
Bleeding and Perforation Complications after Follow-Up Colonoscopies in Faecal Immunochemical Test-Based Colorectal Cancer Screening: Insights from a Retrospective Case–Control Study
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Study Population
2.2. Rates of Bleeding and Perforation over Time
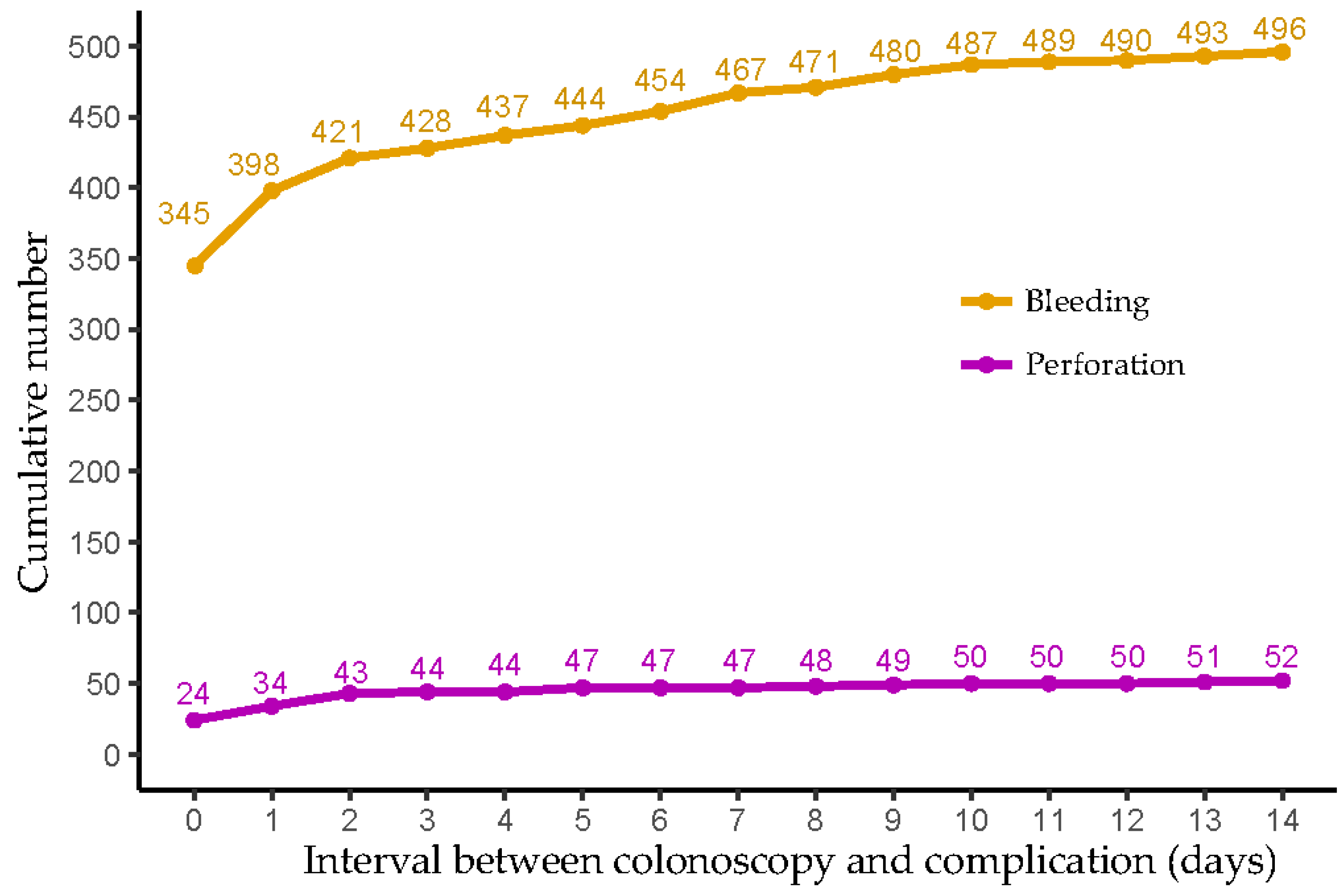
2.3. Time Interval between Index Colonoscopy and Bleeding/Perforation Events
2.4. Factors Associated with the Occurrence of Bleeding and Perforation following Colonoscopies Performed after a Positive Faecal Immunochemical Test
2.4.1. Univariable Analyses
2.4.2. Multivariable Analyses
Bleeding
Perforation
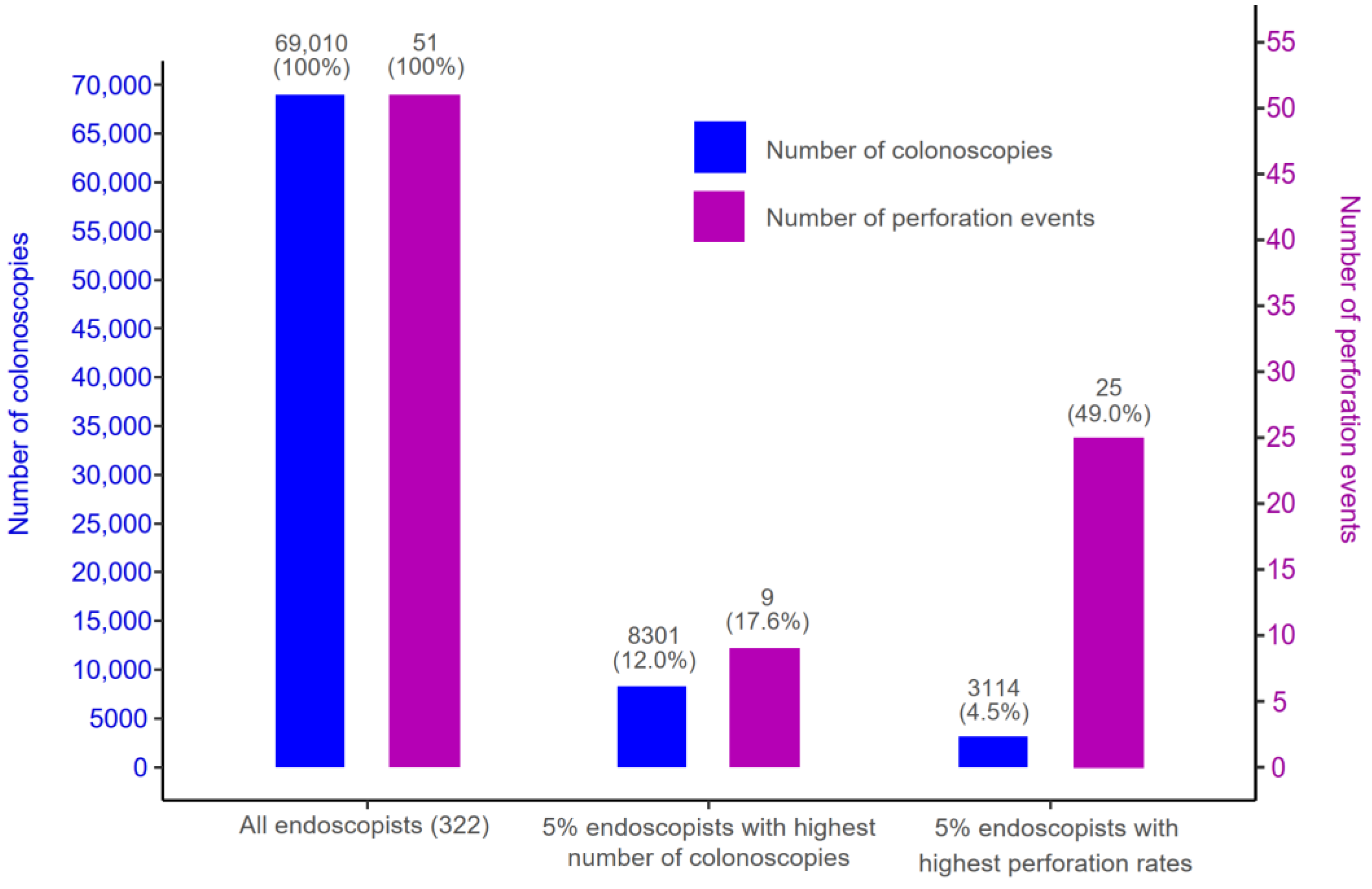
2.5. Endoscopist’s Volume of Colonoscopies Performed after a Positive Faecal Immunochemical Test and Bleeding/Perforation Rates
3. Discussion
3.1. Summary of Main Findings
3.2. Rates of Bleeding and Perforation Align with the Literature
3.3. Declining Bleeding Rates Coupled with Stable Perforation Rates
3.4. Risk Factors of Colonoscopy-Related Bleeding and Perforation Occurrence
3.4.1. Patient Sex and Age
3.4.2. Polypectomy
3.4.3. Anaesthesia
3.4.4. Recent Use of Antiplatelet/Antithrombotic Drugs
3.4.5. Incomplete Colonoscopy
3.4.6. Endoscopist Experience and Specialty
3.5. Issue of the High False Positive Rates of Faecal Immunochemical Tests
3.6. Strengths and Limitations
3.7. Implications of Study Findings
3.7.1. Integrating Information Regarding Colonoscopy Complications into Screening Materials
3.7.2. Strategies Based on Identified Risk Factors to Mitigate Bleeding and Perforation Complications
3.7.3. Further Research to Explore the Subgroup of Endoscopists Who Significantly Contributed to the Recorded Bleeding and Perforation Events
3.7.4. Establishing a Centralised Colonoscopy Register in Belgium
3.8. Generalizability of Study Findings
4. Methods
4.1. The Flemish Colorectal Cancer Screening Programme
4.2. Study Population
Exclusion Criteria
4.3. Study Design
Definitions of Cases and Controls
4.4. Study Variables, Data Collection, and Data Sources
4.5. Statistical Analysis
4.5.1. Population Size
4.5.2. Main Analysis
Descriptive Analysis
