Main Disorders of Gastrointestinal Tract in Older People: An Overview

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Aim
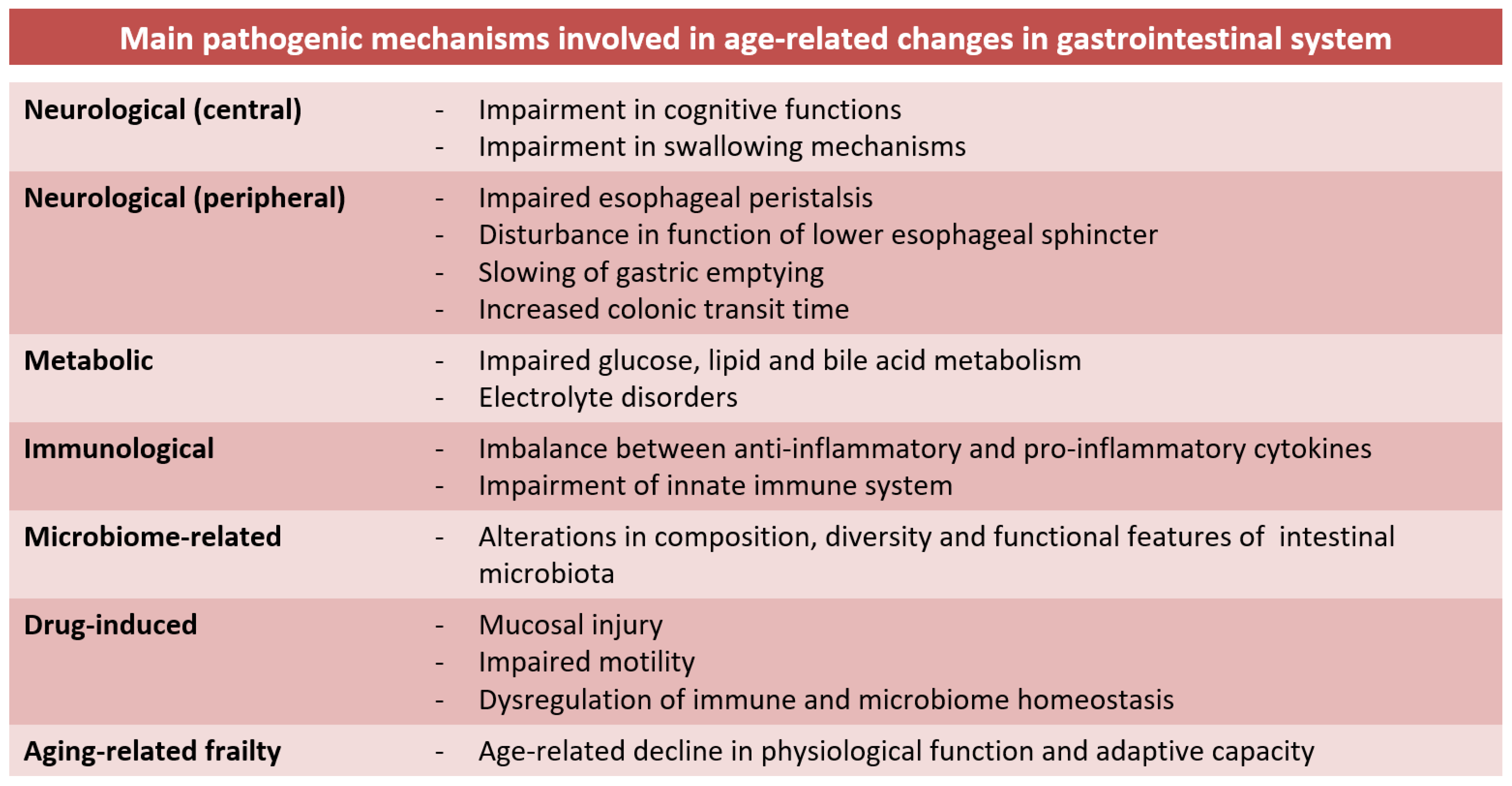
3. Basic Mechanisms of Aging Gastrointestinal Tract
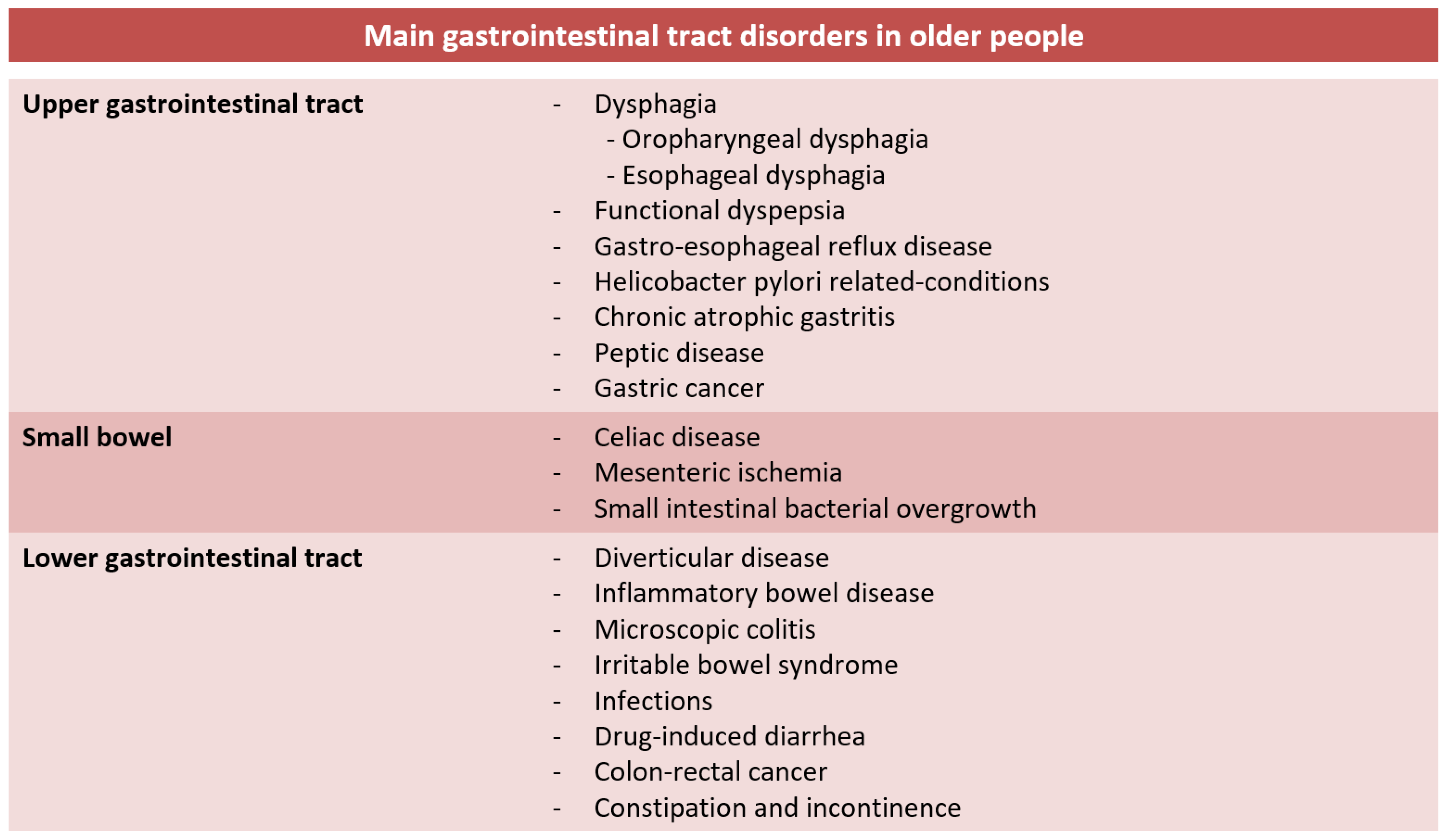
4. Main Gastrointestinal Tract Disorders in Older People
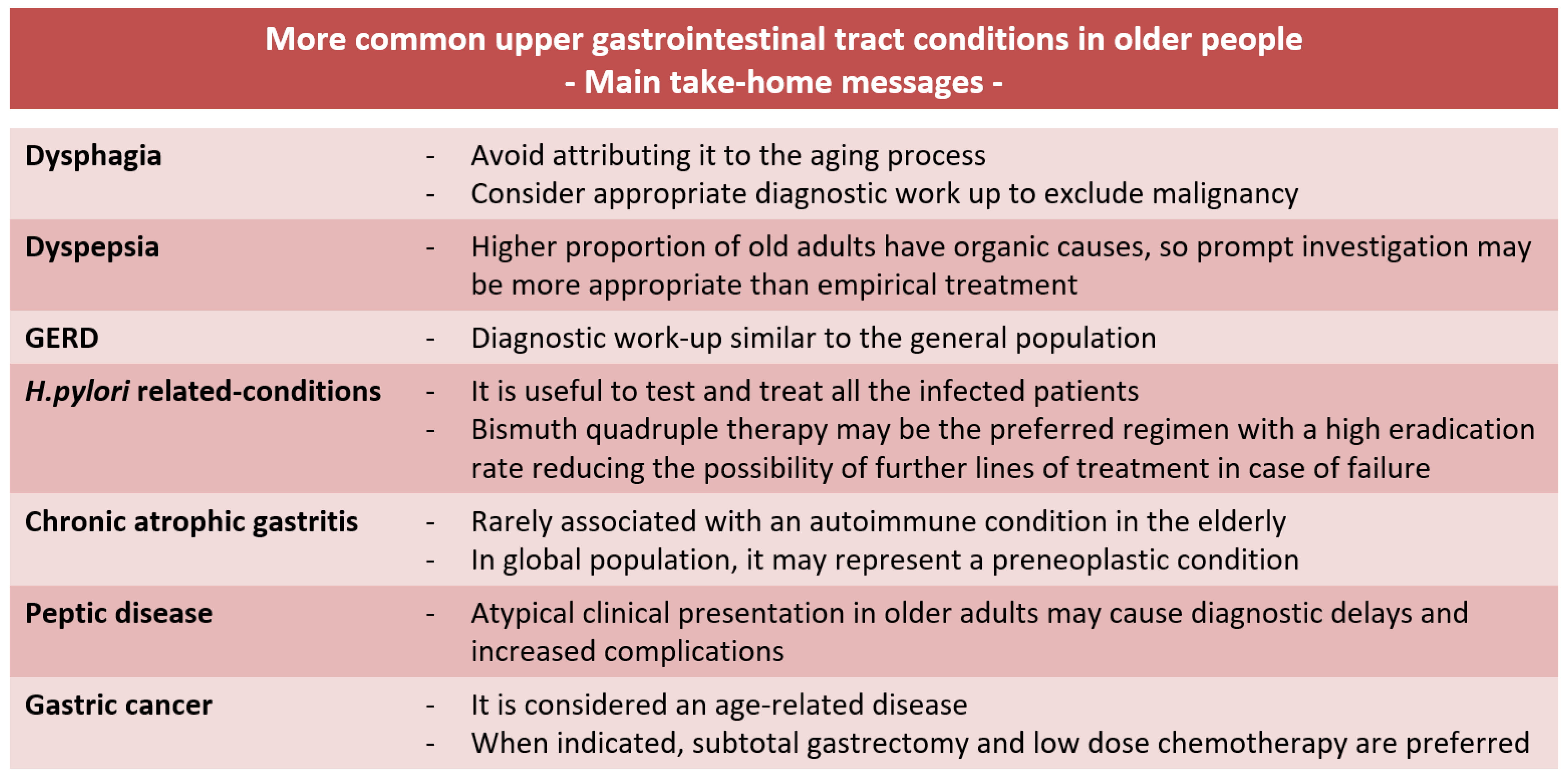
4.1. Upper Gastrointestinal Tract Diseases
4.1.1. Dysphagia
4.1.2. Functional Dyspepsia
4.1.3. Gastroesophageal Reflux Disease
4.1.4. Helicobacter pylori
4.1.5. Chronic Atrophic Gastritis
4.1.6. Peptic Disease
4.1.7. Gastric Cancer
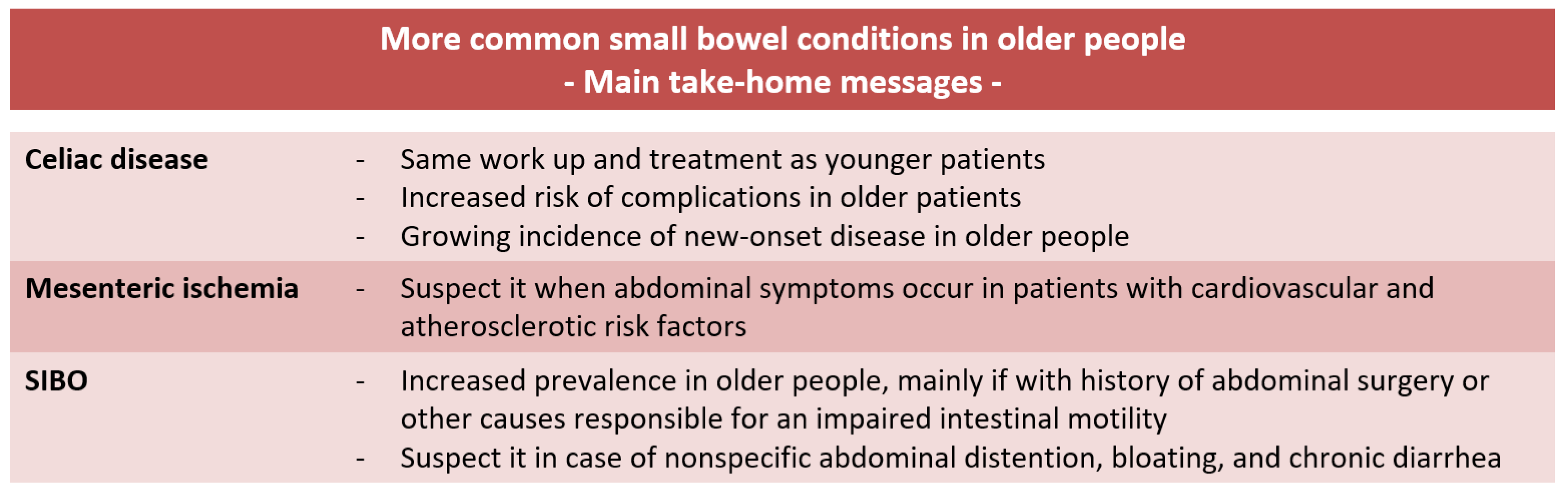
4.2. Small Bowel Diseases
4.2.1. Celiac Disease
4.2.2. Mesenteric Ischemia
4.2.3. Small Intestinal Bacterial Overgrowth
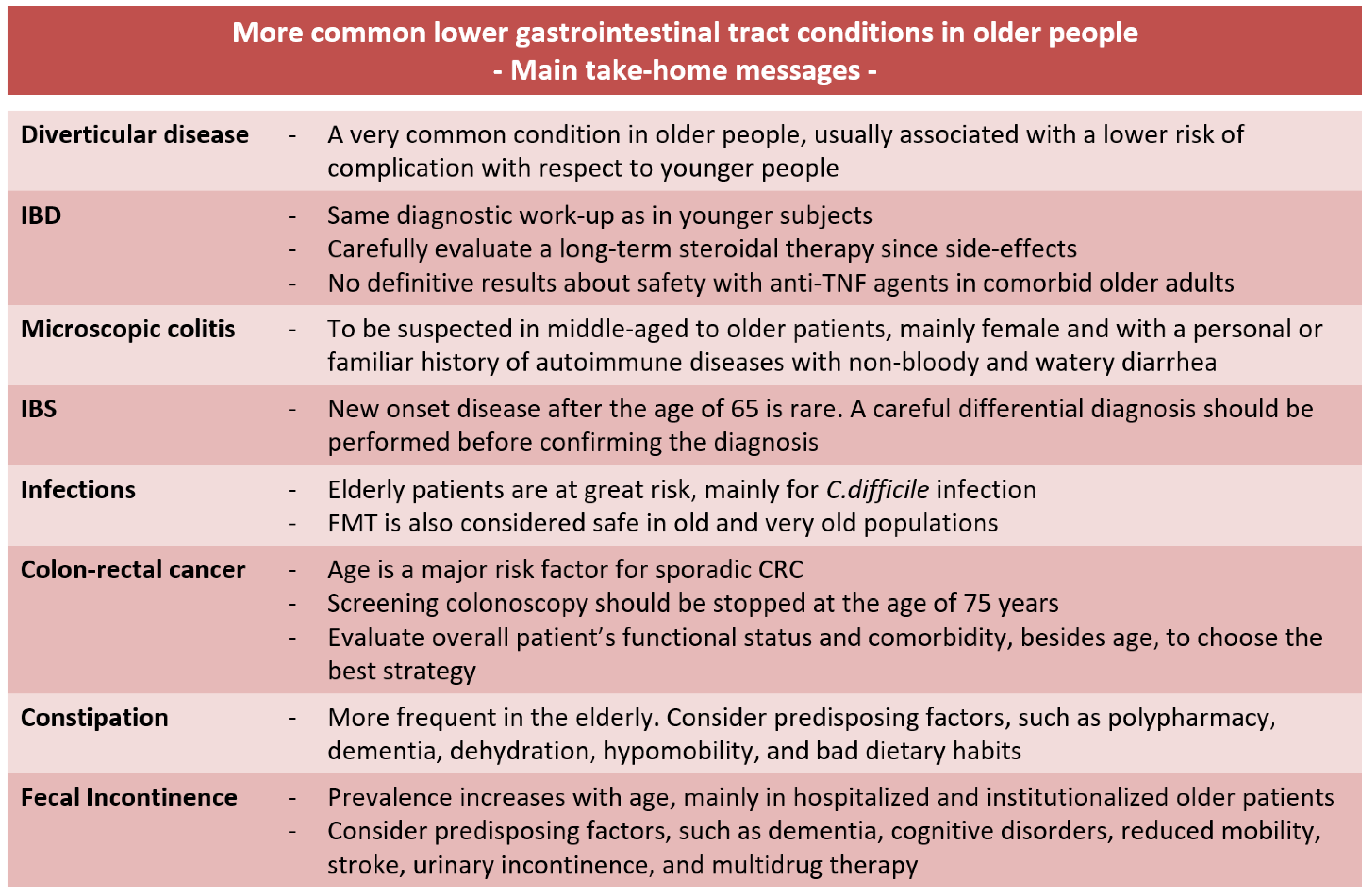
4.3. Lower Gastrointestinal Tract Diseases
4.3.1. Diverticular Disease
4.3.2. Inflammatory Bowel Diseases
4.3.3. Microscopic Colitis
4.3.4. Irritable Bowel Syndrome
4.3.5. Gut Infections
4.3.6. Colon–Rectal Cancer
4.3.7. Constipation
4.3.8. Fecal Incontinence
5. Discussion
6. Limitations of the Study
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Soenen, S.; Rayner, C.K.; Jones, K.L.; Horowitz, M. The Ageing Gastrointestinal Tract. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 12–18. [Google Scholar] [CrossRef]
- Bhutto, A.; Morley, J.E. The Clinical Significance of Gastrointestinal Changes with Aging. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 651–660. [Google Scholar] [CrossRef]
- Salles, N. Basic Mechanisms of the Aging Gastrointestinal Tract. Dig. Dis. 2007, 25, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. The Aging Gut: Physiology. Clin. Geriatr. Med. 2007, 23, 757–767, v–vi. [Google Scholar] [CrossRef]
