiotrophin-1 is elevated in human hypertension and stimulated by ventricular stretch. Cardiovasc. Res. 2005, 68, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hishinuma, S.; Funamoto, M.; Fujio, Y.; Kunisada, K.; Yamauchi-Takihara, K. Hypoxic stress induces cardiotrophin-1 expression in cardiac myocytes. Biochem. Biophys. Res. Commun. 1999, 264, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Fukuzawa, J.; Booz, G.W.; Hunt, R.A.; Shimizu, N.; Karoor, V.; Baker, K.M.; Dostal, D.E. Cardiotrophin-1 increases angiotensinogen mRNA in rat cardiac myocytes through STAT3: An autocrine loop for hypertrophy. Hypertension 2000, 35, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- López-Andrés, N.; Iñigo, C.; Gallego, J.; Díez, J.; Fortuño, M.A. Aldosterone induces cardiotrophin-1 expression in HL-1 adult cardiomyocytes. Endocrinology 2008, 149, 4970–4978. [Google Scholar] [CrossRef] [PubMed]
- Funamoto, M.; Hishinuma, S.; Fujio, Y.; Matsuda, Y.; Kunisada, K.; Oh, H.; Negoro, S.; Tone, E.; Kishimoto, T.; Yamauchi-Takihara, K. Isolation and characterization of the murine cardiotrophin-1 gene: Expression and norepinephrine-induced transcriptional activation. J. Mol. Cell. Cardiol. 2000, 32, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Janjua, S.; Lawrence, K.M.; Ng, L.L.; Latchman, D.S. The cardioprotective agent urocortin induces expression of CT-1. Cardiovasc. Toxicol. 2003, 3, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.S.; Jeyaraman, M.; Wen, G.B.; Fandrich, R.R.; Dixon, I.M.; Cattini, P.A.; Kardami, E. High-but not low-molecular weight FGF-2 causes cardiac hypertrophy in vivo; possible involvement of cardiotrophin-1. J. Mol. Cell. Cardiol. 2007, 42, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Park, J.H.; Lee, S.; Lim, H.J.; Choi, H.E.; Park, H.Y. HB-EGF induces delayed STAT3 activation via NF-kappaB mediated IL-6 secretion in vascular smooth muscle cell. Biochim. Biophys. Acta 2007, 1773, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, Z.; Huang, F.; Xing, Z.; Wang, H.; Li, Z. Pioglitazone inhibits hypertrophy induced by high glucose and insulin in cultured neonatal rat cardiomyocytes. Pharmazie 2007, 62, 925–929. [Google Scholar] [PubMed]
- Ateghang, B.; Wartenberg, M.; Gassmann, M.; Sauer, H. Regulation of cardiotrophin-1 expression in mouse embryonic stem cells by HIF-1α and intracellular reactive oxygen species. J. Cell Sci. 2006, 119, 1043–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asai, S.; Saito, Y.; Kuwahara, K.; Mizuno, Y.; Yoshimura, M.; Higashikubo, C.; Tsuji, T.; Kishimoto, I.; Harada, M.; Hamanaka, I.; et al. The heart is a source of circulating cardiotrophin-1 in humans. Biochem. Biophys. Res. Commun. 2000, 279, 320–323. [Google Scholar] [CrossRef] [PubMed]
- González, A.; Ravassa, S.; Loperena, I.; López, B.; Beaumont, J.; Querejeta, R.; Larman, M.; Díez, J. Association of depressed cardiac gp130-mediated antiapoptotic pathways with stimulated cardiomyocyte apoptosis in hypertensive patients with heart failure. J. Hypertens. 2007, 25, 2148–2157. [Google Scholar]
