Endoscopic Botulinum Toxin for Gastroparesis: Results of a Retrospective Series

 ,
,
Abstract
:1. Introduction
2. Results
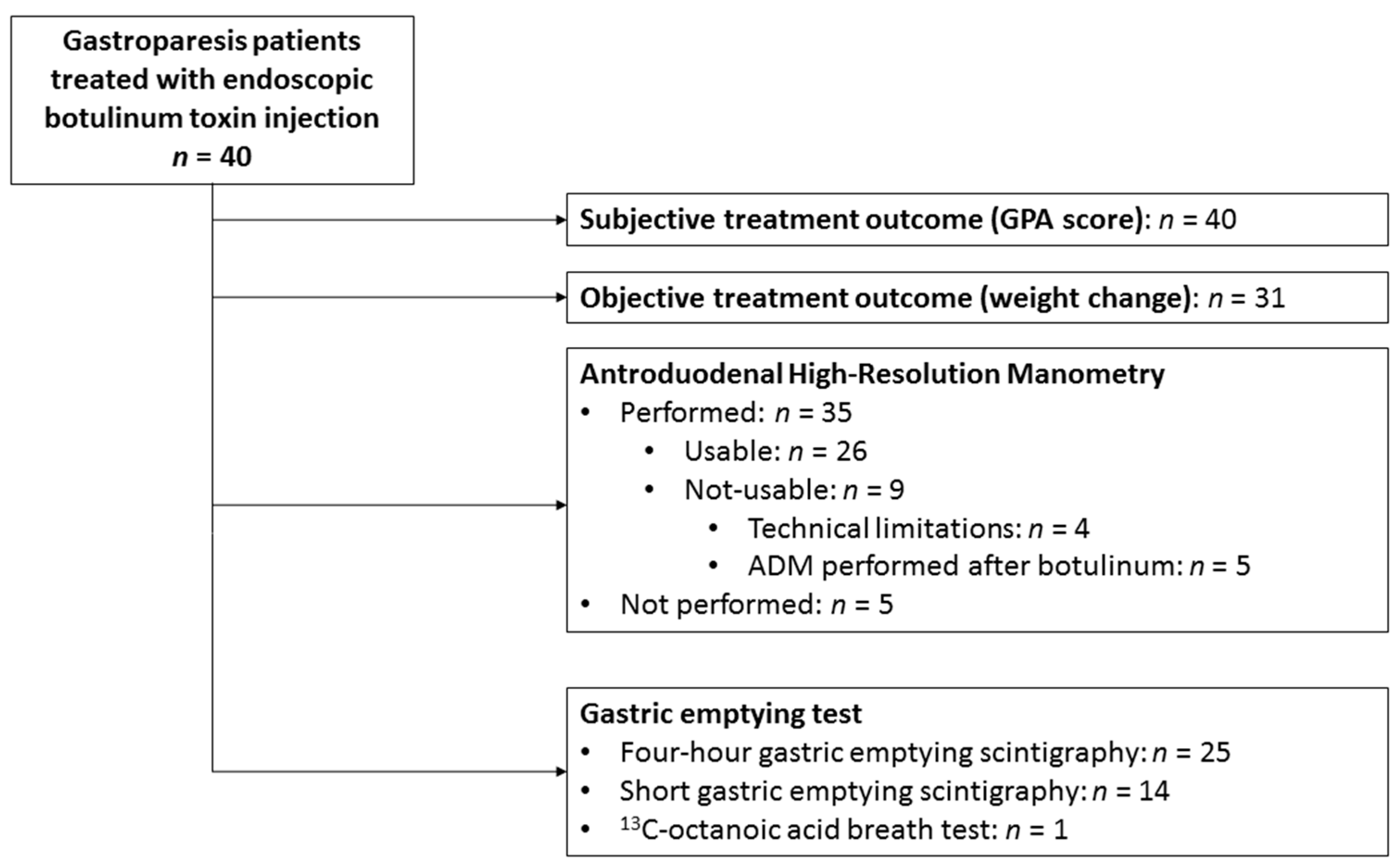
2.1. Patient Characteristics
2.2. Subjective Treatment Outcome
2.3. Objective Treatment Outcome
2.4. Predictors
2.5. Follow-Up and Additional Treatment Procedures
3. Discussion
4. Materials and Methods
4.1. Design, Setting, and Participants
4.2. Scintigraphy
4.3. High-Resolution Antroduodenal Manometry
4.4. Endoscopic Pyloric Botulinum Toxin Injection
4.5. Outcomes
4.6. Data Analysis
4.6.1. Scintigraphy
4.6.2. High-Resolution Antroduodenal Manometry
4.7. Statistical Methods
Author Contributions
Funding
Conflicts of Interest
References
- Shin, A.S.; Camilleri, M. Diagnostic assessment of diabetic gastroparesis. Diabetes 2013, 62, 2667–2673. [Google Scholar] [CrossRef] [PubMed]
- Abell, T.L.; Bernstein, R.K.; Cutts, T.; Farrugia, G.; Forster, J.; Hasler, W.L.; McCallum, R.W.; Olden, K.W.; Parkman, H.P.; Parrish, C.R.; et al. Treatment of gastroparesis: A multidisciplinary clinical review. Neurogastroenterol. Motil. 2006, 18, 263–283. [Google Scholar] [CrossRef]
- Ali, T.; Hasan, M.; Hamadani, M.; Harty, R.F. Gastroparesis. South. Med. J. 2007, 100, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Parkman, H.P.; Hasler, W.L.; Fisher, R.S.; American Gastroenterological Association. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology 2004, 127, 1592–1622. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Brown, M.L.; Malagelada, J.R. Relationship between impaired gastric emptying and abnormal gastrointestinal motility. Gastroenterology 1986, 91, 94–99. [Google Scholar] [CrossRef]
- Mearin, F.; Camilleri, M.; Malagelada, J.R. Pyloric dysfunction in diabetics with recurrent nausea and vomiting. Gastroenterology 1986, 90, 1919–1925. [Google Scholar] [CrossRef]
- Gourcerol, G.; Tissier, F.; Melchior, C.; Touchais, J.Y.; Huet, E.; Prevost, G.; Leroi, A.M.; Ducrotte, P. Impaired fasting pyloric compliance in gastroparesis and the therapeutic response to pyloric dilatation. Aliment. Pharmacol. Ther. 2015, 41, 360–367. [Google Scholar] [CrossRef]
- Langworthy, J.; Parkman, H.P.; Schey, R. Emerging strategies for the treatment of gastroparesis. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Vanheel, H.; Vicario, M.; Vanuytsel, T.; Van Oudenhove, L.; Martinez, C.; Keita, A.V.; Pardon, N.; Santos, J.; Soderholm, J.D.; Tack, J.; et al. Impaired duodenal mucosal integrity and low-grade inflammation in functional dyspepsia. Gut 2014, 63, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Olausson, E.A.; Storsrud, S.; Grundin, H.; Isaksson, M.; Attvall, S.; Simren, M. A small particle size diet reduces upper gastrointestinal symptoms in patients with diabetic gastroparesis: A randomized controlled trial. Am. J. Gastroenterol. 