- Besanko, L.K.; Burgstad, C.M.; Cock, C.; Heddle, R.; Fraser, A.; Fraser, R.J.L. Changes in Esophageal and Lower Esophageal Sphincter Motility with Healthy Aging. J. Gastrointest. Liver Dis. JGLD 2014, 23, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Soenen, S.; Rayner, C.K.; Horowitz, M.; Jones, K.L. Gastric Emptying in the Elderly. Clin. Geriatr. Med. 2015, 31, 339–353. [Google Scholar] [CrossRef]
- Sarna, S.K. Physiology and Pathophysiology of Colonic Motor Activity (2). Dig. Dis. Sci. 1991, 36, 998–1018. [Google Scholar] [CrossRef] [PubMed]
- Kagaya, M.; Iwata, N.; Toda, Y.; Nakae, Y.; Kondo, T. Small Bowel Transit Time and Colonic Fermentation in Young and Elderly Women. J. Gastroenterol. 1997, 32, 453–456. [Google Scholar] [CrossRef]
- Husebye, E.; Engedal, K. The Patterns of Motility Are Maintained in the Human Small Intestine throughout the Process of Aging. Scand. J. Gastroenterol. 1992, 27, 397–404. [Google Scholar] [CrossRef]
- Robbins, J.; Bridges, A.D.; Taylor, A. Oral, Pharyngeal and Esophageal Motor Function in Aging. GI Motil. Online 2006. [Google Scholar] [CrossRef]
- Namasivayam-MacDonald, A.M.; Riquelme, L.F. Presbyphagia to Dysphagia: Multiple Perspectives and Strategies for Quality Care of Older Adults. Semin. Speech Lang. 2019, 40, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Smith, K. Neurogastroenterology: Ageing, ENS Senescence and Gastrointestinal Motility. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 141. [Google Scholar] [CrossRef] [PubMed]
- Saffrey, M.J. Aging of the Mammalian Gastrointestinal Tract: A Complex Organ System. AGE 2014, 36, 9603. [Google Scholar] [CrossRef] [PubMed]
