Enhancing Mentorship in Psychiatry and Health Sciences: A Study Investigating Needs and Preferences in the Development of a Mentoring Program

Abstract
:1. Introduction
2. Methods
2.1. Participants and Surveys
2.2. Quantitative Analysis
2.3. Qualitative Analysis
3. Results
3.1. Participant Demographics
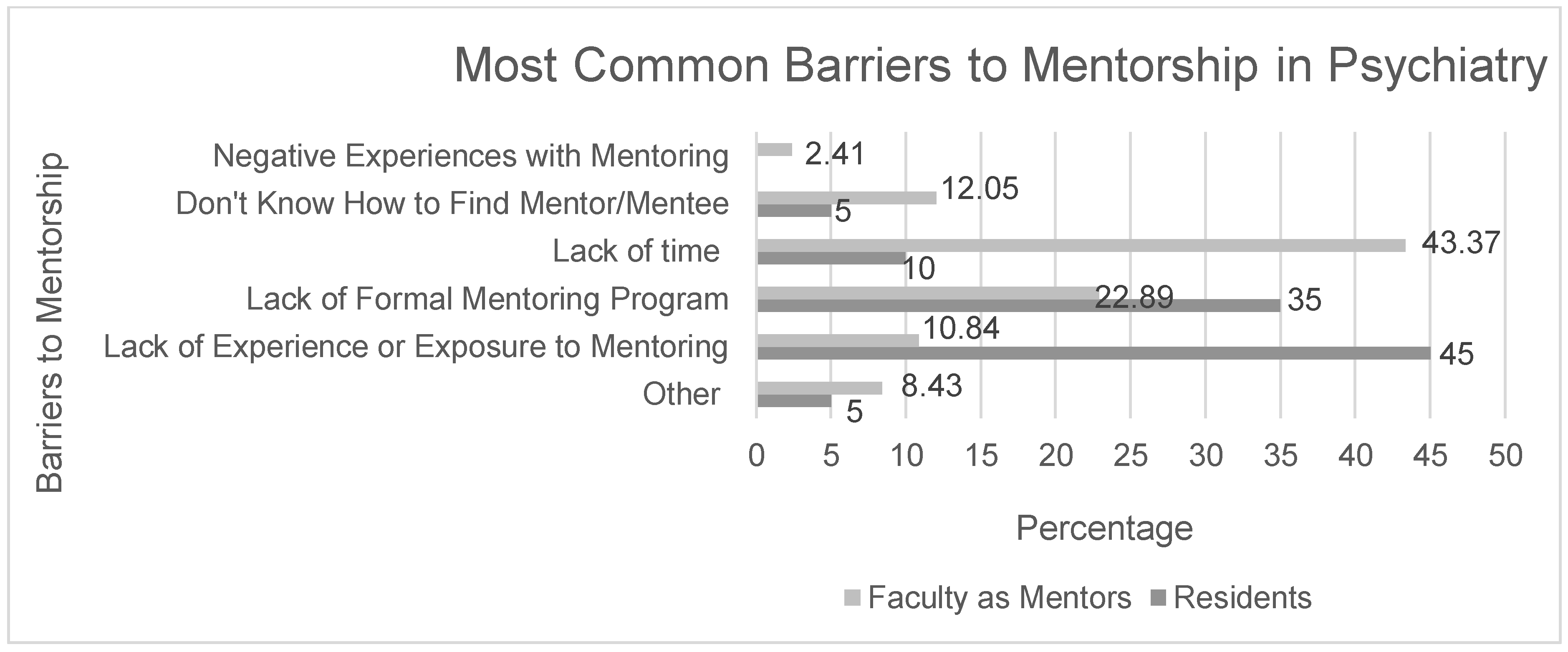
3.2. Barriers to Mentees Seeking Mentorship
3.3. Preferences in Mentorship
3.4. Qualitative Data Results
3.4.1. Fostering a Culture That Encourages Mentorship
“I think creating a culture where mentorship is encouraged is already a big step”.
“I did not have [a mentor] and think it has negatively affected my entire academic career. I know now I should have done a lot of things differently”.
3.4.2. Seeking Mentors Not Directly Involved in Supervision
“Matching residents…with mentors who will have no implications on their performance and future career standing so as to minimize power struggle”.
3.4.3. Mentor-Mentee Pairings
“I think that a sort of ‘catalogue’ of interested mentors who describe the knowledge, skills and opportunities that they bring would be helpful to allow individuals who are seeking mentorship to find someone of interest.”