Logistic Regression Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khalid, M.; Khalid, M.; Gayam, V.; Yeddi, A.; Adam, O.; Chakraborty, S.; Abdallah, M.; Abu-Heija, A.; Kaloti, Z.; Mukhtar, O.; et al. The Impact of Hospital Teaching Status on Colonoscopy Perforation Risk: A National Inpatient Sample Study. Gastroenterol. Res. 2020, 13, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bronzwaer, M.E.S.; Depla, A.; van Lelyveld, N.; Spanier, B.W.M.; Oosterhout, Y.H.; van Leerdam, M.E.; Spaander, M.C.W.; Dekker, E. Quality assurance of colonoscopy within the Dutch national colorectal cancer screening program. Gastrointest. Endosc. 2019, 89, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Levy, I.; Gralnek, I.M. Complications of diagnostic colonoscopy, upper endoscopy, and enteroscopy. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Benazzato, L.; Zorzi, M.; Antonelli, G.; Guzzinati, S.; Hassan, C.; Fantin, A. Colonoscopy-related adverse events and mortality in an Italian organized colorectal cancer screening program. Endoscopy 2020, 53, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Laanani, M.; Coste, J.; Blotiere, P.O.; Carbonnel, F.; Weill, A. Patient, Procedure, and Endoscopist Risk Factors for Perforation, Bleeding, and Splenic Injury after Colonoscopies. Clin. Gastroenterol. Hepatol. 2019, 17, 719–727.e13. [Google Scholar] [CrossRef] [PubMed]
- Dafnis, G.; Ekbom, A.; Pahlman, L.; Blomqvist, P. Complications of diagnostic and therapeutic colonoscopy within a defined population in Sweden. Gastrointest. Endosc. 2001, 54, 302–309. [Google Scholar] [CrossRef]
- Ko, C.W.; Riffle, S.; Michaels, L.; Morris, C.; Holub, J.; Shapiro, J.A.; Ciol, M.A.; Kimmey, M.B.; Seeff, L.C.; Lieberman, D. Serious complications within 30 days of screening and surveillance colonoscopy are uncommon. Clin. Gastroenterol. Hepatol. 2010, 8, 166–173. [Google Scholar] [CrossRef]
- Levin, T.R.; Zhao, W.; Conell, C.; Seeff, L.C.; Manninen, D.L.; Shapiro, J.A.; Schulman, J. Complications of colonoscopy in an integrated health care delivery system. Ann. Intern. Med. 2006, 145, 880–886. [Google Scholar] [CrossRef]
- Suissa, A.; Bentur, O.S.; Lachter, J.; Yassin, K.; Chermesh, I.; Gralnek, I.; Karban, A.; Khamaysi, I.; Naveh, Y.; Tamir, A.; et al. Outcome and complications of colonoscopy: A prospective multicenter study in northern Israel. Diagn. Ther. Endosc. 2012, 2012, 612542. [Google Scholar] [CrossRef]
- Blotière, P.O.; Weill, A.; Ricordeau, P.; Alla, F.; Allemand, H. Perforations and haemorrhages after colonoscopy in 2010: A study based on comprehensive French health insurance data (SNIIRAM). Clin. Res. Hepatol. Gastroenterol. 2014, 38, 112–117. [Google Scholar] [CrossRef]
