
Probiotic Interventions in Coeliac Disease: A Systematic Review with a Focus on Cardiovascular Risk
 , , , and
, , , and 
Abstract
:1. Introduction
2. Results
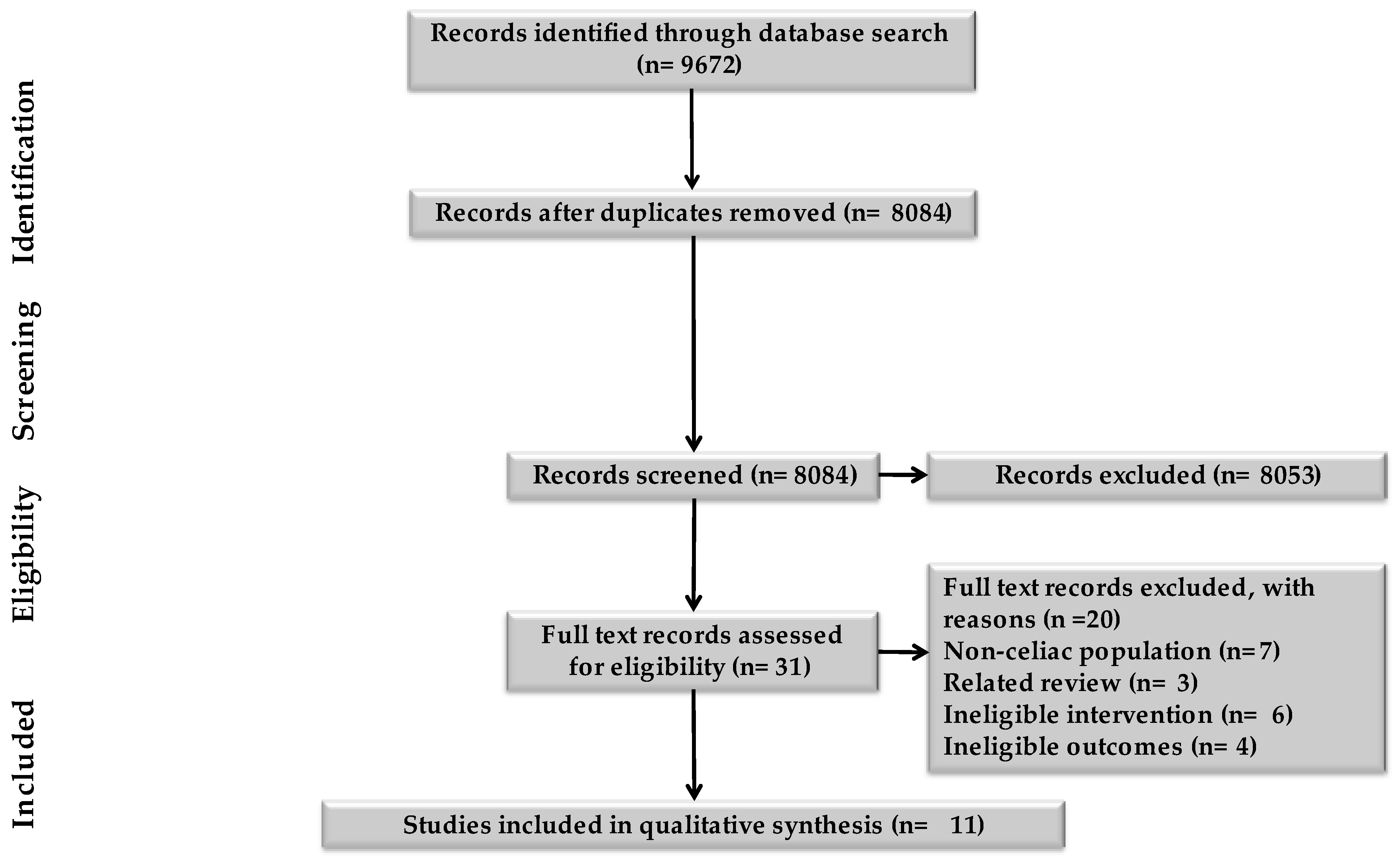
2.1. Characteristics of Studies
2.2. Risk of Bias Assessment

{kind=link}
| Randomisation Process | Deviations from Intended Intervention | Missing Outcome Data | Measurement of Outcome Gastro Symptoms | Measurement of Outcome Inflammation | Selection of Reported Results | Overall | |
|---|---|---|---|---|---|---|---|
| Smecuol et al., 2013 [27] | Some concerns | ||||||
| Olivares et al., 2014 [28] | Some Concerns | ||||||
| Klemenak et al., 2015 [29] | Not measured | Low risk of bias | |||||
| Harnett et al., 2016 [30] | Not measured | Not measured | Low risk of bias | ||||
| Quagliariello et al., 2016 [31] | Not measured | Not measured | Low risk of bias | ||||
| Primec et al., 2019 [34] | Not measured | Not measured | Low risk of bias | ||||
| Francavilla et al., 2019 [35] | Not measured | Low risk of bias | |||||
| Smecuol et al., 2020 [36] | Not measured | Some concerns | |||||
| Ali et al., 2022 [37] | Not measured | High risk of bias |
| Non RCTs | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall |
|---|---|---|---|---|---|---|---|---|
| Pinto-Sanchez et al., 2016 [32] | High risk of bias | |||||||
| Martinello et al., 2017 [33] | High risk of bias |
2.3. Impact of Probiotic Intervention on Outcomes
| Author Year Country Study Design | Sample Size | Population Characteristics | Interventions (Probiotic and Placebo) | Follow Up Duration | Outcomes |
|---|---|---|---|---|---|
| Smecuol et al., 2013 [27] Argentina DBRCT | Probiotic: 12 Placebo: 10 | M/F: 4/18 Probiotic: Age 46 (29–62) years Placebo: Age 40 (20–71) years Dx: active CD, on gluten containing diet before GFD. No other active chronic gastrointestinal pathologies No additional diagnosis. Blood and urine sample analysed. | B. infantis NLS super strain (2 × 109 Colony-Forming Units) vs. Placebo, 3 times per day, 15 min before meals 5 g of lactulose and 2 g of Mannitol in 450 mL of water for fractional excretion ratio | 2-week run -in, 3-week treatment, 50-day f/u to initiate GFD | Quality of life: None reported. Gastro Symptoms: bloating and abdominal distention (20/22), abdominal pain (19/22), diarrhoea (11/22) for both groups Markers of active disease: Probiotics: Reduction in serum antibody concentrations (10% for IgA tTG and IgA DGP antibodies) Placebo: Increased antibody serum concentrations (IgA tTG, 7% and IgA DGP, 10%) at the end of the trial. Biochemical and microbial data: Primary endpoint: Non-significant increase of mean lactulose/mannitol ratio from baseline for the probiotic (p = 0.064) and placebo (p = 0.342) and Secondary endpoint: Probiotic: significant reduction in indigestion (p = 0.0035) and constipation (p = 0.0483) symptoms, however, borderline for reflux symptoms (p = 0.0586). Placebo: No significant changes in any syndrome (indigestion, diarrhoea, constipation, abdominal pain). Significant improvement in diarrhoea symptoms Outcome of inflammatory mediators: Probiotic and placebo: No significant changes in Th1 serum cytokines and serum chemokines. Significant increase in high baseline serum concentration of MIP-1β, (p < 0.04), but not in the placebo group. Cardiovascular risk factors: None reported. |