- Ren, W.; Wu, K.; Li, X.; Luo, M.; Liu, H.; Zhang, S.; Hu, Y. Age-Related Changes in Small Intestinal Mucosa Epithelium Architecture and Epithelial Tight Junction in Rat Models. Aging Clin. Exp. Res. 2014, 26, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Man, A.L.; Bertelli, E.; Rentini, S.; Regoli, M.; Briars, G.; Marini, M.; Watson, A.J.M.; Nicoletti, C. Age-Associated Modifications of Intestinal Permeability and Innate Immunity in Human Small Intestine. Clin. Sci. 2015, 129, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Newton, J.L. Effect of Age-Related Changes in Gastric Physiology on Tolerability of Medications for Older People. Drugs Aging 2005, 22, 655–661. [Google Scholar] [CrossRef]
- Mabbott, N.A. A Breakdown in Communication? Understanding the Effects of Aging on the Human Small Intestine Epithelium. Clin. Sci. 2015, 129, 529–531. [Google Scholar] [CrossRef]
- Man, A.L.; Gicheva, N.; Nicoletti, C. The Impact of Ageing on the Intestinal Epithelial Barrier and Immune System. Cell. Immunol. 2014, 289, 112–118. [Google Scholar] [CrossRef]
- O’Connor, A.; O’Moráin, C. Digestive Function of the Stomach. Dig. Dis. 2014, 32, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Grishina, I.; Fenton, A.; Sankaran-Walters, S. Gender Differences, Aging and Hormonal Status in Mucosal Injury and Repair. Aging Dis. 2014, 5, 160–169. [Google Scholar] [CrossRef] [PubMed]
- ECRI Health Technology Assessment Group. Diagnosis and Treatment of Swallowing Disorders (Dysphagia) in Acute-Care Stroke Patients: Summary; Agency for Healthcare Research and Quality: Rockville, MD, USA, 1999.