- Manta, R.; Tremolaterra, F.; Arezzo, A.; Verra, M.; Galloro, G.; Dioscoridi, L.; Pugliese, F.; Zullo, A.; Mutignani, M.; Bassotti, G. Complications during colonoscopy: Prevention, diagnosis, and management. Tech. Coloproctol. 2015, 19, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Reumkens, A.; Rondagh, E.J.A.; Bakker, M.C.; Winkens, B.; Masclee, A.A.M.; Sanduleanu, S. Post-Colonoscopy Complications: A Systematic Review, Time Trends, and Meta-Analysis of Population-Based Studies. Am. J. Gastroenterol. 2016, 111, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Coser, R.B.; Dalio, M.B.; Martins, L.C.P.; Alvarenga, G.F.; Cruz, C.A.; Imperiale, A.R.; Padovese, C.C.; Paulo, G.A.; Teixeira Junior, J.C. Colonoscopy complications: Experience with 8968 consecutive patients in a single institution. Rev. Col. Bras. Cir. 2018, 45, e1858. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, E.M.; Thomsen, M.K.; Tybjerg, J.; Friis-Hansen, L.; Andersen, B.; Jørgensen, J.C.R.; Baatrup, G.; Njor, S.H.; Mehnert, F.; Rasmussen, M. Colonoscopy-related complications in a nationwide immunochemical fecal occult blood test-based colorectal cancer screening program. Clin. Epidemiol. 2018, 10, 1649–1655. [Google Scholar] [CrossRef] [PubMed]
- Pox, C.P.; Altenhofen, L.; Brenner, H.; Theilmeier, A.; Von Stillfried, D.; Schmiegel, W. Efficacy of a nationwide screening colonoscopy program for colorectal cancer. Gastroenterology 2012, 142, 1460–1467.e2. [Google Scholar] [CrossRef] [PubMed]
- Arora, G.; Mannalithara, A.; Singh, G.; Gerson, L.B.; Triadafilopoulos, G. Risk of perforation from a colonoscopy in adults: A large population-based study. Gastrointest. Endosc. 2009, 69 Pt 2, 654–664. [Google Scholar] [CrossRef]
- Lorenzo-Zúñiga, V.; Moreno de Vega, V.; Doménech, E.; Mañosa, M.; Planas, R.; Boix, J. Endoscopist experience as a risk factor for colonoscopic complications. Color. Dis. 2010, 12, e273–e277. [Google Scholar] [CrossRef]
- Rabeneck, L.; Paszat, L.F.; Hilsden, R.J.; Saskin, R.; Leddin, D.; Grunfeld, E.; Wai, E.; Goldwasser, M.; Sutradhar, R.; Stukel, T.A. Bleeding and Perforation After Outpatient Colonoscopy and Their Risk Factors in Usual Clinical Practice. Gastroenterology 2008, 135, 1899–1906.e1. [Google Scholar] [CrossRef]
- Centre for Cancer Detection. What Are the Possible Outcomes of the Colonoscopy? Available online: https://dikkedarmkanker.bevolkingsonderzoek.be/nl/ddk/wat-zijn-de-mogelijke-resultaten-van-de-coloscopie (accessed on 20 August 2023). (In Dutch).