- Limongelli, G.; Calabrò, P.; Maddaloni, V.; Russo, A.; Masarone, D.; D’Aponte, A.; Roselli, T.; Bonauro, R.; D’Alessandro, R.; D’Andrea, A.; et al. Cardiotrophin-1 and TNF-α circulating levels at rest and during cardiopulmonary exercise test in athletes and healthy individuals. Cytokine 2010, 50, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Wollert, K.C.; Chien, K.R. Cardiotrophin-1 and the role of gp130-dependent signaling pathways in cardiac growth and development. J. Mol. Med. 1997, 75, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, P.; Limongelli, G.; Riegler, L.; Maddaloni, V.; Palmieri, R.; Golia, E.; Roselli, T.; Masarone, D.; Pacileo, G.; Golino, P.; et al. Novel insights into the role of cardiotrophin-1 in cardiovascular diseases. J. Mol. Cell. Cardiol. 2009, 46, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Hamanaka, I.; Saito, Y.; Nishikimi, T.; Magaribuchi, T.; Kamitani, S.; Kuwahara, K.; Ishikawa, M.; Miyamoto, Y.; Harada, M.; Ogawa, E.; et al. Effects of cardiotrophin-1 on hemodynamics and endocrine function of the heart. Am. J. Physiol. Heart Circ. Physiol. 2000, 279, H388–H396. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Yang, R.; Keller, G.A.; Ryan, A.; Ko, A.; Finkle, D.; Swanson, T.A.; Li, W.; Pennica, D.; Wood, W.I.; et al. In vivo effects of cardiotrophin-1. Cytokine 1996, 8, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Zhou, D.; Sow, C.Y.; Bai, T.R. Cardiotrophin-1 alters airway smooth muscle structure and mechanical properties in airway explants. Am. J. Physiol. Lung Cell. Mol. Physiol. 2004, 287, L1165–L1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-Aliaga, M.J.; Pérez-Echarri, N.; Marcos-Gómez, B.; Larequi, E.; Gil-Bea, F.J.; Viollet, B.; Gimenez, I.; Martínez, J.A.; Prieto, J.; Bustos, M. Cardiotrophin-1 is a key regulator of glucose and lipid metabolism. Cell Metab. 2011, 14, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Pennica, D.; Shaw, K.J.; Swanson, T.A.; Moore, M.W.; Shelton, D.L.; Zioncheck, K.A.; Rosenthal, A.; Taga, T.; Paoni, N.F.; Wood, W.I. Cardiotrophin-1: Biological activities and binding to the leukemia inhibitory factor receptor/gp130 signalling complex. J. Biol. Chem. 1995, 270, 10915–10922. [Google Scholar] [CrossRef] [PubMed]
- Robledo, O.; Fourcin, M.; Chevalier, S.; Guillet, C.; Auguste, P.; Pouplard-Barthelaix, A.; Pennica, D.; Gascan, H. Signaling of the cardiotrophin-1 receptor. Evidence for a third receptor component. J. Biol. Chem. 1997, 272, 4855–4863. [Google Scholar] [CrossRef] [PubMed]
- Escoté, X.; Gómez-Zorita, S.; López-Yoldi, M.; Milton-Laskibar, I.; Fernández-Quintela, A.; Martínez, L.A.; Moreno-Aliaga, M.J.; Portillo, M.P. Role of omentin, vaspin, cardiotrophin-1, TWEAK and NOV/CCN3 in obesity and diabetes development. Int. J. Mol. Sci. 2017, 18, 1770. [Google Scholar] [CrossRef] [PubMed]
- Gkaliagkousi, E.; Gavriilaki, E.; Chatzopoulou, F.; Anyfanti, P.; Triantafyllou, A.; Petidis, K.; Zamboulis, C.; Douma, S. Association between cardiotrophin 1 levels and central blood pressure in untreated patients with essential hypertension. Am. J. Hypertens. 2014, 27, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Song, K.; Wang, S.; Huang, B.; Luciano, A.; Srivastava, R.; Mani, A. Plasma cardiotrophin-1 levels are associated with hypertensive heart disease: A meta-analysis. J. Clin. Hypertens. 2014, 16, 686–692. [Google Scholar] [CrossRef] [PubMed]
- López, B.; Castellano, J.M.; González, A.; Barba, J.; Díez, J. Association of increased plasma cardiotrophin-1 with inappropriate left ventricular mass in essential hypertension. Hypertension 2007, 50, 977–983. [Google Scholar] [CrossRef] [PubMed]