- Reynolds, J.C.; George, B.R. Dysphagia. In Geriatric Gastroenterology; Pitchumoni, C.S., Dharmarajan, T.S., Eds.; Springer: New York, NY, USA, 2012; pp. 293–300. ISBN 978-1-4419-1623-5. [Google Scholar]
- Barczi, S.R.; Sullivan, P.A.; Robbins, J. How Should Dysphagia Care of Older Adults Differ? Establishing Optimal Practice Patterns. Semin. Speech Lang. 2000, 21, 347–361. [Google Scholar] [CrossRef]
- Barrera, M.; Wells, B. Presbyphagia Versus Dysphagia: Normal Versus Abnormal Swallowing Symptoms in Older Adults with Parkinson Disease and Multiple Sclerosis. Top. Geriatr. Rehabil. 2019, 35, 217–233. [Google Scholar] [CrossRef]
- Humbert, I.A.; Robbins, J. Dysphagia in the Elderly. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 853–866, ix–x. [Google Scholar] [CrossRef] [PubMed]
- McCarty, E.B.; Chao, T.N. Dysphagia and Swallowing Disorders. Med. Clin. N. Am. 2021, 105, 939–954. [Google Scholar] [CrossRef] [PubMed]
- Firth, M.; Prather, C.M. Gastrointestinal Motility Problems in the Elderly Patient. Gastroenterology 2002, 122, 1688–1700. [Google Scholar] [CrossRef] [PubMed]
- Cock, C.; Besanko, L.K.; Burgstad, C.M.; Thompson, A.; Kritas, S.; Heddle, R.; Fraser, R.J.; Omari, T.I. Age-Related Impairment of Esophagogastric Junction Relaxation and Bolus Flow Time. World J. Gastroenterol. 2017, 23, 2785–2794. [Google Scholar] [CrossRef] [PubMed]
- Shenoda, B.; Degen, K.C.; Ford, W. Presbyesophagus Presented with Chronic Intermittent Dysphagia. Aging Clin. Exp. Res. 2019, 31, 1343–1346. [Google Scholar] [CrossRef] [PubMed]
- Stanghellini, V.; Chan, F.K.L.; Hasler, W.L.; Malagelada, J.R.; Suzuki, H.; Tack, J.; Talley, N.J. Gastroduodenal Disorders. Gastroenterology 2016, 150, 1380–1392. [Google Scholar] [CrossRef]
- Drossman, D.A.; Hasler, W.L. Rome IV-Functional GI Disorders: Disorders of Gut-Brain Interaction. Gastroenterology 2016, 150, 1257–1261. [Google Scholar] [CrossRef]
- Walker, M.M.; Talley, N.J. Functional Dyspepsia in the Elderly. Curr. Gastroenterol. Rep. 2019, 21, 54. [Google Scholar] [CrossRef]
- Kay, L. Prevalence, Incidence and Prognosis of Gastrointestinal Symptoms in a Random Sample of an Elderly Population. Age Ageing 1994, 23, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.H.; Lydeard, S.E.; Hobbs, F.D.; Kenkre, J.E.; Williams, E.I.; Jones, S.J.; Repper, J.A.; Caldow, J.L.; Dunwoodie, W.M.; Bottomley, J.M. Dyspepsia in England and Scotland. Gut 1990, 31, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Ronkainen, J. Age and Male Gender Are Associated with a Decline in Functional Gastrointestinal Symptoms: Prospective 10 Year Follow-Up of the Kalixanda Study. Available online: https://www.academia.edu/82153225/Su1640_Age_and_Male_Gender_are_Associated_with_a_Decline_in_Functional_Gastrointestinal_Symptoms_Prospective_10_Year_Follow_Up_of_the_Kalixanda_Study (accessed on 2 April 2023).
- Pound, S.E.; Heading, R.C. Diagnosis and Treatment of Dyspepsia in the Elderly. Drugs Aging 1995, 7, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Moayyedi, P.M.; Lacy, B.E.; Andrews, C.N.; Enns, R.A.; Howden, C.W.; Vakil, N. ACG and CAG Clinical Guideline: Management of Dyspepsia. Off. J. Am. Coll. Gastroenterol. ACG 2017, 112, 988. [Google Scholar] [CrossRef]
- Chait, M.M. Gastroesophageal Reflux Disease: Important Considerations for the Older Patients. World J. Gastrointest. Endosc. 2010, 2, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L.; Boscardin, W.J.; Steinman, M.A.; Schwartz, J.B. Age and Sex Variation in Prevalence of Chronic Medical Conditions in Older Residents of U.S. Nursing Homes. J. Am. Geriatr. Soc. 2012, 60, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Kurin, M.; Fass, R. Management of Gastroesophageal Reflux Disease in the Elderly Patient. Drugs Aging 2019, 36, 1073–1081. [Google Scholar] [CrossRef]
- Pilotto, A.; Franceschi, M.; Paris, F. Recent Advances in the Treatment of GERD in the Elderly: Focus on Proton Pump Inhibitors. Int. J. Clin. Pract. 2005, 59, 1204–1209. [Google Scholar] [CrossRef]
- Fei, L.; Rossetti, G.; Moccia, F.; Marra, T.; Guadagno, P.; Docimo, L.; Cimmino, M.; Napolitano, V.; Docimo, G.; Napoletano, D.; et al. Is the Advanced Age a Contraindication to GERD Laparoscopic Surgery? Results of a Long Term Follow-Up. BMC Surg. 2013, 13, S13. [Google Scholar] [CrossRef]
- Suerbaum, S.; Michetti, P. Helicobacter Pylori Infection. N. Engl. J. Med. 2002, 347, 1175–1186. [Google Scholar] [CrossRef]
- Burucoa, C.; Axon, A. Epidemiology of Helicobacter Pylori Infection. Helicobacter 2017, 22, e12403. [Google Scholar] [CrossRef]
- Goh, K.-L.; Chan, W.-K.; Shiota, S.; Yamaoka, Y. Epidemiology of Helicobacter Pylori Infection and Public Health Implications. Helicobacter 2011, 16, 1–9. [Google Scholar] [CrossRef]
- Pilott, A.; Fabrello, R.; Franceschi, M.; Scagnelli, M.; Soffiati, F.; Di Mario, F.; Fortunato, A.; Valerio, G. Helicobacter Pylori Infection in Asymptomatic Elderly Subjects Living at Home or in a Nursing Home: Effects on Gastric Function and Nutritional Status. Age Ageing 1996, 25, 245–249. [Google Scholar] [CrossRef]
- Liu, D.-S.; Wang, Y.-H.; Zeng, Z.-R.; Zhang, Z.-Y.; Lu, H.; Xu, J.-M.; Du, Y.-Q.; Li, Y.; Wang, J.-B.; Xu, S.-P.; et al. Primary Antibiotic Resistance of Helicobacter Pylori in Chinese Patients: A Multiregion Prospective 7-Year Study. Clin. Microbiol. Infect. 2018, 24, 780.e5–780.e8. [Google Scholar] [CrossRef] [PubMed]