- Kim, S.Y.; Kim, H.S.; Park, H.J. Adverse events related to colonoscopy: Global trends and future challenges. World J. Gastroenterol. 2019, 25, 190–204. [Google Scholar] [CrossRef]
- Warren, J.L.; Klabunde, C.N.; Mariotto, A.B.; Meekins, A.; Topor, M.; Brown, M.L.; Ransohoff, D.F. Adverse events after outpatient colonoscopy in the Medicare population. Ann. Intern. Med. 2009, 150, 849–857, W152. [Google Scholar] [CrossRef]
- Zwink, N.; Holleczek, B.; Stegmaier, C.; Hoffmeister, M.; Brenner, H. Complication Rates in Colonoscopy Screening for Cancer. Dtsch. Arztebl. Int. 2017, 114, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Saraste, D.; Martling, A.; Nilsson, P.J.; Blom, J.; Tornberg, S.; Hultcrantz, R.; Janson, M. Complications after colonoscopy and surgery in a population-based colorectal cancer screening programme. J. Med. Screen. 2016, 23, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Rex, D.K.; Schoenfeld, P.S.; Cohen, J.; Pike, I.M.; Adler, D.G.; Fennerty, M.B.; Lieb, J.G., 2nd; Park, W.G.; Rizk, M.K.; Sawhney, M.S.; et al. Quality indicators for colonoscopy. Gastrointest. Endosc. 2015, 81, 31–53. [Google Scholar] [CrossRef] [PubMed]
- Rembacken, B.; Hassan, C.; Riemann, J.F.; Chilton, A.; Rutter, M.; Dumonceau, J.M.; Omar, M.; Ponchon, T. Quality in screening colonoscopy: Position statement of the European Society of Gastrointestinal Endoscopy (ESGE). Endoscopy 2012, 44, 957–968. [Google Scholar] [CrossRef] [PubMed]
- Feagins, L.A. Colonoscopy, Polypectomy, and the Risk of Bleeding. Med. Clin. N. Am. 2019, 103, 125–135. [Google Scholar] [CrossRef]
- Muniraj, T.; Sahakian, A.; Ciarleglio, M.M.; Deng, Y.; Aslanian, H.R. Cold snare polypectomy for large sessile colonic polyps: A single-center experience. Gastroenterol. Res. Pract. 2015, 2015, 175959. [Google Scholar] [CrossRef]
- Choksi, N.; Elmunzer, B.J.; Stidham, R.W.; Shuster, D.; Piraka, C. Cold snare piecemeal resection of colonic and duodenal polyps ≥1 cm. Endosc. Int. Open 2015, 3, E508–E513. [Google Scholar] [CrossRef]
- Bielawska, B.; Day, A.G.; Lieberman, D.A.; Hookey, L.C. Risk factors for early colonoscopic perforation include non-gastroenterologist endoscopists: A multivariable analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 85–92. [Google Scholar] [CrossRef]
- Anderloni, A.; Jovani, M.; Hassan, C.; Repici, A. Advances, problems, and complications of polypectomy. Clin. Exp. Gastroenterol. 2014, 7, 285–296. [Google Scholar] [CrossRef]
- Leyden, J.E.; Doherty, G.A.; Hanley, A.; McNamara, D.A.; Shields, C.; Leader, M.; Murray, F.E.; Patchett, S.E.; Harewood, G.C. Quality of colonoscopy performance among gastroenterology and surgical trainees: A need for common training standards for all trainees? Endoscopy 2011, 43, 935–940. [Google Scholar] [CrossRef]
- Turan, A.S.; Pohl, H.; Matsumoto, M.; Lee, B.S.; Aizawa, M.; Desideri, F.; Albeniz, E.; Raju, G.S.; Luba, D.; Barret, M.; et al. The Role of Clips in Preventing Delayed Bleeding after Colorectal Polyp Resection: An Individual Patient Data Meta-Analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 362–371.e23. [Google Scholar] [CrossRef] [PubMed]
- Arana-Arri, E.; Imaz-Ayo, N.; Fernández, M.J.; Idigoras, I.; Bilbao, I.; Bujanda, L.; Bao, F.; Ojembarrena, E.; Gil, I.; Gutiérrez-Ibarluzea, I.; et al. Screening colonoscopy and risk of adverse events among individuals undergoing fecal immunochemical testing in a population-based program: A nested case-control study. United Eur. Gastroenterol. J. 2018, 6, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.O.; Lee, L.N.; Chan, A.C.; Ho, W.N.; Chan, Q.W.; Lau, S.; Chan, J.W. Predictive factors for colonoscopy complications. Hong Kong Med. J. 2015, 21, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Waye, J.D.; Lewis, B.S.; Yessayan, S. Colonoscopy: A prospective report of complications. J. Clin. Gastroenterol. 1992, 15, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Wernli, K.J.; Brenner, A.T.; Rutter, C.M.; Inadomi, J.M. Risks Associated with Anesthesia Services during Colonoscopy. Gastroenterology 2016, 150, 888–894, quiz e818. [Google Scholar] [CrossRef] [PubMed]
- Adeyemo, A.; Bannazadeh, M.; Riggs, T.; Shellnut, J.; Barkel, D.; Wasvary, H. Does sedation type affect colonoscopy perforation rates? Dis. Colon Rectum 2014, 57, 110–114. [Google Scholar] [CrossRef]