- López, B.; González, A.; Querejeta, R.; Barba, J.; Díez, J. Association of plasma cardiotrophin-1 with stage C heart failure in hypertensive patients: Potential diagnostic implications. J. Hypertens. 2009, 27, 418–424. [Google Scholar] [CrossRef] [PubMed]
- López, B.; González, A.; Querejeta, R.; Larman, M.; Rábago, G.; Díez, J. Association of cardiotrophin-1 with myocardial fibrosis in hypertensive patients with heart failure. Hypertension 2014, 63, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Zvonic, S.; Hogan, J.C.; Arbour-Reily, P.; Mynatt, R.L.; Stephens, J.M. Effects of cardiotrophin on adipocytes. J. Biol. Chem. 2004, 279, 47572–47579. [Google Scholar] [CrossRef] [PubMed]
- Asrih, M.; Mach, F.; Quercioli, A.; Dallegri, F.; Montecucco, F. Update on the pathophysiological activities of the cardiac molecule cardiotrophin-1 in obesity. Mediat. Inflamm. 2013, 2013, 1–8. [Google Scholar] [CrossRef] [PubMed]
- López-Yoldi, M.; Stanhope, K.L.; Garaulet, M.; Chen, X.G.; Marcos-Gómez, B.; Carrasco-Benso, M.P.; Santa Maria, E.M.; Escoté, X.; Lee, V.; Nunez, M.V.; et al. Role of cardiotrophin-1 in the regulation of metabolic circadian rhythms and adipose core clock genes in mice and characterization of 24-h circulating CT-1 profiles in normal-weight and overweight/obese subjects. FASEB J. 2017, 31, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- Anik Ilhan, G.; Kanlioglu, C.; Arslan, G.; Yildizhan, B.; Pekin, T. Cardiotrophin-1 as a new metabolic biomarker in women with PCOS. Gynecol. Endocrinol. 2018, 30, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Hung, H.C.; Lu, F.H.; Ou, H.Y.; Wu, H.T.; Wu, J.S.; Yang, Y.C.; Chang, C.J. Increased cardiotrophin-1 in subjects with impaired glucose tolerance and newly diagnosed diabetes. Int. J. Cardiol. 2013, 169, e33–e34. [Google Scholar] [CrossRef] [PubMed]
- García-Ortiz, L.; Martínez-Salgado, C. Plasma cardiotrophin-1 as a marker of hypertension and diabetes-induced target organ damage and cardiovascular risk. Medicine 2015, 94, e1218. [Google Scholar]
- Lutz, S.Z.; Franck, O.; Böhm, A.; Machann, J.; Schick, F.; Machicao, F.; Fritsche, A.; Häring, H.; Staiger, H. Common genetic variation in the human CTF1 locus, encoding cardiotrophin-1, determines insulin sensitivity. PLoS ONE 2014, 9, e100391. [Google Scholar] [CrossRef] [PubMed]
- Talwar, S.; Downie, P.F.; Squire, I.B.; Davies, J.E.; Barnett, D.B.; Ng, L.L. Plasma N-terminal pro BNP and cardiotrophin-1 are elevated in aortic stenosis. Eur. J. Heart Fail. 2001, 3, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Monserrat, L.; López, B.; González, A.; Hermida, M.; Fernández, X.; Ortiz, M.; Barriales-Villa, R.; Castro-Beiras, A.; Díez, J. Cardiotrophin-1 plasma levels are associated with the severity of hypertrophy in hypertrophic cardiomyopathy. Eur. Heart J. 2011, 32, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.Z.; Fu, X.T.; Liang, J.; Guo, Z.B. CT-1 induces angiogenesis by regulating the ADMA/DDAH pathway. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czechoslov. Repub. 2015, 159, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Fritzenwanger, M.; Meusel, K.; Foerster, M.; Kuethe, F.; Krack, A.; Figulla, H.R. Cardiotrophin-1 induces interleukin-6 synthesis in human umbilical vein endothelial cells. Cytokine 2006, 36, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Fritzenwanger, M.; Foerster, M.; Meusel, K.; Jung, C.; Figulla, H.R. Cardiotrophin-1 induces intercellular adhesion molecule-1 expression by nuclear factor κB activation in human umbilical vein endothelial cells. Chin. Med. J. 2008, 121, 2592–2598. [Google Scholar] [PubMed]