2014, 109, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Parkman, H.P.; Shafi, M.A.; Abell, T.L.; Gerson, L. Clinical guideline: Management of gastroparesis. Am. J. Gastroenterol. 2013, 108, 18–38. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, N.K.; Clarke, J.O. Pyloric Therapies for Gastroparesis. Curr. Treat. Options Gastroenterol. 2017, 15, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Weiser, K.; Kennedy, A. Botulinum toxin and gastrointestinal tract disorders: Panacea, placebo, or pathway to the future? Gastroenterol. Hepatol. 2008, 4, 283–295. [Google Scholar]
- James, A.N.; Ryan, J.P.; Parkman, H.P. Inhibitory effects of botulinum toxin on pyloric and antral smooth muscle. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 285, G291–G297. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Crowell, M.D.; Schettler-Duncan, A.; Mathis, C.; Pasricha, P.J. The treatment of diabetic gastroparesis with botulinum toxin injection of the pylorus. Diabetes Care 2004, 27, 2341–2347. [Google Scholar] [CrossRef] [PubMed]
- Friedenberg, F.K.; Palit, A.; Parkman, H.P.; Hanlon, A.; Nelson, D.B. Botulinum toxin A for the treatment of delayed gastric emptying. Am. J. Gastroenterol. 2008, 103, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Arts, J.; Holvoet, L.; Caenepeel, P.; Bisschops, R.; Sifrim, D.; Verbeke, K.; Janssens, J.; Tack, J. Clinical trial: A randomized-controlled crossover study of intrapyloric injection of botulinum toxin in gastroparesis. Aliment. Pharmacol. Ther. 2007, 26, 1251–1258. [Google Scholar] [CrossRef]
- Coleski, R.; Anderson, M.A.; Hasler, W.L. Factors associated with symptom response to pyloric injection of botulinum toxin in a large series of gastroparesis patients. Dig. Dis. Sci. 2009, 54, 2634–2642. [Google Scholar] [CrossRef]
- Bromer, M.Q.; Friedenberg, F.; Miller, L.S.; Fisher, R.S.; Swartz, K.; Parkman, H.P. Endoscopic pyloric injection of botulinum toxin A for the treatment of refractory gastroparesis. Gastrointest. Endosc. 2005, 61, 833–839. [Google Scholar] [CrossRef]
- de Caestecker, J.S.; Ewing, D.J.; Tothill, P.; Clarke, B.F.; Heading, R.C. Evaluation of oral cisapride and metoclopramide in diabetic autonomic neuropathy: An eight-week double-blind crossover study. Aliment. Pharmacol. Ther. 1989, 3, 69–81. [Google Scholar] [CrossRef]
- Horowitz, M.; Harding, P.E.; Maddox, A.F.; Wishart, J.M.; Akkermans, L.M.; Chatterton, B.E.; Shearman, D.J. Gastric and oesophageal emptying in patients with type 2 (non-insulin-dependent) diabetes mellitus. Diabetologia 1989, 32, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Keshavarzian, A.; Iber, F.L.; Vaeth, J. Gastric emptying in patients with insulin-requiring diabetes mellitus. Am. J. Gastroenterol. 1987, 82, 29–35. [Google Scholar]