- Tielleman, T.; Bujanda, D.; Cryer, B. Epidemiology and Risk Factors for Upper Gastrointestinal Bleeding. Gastrointest. Endosc. Clin. N. Am. 2015, 25, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; Gravina, A.G.; Eusebi, L.H.; Pellegrino, R.; Palladino, G.; Frazzoni, L.; Dajti, E.; Gasbarrini, A.; Di Mario, F.; Zagari, R.M.; et al. Management of Helicobacter Pylori Infection: Guidelines of the Italian Society of Gastroenterology (SIGE) and the Italian Society of Digestive Endoscopy (SIED). Dig. Liver Dis. 2022, 54, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Joshita, S.; Yamamoto, C.; Yanagisawa, T.; Miyazawa, T.; Miyazawa, M.; Kubota, D.; Sato, J.; Umemura, T.; Tanaka, E. Efficacy and Safety of Eradication Therapy for Elderly Patients with Helicobacter Pylori Infection. Medicine 2019, 98, e16619. [Google Scholar] [CrossRef] [PubMed]
- Dore, M.P.; Maragkoudakis, E.; Pironti, A.; Tadeu, V.; Tedde, R.; Realdi, G.; Delitala, G. Twice-a-Day Quadruple Therapy for Eradication of Helicobacter Pylori in the Elderly. Helicobacter 2006, 11, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.; Xu, H.-M.; Zhang, D.-K. Focusing on Helicobacter Pylori Infection in the Elderly. Front. Cell. Infect. Microbiol. 2023, 13, 1121947. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.C.; Piazuelo, M.B.; Kuipers, E.J.; Li, D. AGA Clinical Practice Update on the Diagnosis and Management of Atrophic Gastritis: Expert Review. Gastroenterology 2021, 161, 1325–1332.e7. [Google Scholar] [CrossRef]
- Pilotto, A.; Salles, N. Helicobacter Pylori Infection in Geriatrics. Helicobacter 2002, 7 (Suppl. S1), 56–62. [Google Scholar] [CrossRef]
- Kim, N.; Park, Y.S.; Cho, S.-I.; Lee, H.S.; Choe, G.; Kim, I.W.; Won, Y.-D.; Park, J.H.; Kim, J.S.; Jung, H.C.; et al. Prevalence and Risk Factors of Atrophic Gastritis and Intestinal Metaplasia in a Korean Population without Significant Gastroduodenal Disease. Helicobacter 2008, 13, 245–255. [Google Scholar] [CrossRef]
- Parlesak, A.; Klein, B.; Schecher, K.; Bode, J.C.; Bode, C. Prevalence of Small Bowel Bacterial Overgrowth and Its Association with Nutrition Intake in Nonhospitalized Older Adults. J. Am. Geriatr. Soc. 2003, 51, 768–773. [Google Scholar] [CrossRef]
- Kokkola, A.; Sipponen, P.; Rautelin, H.; Härkönen, M.; Kosunen, T.U.; Haapiainen, R.; Puolakkainen, P. The Effect of Helicobacter Pylori Eradication on the Natural Course of Atrophic Gastritis with Dysplasia. Aliment. Pharmacol. Ther. 2002, 16, 515–520. [Google Scholar] [CrossRef]
- Lu, B.; Chen, M.-T.; Fan, Y.-H.; Liu, Y.; Meng, L.-N. Effects of Helicobacter Pylori Eradication on Atrophic Gastritis and Intestinal Metaplasia: A 3-Year Follow-up Study. World J. Gastroenterol. WJG 2005, 11, 6518–6520. [Google Scholar] [CrossRef] [PubMed]
- Malik, T.F.; Gnanapandithan, K.; Singh, K. Peptic Ulcer Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Pilotto, A.; Franceschi, M.; Maggi, S.; Addante, F.; Sancarlo, D. Optimal Management of Peptic Ulcer Disease in the Elderly. Drugs Aging 2010, 27, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Lanas, A.; Scheiman, J. Low-Dose Aspirin and Upper Gastrointestinal Damage: Epidemiology, Prevention and Treatment. Curr. Med. Res. Opin. 2007, 23, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Tarnawski, A.S.; Ahluwalia, A. Increased Susceptibility of Aging Gastric Mucosa to Injury and Delayed Healing: Clinical Implications. World J. Gastroenterol. 2018, 24, 4721–4727. [Google Scholar] [CrossRef]
- Liang, Y.-X.; Deng, J.-Y.; Guo, H.-H.; Ding, X.-W.; Wang, X.-N.; Wang, B.-G.; Zhang, L.; Liang, H. Characteristics and Prognosis of Gastric Cancer in Patients Aged ≥ 70 Years. World J. Gastroenterol. 2013, 19, 6568–6578. [Google Scholar] [CrossRef]
- Orsenigo, E.; Tomajer, V.; Palo, S.D.; Carlucci, M.; Vignali, A.; Tamburini, A.; Staudacher, C. Impact of Age on Postoperative Outcomes in 1118 Gastric Cancer Patients Undergoing Surgical Treatment. Gastric Cancer 2007, 10, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Tsujitani, S.; Katano, K.; Oka, A.; Ikeguchi, M.; Maeta, M.; Kaibara, N. Limited Operation for Gastric Cancer in the Elderly. Br. J. Surg. 1996, 83, 836–839. [Google Scholar] [CrossRef] [PubMed]
- Hall, P.S.; Swinson, D.; Cairns, D.A.; Waters, J.S.; Petty, R.; Allmark, C.; Ruddock, S.; Falk, S.; Wadsley, J.; Roy, R.; et al. Efficacy of Reduced-Intensity Chemotherapy With Oxaliplatin and Capecitabine on Quality of Life and Cancer Control Among Older and Frail Patients With Advanced Gastroesophageal Cancer: The GO2 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Rashtak, S.; Murray, J.A. Celiac Disease in the Elderly. Gastroenterol. Clin. N. Am. 2009, 38, 433–446. [Google Scholar] [CrossRef]
- Lohi, S.; Mustalahti, K.; Kaukinen, K.; Laurila, K.; Collin, P.; Rissanen, H.; Lohi, O.; Bravi, E.; Gasparin, M.; Reunanen, A.; et al. Increasing Prevalence of Coeliac Disease over Time. Aliment. Pharmacol. Ther. 2007, 26, 1217–1225. [Google Scholar] [CrossRef]
- Freeman, H.J. Adult Celiac Disease in the Elderly. World J. Gastroenterol. 2008, 14, 6911–6914. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Murray, J.A. Liver Involvement in Celiac Disease. Minerva Med. 2008, 99, 595–604. [Google Scholar]
- Ch’ng, C.L.; Jones, M.K.; Kingham, J.G.C. Celiac Disease and Autoimmune Thyroid Disease. Clin. Med. Res. 2007, 5, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Cappello, M.; Morreale, G.C.; Licata, A. Elderly Onset Celiac Disease: A Narrative Review. Clin. Med. Insights Gastroenterol. 2016, 9, 41–49. [Google Scholar] [CrossRef]
- van Gils, T.; Nijeboer, P.; Overbeek, L.I.; Hauptmann, M.; Castelijn, D.A.; Bouma, G.; Mulder, C.J.; van Leeuwen, F.E.; de Jong, D. Risks for Lymphoma and Gastrointestinal Carcinoma in Patients with Newly Diagnosed Adult-Onset Celiac Disease: Consequences for Follow-up: Celiac Disease, Lymphoma and GI Carcinoma. United Eur. Gastroenterol. J. 2018, 6, 1485–1495. [Google Scholar] [CrossRef]
- Bala, M.; Catena, F.; Kashuk, J.; De Simone, B.; Gomes, C.A.; Weber, D.; Sartelli, M.; Coccolini, F.; Kluger, Y.; Abu-Zidan, F.M.; et al. Acute Mesenteric Ischemia: Updated Guidelines of the World Society of Emergency Surgery. World J. Emerg. Surg. 2022, 17, 54. [Google Scholar] [CrossRef]