| Olivares et al., 2014 [32] Spain DBRCT | Probiotics: 17 Placebo: 16 | Probiotic: Age 6.8 ± 0.9 years M/F (7/10) Placebo: Age 8.5 ± 1.2 years M/F (8/8) Dx: biopsy newly diagnosed CD. Adherence to GFD after diagnosis confirmation. Food records for 72 h (2 weekdays, 1 weekend day) before start and after 3 mnths intervention. No additional diagnosis. Blood and faecal sample analysed; DNA sequencing with QIAamp DNA stool Mini Kit and Real time PCR to quantify content of bacterial groups. | Bifidobacterium longum CECT 7347 (109 CFU) vs. Placebo At lunch time | 3 months | Quality of life: Not reported. Gastro Symptoms: Self-reported improvements in diarrhoea, constipation, abdominal pain, and vomiting. No significant changes in both groups for energy intake other specific nutrients (p > 0.05). GFD adherence led to slight decrease in dietary fibre. Probiotic: higher mean increment in weight and height percentiles than in the placebo group. Markers of active disease: Probiotic: Decreases in CD3+ (p = 0.013) and HLA-DR+ (p = 0.029) T cell populations but no significant changes in placebo. No significant differences seen in T lymphocytes HLA-DR+, CD4+, CD4+Foxp3+ and CD8+ for both groups (p = 0.328, p = 0.970, p = 0.504 and p = 0.376). Biochemical and microbial data: Slight reduction in serum TNF-α for probiotic group (p = 0.067); but difference between both groups was not significant (p = 0.085). No significant differences found in both groups for serum IL-10, interferon-y, IL-13, transforming growth factor-β1, IgG1 and IgG4. Placebo: Significant increase in gene copy Bacteroides fragilis group (p = 0.013), Enterobacteriaceae (p = 0.038), non-significant decrease in Bifidobacterium spp. (p = 0.151). Probiotic: No significant differences in Lactobacillus group, Bifidobacterium spp./B. fragilis group and Enterobacteriaceae. Significant decrease in faecal sIgA concentration Cardiovascular risk factors: None reported. |
| Slovenia RCT 3 publications | |||||
| Klemenak et al., 2015 [33] Slovenia DBRCT | 49 patients Placebo: 24 Probiotic: 22 HC: 18 | Placebo: Age 10.81 ± 5.0 years, M/F (10/14) Time on GFD 7.1 ± 5.5 years, Compliance on GFD (80%) Probiotic: Age 10.4 ± 4.2 years M/F (6/16) Time on GFD 5.6 ± 3.7 years, HC: Age 8.8 ± 6.0 years M/F (7/11) Dx: biopsy On GFD from 0.5 to 15 years. No additional diagnosis. Compliance on GFD (91%) in probiotic group and 80% in placebo Blood sample analysed. | Lyophilized 50% B. breve BR03 (109 CFU) and 50% B. breve B632 (109 CFU) vs. Placebo Daily at breakfast | 3 months; 3 months f/u | Quality of life: None reported. Gastro Symptoms: None reported. Markers of active disease: None reported. Biochemical and microbial data: TNF-α in serum at baseline, significantly higher (p = 0.015) in the probiotic group (14.78 ± 6.43) than placebo group (10.58 ± 3.57). TNF-α in serum at the end of the study, significant decrease (p = 0.020) in the probiotic group (11.97 ± 3.58) from baseline levels. TNF-α in serum on f/u, significantly higher in the probiotic group No correlation between positive serologic markers of CD and levels of TNF-α and IL-10 in individual patient with CD. Values for cytokine IL-10 in serum, below assay detection limit (5 pg/mL) and so not analysed. Cardiovascular risk factors: None reported. |