3.4.4. Establishing Structure in Mentoring Relationships
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A. Comments from Faculty Members and Residents across the Two Surveys *
Resident Survey
ID Response
- 17
- Not in particular, but I think it’s a worthwhile idea.
- 15
- Needs to be flexible—don’t just match people and expect it to work. Should review CAIR’s work on mentorship—they did a session at ICRE—[EMAIL REMOVED FOR PRIVACY REASONS] is contact.
- 16
- Not particularly. I had group mentoring at the undergraduate level previously, however if the group becomes too big, it becomes very tough to get everyone together given busy schedules. So I would suggest if a group format is used, that groups are kept small.
- 18
- McMaster medical school implements a mentorship program throughout the training period, and may be a helpful model to consult.
- 23
- I would be unlikely to participate if the program assigns pairings. I have had previous experiences with this method that didn’t work out, and there is good research evidence to support that assigned pairings only works well when the method of pairing is highly sophisticated. Personal selection is far more likely to be successful, and is indeed my preference.
- 24
- My personal experience has been that mentorship develops the best when it is a relationship that is developed from a natural transition within a working environment/relationship. My experiences of forced or assigned mentorship have been much less helpful.
- 30
- Clearly identify role of mentor and limits therein.
- 31
- No particular suggestions, but this is a wonderful project and I think could become a tremendous asset to the program! I would advocate for also encouraging faculty at the Waterloo Regional Campus to participate as potential mentors; however, keeping the opportunities open for residents to choose a mentor at either site (depending on interests and goals) would be appreciated!
- 38
- Please do not make it mandatory–allow people to find their own mentors if they prefer.
- 46
- I think creating a culture where mentorship is encouraged is already a big step. For myself, the mentor/mentee relationship developed naturally with a supervisor I had done a rotation with. Although my clinical interests do not match those of my mentor, she provided me with guidance, support and took an interest in me as a whole person, and this is what really made the difference between seeing her as simply a ‘supervisor’ and developing more of a mentoring relationship. She helped me to identify my own strengths (which I would not have identified as being “strengths” had she not provided me with that feedback) and built a lot of my confidence in that I could pursue avenues in line with my strengths and interests. She was also very open and candid with me about her own career, work/life balance, etc., and this made me feel comfortable enough to open up to her. I think there has to be a comfort level between mentor/mentee where you feel safe opening up and asking questions without the fear of being judged or criticized, or jeopardizing future career opportunities. To a certain extent, in my case at least, a part of the connection had to do with personality and similar values, and feeling like this person understands me and my goals. Maybe for others that would be less important however–but I do think there is something intangible and relationship-based that makes a mentor/mentee relationship work or not. I also do think that the mentor should encourage connecting with other mentors for different areas–so for example because my clinical interests are not similar to what my mentor is doing, she gave me ideas of other mentors that I could connect with whose clinical interests were in keeping with mine, without making me feel like I’m disappointing her by not becoming her protégé.
- 47
- I do think residents should be mentored from junior stages PGY1-2 throughout the 5 years.
ID Response
- 108
- I would work selectively, identify prospective mentors based on their track record and seek to match them with a small group of learners (students to faculty) who are likely to benefit from the process. I would start small (pilot) and move towards scale. The best results in my view come from ‘natural pairings’ which can be facilitated by providing opportunities for mentee/mentors to meet... Good luck.
- 110
- (1) All new faculty should be assigned a mentor immediately upon being appointed. This may be informal for new senior people, but definitely formalized for new junior faculty. (2) There should be a way of vetting mentors. Not all people who want to be mentors would necessarily be good mentors. The Chair may want to have a small group of senior people make this decision.
- 130
- —assuming there’s enough interest from the residents, there should be guidelines given to the mentors outlining the goals/responsibilities of a mentor—there should be some process to try and match mentees and mentors so that there are common interests.
- 143
- McMaster already has a mentorship program–would be useful to review this course and see what may be transferable to Psychiatry mentorship program.
- 168
- Matching residents, including senior residents and junior faculty / staff with mentors who will have no implications on their performance and future career standing so as to minimize power struggle, to encourage openness in communication and to enhance effectiveness in fulfilling purposes of mentorship.
- 177
- I like the idea of a mentorship training program which would provide a pool of potential mentors. I recognize that I have the potential to provide mentorship but could also benefit from receiving it. A list mentors who have completed training would be a good starting place to developing a matching system. I believe that goodness of fit is of relatively high importance in forming a useful mentoring relationship.
- 179
- yes a workshop with clear objectives.