- Kärkkäinen, J.M.; Lehtimäki, T.T.; Manninen, H.; Paajanen, H. Acute Mesenteric Ischemia Is a More Common Cause than Expected of Acute Abdomen in the Elderly. J. Gastrointest. Surg. 2015, 19, 1407–1414. [Google Scholar] [CrossRef]
- Kärkkäinen, J.M. Acute Mesenteric Ischemia in Elderly Patients. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 985–988. [Google Scholar] [CrossRef]
- Cangemi, J.R.; Picco, M.F. Intestinal Ischemia in the Elderly. Gastroenterol. Clin. N. Am. 2009, 38, 527–540. [Google Scholar] [CrossRef]
- van Dijk, L.J.; van Noord, D.; de Vries, A.C.; Kolkman, J.J.; Geelkerken, R.H.; Verhagen, H.J.; Moelker, A.; Bruno, M.J. Clinical Management of Chronic Mesenteric Ischemia. United Eur. Gastroenterol. J. 2019, 7, 179–188. [Google Scholar] [CrossRef]
- Dukowicz, A.C.; Lacy, B.E.; Levine, G.M. Small Intestinal Bacterial Overgrowth: A Comprehensive Review. Gastroenterol. Hepatol. 2007, 3, 112–122. [Google Scholar]
- Comparato, G.; Pilotto, A.; Franzè, A.; Franceschi, M.; Di Mario, F. Diverticular Disease in the Elderly. Dig. Dis. 2007, 25, 151–159. [Google Scholar] [CrossRef]
- Matrana, M.R.; Margolin, D.A. Epidemiology and Pathophysiology of Diverticular Disease. Clin. Colon Rectal Surg. 2009, 22, 141–146. [Google Scholar] [CrossRef]
- Strate, L.L.; Modi, R.; Cohen, E.; Spiegel, B.M.R. Diverticular Disease as a Chronic Illness: Evolving Epidemiologic and Clinical Insights. Am. J. Gastroenterol. 2012, 107, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Boynton, W.; Floch, M. New Strategies for the Management of Diverticular Disease: Insights for the Clinician. Ther. Adv. Gastroenterol. 2013, 6, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, F.; Crichton, M.; Dahl, C.; Nucera, R.; Jenkins, J.; Marx, W.; Marshall, S. Role of Dietary Fibre in Older Adults with Asymptomatic (AS) or Symptomatic Uncomplicated Diverticular Disease (SUDD): Systematic Review and Meta-Analysis. Maturitas 2019, 130, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Calini, G.; Abd El Aziz, M.A.; Paolini, L.; Abdalla, S.; Rottoli, M.; Mari, G.; Larson, D.W. Symptomatic Uncomplicated Diverticular Disease (SUDD): Practical Guidance and Challenges for Clinical Management. Clin. Exp. Gastroenterol. 2023, 16, 29–43. [Google Scholar] [CrossRef]
- Loftus, E.; Silverstein, M.; Sandborn, W.; Tremaine, W.; Harmsen, W.; Zinsmeister, A. Ulcerative Colitis in Olmsted County, Minnesota, 1940-1993: Incidence, Prevalence, and Survival. Gut 2000, 46, 336–343. [Google Scholar] [CrossRef]
- Danpanichkul, P.; Suparan, K.; Arayakarnkul, S.; Jaroenlapnopparat, A.; Polpichai, N.; Fangsaard, P.; Kongarin, S.; Srisurapanont, K.; Sukphutanan, B.; Wanchaitanawong, W.; et al. Global Epidemiology and Burden of Elderly-Onset Inflammatory Bowel Disease: A Decade in Review. J. Clin. Med. 2023, 12, 5142. [Google Scholar] [CrossRef] [PubMed]
- Lakatos, P.L.; David, G.; Pandur, T.; Erdelyi, Z.; Mester, G.; Balogh, M.; Szipocs, I.; Molnar, C.; Komaromi, E.; Kiss, L.S.; et al. IBD in the Elderly Population: Results from a Population-Based Study in Western Hungary, 1977–2008. J. Crohns Colitis 2011, 5, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Charpentier, C.; Salleron, J.; Savoye, G.; Fumery, M.; Merle, V.; Laberenne, J.-E.; Vasseur, F.; Dupas, J.-L.; Cortot, A.; Dauchet, L.; et al. Natural History of Elderly-Onset Inflammatory Bowel Disease: A Population-Based Cohort Study. Gut 2014, 63, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Tran, V.; Limketkai, B.N.; Sauk, J.S. IBD in the Elderly: Management Challenges and Therapeutic Considerations. Curr. Gastroenterol. Rep. 2019, 21, 60. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target Strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, J.-F.; Wiseman, D.; Lakatos, P.L.; Bessissow, T. Elderly Patients with Inflammatory Bowel Disease: Updated Review of the Therapeutic Landscape. World J. Gastroenterol. 2019, 25, 4158–4171. [Google Scholar] [CrossRef] [PubMed]
- Sturm, A.; Maaser, C.; Mendall, M.; Karagiannis, D.; Karatzas, P.; Ipenburg, N.; Sebastian, S.; Rizzello, F.; Limdi, J.; Katsanos, K.; et al. European Crohn’s and Colitis Organisation Topical Review on IBD in the Elderly. J. Crohns Colitis 2017, 11, 263–273. [Google Scholar] [CrossRef]
- Gisbert, J.P.; González-Lama, Y.; Maté, J. 5-Aminosalicylates and Renal Function in Inflammatory Bowel Disease: A Systematic Review. Inflamm. Bowel Dis. 2007, 13, 629–638. [Google Scholar] [CrossRef]
- Lobatón, T.; Ferrante, M.; Rutgeerts, P.; Ballet, V.; Van Assche, G.; Vermeire, S. Efficacy and Safety of Anti-TNF Therapy in Elderly Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2015, 42, 441–451. [Google Scholar] [CrossRef]
- Cottone, M.; Kohn, A.; Daperno, M.; Armuzzi, A.; Guidi, L.; D’Inca, R.; Bossa, F.; Angelucci, E.; Biancone, L.; Gionchetti, P.; et al. Advanced Age Is an Independent Risk Factor for Severe Infections and Mortality in Patients given Anti-Tumor Necrosis Factor Therapy for Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2011, 9, 30–35. [Google Scholar] [CrossRef]
- Adar, T.; Faleck, D.; Sasidharan, S.; Cushing, K.; Borren, N.Z.; Nalagatla, N.; Ungaro, R.; Sy, W.; Owen, S.C.; Patel, A.; et al. Comparative Safety and Effectiveness of Tumor Necrosis Factor α Antagonists and Vedolizumab in Elderly IBD Patients: A Multicentre Study. Aliment. Pharmacol. Ther. 2019, 49, 873–879. [Google Scholar] [CrossRef]
- Yajnik, V.; Khan, N.; Dubinsky, M.; Axler, J.; James, A.; Abhyankar, B.; Lasch, K. Efficacy and Safety of Vedolizumab in Ulcerative Colitis and Crohn’s Disease Patients Stratified by Age. Adv. Ther. 2017, 34, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Bureau, U.C. An Aging World: 2015. Available online: https://www.census.gov/library/publications/2016/demo/P95-16-1.html (accessed on 27 November 2023).