| Quagliariello et al., 2016 [35] Slovenia DBRCT | Probiotic: 20 Placebo: 20 HC: 16 | Age 1–19 years Dx: biopsy On GFD for at least 3 months. No additional diagnosis. Faecal sample analysed; DNA extraction and sequencing with QIAamp DNA stool Mini Kit and molecular analyses; absolute quantification using Quantitative PCR. | B. breve BR03 (DSM 16604) (109 CFU) and B. breve B632 (DSM 24706) (1:1) (109 CFU) vs. Placebo daily at breakfast | 3 months | Quality of life: None reported. Gastro Symptoms: None reported. Markers of active disease: None reported. Biochemical and microbial data: Metagenomic analysis; 6 phyla revealed after sequencing (5 Bacteria and 1 Archaea). Firmicutes, high in control group (60–70%) and 50–60% in probiotic group. Bacteriodetes 20–40% in CD group, 10–20% in control group. Proteobacteria and Verrucomicrobia high in the placebo group. Statistically, Actinobacteria was low in CD group but increased after probiotic intake. Euryarchaeota, the only Archaea was found predominately in the control group. Cardiovascular risk factors: None reported. |
| Primec et al., 2019 [38] Slovenia DBRCT | Probiotic: 20 Placebo: 19 HC: 14 | Probiotic: Age 9.2 ± 4.4 yeras Male 20% Placebo: Age 10.5 ± 5.1 years Male 31% HC: Age 10.1 ± 6.0 years Male 36% Dx: biopsy On GFD from 6 months to 15 years. No additional diagnosis. Blood and faecal sample analysed; DNA extraction and sequencing with QIAamp DNA stool Mini Kit and molecular analyses; absolute quantification using Quantitative PCR. | B. breve 72 BR03 (DSM 16604) (2 × 109 CFU) and B. breve B632 (DSM 24706) (2 × 109 CFU) vs. Placebo Daily at breakfast | 3 months; 3 months follow-up | Quality of life: None reported. Gastro Symptoms: None reported. Markers of active disease: None reported. Biochemical and microbial data: In the probiotic and placebo group, TNF-α had a similar level as the healthy children. In CD patients, TNF-α had positive correlation with Verrucomicrobia and negative one with Parcubacteria. There was a high statistical significance between TNF-α and unclassified Bacteria group and positive correlation with TNF- alpha and unclassified Archaea. In CD patients, Proteobacteria correlated positively with acetic and propionic acid (p = 0.452, p = 0.004 and p = 0.331, p = 0.045, respectively), which led to Proteobacteria and total SCFAs (p = 0.380. p = 0.017). Euryarchaeota phylum had a positive correlation (p = 0.351, p = 0.029) to acetic acid. In Healthy Children, TNF-alpha had a negative association with Firmicutes (p = 0.660, p = 0.010) and negative correlation to Euryarchaeota (p = 0.654, p = 0.011). Cardiovascular risk factors: None reported. |
| Harnett et al., 2016 [34] Australia DBRCT | Probiotics: 21 Placebo: 21 | Probiotic: Age 47.1 ± 16.1 years M/F (3/18) Placebo: Age 47.5 ± 12.9 years M/F (4/17) Dx: biopsy On GFD for at least 12 months and with persistent symptoms GFD Adherence: the three-day diet diary Compliance was 95.2% No additional diagnosis. Duodenal biopsy, blood and faecal samples analysed; DNA and PCR analysis. | VSL #3 blend of probiotic bacteria vs. Placebo sachet orally with water/juice at breakfast and super | 12-week treatment | Quality of life: Assessed with the CDQ. 2 participants on the placebo and 2 participants on probiotic reported mild bloating. Partial improvement due to GFD, 100% of participants. However, residual gastrointestinal symptoms (mild to moderate) and fatigue were reported by all. Gastro Symptoms: None reported. Markers of active disease: 1 probiotic and 1 placebo participant had persistent villous atrophy. Biochemical and microbial data: Descriptive statistics for the predominant bacteria showed that only Streptomyces spp. (p = 0.058) was different between the two groups at baseline and 12 weeks and Mycoplasma sp. (p = 0.026), 12 weeks only. Bifidobacteria (p = 0.001) reduced significantly, and Escherichia coli (p = 0.005) increased over time. Cardiovascular risk factors: None reported. |