- Loo, F.D.; Palmer, D.W.; Soergel, K.H.; Kalbfleisch, J.H.; Wood, C.M. Gastric emptying in patients with diabetes mellitus. Gastroenterology 1984, 86, 485–494. [Google Scholar]
- Janssen, P.; Harris, M.S.; Jones, M.; Masaoka, T.; Farre, R.; Tornblom, H.; Van Oudenhove, L.; Simren, M.; Tack, J. The relation between symptom improvement and gastric emptying in the treatment of diabetic and idiopathic gastroparesis. Am. J. Gastroenterol. 2013, 108, 1382–1391. [Google Scholar] [CrossRef] [PubMed]
- Thazhath, S.S.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Diabetic gastroparesis: Recent insights into pathophysiology and implications for management. Expert Rev. Gastroenterol. Hepatol. 2013, 7, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Thumshirn, M.; Bruninga, K.; Camilleri, M. Simplifying the evaluation of postprandial antral motor function in patients with suspected gastroparesis. Am. J. Gastroenterol. 1997, 92, 1496–1500. [Google Scholar] [PubMed]
- Camilleri, M.; Hasler, W.L.; Parkman, H.P.; Quigley, E.M.; Soffer, E. Measurement of gastrointestinal motility in the GI laboratory. Gastroenterology 1998, 115, 747–762. [Google Scholar] [CrossRef]
- Parthasarathy, G.; Ravi, K.; Camilleri, M.; Andrews, C.; Szarka, L.A.; Low, P.A.; Zinsmeister, A.R.; Bharucha, A.E. Effect of neostigmine on gastroduodenal motility in patients with suspected gastrointestinal motility disorders. Neurogastroenterol. Motil. 2015, 27, 1736–1746. [Google Scholar] [CrossRef] [Green Version]
- Lacy, B.E.; Zayat, E.N.; Crowell, M.D.; Schuster, M.M. Botulinum toxin for the treatment of gastroparesis: A preliminary report. Am. J. Gastroenterol. 2002, 97, 1548–1552. [Google Scholar] [CrossRef]
- Snape, W.J.; Lin, M.S.; Agarwal, N.; Shaw, R.E. Evaluation of the pylorus with concurrent intraluminal pressure and EndoFLIP in patients with nausea and vomiting. Neurogastroenterol. Motil. 2016, 28, 758–764. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.; Rao, S.S. Attenuation of isolated pyloric pressure waves in gastroparesis in response to botulinum toxin injection: A case report. Gastrointest. Endosc. 2002, 56, 770–772. [Google Scholar] [CrossRef]
- Deane, A.M.; Besanko, L.K.; Burgstad, C.M.; Chapman, M.J.; Horowitz, M.; Fraser, R.J. Modulation of individual components of gastric motor response to duodenal glucose. World J. Gastroenterol. 2013, 19, 5863–5869. [Google Scholar] [CrossRef] [PubMed]