- Tokito, A.; Jougasaki, M.; Ichiki, T.; Hamasaki, S. Cardiotrophin-1 induces matrix metalloproteinase-1 in human aortic endothelial cells. PLoS ONE 2013, 8, e68801. [Google Scholar]
- Fritzenwanger, M.; Meusel, K.; Foerster, M.; Kuethe, F.; Krack, A.; Figulla, H.R. Cardiotrophin-1 induces interleukin-6 synthesis in human monocytes. Cytokine 2007, 38, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Fritzenwanger, M.; Jung, C.; Franz, M.; Foerster, M.; Figulla, H.R. Immunomodulatory effects of cardiotrophin-1 on in vitro cytokine production of monocytes & CD4 + T-lymphocytes. Indian J. Med. Res. 2012, 136, 471–476. [Google Scholar] [PubMed]
- Fritzenwanger, M.; Meusel, K.; Jung, C.; Franz, M.; Wang, Z.; Foerster, M.; Figulla, H.R. Cardiotrophin-1 induces tumor necrosis factor α synthesis in human peripheral blood mononuclear cells. Mediat. Inflamm. 2009, 2009, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.U.; San José, G.; Pejenaute, Á.; Landecho, M.F.; Díez, J.; Beloqui, Ó.; Fortuño, A.; Zalba, G. Association of phagocytic NADPH oxidase activity with hypertensive heart disease: A role for cardiotrophin-1? Hypertension 2014, 63, 468–474. [Google Scholar] [CrossRef] [PubMed]
- López-Andrés, N.; Calvier, L.; Labat, C.; Fay, R.; Díez, J.; Benetos, A.; Zannad, F.; Lacolley, P.; Rossignol, P. Absence of cardiotrophin 1 is associated with decreased age-dependent arterial stiffness and increased longevity in mice. Hypertension 2013, 61, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Demyanets, S.; Kaun, C.; Rychli, K.; Rega, G.; Pfaffenberger, S.; Afonyushkin, T.; Bochkov, V.N.; Maurer, G.; Huber, K.; Wojta, J. The inflammatory cytokine oncostatin M induces PAI-1 in human vascular smooth muscle cells in vitro via PI3-kinase and ERK1/2-dependent pathways. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H1962–H1968. [Google Scholar] [CrossRef] [PubMed]
- López-Andrés, N.; Rousseau, A.; Akhtar, R.; Calvier, L.; Iñigo, C.; Labat, C.; Zhao, X.; Cruickshank, K.; Díez, J.; Zannad, F.; et al. Cardiotrophin 1 is involved in cardiac, vascular, and renal fibrosis and dysfunction. Hypertension 2012, 60, 563–573. [Google Scholar] [CrossRef] [PubMed]
- López-Andrés, N.; Martin-Fernandez, B.; Rossignol, P.; Zannad, F.; Lahera, V.; Fortuño, M.A.; Cachofeiro, V.; Díez, J. A role for cardiotrophin-1 in myocardial remodeling induced by aldosterone. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H2372–H2382. [Google Scholar] [CrossRef] [PubMed]
- Talwar, S.; Squire, I.B.; O’brien, R.J.; Downie, P.F.; Davies, J.E.; Ng, L.L. Plasma cardiotrophin-1 following acute myocardial infarction: Relationship with left ventricular systolic dysfunction. Clin. Sci. 2002, 102, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Talwar, S.; Squire, I.B.; Downie, P.F.; O’Brien, R.J.; Davies, J.E.; Ng, L.L. Elevated circulating cardiotrophin-1 in heart failure: Relationship with parameters of left ventricular systolic dysfunction. Clin. Sci. 2000, 99, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Celik, A.; Sahin, S.; Koc, F.; Karayakali, M.; Sahin, M.; Benli, I.; Kadi, H.; Burucu, T.; Ceyhan, K.; Erkorkmaz, U. Cardiotrophin-1 plasma levels are increased in patients with diastolic heart failure. Med. Sci. Monit. 2012, 18, CR25–CR31. [Google Scholar] [CrossRef] [PubMed]