| Francavilla et al., 2019 [39] Italy DBRCT | Probiotics: 54 Placebo: 55 | Probiotic: Age 43.3 (18.8–62.2) years Male 11% Placebo: Age: 44.6 (19.3–63.4) years Male: 16% Dx: biopsy on GFD > 2 years Persistent symptoms [IBS Severity Score System >75] Duration of GFD: Probiotic, 6.8 (2.6–16.7) years Placebo, 7.4 (3.5–17.5) years Additional Diagnosis: IBS Faecal sample analysed; DNA extraction with FastDNA Spin kit for soil, RNA extraction with stool total RNA purification kit. | Mixture of: Lactobacillus casei LMG 101/37 P-17504 (5 × 109 CFU), Lactobacillus plantarum CECT 4528 (5 × 109 CFU), Bifidobacterium animalis subsp. lactis Bi1 LMG P-17502 (10 × 109 CFU), Bifidobacterium breve Bbr8 LMG P-17501 (10 × 109 CFU), B. breve Bl10 LMG P-17500 (10 × 109 CFU) vs. Placebo sachet Daily | 2-week run-in; 6-week treatment; 6-week follow-up | Quality of life: Irritable bowel syndrome quality of life scores was not different in both probiotic and placebo groups. Gastro Symptoms: GI symptoms reduced. Gastrointestinal symptom rating scale: Probiotic, 12.2 ± 5.5 and Placebo, 16.7 ± 6.7, reduced significantly for both groups from baseline. At the end of follow up Probiotic, 10.1 ± 4.1 Placebo 9.6 ± 4.2. Markers of active disease: TTG-IgA (IU/mL): Probiotic, 0.8 (0–1.2); Placebo, 0.5 (0.2.1) Biochemical and microbial data: Probiotics: significant increased levels of presumptive lactic acid bacteria (Lactobacillus, Lactococcus, and Streptococcus) Bifidobacterium spp. and Staphylococcus spp. Higher levels of Bifidobacterium spp. after 6 weeks. Placebo: No statical differences found in cultivable microbes. No statistical differences found between both groups for total bacterial community richness. Cardiovascular risk factors: None reported. |
| Smecuol et al., 2020 [40] Argentina DBRCT | Probiotic: 7 Placebo: 5 | Probiotic: Male 0% Placebo: Male 20% Age 53 (43–57) years Dx: biopsy On GFD for >2 years No additional diagnosis. Blood and faecal sample analysed; Faecal total DNA extracted and sequenced. | B. infantis NLS-SS (4 × 109 CFU) vs. Placebo Daily | One week run in 3 weeks treatment 2 weeks washout 3 weeks switched treatment | Quality of life: None reported. Gastro Symptoms: Two patients in the probiotic group had gluten indigestion. Markers of active disease: No significant changes in the coeliac symptom index when comparing probiotic and placebo groups. Biochemical and microbial data: Significant improvement in CD symptom in probiotic group compared to highly symptomatic placebo group, p = 0.046. No difference between both groups with positive and negative serology. No significant differences in both groups for gluten immunogenic peptide excretion. Probiotic group had decreased levels of Ruminococcus spp. and Bifidobacterium adolescentis. Cardiovascular risk factors: None reported. |
| Ali et al., 2022 [41] Pakistan Randomized clinical trial, descriptive cross-sectional study. | Probiotic: 85 No medication: 85 | Age 8–10 years Dx: CD from intestinal biopsy. No additional diagnosis. Stool frequency analysed. | Clostridium butyricum and Bifidobacterium spp. in 75–100 mL of boiled water twice daily. | 28 days | Quality of life: None reported. Gastro Symptoms: Significant reduction in frequency of stools per day. Markers of active disease: None reported. Biochemical and microbial data: None reported. Cardiovascular risk factors: None reported. |