- 180
- I think that a sort of ‘catalogue’ of interested mentors who describe the knowledge, skills and opportunities that they bring would be helpful to allow individuals who are seeking mentorship to find someone of interest. I think that you should consider building relationships with folks outside of the department because having a mentor who works outside of your immediate work/learning environment and who brings a different perspective is so beneficial (I personally have an internal and external mentor).
- 181
- No
- 191
- Informal mentorships occur spontaneously and depend on each party bringing interest and enthusiasm to the role. A structured program should not set limits or too much structure on the process. Each dyad must come to their own understanding of what should take place, but obviously there have to be some general goals and processes.
- 195
- When there is so much that needs to be done to move the educational curriculum (e.g., CBE) forward, not sure about the timing of a mentorship program (unless they are tied together to some degree!). Seems hard enough to get people to do anything more within their work!
- 201
- Faculty interests and mentorship are necessarily idiosyncratic, but may be optimized if structured toward a common endpoint (e.g., submitting a grant). This has worked well in my experience.
- 203
- I am just a little worried that people don’t have the time, therefore, what gets started may not be possible to finish. I would recommend very clear and operationalized definitions of mentorship, so that expectations are clear to all. Solution-focused therapy and motivational interviewing techniques would be very helpful in keeping the mentorship short, goal-oriented, and focused, with clear guidelines as to how to evaluate its effectiveness. In my opinion, mentors should be there to help empower the mentee to find solutions and make informed decisions; not to make the decisions or solve the problems for the mentee.
- 213
- There needs to be more focus on mentoring of GPTs and the different trajectories that their careers can take. In my 20 years in the Department, I think I have only had 3 conversations about promotion, etc.
- 222
- Have clear expectations for both the mentor and mentee regarding what they can expect. I don’t necessarily mean a very formalized program, but clear expectations so all are on the same page. Identify the areas that different groups of mentees would like mentorship on–and link them with mentors who can support them in these areas. Not all mentees will have the same needs, so it would be helpful to target the response to these needs.
- 225
- I think it is important to recognize the importance of the networks of informal, content or problem specific mentors available here.
- 226
- being a community psychiatrist in [REMOVED TO PROTECT IDENTITY], and part time faculty, and wanting to have a research focus, I would love the opportunity to have such mentor, so would strongly support your idea of developing such a program.
- 231
- Just a thought. I am a social worker and initially did not response to the survey because I wasn’t sure that it was meant for me. I may have different needs and different things that I can offer. It is a great opportunity for drawing on the skills of allied health Faculty.
- 234
- I think you should just start. Every new faculty member should have a mentor to work with in the first year of their appointment. I did not have this and think it has negatively affected my entire academic career. I know now I should have done a lot of things differently.
- 236
- Not sure about idea of assigned mentors and mentees–there is a chemistry to this relationship that has to work and can’t be forced. As a resident though I think a mentor would have been incredibly helpful, particularly in years 4 and 5.
- 242
- See what else is available as models at McMaster and elsewhere.
- 250
- encourage development of clinician–scientist program encourage learning of mechanisms involves in disease process.
References
- Shollen, S.L.; Bland, C.J.; Games, A.I.; Fitzgerald, D.A.; Taylor, A.L. Relating mentor type and mentoring behaviors to academic medicine faculty satisfaction and productivity at one medical school. Acad. Med. 2014, 89, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Posporelis, S.; Sawa, A.; Smith, G.S.; Stitzer, M.L.; Lyketsos, C.G.; Chisolm, M.S. Promoting careers in academic research to psychiatry residents. Acad. Psychiatry 2014, 38, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, D.T.; Varkey, P.; Cook, D.A. Mentoring programs for physicians in academic medicine: A systematic review. Acad. Med. 2013, 88, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Buddeberg-Fischer, B.; Herta, K.D. Formal mentoring programmes for medical students and doctors—A review of the Medline literature. Med. Teach. 2006, 28, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Straus, E.; Chatur, F.; Taylor, M. Issues in the mentor–mentee relationship in academic medicine: A qualitative study. Acad. Med. 2009, 84, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Sambunjak, D.; Straus, S.E.; Marušić, A. Mentoring in academic medicine: A systematic review. JAMA 2006, 296, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Blood, E.A.; Ullrich, N.J.; Hirshfeld-Becker, D.R.; Seely, E.W.; Connelly, M.T.; Warfield, C.A.; Emans, S.J. Academic women faculty: Are they finding the mentoring they need? J. Womens Health 2012, 21, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Bickel, J. Women in academic psychiatry. Acad. Psychiatry 2004, 28, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Heiligers, P.J.; Hingstman, L. Career preferences and the work–family balance in medicine: Gender differences among medical specialists. Soc. Sci. Med. 2000, 50, 1235–1246. [Google Scholar] [CrossRef]
- Limacher, M.; Zaher, C.; Walsh, M.; Wolf, W.; Douglas, P.; Schwartz, J.; Bodycombe, D. The ACC professional life survey: Career decisions of women and men in cardiology: A report of the Committee on Women in Cardiology. J. Am. Coll. Cardiol. 1998, 32, 827–835. [Google Scholar] [CrossRef]
- The Association of Faculties of Medicine of Canada. Canadian Medical Education Statistics 2011. Available online: http://www.afmc.ca/publications-statistics-e.php (accessed on 21 March 2018).