- Ananthakrishnan, A.N.; Shi, H.Y.; Tang, W.; Law, C.C.Y.; Sung, J.J.Y.; Chan, F.K.L.; Ng, S.C. Systematic Review and Meta-Analysis: Phenotype and Clinical Outcomes of Older-Onset Inflammatory Bowel Disease. J. Crohns Colitis 2016, 10, 1224–1236. [Google Scholar] [CrossRef] [PubMed]
- Ooijevaar, R.E.; Terveer, E.M.; Verspaget, H.W.; Kuijper, E.J.; Keller, J.J. Clinical Application and Potential of Fecal Microbiota Transplantation. Annu. Rev. Med. 2019, 70, 335–351. [Google Scholar] [CrossRef] [PubMed]
- Boicean, A.; Birlutiu, V.; Ichim, C.; Anderco, P.; Birsan, S. Fecal Microbiota Transplantation in Inflammatory Bowel Disease. Biomedicines 2023, 11, 1016. [Google Scholar] [CrossRef]
- Boicean, A.; Birlutiu, V.; Ichim, C.; Brusnic, O.; Onișor, D.M. Fecal Microbiota Transplantation in Liver Cirrhosis. Biomedicines 2023, 11, 2930. [Google Scholar] [CrossRef]
- Cheng, Y.-W.; Fischer, M. The Present Status of Fecal Microbiota Transplantation and Its Value in the Elderly. Curr. Treat. Options Gastroenterol. 2017, 15, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Tome, J.; Kamboj, A.K.; Pardi, D.S. Microscopic Colitis: A Concise Review for Clinicians. Mayo Clin. Proc. 2021, 96, 1302–1308. [Google Scholar] [CrossRef]
- Nielsen, O.H.; Fernandez-Banares, F.; Sato, T.; Pardi, D.S. Microscopic Colitis: Etiopathology, Diagnosis, and Rational Management. eLife 2022, 11, e79397. [Google Scholar] [CrossRef]
- Tong, J.; Zheng, Q.; Zhang, C.; Lo, R.; Shen, J.; Ran, Z. Incidence, Prevalence, and Temporal Trends of Microscopic Colitis: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2015, 110, 265–276. [Google Scholar] [CrossRef]
- Miehlke, S.; Guagnozzi, D.; Zabana, Y.; Tontini, G.E.; Kanstrup Fiehn, A.-M.; Wildt, S.; Bohr, J.; Bonderup, O.; Bouma, G.; D’Amato, M.; et al. European Guidelines on Microscopic Colitis: United European Gastroenterology and European Microscopic Colitis Group Statements and Recommendations. United Eur. Gastroenterol. J. 2021, 9, 13–37. [Google Scholar] [CrossRef]
- Agrawal, A.; Khan, M.H.; Whorwell, P.J. Irritable Bowel Syndrome in the Elderly: An Overlooked Problem? Dig. Liver Dis. 2009, 41, 721–724. [Google Scholar] [CrossRef]
- Kurniawan, I.; Kolopaking, M.S. Management of Irritable Bowel Syndrome in the Elderly. Acta Medica Indones. 2014, 46, 138–147. [Google Scholar]
- Zar-Kessler, C.A.M.; Belkind-Gerson, J.; Bender, S.; Kuo, B.M. Treatment of Functional Abdominal Pain With Antidepressants: Benefits, Adverse Effects, and the Gastroenterologist’s Role. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 16–21. [Google Scholar] [CrossRef]
- Ianiro, G.; Eusebi, L.H.; Black, C.J.; Gasbarrini, A.; Cammarota, G.; Ford, A.C. Systematic Review with Meta-Analysis: Efficacy of Faecal Microbiota Transplantation for the Treatment of Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2019, 50, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Pimentel, M.; Brenner, D.M.; Chey, W.D.; Keefer, L.A.; Long, M.D.; Moshiree, B. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. Am. J. Gastroenterol. 2021, 116, 17–44. [Google Scholar] [CrossRef] [PubMed]
- Lucado, J.; Gould, C.; Elixhauser, A. Clostridium Difficile Infections (CDI) in Hospital Stays, 2009. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2006. [Google Scholar]
- Song, J.H.; Kim, Y.S. Recurrent Clostridium Difficile Infection: Risk Factors, Treatment, and Prevention. Gut Liver 2019, 13, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Montalto, M.; Gallo, A.; Agnitelli, M.C.; Pellegrino, S.; Lipari, A.; Pero, E.; Covino, M.; Landi, F.; Gasbarrini, A.; Cammarota, G.; et al. Fecal Microbiota Transplantation for Recurrent Clostridioides difficile Infection in Frail and Very Old Patients. J. Am. Geriatr. Soc. 2023, 71, 3530–3537. [Google Scholar] [CrossRef] [PubMed]
- Minkoff, N.Z.; Aslam, S.; Medina, M.; Tanner-Smith, E.E.; Zackular, J.P.; Acra, S.; Nicholson, M.R.; Imdad, A. Fecal Microbiota Transplantation for the Treatment of Recurrent Clostridioides difficile (Clostridium difficile). Cochrane Database Syst. Rev. 2023, 4, CD013871. [Google Scholar] [CrossRef]
- Elchert, J.A.; Mansoor, E.; Abou-Saleh, M.; Cooper, G.S. The Epidemiology of Whipple’s Disease in the United States between 2012 and 2017: A Population Based National Study. Dig. Dis. Sci. 2019, 64, 1305–1311. [Google Scholar] [CrossRef]
- Cancer (International Agency for Research on Cancer), T.I.A. for R. On Global Cancer Observatory. Available online: https://gco.iarc.fr/ (accessed on 27 November 2023).