| Author Year Country Study Design | Sample Size | Population Characteristics | Interventions (Probiotic and Placebo) | Follow Up Duration | Outcomes |
|---|---|---|---|---|---|
| Pinto-Sanchez et al., 2016 [36] Argentina Clinical trial with external controls | Active CD with probiotic: 12 Active CD without probiotic: 24. Control CD on 1 y GFD: 5 | CD Active on probiotics: Age 41 (22–53) years Female n (%): 8 (67) CD Active no treatment: Age 40 (29–54) years Female n (%): 23 (95.8) CD on GFD: Age 35 (31–45) years Female n (%): 4 (80) Dx: biopsy Active cases No additional diagnosis. Duodenal biopsy analysed. | Bifdobacterium infantis NSL-SS | 3 weeks | Quality of life: None reported. Gastro Symptoms: None reported. Markers of active disease: None reported. Biochemical and microbial data: The probiotic reduced the Paneth cells (PC) counts without the GFD. However, decreased macrophage counts (p = 0.02) were seen after 1 y GFD as well as further decreased in patients treated with the probiotic only. Similarly, the expression of mucosal HD-5 was significantly decreased in the probiotic group but not in 1 y GFD (p < 0.001). IgA TG: Active CD without probiotic 129 (104–200), Active CD with probiotic 200 (192–216), CD on 1 y GFD 8 (4–17) IgA DGP: Active CD without probiotic 200 (120–300), Active CD with probiotic 152 (64–300), CD on 1 y GFD 7 (4–18) Cardiovascular risk factors: None reported. |
| Martinello et al., 2017 [37] Brazil Non-randomized clinical trial | CD: 14 HC: 17 | CD: Age 18–60 years 10/4 (F/M) HC: Age 18–85 years years 10/7 (F/M) Dx: biopsy On GFD and asymptomatic No additional diagnosis. Faecal sample analysed; for bifidobacteria content and faecal pH. | 108 CFU of Lactobacillus acidophilus and Bifdobacterium lactis as 100 g of yogurt per day. the average concentration of bifidobacteria was 6.67 × 108 ± 10.3 × 108 CFU/g of yoghurt. | 30 days | Quality of life: None reported. Gastro Symptoms: None reported. Markers of active disease: None reported. Biochemical and microbial data: Healthy individuals presented a significantly higher concentration of bifidobacteria (2.3 × 108 ± 6.3 × 107 CFU/g) before the probiotic-containing yogurt intake when compared to the celiac group (1.0 × 107 ± 1.7 × 107 CFU/g) Celiac patients presented, in average, 83% less bifidobacteria than healthy individuals. Still, celiac faecal pH (7.19 ± 0.521) was not significantly different from the faecal pH of the control group (7.18 ± 0.522). Healthy individuals presented a significantly higher bifidobacteria concentration (14.7 × 108 ± 0.2 × 108 CFU/g) than celiac patients (0.76 × 108 ± 0.1 × 108 CFU/g). However, faecal pH of celiac patients (7.28 ± 0.518) did not show significant difference from the faecal pH of healthy individuals (7.07 ± 0.570) after the yogurt intake. Cardiovascular risk factors: None reported. |
3. Discussion
4. Methods
4.1. Inclusion and Exclusion
4.2. Type of Studies
4.3. Search Terms
4.4. Selection of Studies
4.5. Data Synthesis Strategy
4.6. Risk of Bias Assessment
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global prevalence of celiac disease: Systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Coeliac Disease Quality Standard. 2016. Available online: www.Nice.Org.Uk/guidance/qs134 (accessed on 1 October 2023).