- Fraser, R.J.; Horowitz, M.; Maddox, A.F.; Dent, J. Postprandial antropyloroduodenal motility and gastric emptying in gastroparesis--effects of cisapride. Gut 1994, 35, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Heddle, R.; Dent, J.; Toouli, J.; Read, N.W. Topography and measurement of pyloric pressure waves and tone in humans. Am. J. Physiol. 1988, 255, G490–G497. [Google Scholar] [CrossRef] [PubMed]
- Desipio, J.; Friedenberg, F.K.; Korimilli, A.; Richter, J.E.; Parkman, H.P.; Fisher, R.S. High-resolution solid-state manometry of the antropyloroduodenal region. Neurogastroenterol. Motil. 2007, 19, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Herbella, F.A.; Aprile, L.R.; Patti, M.G. High-resolution manometry for the evaluation of gastric motility. Updates Surg. 2014, 66, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Malik, Z.; Sankineni, A.; Parkman, H.P. Assessing pyloric sphincter pathophysiology using EndoFLIP in patients with gastroparesis. Neurogastroenterol. Motil. 2015, 27, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Wellington, J.; Scott, B.; Kundu, S.; Stuart, P.; Koch, K.L. Effect of endoscopic pyloric therapies for patients with nausea and vomiting and functional obstructive gastroparesis. Auton. Neurosci. 2017, 202, 56–61. [Google Scholar] [CrossRef]
- Jacques, J.; Pagnon, L.; Hure, F.; Legros, R.; Crepin, S.; Fauchais, A.L.; Palat, S.; Ducrotte, P.; Marin, B.; Fontaine, S.; et al. Peroral endoscopic pyloromyotomy is efficacious and safe for refractory gastroparesis: Prospective trial with assessment of pyloric function. Endoscopy 2018. [Google Scholar] [CrossRef]
- Abell, T.L.; Camilleri, M.; Donohoe, K.; Hasler, W.L.; Lin, H.C.; Maurer, A.H.; McCallum, R.W.; Nowak, T.; Nusynowitz, M.L.; Parkman, H.P.; et al. Consensus recommendations for gastric emptying scintigraphy: A joint report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. Am. J. Gastroenterol. 2008, 103, 753–763. [Google Scholar] [CrossRef]
- Farrell, M.B.; Costello, M.; McKee, J.D.; Gordon, L.L.; Fig, L.M. Compliance with Gastric-Emptying Scintigraphy Guidelines: An Analysis of the Intersocietal Accreditation Commission Database. J. Nucl. Med. Technol. 2017, 45, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Parkman, H.P.; Fass, R.; Foxx-Orenstein, A.E. Treatment of patients with diabetic gastroparesis. Gastroenterol. Hepatol. 2010, 6, 1–16. [Google Scholar]
- Hasler, W.L. Gastroparesis--current concepts and considerations. Medscape J. Med. 2008, 10, 16. [Google Scholar]
- Szarka, L.A.; Camilleri, M. Methods for measurement of gastric motility. Am. J. Physiol. Gastrointest. Liver Physiol. 2009, 296, G461–G475. [Google Scholar] [CrossRef] [PubMed]
- Scaglione, F. Conversion Ratio between Botox®, Dysport®, and Xeomin® in Clinical Practice. Toxins 2016, 8, 65. [Google Scholar] [CrossRef] [PubMed]