- Wernli, K.J.; Inadomi, J.M. Anesthesia for colonoscopy: Too much of a good thing? JAMA Intern. Med. 2013, 173, 556–558. [Google Scholar] [CrossRef]
- Hansen, J.J.; Ulmer, B.J.; Rex, D.K. Technical performance of colonoscopy in patients sedated with nurse-administered propofol. Am. J. Gastroenterol. 2004, 99, 52–56. [Google Scholar] [CrossRef]
- Korman, L.Y.; Haddad, N.G.; Metz, D.C.; Brandt, L.J.; Benjamin, S.B.; Lazerow, S.K.; Miller, H.L.; Mete, M.; Patel, M.; Egorov, V. Effect of propofol anesthesia on force application during colonoscopy. Gastrointest. Endosc. 2014, 79, 657–662. [Google Scholar] [CrossRef]
- Bielawska, B.; Hookey, L.C.; Sutradhar, R.; Whitehead, M.; Xu, J.; Paszat, L.F.; Rabeneck, L.; Tinmouth, J. Anesthesia Assistance in Outpatient Colonoscopy and Risk of Aspiration Pneumonia, Bowel Perforation, and Splenic Injury. Gastroenterology 2018, 154, 77–85.e3. [Google Scholar] [CrossRef]
- Okholm, C.; Hadikhadem, T.; Andersen, L.T.; Donatsky, A.M.; Vilmann, P.; Achiam, M.P. No increased risk of perforation during colonoscopy in patients undergoing Nurse Administered Propofol Sedation. Scand. J. Gastroenterol. 2013, 48, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, T.K.; Hung, L.; Kang, F.C.; Lan, K.M.; Poon, P.W.; So, E.C. Anesthesia does not increase the rate of bowel perforation during colonoscopy: A retrospective study. Acta Anaesthesiol. Taiwan 2009, 47, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Pigò, F.; Bertani, H.; Grande, G.; Abate, F.; Vavassori, S.; Conigliaro, R.L. Post-polypectomy bleeding after colonoscopy on uninterrupted aspirin/non steroideal antiflammatory drugs: Systematic review and meta-analysis. Dig. Liver Dis. 2018, 50, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Vanaclocha-Espi, M.; Ibáñez, J.; Molina-Barceló, A.; Valverde-Roig, M.J.; Pérez, E.; Nolasco, A.; de la Vega, M.; de la Lastra-Bosch, I.D.; Oceja, M.E.; Espinàs, J.A.; et al. Risk factors for severe complications of colonoscopy in screening programs. Prev. Med. 2019, 118, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Telford, J.J.; Abraham, N.S. Management of Antiplatelet and Anticoagulant Agents before and after Polypectomy. Gastrointest. Endosc. Clin. N. Am. 2022, 32, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Abraham, N.S.; Barkun, A.N.; Sauer, B.G.; Douketis, J.; Laine, L.; Noseworthy, P.A.; Telford, J.J.; Leontiadis, G.I. American College of Gastroenterology-Canadian Association of Gastroenterology Clinical Practice Guideline: Management of Anticoagulants and Antiplatelets during Acute Gastrointestinal Bleeding and the Periendoscopic Period. Am. J. Gastroenterol. 2022, 117, 542–558. [Google Scholar] [CrossRef] [PubMed]
- Chan, F.K.L.; Goh, K.L.; Reddy, N.; Fujimoto, K.; Ho, K.Y.; Hokimoto, S.; Jeong, Y.H.; Kitazono, T.; Lee, H.S.; Mahachai, V.; et al. Management of patients on antithrombotic agents undergoing emergency and elective endoscopy: Joint Asian Pacific Association of Gastroenterology (APAGE) and Asian Pacific Society for Digestive Endoscopy (APSDE) practice guidelines. Gut 2018, 67, 405–417. [Google Scholar] [CrossRef]
- ASGE Standards of Practice Committee; Acosta, R.D.; Abraham, N.S.; Chandrasekhara, V.; Chathadi, K.V.; Early, D.S.; Eloubeidi, M.A.; Evans, J.A.; Faulx, A.L.; Fisher, D.A.; et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest. Endosc. 2016, 83, 3–16. [Google Scholar] [CrossRef]
- Veitch, A.M.; Vanbiervliet, G.; Gershlick, A.H.; Boustiere, C.; Baglin, T.P.; Smith, L.A.; Radaelli, F.; Knight, E.; Gralnek, I.M.; Hassan, C.; et al. Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guidelines. Gut 2016, 65, 374–389. [Google Scholar] [CrossRef]
- Singh, H.; Penfold, R.B.; DeCoster, C.; Kaita, L.; Proulx, C.; Taylor, G.; Bernstein, C.N.; Moffatt, M. Colonoscopy and its complications across a Canadian regional health authority. Gastrointest. Endosc. 2009, 69, 665–671. [Google Scholar] [CrossRef]
- Choung, B.S.; Kim, S.H.; Ahn, D.S.; Kwon, D.H.; Koh, K.H.; Sohn, J.Y.; Park, W.S.; Kim, I.H.; Lee, S.O.; Lee, S.T.; et al. Incidence and risk factors of delayed postpolypectomy bleeding: A retrospective cohort study. J. Clin. Gastroenterol. 2014, 48, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Kortlever, T.; van der Vlugt, M.; Dekker, E. Future of Colorectal Cancer Screening: From One-Size-FITs-All to Tailor-Made. Front. Gastroenterol. 2022, 1, 906052. [Google Scholar] [CrossRef]