- Muhammad, H.; Reeves, S.; Jeanes, Y.M. Identifying and improving adherence to the gluten-free diet in people with coeliac disease. Proc. Nut. Soc. 2019, 78, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, L.; Nardelli, C. Gut microbiome investigation in celiac disease: From methods to its pathogenetic role. Clin. Chem. Lab. Med. 2020, 58, 340–349. [Google Scholar] [CrossRef] [PubMed]
- De Palma, G.; Nadal, I.; Collado, M.C.; Sanz, Y. Effects of a gluten-free diet on gut microbiota and immune function in healthy adult human subjects. Br. J. Nutr. 2009, 102, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Cristofori, F.; Indrio, F.; Miniello, V.L.; Angelis, M.D.; Francavilla, R. Probiotics in celiac disease. Nutrients 2018, 10, 1824. [Google Scholar] [CrossRef]
- Naseri, K.; Saadati, S.; Ghaemi, F.; Ashtary-Larky, D.; Asbaghi, O.; Sadeghi, A.; Afrisham, R.; de Courten, B. The effects of probiotic and synbiotic supplementation on inflammation, oxidative stress, and circulating adiponectin and leptin concentration in subjects with prediabetes and type 2 diabetes mellitus: A GRADE-assessed systematic review, meta-analysis, and meta-regression of randomized clinical trials. Eur. J. Nutr. 2023, 62, 543–561. [Google Scholar]
- Yntema, T.; Koonen, D.P.Y.; Kuipers, F. Emerging Roles of Gut Microbial Modulation of Bile Acid Composition in the Etiology of Cardiovascular Diseases. Nutrients 2023, 15, 1850. [Google Scholar] [CrossRef]
- Naaraayan, A.; Nimkar, A.; Jesmajian, S.; Gitler, B.; Acharya, P. Atherosclerotic cardiovascular disease prevalence among patients with celiac disease in the United States. Mayo Clin. Proc. 2021, 96, 666–676. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, B.; Ciaccio, E.J.; Jneid, H.; Virani, S.S.; Lavie, C.J.; Lebovits, J.; Green, P.H.R.; Krittanawong, C. Celiac Disease and the Risk of Cardiovascular Diseases. Int. J. Mol. Sci. 2023, 24, 9974. [Google Scholar] [CrossRef]
- Tovoli, F.; Negrini, G.; Farì, R.; Guidetti, E.; Faggiano, C.; Napoli, L.; Bolondi, L.; Granito, A. Increased risk of nonalcoholic fatty liver disease in patients with coeliac disease on a gluten-free diet: Beyond traditional metabolic factors. Aliment Pharmacol. Ther. 2018, 48, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Conroy, M.; Allen, N.; Lacey, B.; Soilleux, E.; Littlejohns, T. Association between coeliac disease and cardiovascular disease: Prospective analysis of UK Biobank data. BMJ Med. 2023, 2, e000371. [Google Scholar] [CrossRef]
- Zanini, B.; Mazzoncini, E.; Lanzarotto, F.; Ricci, C.; Cecana, B.; Villanacci, V.; Lanzini, A. Impact of gluten-free diet on cardiovascular risk factors. A retrospective analysis in a large cohort of coeliac patients. Dig. Liver Dis. 2013, 45, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Tortora, R.; Capone, P.; De Stefano, G.; Imperatore, N.; Gerbino, N.; Donetto, S.; Monaco, V.; Caporaso, N.; Rispo, A. Metabolic syndrome in patients with coeliac disease on a gluten-free diet. Aliment Pharmacol. Ther. 2015, 41, 352–359. [Google Scholar] [CrossRef]
- Assa, A.; Frenkel-Nir, Y.; Tzur, D.; Katz, L.H.; Shamir, R. Cardiovascular risk factors in adolescents with celiac disease: A cross-sectional population-based study. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 190–194. [Google Scholar] [CrossRef]
- Tetzlaff, W.F.; Merono, T.; Menafra, M.; Martin, M.; Botta, E.; Matoso, M.D.; Sorroche, P.; DePaula, J.A.; Boero, L.E.; Brites, F. Markers of inflammation and cardiovascular disease in recently diagnosed celiac disease patients. World J. Cardiol. 2017, 9, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Singh, A.; Mehtab, W.; Gupta, V.; Chauhan, A.; Rajput, M.S.; Singh, N.; Ahuja, V.; Makharia, G. Patients with celiac disease are at high risk of developing metabolic syndrome and fatty liver. Intest. Res. 2021, 19, 106–114. [Google Scholar] [CrossRef]