- Hanauer, S.; Schwartz, J.; Robinson, M.; Roufail, W.; Arora, S.; Cello, J.; Safdi, M. Mesalamine capsules for treatment of active ulcerative colitis: Results of a controlled trial. Pentasa Study Group. Am. J. Gastroenterol. 1993, 88, 1188–1197. [Google Scholar] [PubMed]
- Strijbos, D.; Keszthelyi, D.; Masclee, A.A.M.; Gilissen, L.P.L. Percutaneous endoscopic colostomy for adults with chronic constipation: Retrospective case series of 12 patients. Neurogastroenterol. Motil. 2018, 30, e13270. [Google Scholar] [CrossRef] [PubMed]
- Bortolotti, M.; Annese, V.; Coccia, G. Twenty-four hour ambulatory antroduodenal manometry in normal subjects (co-operative study). Neurogastroenterol. Motil. 2000, 12, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Quigley, E.M.; Donovan, J.P.; Lane, M.J.; Gallagher, T.F. Antroduodenal manometry. Usefulness and limitations as an outpatient study. Dig. Dis. Sci. 1992, 37, 20–28. [Google Scholar] [CrossRef]
- Verhagen, M.A.; Samsom, M.; Smout, A.J. Gastric myoelectrical and antroduodenal motor activity in patients with achalasia. Neurogastroenterol. Motil. 1998, 10, 211–218. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Median (IQR ‡) |
|---|---|
| Demographic parameters | |
| Age (years) | 49 (36–56) |
| Length (cm) | 168 (164–178) |
| Weight before botulinum toxin (kg) | 66.3 (57–80) |
| BMI before botulinum toxin (kg/m2) | 23.7 (20.2–26.6) |
| Etiology | N (%) |
| Idiopathic | 17 (42.5%) |
| Diabetic | 13 (32.5%) |
| Post-surgical | 10 (25%) |
| HbA1C * (%) | 8.4 (7.5–10.9) |
| Gastric emptying parameters | |
| T50 solid (min; normal 64–103 min) | 146 (127–188) |
| Stasis 60 min (%; normal 53–79%) | 89 (82–91) |
| Stasis 120 min (%; normal 16–37%) | 61 (53–76) |
| Stasis 240 min (%; normal 0–4%) | 17 (2–31) |
| Antroduodenal manometric parameters | |
| Antral frequency (contractions/min) | 1.27 (1.02–1.75) |
| Antral amplitude (mmHg) | 58 (38–77) |
| Antral Motility Index (MI) (mmHg) | 13.59 (12.57–14.81) |
| Antral hypomotility § (n, %) | 14 (53.8%) |
| BMI Before Botulinum Toxin (Median; IQR) | BMI after Botulinum Toxin (Median; IQR) | p-Value | |
|---|---|---|---|
| Overall (n = 30) | 23.9 (20.5–26.5) | 23.0 (19.8–26.8) | 0.01 |
| Responders (n = 8) | 27.6 (24.3–30.2) | 27.6 (22.9–30.2) | 0.67 |
| Non-responders (n = 22) | 22.6 (19.3–24.9) | 21.8 (19.3–24.3) | <0.01 |
| Parameters | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Age | 1.01 (0.96–1.06) | 0.62 |
| Gender | 1.25 (0.32–4.94) | 0.75 |
| Etiology | ||
| Idiopathic vs. non-idiopathic | 0.63 (0.17–2.32) | 0.48 |
| Diabetic vs. non-diabetic | 0.80 (0.20–3.16) | 0.75 |