- Sali, L.; Regge, D. CT colonography for population screening of colorectal cancer: Hints from European trials. Br. J. Radiol. 2016, 89, 20160517. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.; Milà, N.; Binefa, G.; Borràs, J.M.; Espinàs, J.A.; Moreno, V. False-positive results from colorectal cancer screening in Catalonia (Spain), 2000–2010. J. Med. Screen. 2012, 19, 77–82. [Google Scholar] [CrossRef] [PubMed]
- de Haan, M.C.; Pickhardt, P.J.; Stoker, J. CT colonography: Accuracy, acceptance, safety and position in organised population screening. Gut 2015, 64, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Spada, C.; Stoker, J.; Alarcon, O.; Barbaro, F.; Bellini, D.; Bretthauer, M.; De Haan, M.C.; Dumonceau, J.M.; Ferlitsch, M.; Halligan, S.; et al. Clinical indications for computed tomographic colonography: European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Gastrointestinal and Abdominal Radiology (ESGAR) Guideline. Eur. Radiol. 2015, 25, 331–345. [Google Scholar] [CrossRef] [PubMed]
- Berete, F.; Demarest, S.; Charafeddine, R.; Bruyere, O.; Van der Heyden, J. Comparing health insurance data and health interview survey data for ascertaining chronic disease prevalence in Belgium. Arch. Public Health 2020, 78, 120. [Google Scholar] [CrossRef]
- Breekveldt, E.C.H.; Toes-Zoutendijk, E.; de Jonge, L.; Spaander, M.C.W.; Dekker, E.; van Kemenade, F.J.; van Vuuren, A.J.; Ramakers, C.R.B.; Nagtegaal, I.D.; van Leerdam, M.E.; et al. Personalized colorectal cancer screening: Study protocol of a mixed-methods study on the effectiveness of tailored intervals based on prior f-Hb concentration in a fit-based colorectal cancer screening program (PERFECT-FIT). BMC Gastroenterol. 2023, 23, 45. [Google Scholar] [CrossRef]
- Pellat, A.; Deyra, J.; Husson, M.; Benamouzig, R.; Coriat, R.; Chaussade, S. Colorectal cancer screening programme: Is the French faecal immunological test (FIT) threshold optimal? Ther. Adv. Gastroenterol. 2021, 14, 1–8. [Google Scholar] [CrossRef]
- Blom, J.; Lowbeer, C.; Elfstrom, K.M.; Sventelius, M.; Ohman, D.; Saraste, D.; Tornberg, S. Gender-specific cut-offs in colorectal cancer screening with FIT: Increased compliance and equal positivity rate. J. Med. Screen. 2019, 26, 92–97. [Google Scholar] [CrossRef]
- Hoeck, S.; Pringels, S.; Kellen, E.; Van Herck, K.; Martens, P.; Van Limbergen, E.; Francart, J.; Van Hal, G. First results of the Flemish colorectal cancer screening program: Start-up-period late 2013. Acta Gastroenterol. Belg. 2016, 79, 421–428. [Google Scholar] [PubMed]
- Hsu, W.-F.; Chang, C.-Y.; Chang, C.-C.; Chang, L.-C.; Chen, C.-H.; Lin, C.-C.; Lin, Y.-M.; Lee, C.-L.; Wu, H.-Y.; Lee, H.-C.; et al. Risk of colonoscopy-related complications in a fecal immunochemical test-based population colorectal cancer screening program. Endoscopy 2021, 54, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Lallana, M.J.; Feja, C.; Aguilar-Palacio, I.; Malo, S.; Rabanaque, M.J. Use of Non-Steroidal Anti-Inflammatory Drugs and Associated Gastroprotection in a Cohort of Workers. Int. J. Environ. Res. Public Health 2018, 15, 1836. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Number (%) N = 69,723 |
|---|---|---|
| Gender | Women | 29,086 (41.7%) |
| Men | 40,637 (58.3%) | |
| Age at colonoscopy performance | ≤59 | 16,805 (24.1%) |
| 60–64 | 20,417 (29.3%) | |
| 65–69 | 15,195 (21.8%) | |
| ≥70 | 17,306 (24.8%) | |
| Type of colonoscopy | Complete | 68,855 (98.8%) |
| Incomplete | 868 (1.2%) | |
| Endoscopist’s specialty | Gastroenterologist | 68,234 (97.9%) |
| Internist | 1151 (1.7%) | |
| Surgeon | 233 (0.3%) | |
| Other | 105 (0.2%) | |
| Endoscopist’s number of FIT-colonoscopies each year | <20 | 3305 (4.7%) |
| 20–39 | 12,901 (18.5%) | |
| 40–59 | 18,855 (27.0%) | |
| 60–79 | 15,933 (22.9%) | |
| 80–99 | 10,046 (14.4%) | |
| 100–119 | 5051 (7.2%) | |
| 120–139 | 2444 (3.5%) | |
| ≥140 | 1188 (1.7%) | |
| Presence of polypectomy | No | 28,333 (40.6%) |
| Yes | 41,390 (59.4%) | |
| Type of anaesthesia | No registration of anaesthesia | 9548 (13.7%) |
| General anaesthesia | 38,970 (55.9%) | |
| Conscious sedation | 17,980 (25.8%) | |
| Anaesthesia of unknown type | 3225 (4.6%) | |
| Recent use of systemic corticosteroids | No | 65,645 (94.2%) |
| Yes | 4078 (5.9%) | |