- Fry, L.; Madden, A.M.; Fallaize, R. An investigation into the nutritional composition and cost of gluten free versus regular food products in the UK. J. Hum. Nutr. Diet. 2018, 31, 108–120. [Google Scholar] [CrossRef]
- Lebwohl, B.; Cao, Y.; Zong, G.; Hu, F.B.; Green, P.H.R.; Neugut, A.I.; Rimm, E.B.; Sampson, L.; Dougherty, L.W.; Giovannucci, E.; et al. Long term gluten consumption in adults without celiac disease and risk of coronary heart disease: Prospective cohort study. BMJ 2017, 357, j1892. [Google Scholar] [CrossRef]
- Schmucker, C.; Eisele-Metzger, A.; Meerpohl, J.J.; Lehane, C.; Kuellenberg de Gaudry, D.; Lohner, S.; Schwingshackl, L. Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2022, CD013556. [Google Scholar] [CrossRef]
- Costabile, A.; Buttarazzi, I.; Kolida, S.; Quercia, S.; Baldini, J.; Swann, J.R.; Brigidi, P.; Gibson, G.R. An in vivo assessment of the cholesterol-lowering efficacy of Lactobacillus plantarum ECGC 13110402 in normal to mildly hypercholesterolaemic adults. PLoS ONE 2017, 12, e0187964. [Google Scholar] [CrossRef]
- Keleszade, E.; Kolida, S.; Costabile, A. The cholesterol lowering efficacy of Lactobacillus plantarum ECGC 13110402 in hypercholesterolemic adults: A double-blind, randomized, placebo controlled, pilot human intervention study. J. Func. Foods 2022, 89, 1756–4646. [Google Scholar] [CrossRef]
- Derosa, G.; Gaudio, G.; D’Angelo, A.; Maffioli, P. Evaluation in Patients with High NORMAL Blood Pressure of a Supplement Containing Arginine, Lactobacillus Plantarum Lp-LDL, Coenzime Q10 and Vitamin B1: A PILOT Study. J. Food Nutr. Res. 2020, 8, 273–278. [Google Scholar] [CrossRef]
- Seiler, C.; Kiflen, M.; Stefanolo, J.P.; Bai, J.C.; Bercik, P.; Kelly, C.P.; Verdu, E.F.; Moayyedi, P.; Pinto-Sanchez, M.I. Probiotics for Celiac Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Gastroenterol. 2020, 115, 1584–1595. [Google Scholar] [CrossRef]
- Mozafarybazargany, M.; Khonsari, M.; Sokoty, L.; Ejtahed, H.S.; Qorbani, M. The effects of probiotics on gastrointestinal symptoms and microbiota in patients with celiac disease: A systematic review and meta-analysis on clinical trials. Clin. Exp. Med. 2023, 23, 2773–2788. [Google Scholar] [CrossRef]
- Smecuol, E.; Hwang, H.J.; Sugai, E.; Corso, L.; Chernavsky, A.C.; Bellavite, F.P.; Gonzalez, A.; Vodanovich, F.; Moreno, M.L.; Vazquez, H.; et al. Exploratory, randomized, doubleblind, placebo-controlled study on the effects of Bifidobacterium infantis natren life start strain super strain in active celiac disease. J. Clin. Gastroenterol. 2013, 47, 139–147. [Google Scholar] [CrossRef]
- Olivares, M.; Castillejo, G.; Varea, V.; Sanz, Y. Double-blind, randomised, placebo-controlled intervention trial to evaluate the effects of Bifidobacterium longum CECT 7347 in children with newly diagnosed coeliac disease. Br. J. Nutr. 2014, 112, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Klemenak, M.; Dolinsek, J.; Langerholc, T.; Gioia, D.D.; Micetic-Turk, D. Administration of Bifidobacterium breve decreases the production of TNF- α in children with celiac disease. Dig. Dis. Sci. 2015, 60, 3386–3392. [Google Scholar] [CrossRef]
- Harnett, J.; Myers, S.; Rolfe, M. Probiotics and the microbiome in celiac disease: A randomised controlled trial. Evid. Based Complement Altern Med. 2016, 2016, 9048574. [Google Scholar] [CrossRef]
- Quagliariello, A.; Aloisio, I.; Cionci, N.B.; Luiselli, D.; D’Auria, G.; Martinez-Priego, L.; Perez-Villarroya, D.; Langerholc, T.; Primec, M.; Micetic-Turk, D.; et al. Effect of Bifidobacterium breve on the intestinal microbiota of coeliac children on a gluten free diet: A pilot study. Nutrients 2016, 8, 660. [Google Scholar] [CrossRef]
- Pinto-Sanchez, M.I.; Smecuol, E.C.; Temprano, M.P.; Sugai, E.; Gonzalez, A.; Moreno, M.L.; Huang, X.; Bercik, P.; Cabanne, A.; Vazquez, H.; et al. Bifidobacterium infantis NLS super strain reduces the expression of α-defensin-5, a marker of innate immunity, in the mucosa of active celiac disease patients. J. Clin. Gastroenterol. 2016, 51, 814–817. [Google Scholar] [CrossRef] [PubMed]