- Cottone, S.; Nardi, E.; Mulè, G.; Vadalà, A.; Lorito, M.C.; Riccobene, R.; Palermo, A.; Arsena, R.; Guarneri, M.; Cerasola, G. Association between biomarkers of inflammation and left ventricular hypertrophy in moderate chronic kidney disease. Clin. Nephrol. 2007, 67, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Hung, H.C.; Lu, F.H.; Ou, H.Y.; Wu, H.T.; Wu, J.S.; Yang, Y.C.; Chang, C.J. Cardiotrophin-1 is associated with increased risk of arterial stiffness. Biomark. Med. 2015, 9, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; Gluba-Brzózka, A.; Michalska-Kasiczak, M.; Misztal, M.; Rysz, J.; Banach, M. The multi-biomarker approach for heart failure in patients with hypertension. Int. J. Mol. Sci. 2015, 16, 10715–10733. [Google Scholar] [CrossRef] [PubMed]
- Tsutamoto, T.; Asai, S.; Tanaka, T.; Sakai, H.; Nishiyama, K.; Fujii, M.; Yamamoto, T.; Ohnishi, M.; Wada, A.; Saito, Y.; et al. Plasma level of cardiotrophin-1 as a prognostic predictor in patients with chronic heart failure. Eur. J. Heart Fail. 2007, 9, 1032–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heying, R.; Qing, M.; Schumacher, K.; Sokalska-Duhme, M.; Vazquez-Jimenez, J.F.; Seghaye, M.C. Myocardial cardiotrophin-1 is differentially induced in congenital cardiac defects depending on hypoxemia. Future Cardiol. 2014, 10, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Freed, D.H.; Moon, M.C.; Borowiec, A.M.; Jones, S.C.; Zahradka, P.; Dixon, I.M.C. Cardiotrophin-1: Expression in experimental myocardial infarction and potential role in post-MI wound healing. Mol. Cell. Biochem. 2003, 254, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Freed, D.H.; Cunnington, R.H.; Dangerfield, A.L.; Sutton, J.S.; Dixon, I.M.C. Emerging evidence for the role of cardiotrophin-1 in cardiac repair in the infarcted heart. Cardiovasc. Res. 2005, 65, 782–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul-Ghani, M.; Suen, C.; Jiang, B.; Deng, Y.; Weldrick, J.J.; Putinski, C.; Brunette, S.; Fernando, P.; Lee, T.T.; Flynn, P.; et al. Cardiotrophin 1 stimulates beneficial myogenic and vascular remodeling of the heart. Cell Res. 2017, 27, 1195–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, Y.; Ruan, X.; Laurikka, J.; Laine, S.; Tarkka, M.; Wei, M. The human heart releases cardiotrophin-1 after coronary artery bypass grafting with cardiopulmonary bypass. Scand. Cardiovasc. J. 2011, 45, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.Q.; Kelly, D.; Quinn, P.; Davies, J.E.; Ng, L.L. Cardiotrophin-1 predicts death or heart failure following acute myocardial infarction. J. Card. Fail. 2006, 12, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Marti, A.; Morell-Azanza, L.; Rendo-Urteaga, T.; García-Calzón, S.; Ojeda-Rodríguez, A.; Martín-Calvo, N.; Moreno-Aliaga, M.J.; Martínez, J.A.; Azcona-San Julián, M.C. Serum and gene expression levels of CT-1, IL-6, and TNF-α after a lifestyle intervention in obese children. Pediatr. Diabetes 2018, 19, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Hang, Y.; Qin, X.; Ren, T.; Cao, J. Baicalin reduces blood lipids and inflammation in patients with coronary artery disease and rheumatoid arthritis: A randomized, double-blind, placebo-controlled trial. Lipids Health Dis. 2018, 17, 146. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Peng, R.; Zhao, W.; Liu, Q.; Guo, Y.; Zhao, S.; Xu, D. Zhibital and low-dose atorvastatin reduce blood lipids and inflammation in patients with coronary artery disease. Medicine 2017, 96, 7. [Google Scholar]