| Recent use of antiplatelet/antithrombotic drugs | No | 45,075 (64.7%) |
| Yes | 24,648 (35.4%) | |
| FIT result (ng Hb/mL): median (IQR) | 207 (117, 509.5) | |
| Lesion location | No lesion | 19,315 (27.7%) |
| Left colon | 16,007 (23.0%) | |
| Right colon | 8672 (12.4%) | |
| Rectum | 5464 (7.8%) | |
| Other † | 20,265 (29.1%) |
| Variable | p-Value of Likelihood Ratio Test | |
|---|---|---|
| Bleeding | Perforation | |
| Gender | <0.01 * | 0.93 |
| Age | <0.01 * | 0.60 |
| Type of colonoscopy | 0.96 | <0.01 * |
| Endoscopist’s specialty | <0.01 * | 0.29 |
| Endoscopist’s number of FIT-colonoscopies performed annually | <0.01 * | 0.57 |
| Presence of polypectomy | <0.01 * | 0.04 * |
| Type of anaesthesia | <0.01 * | 0.02 * |
| Recent use of systemic corticosteroids | 0.84 | 0.59 |
| Recent use of antiplatelet/antithrombotic drugs | 0.12 * | <0.01 * |
| FIT result | 0.58 | 0.95 |
| Lesion location | <0.01 * | 0.10 * |
| Variable | Category | No Bleeding (%) N = 68,889 | Bleeding (%) N = 496 | aOR ‡ (95% CI) | p-Value |
|---|---|---|---|---|---|
| Gender | Women | 28,819 (41.8%) | 132 (26.6%) | Ref | |
| Men | 40,070 (58.2%) | 364 (73.4%) | 1.46 [1.19–1.78] | <0.001 * | |
| Age at colonoscopy performance | ≤59 | 16,651 (24.2%) | 89 (17.9%) | Ref | |
| 60–64 | 20,179 (29.3%) | 141 (28.4%) | 0.96 [0.73–1.26] | 0.764 | |
| 65–69 | 15,014 (21.8%) | 110 (22.2%) | 1.01 [0.76–1.35] | 0.2928 | |
| ≥70 | 17,045 (24.7%) | 156 (31.5%) | 1.13 [0.86–1.48] | 0.384 | |
| Endoscopist’s specialty | Gastroenterologist | 67,740 (98.3%) | 494 (99.6%) | Ref | |
| Internist | 1149 (1.7%) | 2 (0.4%) | 0.67 [0.16–2.74] | 0.574 | |
| Endoscopist’s number of FIT-colonoscopies annually | 20–39 | 12,634 (18.3%) | 112 (22.6%) | Ref | |
| <20 | 3111 (4.5%) | 11 (2.2%) | 0.46 [0.24–0.85] | 0.013 * | |
| 40–59 | 18,732 (27.2%) | 123 (24.8%) | 0.69 [0.53–0.89] | 0.005 * | |
| 60–79 | 15,808 (22.9%) | 125 (25.2%) | 0.87 [0.67–1.13] | 0.297 | |
| 80–99 | 9980 (14.5%) | 66 (13.3%) | 0.75 [0.55–1.01] | 0.062 | |
| 100–119 | 5023 (7.3%) | 28 (5.6%) | 0.60 [0.40–0.92] | 0.019 * | |
| 120–139 | 2430 (3.5%) | 14 (2.8%) | 0.55 [0.31–0.96] | 0.037 * | |
| ≥140 | 1171 (1.7%) | 17 (3.4%) | 1.42 [0.84–2.41] | 0.189 | |
| Presence of polypectomy | No | 28,005 (40.7%) | 32 (6.5%) | Ref | |
| Yes | 40,884 (59.3%) | 464 (93.5%) | 2.73 [1.83–4.09] | <0.001 * | |
| Type of anaesthesia | No registration of anaesthesia | 9422 (13.7%) | 43 (8.7%) | Ref | |
| General anaesthesia | 38,458 (55.8%) | 328 (66.1%) | 1.80 [1.30–2.48] | <0.001 * | |
| Conscious sedation | 17,841 (25.9%) | 88 (17.7%) | 1.23 [0.85–1.77] | 0.282 | |
| Anaesthesia of unknown type | 3168 (4.6%) | 37 (7.5%) | 2.26 [1.44–3.54] | <0.001 * | |
| Recent use of antiplatelet/antithrombotic drugs | No | 44,546 (64.7%) | 304 (61.3%) | Ref | |
| Yes | 24,343 (35.3%) | 192 (38.7%) | 1.22 [1.02–1.48] | 0.031 * | |
| Lesion location | No lesion | 19,211 (27.9%) | 7 (1.4%) | Ref | |
| Left colon | 15,794 (22.9%) | 169 (34.1%) | 1.58 [0.40–6.22] | 0.513 | |
| Right colon | 8529 (12.4%) | 101 (20.4%) | 2.26 [0.57–8.91] | 0.243 | |
| Rectum | 5381 (7.8%) | 46 (9.3%) | 1.42 [0.35–5.70] | 0.624 | |
| Other † | 19,974 (29.0%) | 173 (34.9%) | 2.04 [0.52–7.95] | 0.305 |
| Variable | Category | No Perforation (%) (N = 69,333) | Perforation (%) (N = 52) | aOR ‡ (95% CI) | p-Value |
|---|---|---|---|---|---|
| Type of colonoscopy | Complete | 68,519 (98.8%) | 45 (86.5%) | Ref | |
| Incomplete | 814 (1.2%) | 7 (13.5%) | 43.93 [15.40–131.09] | <0.001 * | |
| Presence of polypectomy | No | 28,023 (40.4%) | 14 (26.9%) | Ref | |
| Yes | 41,310 (59.6%) | 38 (73.1%) | 3.06 [1.18–7.93] | 0.021 * | |
| Type of anaesthesia | No registration of anaesthesia | 9463 (13.6%) | 2 (3.8%) | Ref | |
| General anaesthesia | 38,747 (55.9%) | 39 (55.9%) | 7.58 [1.75–32.82] | 0.007 * | |
| Conscious sedation | 17,920 (25.8%) | 9 (25.8%) | 3.98 [0.83–19.10] | 0.084 | |
| Anaesthesia of unknown type | 3203 (4.6%) | 2 (3.8%) | 4.43 [0.61–32.42] | 0.143 | |
| Recent use of antiplatelet/antithrombotic drugs | No | 44,832 (64.7%) | 18 (34.6%) | Ref | |
| Yes | 24,501 (35.3%) | 34 (65.4%) | 3.59 [2.02–6.36] | <0.001 * | |
| Lesion location | No lesion | 19,210 (27.7%) | 8 (15.4%) | Ref | |
| Left colon | 15,945 (23.0%) | 18 (34.6%) | 1.41 [0.52–3.83] | 0.500 | |
| Right colon | 8621 (12.4%) | 9 (17.3%) | 1.53 [0.50–4.68] | 0.459 | |