- Perna, L.W. Sex differences in faculty tenure and promotion: The contribution of family ties. Res. High Educ. 2005, 46, 277–307. [Google Scholar] [CrossRef]
- Turner, J.; Tippett, V.; Raphael, B. Women in medicine-socialization, stereotypes and self perceptions. Aust. Psychiatry 1994, 28, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Pololi, L.; Knight, S. Mentoring faculty in academic medicine. J. Gen. Intern. Med. 2005, 20, 866–870. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A.; Taylor, J.C.; Stoller, J.K. The influence of mentorship and role modeling on developing physician-leaders: Views of aspiring and established physician-leaders. J. Gen. Intern. Med. 2009, 24, 1130–1134. [Google Scholar] [CrossRef] [PubMed]
- Soklaridis, S.; López, J.; Charach, N.; Broad, K.; Teshima, J.; Fefergrad, M. Developing a mentorship program for psychiatry residents. Acad. Psychiatry 2015, 39, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Kahlke, R. Generic qualitative approaches: Pitfalls and benefits of methodological mixology. Int. J. Qual. Method 2014, 13, 37–52. [Google Scholar] [CrossRef]
- Lau, C.; Ford, J.; Van Lieshout, R.J.; Saperson, K.; McConnell, M.; McCabe, R.M. Developing Mentoring Competency: Does a One Session Training Workshop Have Impact? Acad. Psychiatry 2016, 40, 429–433. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Number of Respondents (% of Sample) | ||
|---|---|---|---|
| Resident Survey | Gender | Male | 8 (27) |
| Female | 22 (73) | ||
| Years of Training | First | 5 (17) | |
| Second | 6 (20) | ||
| Third | 8 (27) | ||
| Fourth | 7 (23) | ||
| Fifth * | 4 (13) | ||
| Faculty Survey | Gender | Male | 36 (39) |
| Female | 57 (61) | ||
| Current Position | Full-Time Faculty | 31 (33) | |
| Part-Time Faculty | 62 (67) | ||
| Years in Current Profession | Less than 5 | 18 (19) | |
| 6–10 | 14 (15) | ||
| 11–15 | 14 (15) | ||
| 16–20 | 16 (17) | ||
| More than 20 | 31 (33) | ||
| Years in Department | Less than 5 | 33 (35) | |
| 6–10 | 19 (20) | ||
| 11–15 | 13 (14) | ||
| 16–20 | 12 (13) | ||
| More than 20 | 16 (17) | ||
| Professional Discipline | Psychiatry | 44 (47) | |
| Psychology | 26 (28) | ||
| Social Work | 10 (11) | ||
| Other ** | 13 (14) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, C.; Ford, J.; Van Lieshout, R.J.; Saperson, K.; McConnell, M.; McCabe, R. Enhancing Mentorship in Psychiatry and Health Sciences: A Study Investigating Needs and Preferences in the Development of a Mentoring Program. J 2018, 1, 8-18. https://doi.org/10.3390/j1010003
Lau C, Ford J, Van Lieshout RJ, Saperson K, McConnell M, McCabe R. Enhancing Mentorship in Psychiatry and Health Sciences: A Study Investigating Needs and Preferences in the Development of a Mentoring Program. J. 2018; 1(1):8-18. https://doi.org/10.3390/j1010003
Chicago/Turabian StyleLau, Chloe, Jennifer Ford, Ryan J. Van Lieshout, Karen Saperson, Meghan McConnell, and Randi McCabe. 2018. "Enhancing Mentorship in Psychiatry and Health Sciences: A Study Investigating Needs and Preferences in the Development of a Mentoring Program" J 1, no. 1: 8-18. https://doi.org/10.3390/j1010003