- Wu, L.; Zhao, L.; Zheng, Q.; Shang, F.; Wang, X.; Wang, L.; Lang, B. Simvastatin attenuates hypertrophic responses induced by cardiotrophin-1 via JAK-STAT pathway in cultured cardiomyocytes. Mol. Cell. Biochem. 2006, 284, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Shen, Q.; Wu, Y. Simvastatin prevents cardiac hypertrophy in vitro and in vivo via JAK-STAT pathway. Life Sci. 2008, 82, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Scoles, D.R.; Xu, X.; Wang, H.; Tran, H.; Taylor-Harding, B.; Li, A.; Karlan, B.Y. Liver X receptor agonist inhibits proliferation of ovarian carcinoma cells stimulated by oxidized low density lipoprotein. Gynecol. Oncol. 2010, 116, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Yu, Q.; Na, R.; Liu, B. Etanercept protects rat cardiomyocytes against hypertrophy by regulating inflammatory cytokines secretion and cell apoptosis. Braz. J. Med. Biol. Res. 2017, 50, e5868. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Intracellular signal transduction of cardiotrophin-1 (CT-1) in cardiovascular responses. CT-1 activates the gp130 and LIFR complex, followed by the PI3K/Akt, ERK1/2, JAK/STAT, and NF-κB pathways (Adapted from [42]). The combined pathways induce cardiac protection, cardiovascular hypertrophy, atherosclerosis, arterial stiffness, and vascular inflammation (Adapted from [22]). EC = endothelial cell, ERK = extracellular signal-regulated kinase, JAK = Janus kinase, LIFR = leukemia inhibitory factor receptor, Mo = monocyte, MΦ = macrophage, NF-κB = nuclear factor-κB, PI3K = phosphatidylinositol 3-kinase, STAT = signal transducers and activators of transcription, VSMC = vascular smooth muscle cell.
Figure 1.
Intracellular signal transduction of cardiotrophin-1 (CT-1) in cardiovascular responses. CT-1 activates the gp130 and LIFR complex, followed by the PI3K/Akt, ERK1/2, JAK/STAT, and NF-κB pathways (Adapted from [42]). The combined pathways induce cardiac protection, cardiovascular hypertrophy, atherosclerosis, arterial stiffness, and vascular inflammation (Adapted from [22]). EC = endothelial cell, ERK = extracellular signal-regulated kinase, JAK = Janus kinase, LIFR = leukemia inhibitory factor receptor, Mo = monocyte, MΦ = macrophage, NF-κB = nuclear factor-κB, PI3K = phosphatidylinositol 3-kinase, STAT = signal transducers and activators of transcription, VSMC = vascular smooth muscle cell.

Figure 2.
Expression of CT-1 in atherosclerotic lesions. CT-1 is expressed at high levels (brown color) in endothelial cells (red arrows), macrophage-derived foam cells (blue arrows), and smooth muscle cells (black arrows) within atheromatous plaques in Apoe−/− mice (Chosen picture different from [15]).
Figure 2.
Expression of CT-1 in atherosclerotic lesions. CT-1 is expressed at high levels (brown color) in endothelial cells (red arrows), macrophage-derived foam cells (blue arrows), and smooth muscle cells (black arrows) within atheromatous plaques in Apoe−/− mice (Chosen picture different from [15]).