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal Cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Mi, M.; Weng, S.; Xu, Z.; Hu, H.; Wang, Y.; Yuan, Y. CSCO Guidelines for Colorectal Cancer Version 2023: Updates and Insights. Chin. J. Cancer Res. 2023, 35, 233–238. [Google Scholar] [CrossRef]
- Extermann, M.; Aapro, M.; Bernabei, R.; Cohen, H.J.; Droz, J.-P.; Lichtman, S.; Mor, V.; Monfardini, S.; Repetto, L.; Sørbye, L.; et al. Use of Comprehensive Geriatric Assessment in Older Cancer Patients: Recommendations from the Task Force on CGA of the International Society of Geriatric Oncology (SIOG). Crit. Rev. Oncol. Hematol. 2005, 55, 241–252. [Google Scholar] [CrossRef]
- Stewart, W.F.; Liberman, J.N.; Sandler, R.S.; Woods, M.S.; Stemhagen, A.; Chee, E.; Lipton, R.B.; Farup, C.E. Epidemiology of Constipation (EPOC) Study in the United States: Relation of Clinical Subtypes to Sociodemographic Features. Am. J. Gastroenterol. 1999, 94, 3530–3540. [Google Scholar] [CrossRef] [PubMed]
- Sandler, R.S.; Jordan, M.C.; Shelton, B.J. Demographic and Dietary Determinants of Constipation in the US Population. Am. J. Public Health 1990, 80, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Choung, R.S.; Locke, G.R.; Schleck, C.D.; Zinsmeister, A.R.; Talley, N.J. Cumulative Incidence of Chronic Constipation: A Population-Based Study 1988–2003. Aliment. Pharmacol. Ther. 2007, 26, 1521–1528. [Google Scholar] [CrossRef] [PubMed]
- Schmulson, M.J.; Drossman, D.A. What Is New in Rome IV. J. Neurogastroenterol. Motil. 2017, 23, 151–163. [Google Scholar] [CrossRef]
- Deb, B.; Prichard, D.O.; Bharucha, A.E. Constipation and Fecal Incontinence in the Elderly. Curr. Gastroenterol. Rep. 2020, 22, 54. [Google Scholar] [CrossRef] [PubMed]
- Vazquez Roque, M.; Bouras, E.P. Epidemiology and Management of Chronic Constipation in Elderly Patients. Clin. Interv. Aging 2015, 10, 919–930. [Google Scholar] [CrossRef]
- Arco, S.; Saldaña, E.; Serra-Prat, M.; Palomera, E.; Ribas, Y.; Font, S.; Clavé, P.; Mundet, L. Functional Constipation in Older Adults: Prevalence, Clinical Symptoms and Subtypes, Association with Frailty, and Impact on Quality of Life. Gerontology 2022, 68, 397–406. [Google Scholar] [CrossRef]
- Hussain, Z.H.; Whitehead, D.A.; Lacy, B.E. Fecal Impaction. Curr. Gastroenterol. Rep. 2014, 16, 404. [Google Scholar] [CrossRef]
- Chughtai, B.; Thomas, D.; Russell, D.; Phongtankuel, V.; Bowles, K.; Prigerson, H. Prevalence and Risk Factors for Fecal Incontinence in Home Hospice. Am. J. Hosp. Palliat. Care 2019, 36, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Townsend, M.K.; Matthews, C.A.; Whitehead, W.E.; Grodstein, F. Risk Factors for Fecal Incontinence in Older Women. Am. J. Gastroenterol. 2013, 108, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Demir, N.; Yuruyen, M.; Atay, K.; Yavuzer, H.; Hatemi, I.; Doventas, A.; Erdincler, D.S.; Dobrucalı, A. Prevalence of Fecal Incontinence and Associated Risk Factors in Elderly Outpatients: A Cross-Sectional Study. Aging Clin. Exp. Res. 2017, 29, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Pérez, I.; Díaz Lantada, A. Surgical Planning of Sacral Nerve Stimulation Procedure in Presence of Sacral Anomalies by Using Personalized Polymeric Prototypes Obtained with Additive Manufacturing Techniques. Polymers 2020, 12, 581. [Google Scholar] [CrossRef] [PubMed]
- Clarke, G.A.; Jacobson, B.C.; Hammett, R.J.; Carr-Locke, D.L. The Indications, Utilization and Safety of Gastrointestinal Endoscopy in an Extremely Elderly Patient Cohort. Endoscopy 2001, 33, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Finkelmeier, F.; Tal, A.; Ajouaou, M.; Filmann, N.; Zeuzem, S.; Waidmann, O.; Albert, J. ERCP in Elderly Patients: Increased Risk of Sedation Adverse Events but Low Frequency of Post-ERCP Pancreatitis. Gastrointest. Endosc. 2015, 82, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Kikendall, J.W. Pill-Induced Esophagitis. Gastroenterol. Hepatol. 2007, 3, 275–276. [Google Scholar]
- Kim, S.H.; Jeong, J.B.; Kim, J.W.; Koh, S.-J.; Kim, B.G.; Lee, K.L.; Chang, M.S.; Im, J.P.; Kang, H.W.; Shin, C.M. Clinical and Endoscopic Characteristics of Drug-Induced Esophagitis. World J. Gastroenterol. 2014, 20, 10994–10999. [Google Scholar] [CrossRef]
- Philip, N.A.; Ahmed, N.; Pitchumoni, C.S. Spectrum of Drug-Induced Chronic Diarrhea. J. Clin. Gastroenterol. 2017, 51, 111–117. [Google Scholar] [CrossRef]
- Talbot, G.H. Small Bowel Histopathologic Findings Suggestive of Celiac Disease in an Asymptomatic Patient Receiving Olmesartan. Mayo Clin. Proc. 2012, 87, 1231–1232, author reply 1232. [Google Scholar] [CrossRef] [PubMed]
- Targownik, L.E.; Fisher, D.A.; Saini, S.D. AGA Clinical Practice Update on De-Prescribing of Proton Pump Inhibitors: Expert Review. Gastroenterology 2022, 162, 1334–1342. [Google Scholar] [CrossRef] [PubMed]
- García Rodríguez, L.A.; Ruigómez, A.; Panés, J. Use of Acid-Suppressing Drugs and the Risk of Bacterial Gastroenteritis. Clin. Gastroenterol. Hepatol. 2007, 5, 1418–1423. [Google Scholar] [CrossRef]
- Dial, S.; Delaney, J.A.C.; Schneider, V.; Suissa, S. Proton Pump Inhibitor Use and Risk of Community-Acquired Clostridium Difficile-Associated Disease Defined by Prescription for Oral Vancomycin Therapy. CMAJ 2006, 175, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Linsky, A.; Gupta, K.; Lawler, E.V.; Fonda, J.R.; Hermos, J.A. Proton Pump Inhibitors and Risk for Recurrent Clostridium Difficile Infection. Arch. Intern. Med. 2010, 170, 772–778. [Google Scholar] [CrossRef]
- Janarthanan, S.; Ditah, I.; Adler, D.G.; Ehrinpreis, M.N. Clostridium Difficile-Associated Diarrhea and Proton Pump Inhibitor Therapy: A Meta-Analysis. Off. J. Am. Coll. Gastroenterol. ACG 2012, 107, 1001. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallo, A.; Pellegrino, S.; Pero, E.; Agnitelli, M.C.; Parlangeli, C.; Landi, F.; Montalto, M. Main Disorders of Gastrointestinal Tract in Older People: An Overview. Gastrointest. Disord. 2024, 6, 313-336. https://doi.org/10.3390/gidisord6010022
Gallo A, Pellegrino S, Pero E, Agnitelli MC, Parlangeli C, Landi F, Montalto M. Main Disorders of Gastrointestinal Tract in Older People: An Overview. Gastrointestinal Disorders. 2024; 6(1):313-336. https://doi.org/10.3390/gidisord6010022
Chicago/Turabian StyleGallo, Antonella, Simona Pellegrino, Erika Pero, Maria Chiara Agnitelli, Caterina Parlangeli, Francesco Landi, and Massimo Montalto. 2024. "Main Disorders of Gastrointestinal Tract in Older People: An Overview" Gastrointestinal Disorders 6, no. 1: 313-336. https://doi.org/10.3390/gidisord6010022