- Martinello, F.; Roman, C.F.; Alves de Souza, P. Effects of probiotic intake on intestinal bifidobacteria of celiac patients. Arq. Gastroenterol. 2017, 54, 85–90. [Google Scholar] [CrossRef]
- Primec, M.; Klemenak, M.; Gioia, D.D.; Aloisio, I.; Cionci, N.B.; Quagliariello, A.; Gorenjak, M.; Micetic-Turk, D.; Langerholc, T. Clinical intervention using Bifidobacterium strains in celiac disease children reveals novel microbial modulators of TNF- α and short-chain fatty acids. Clin. Nutr. 2019, 38, 1373–1381. [Google Scholar] [CrossRef]
- Francavilla, R.; Piccolo, M.; Francavilla, A.; Polimeno, L.; Semeraro, F.; Cristofori, F.; Castellaneta, S.; Barone, M.; Indrio, F.; Gobbetti, M.; et al. Clinical and microbiological effect of a multispecies probiotic supplementation in celiac patients with persistent IBS-type symptoms: A randomized, double-blind, placebo-controlled, multicenter trial. J. Clin. Gastroenterol. 2019, 53, e117. [Google Scholar] [CrossRef]
- Smecuol, E.; Constante, M.; Temprano, M.P.; Costa, A.F.; Moreno, M.L.; Pinto-Sanchez, M.I.; Vazquez, H.; Stefanolo, J.P.; Gonzalez, A.F.; D’Adamo, C.R.; et al. Effect of Bifidobacterium infantis NSL super strain in symptomatic coeliac disease patients on long-term gluten-free diet: An exploratroy study. Benef Microbes. 2020, 11, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Ali, B.; Khan, A.R. Efficacy of probiotics in management of celiac disease. Cureus 2022, 14, e22031. [Google Scholar] [CrossRef] [PubMed]
- Gan, J.; Nazarian, S.; Teare, J.; Darzi, A.; Ashrafian, H.; Thompson, A.J. A case for improved assessment of gut permeability: A meta-analysis quantifying the lactulose:mannitol ratio in coeliac and Crohn’s disease. BMC Gastroenterol. 2022, 22, 16. [Google Scholar] [CrossRef]
- Syage, J.A.; Mäki, M.; Leffler, D.A.; Silvester, J.A.; Sealey-Voyksner, J.A.; Wu, T.T.; Murray, J.A. A Composite Morphometric Duodenal Biopsy Mucosal Scale for Celiac Disease Encompassing both Morphology and Inflammation. Clin. Gastroenterol. Hepatol. 2023, 10, S1542–S3565. [Google Scholar] [CrossRef]
- Khorzoghi, M.S.; Rostami-Nejad, M.; Yadegar, A.; Dabiri, H.; Hadadi, A.; Rodrigo, L. Impact of probiotics on gut microbiota composition and clinical symptoms of coeliac disease patients following gluten-free diet. Contemp. Clin. Trials Commun. 2023, 35, 101201. [Google Scholar] [CrossRef]
- Zafeiropoulou, K.; Nichols, B.; Mackinder, M.; Biskou, O.; Rizou, E.; Karanikolou, A.; Clark, C.; Buchanan, E.; Cardigan, T.; Duncan, H.; et al. Alterations in Intestinal Microbiota of Children With Celiac Disease at the Time of Diagnosis and on a Gluten-free Diet. Gastroenterology 2020, 159, 2039–2051. [Google Scholar] [CrossRef]
- He, Y.; Wu, W.; Zheng, H.M.; Li, P.; McDonald, D.; Sheng, H.F.; Chen, M.X.; Chen, Z.H.; Ji, G.Y.; Zheng, Z.D.X.; et al. Regional variation limits applications of healthy gut microbiome reference ranges and disease models. Nat. Med. 2018, 24, 1532–1535. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fagbemi, L.O.; Soldaini, C.; Costabile, A.; Kolida, S.; Ciacci, C.; Jeanes, Y. Probiotic Interventions in Coeliac Disease: A Systematic Review with a Focus on Cardiovascular Risk. Gastrointest. Disord. 2024, 6, 114-130. https://doi.org/10.3390/gidisord6010008
Fagbemi LO, Soldaini C, Costabile A, Kolida S, Ciacci C, Jeanes Y. Probiotic Interventions in Coeliac Disease: A Systematic Review with a Focus on Cardiovascular Risk. Gastrointestinal Disorders. 2024; 6(1):114-130. https://doi.org/10.3390/gidisord6010008
Chicago/Turabian StyleFagbemi, Lorretta Olu, Carlo Soldaini, Adele Costabile, Sofia Kolida, Carolina Ciacci, and Yvonne Jeanes. 2024. "Probiotic Interventions in Coeliac Disease: A Systematic Review with a Focus on Cardiovascular Risk" Gastrointestinal Disorders 6, no. 1: 114-130. https://doi.org/10.3390/gidisord6010008