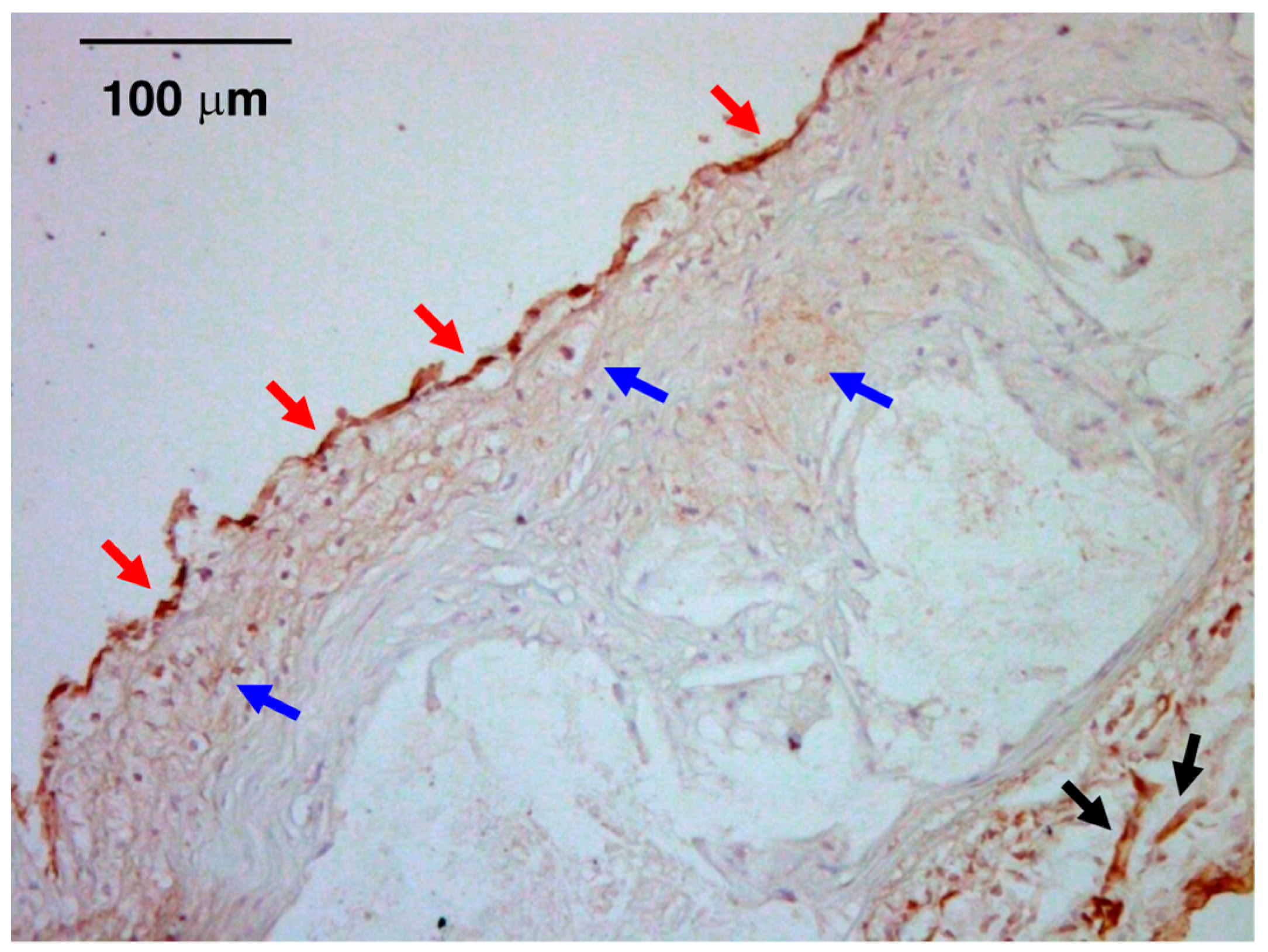
Figure 3.