| Post-surgical vs. non post-surgical | 2.67 (0.48–14.79) | 0.26 |
| Dose of botulinum toxin | 1.00 (1.00–1.00) | 0.62 |
| Antral contraction frequency | 0.66 (0.15–2.99) | 0.59 |
| Antral contraction amplitude | 0.99 (0.96–1.03) | 0.71 |
| Antral motility index | 0.65 (0.36–1.17) | 0.15 |
| Antral hypomotility | 5.25 (0.50–54.91) | 0.17 |
| Gastric half emptying time (solids) | 1.00 (0.99–1.01) | 0.85 |
| Gastric retention at 120 min | 1.01 (0.94–1.08) | 0.84 |
| Gastric retention at 240 min | 1.00 (0.95–1.04) | 0.81 |
| Weight before botulinum toxin | 1.04 (0.98–1.10) | 0.24 |
| BMI before botulinum toxin | 1.15 (0.97–1.36) | 0.11 |
| Parameters | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Age | 1.02 (0.96–1.08) | 0.56 |
| Gender | 0.40 (0.08–1.90) | 0.25 |
| Etiology | ||
| Idiopathic vs. non-idiopathic | 2.23 (0.50–10.00) | 0.30 |
| Diabetic vs. non-diabetic | 0.33 (0.06–1.97) | 0.23 |
| Post-surgical vs. non post-surgical | 1.13 (0.21–5.97) | 0.89 |
| Dose of botulinum toxin | 1.00 (1.00–1.00) | 0.92 |
| Antral contraction frequency | 0.47 (0.10–2.11) | 0.32 |
| Antral contraction amplitude | 1.02 (0.99–1.06) | 0.23 |
| Antral motility index | 0.98 (0.56–1.69) | 0.94 |
| Antral hypomotility | 0.78 (0.04–14.75) | 0.87 |
| Gastric half emptying time (solids) | 0.99 (0.98–1.00) | 0.36 |
| Gastric retention at 120 min | 0.96 (0.89–1.05) | 0.38 |
| Gastric retention at 240 min | 0.97 (0.92–1.02) | 0.21 |
| Weight before botulinum toxin | 1.02 (0.96–1.08) | 0.61 |
| BMI before botulinum toxin | 1.13 (0.94–1.35) | 0.21 |
| Additional Treatment | N (%) (Total n = 40) |
|---|---|
| Symptoms improved, no further treatment | 11 (27.5) |
| Diet/prokinetics | 10 (25.0) |
| Gastric rest and nasoduodenal tube | 6 (15.0) |
| PEG-J | 10 (25.0) |
| Laparoscopic jejunostomy | 1 (2.5) |
| Unknown | 2 (5.0) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smeets, F.G.M.; Strijbos, D.; Keszthelyi, D.; Hoge, C.V.; Kruimel, J.W.; Conchillo, J.M.; Masclee, A.A.M. Endoscopic Botulinum Toxin for Gastroparesis: Results of a Retrospective Series. Gastrointest. Disord. 2019, 1, 164-175. https://doi.org/10.3390/gidisord1010012
Smeets FGM, Strijbos D, Keszthelyi D, Hoge CV, Kruimel JW, Conchillo JM, Masclee AAM. Endoscopic Botulinum Toxin for Gastroparesis: Results of a Retrospective Series. Gastrointestinal Disorders. 2019; 1(1):164-175. https://doi.org/10.3390/gidisord1010012
Chicago/Turabian StyleSmeets, Fabiënne G. M., Denise Strijbos, Daniel Keszthelyi, Chantal V. Hoge, Joanna W. Kruimel, José M. Conchillo, and Ad A.M. Masclee. 2019. "Endoscopic Botulinum Toxin for Gastroparesis: Results of a Retrospective Series" Gastrointestinal Disorders 1, no. 1: 164-175. https://doi.org/10.3390/gidisord1010012