| Rectum | 5422 (7.8%) | 5 (9.6%) | 1.28 [0.37–4.42] | 0.693 | |
| Other † | 20,135 (29.0%) | 12 (23.1%) | 0.95 [0.33–2.77] | 0.926 |
| Variable | Data Source | Definition |
|---|---|---|
| Outcomes | ||
| Bleeding | Insurance Intermutualistic Agency | Registration of nomenclature code(s) referring to the management of bleeding within 14 days after the index colonoscopy (see Supplementary Table S3) |
| Perforation | Insurance Intermutualistic Agency | Registration of nomenclature code(s) referring to the management of perforation within 14 days after the index colonoscopy (see Supplementary Table S3) |
| Determinants of interest | ||
| Age (at year of colonoscopy) | Belgian Cancer Registry | Individual’s age (continuous) |
| Gender | Belgian Cancer Registry | Individual’s gender: men/women |
| Type of colonoscopy | Belgian Cancer Registry (originally Insurance Intermutualistic Agency nomenclature codes) |
|
| Anaesthesia | Insurance Intermutualistic Agency | Registration of nomenclature code(s) referring to anaesthesia procedure (see Supplementary Table S4) and/or registration of medications used in anaesthesia on the same day as the index colonoscopy:
|
| Polypectomy | Insurance Intermutualistic Agency | Registration of nomenclature code(s) referring to the performance of polypectomy on the same day as the index colonoscopy (see Supplementary Table S5). |
| Endoscopist’s specialty | Belgian Cancer Registry | Gastroenterologist Internist Surgeon Other |
| Endoscopist’s number of FIT-colonoscopies each year | Belgian Cancer Registry | Number of FIT-colonoscopies performed by an endoscopist in year of index colonoscopy |
| Use of antiplatelet/antithrombotic drugs shortly before or after the index colonoscopy | Insurance Intermutualistic Agency | Antiplatelet/antithrombotic drugs include antiplatelets, non-steroidal anti-inflammatory drugs, anticoagulants, thrombolytics and other antithrombotic agents (see Supplementary Table S6). Definition of ‘shortly before or after the index colonoscopy’ [64]:
|
| Use of systemic corticosteroids shortly before or after the index colonoscopy | Insurance Intermutualistic Agency | Systemic corticosteroids include beclomethasone, betamethasone, budesonide, dexamethasone, hydrocortisone, methylprednisolone, triamcinolone, fluticasone, and prednisone. Definition of ‘shortly before or after the index colonoscopy’ [64]:
|
| FIT result | Belgian Cancer Registry (originally Centre for Cancer Detection) | The quantitative result of FIT before colonoscopy (ng Hb/mL) |
| Lesion location | Belgian Cancer Registry | Right colon Left colon Rectum Anal region Overlap Unspecified No lesion |
| Additional variables for adjustment | ||
| Year of colonoscopy | Belgian Cancer Registry | 2013–2019 |
| Lesion type | Belgian Cancer Registry | No lesion Lesions other than cancer/adenoma (polyp not further specified, polyposis coli, low grade dysplasia, or benign tumour) Adenoma without villous component Adenoma with villous component In situ cancer Invasive cancer, stage I Invasive cancer, stage II Invasive cancer, stage III Invasive cancer, stage IV Invasive cancer, unknown stage |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, T.N.; Bouchat, J.; Peeters, M.; Berghmans, B.; Van Cutsem, E.; Van Hal, G.; Van Herck, K.; Hoeck, S. Bleeding and Perforation Complications after Follow-Up Colonoscopies in Faecal Immunochemical Test-Based Colorectal Cancer Screening: Insights from a Retrospective Case–Control Study. Gastrointest. Disord. 2024, 6, 26-48. https://doi.org/10.3390/gidisord6010003
Tran TN, Bouchat J, Peeters M, Berghmans B, Van Cutsem E, Van Hal G, Van Herck K, Hoeck S. Bleeding and Perforation Complications after Follow-Up Colonoscopies in Faecal Immunochemical Test-Based Colorectal Cancer Screening: Insights from a Retrospective Case–Control Study. Gastrointestinal Disorders. 2024; 6(1):26-48. https://doi.org/10.3390/gidisord6010003
Chicago/Turabian StyleTran, Thuy Ngan, Joanna Bouchat, Marc Peeters, Bea Berghmans, Eric Van Cutsem, Guido Van Hal, Koen Van Herck, and Sarah Hoeck. 2024. "Bleeding and Perforation Complications after Follow-Up Colonoscopies in Faecal Immunochemical Test-Based Colorectal Cancer Screening: Insights from a Retrospective Case–Control Study" Gastrointestinal Disorders 6, no. 1: 26-48. https://doi.org/10.3390/gidisord6010003