Cellular and molecular mechanisms in atherosclerotic effects of CT-1. CT-1 stimulates endothelial and monocyte inflammation, macrophage foam-cell formation, and the migration and proliferation of VSMCs (Illustrated on the basis of [15,26,65,66,68,69,70]). ACAT-1 = acyl-coenzyme A: cholesterol acyltransferase-1, CE = cholesterol ester, ICAM = intercellular adhesion molecule-1, IL = interleukin, LDL = low-density lipoprotein, MCP-1 = monocyte chemoattractant protein-1, ROS = reactive oxygen species, TNF-α = tumor necrosis factor-α.
Figure 3.
Cellular and molecular mechanisms in atherosclerotic effects of CT-1. CT-1 stimulates endothelial and monocyte inflammation, macrophage foam-cell formation, and the migration and proliferation of VSMCs (Illustrated on the basis of [15,26,65,66,68,69,70]). ACAT-1 = acyl-coenzyme A: cholesterol acyltransferase-1, CE = cholesterol ester, ICAM = intercellular adhesion molecule-1, IL = interleukin, LDL = low-density lipoprotein, MCP-1 = monocyte chemoattractant protein-1, ROS = reactive oxygen species, TNF-α = tumor necrosis factor-α.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Plasma CT-1 concentrations (pM) in various diseases.
| Disease | Control | p Value | Reference | |
|---|---|---|---|---|
| Hypertension (untreated) | 606 ± 18 ↑ | 546 ± 12 | <0.01 | [28] |
| Hypertension (treated) | 618 ± 10 ↑ | 546 ± 12 | <0.01 | [28] |
| Hypertension | 37.9 ± 2.0 ↑ | 17.9 ± 2.7 | >0.05 | [53] |
| Hypertension + LVH | 75.3 ± 7.3 ↑ | 17.9 ± 2.7 | <0.001 | [53] |
| Hypertension + heart failure | 116.6 ± 13.2 ↑ | 17.9 ± 2.7 | <0.001 | [53] |
| Metabolic syndrome | 5644 ± 356 ↑ | 4711 ± 178 | <0.05 | [23] |
| Obesity | 5467 ± 400 ↑ | 4889 ± 222 | <0.05 | [23] |
| Diabetes | 46.7 ± 7.7 ↑ | 21.1 ± 3.7 | <0.005 | [59] |
| Impaired glucose tolerance | 35.5 ± 5.4 ↑ | 21.1 ± 3.7 | <0.05 | [59] |
| Diabetes | 26.1 (10.9–86.0) ↑ | 14.2 (8.8–29.8) | <0.05 | [60] |
| Stable angina pectoris | 73.2 (41.5–102.1) ↑ | 27.0 (6.9–54.1) | <0.01 | [16] |
| Unstable angina pectoris | 142.5 (42.2–527.4) ↑ | 27.0 (6.9–54.1) | <0.01 | [16] |
| Aortic Stenosis | 57.3 (33.0–86.3) ↑ | 28.3 (6.9–48.3) | <0.0005 | [62] |
| Hypertrophic cardiomyopathy | 136.3 ± 72.0 ↑ | 17.9 ± 12.0 | <0.001 | [63] |
Data are expressed as mean ± standard error/deviation or median and range. Arrows show changes in CT-1 concentrations compared with controls. LVH = left ventricular hypertrophy.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Watanabe, T.; Konii, H.; Sato, K. Emerging Roles of Cardiotrophin-1 in the Pathogenesis and Biomarker of Atherosclerosis. J 2018, 1, 94-105. https://doi.org/10.3390/j1010010
AMA Style
Watanabe T, Konii H, Sato K. Emerging Roles of Cardiotrophin-1 in the Pathogenesis and Biomarker of Atherosclerosis. J. 2018; 1(1):94-105. https://doi.org/10.3390/j1010010
Chicago/Turabian StyleWatanabe, Takuya, Hanae Konii, and Kengo Sato. 2018. "Emerging Roles of Cardiotrophin-1 in the Pathogenesis and Biomarker of Atherosclerosis" J 1, no. 1: 94-105. https://doi.org/10.3390/j1010010