
Mobile Applications for Epilepsy: Where Are We? Where Should We Go? A Systematic Review

 ,
,  , ,
, ,
Abstract
:1. Introduction
1.1. Seizure Diary and Self-Report
1.2. Mobile Health in Epilepsy
2. Methodology
2.1. Research Questions
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Mobile App Description
2.4.1. Seizure Log
2.4.2. Medication
2.4.3. Third-Party Communication
2.4.4. During Seizure
2.5. Mobile App Evaluation
2.6. Statistical Analysis on MARS Scores
3. Results
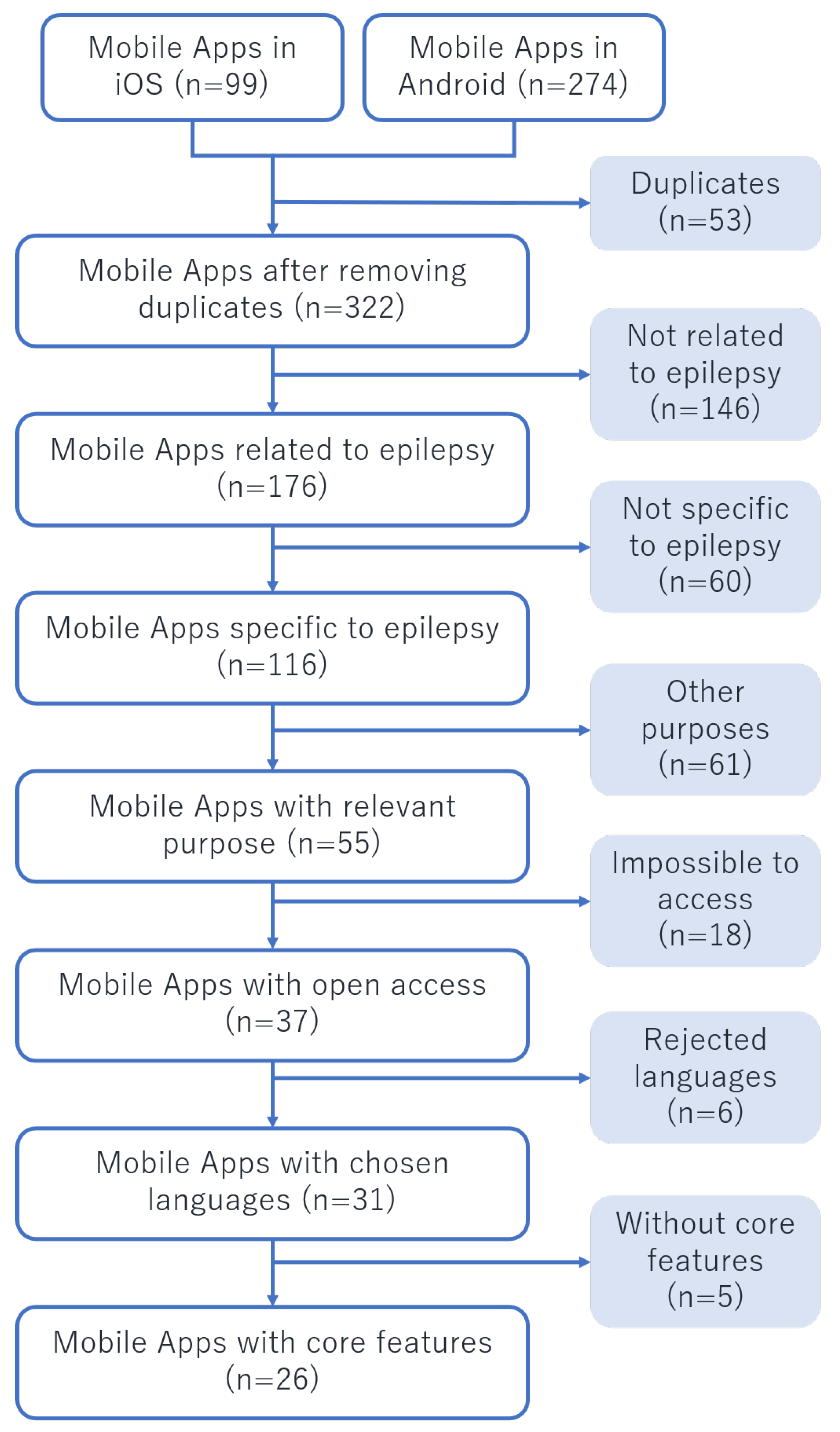
3.1. Mobile App Selection
3.2. Raters
3.3. Analysis of Features Provided
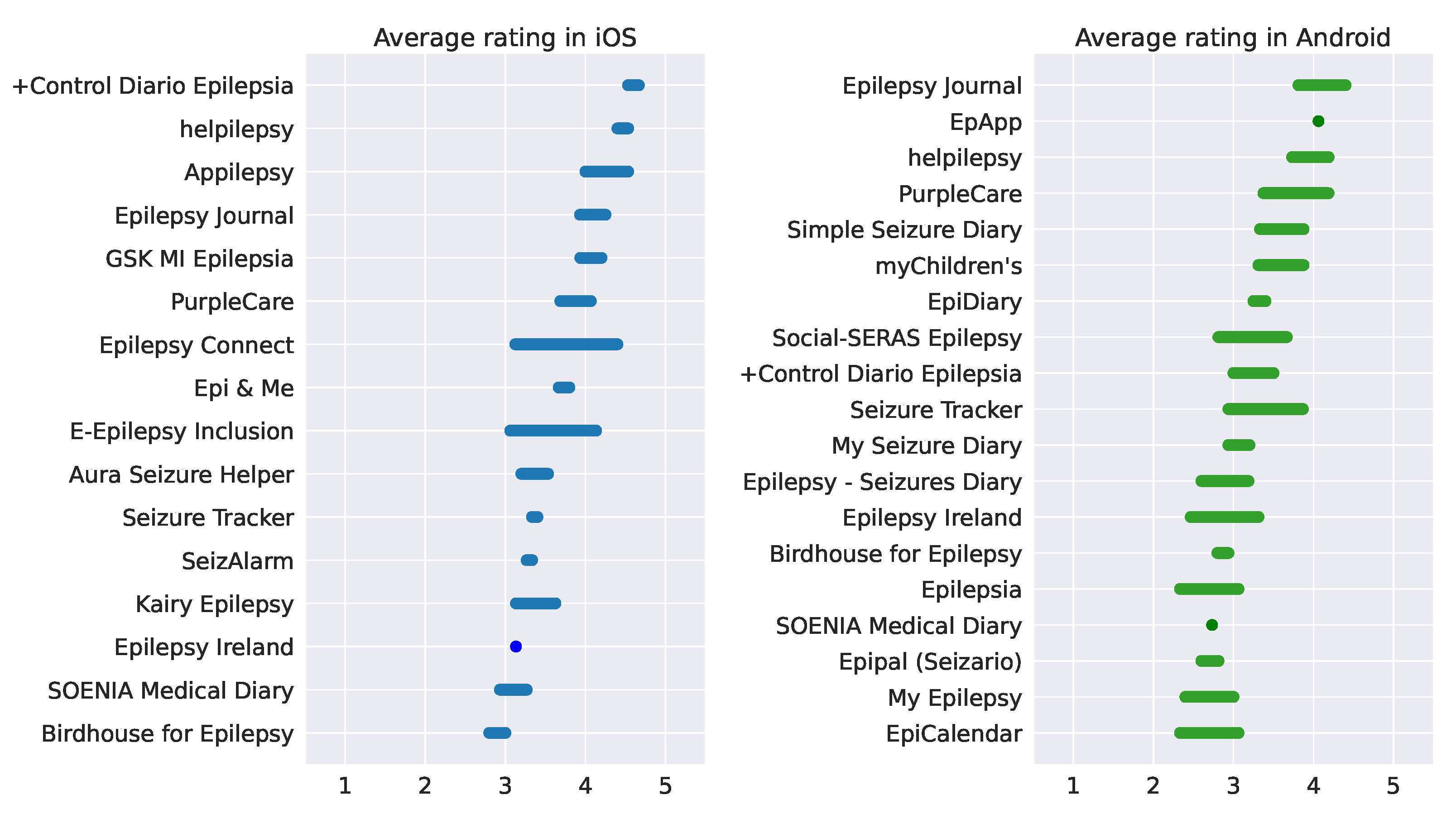
3.4. MARS Ratings
4. Discussion
4.1. Main Findings
4.2. Thoughts on Prior Work
4.3. Key Concepts of an Epilepsy Self-Management App
4.3.1. Customisation
4.3.2. Simplicity
4.3.3. Healthcare Connection
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AFo | Ana Franco |
| AFd | Ana Fred |
| AR | Arabic |
| ARP | Ana Rita Peralta |
| ASC | Ana Sofia Carmo |
| ASM | Anti-seizure Medication |
| BV | Beatriz Vidal |
| CanE | Canadian English |
| CanF | Canadian French |
| CB | Carla Bentes |
| CA | Catalan |
| CI | Confidence Interval |
| DA | Danish |
| DE | German |
| DS | During Seizure |
| EL | Greek |
| EN | English |
| ES | Spanish |
| FI | Finnish |
| FR | French |
| HI | Hindi |
| HPS | Hugo Placido da Silva |
| HR | Croatian |
| HU | Hungarian |
| ID | Indonesian |
| IT | Italian |
| Ja | Japanese |
| Ka | Georgian |
| KO | Korean |
| MA | Mariana Abreu |
| MARS | Mobile App Rating Scale |
| MC | Mariana Costa |
| MDPI | Multidisciplinary Digital Publishing Institute |
| MRA | Mobile Healthcare Apps |
| MR | Marathi |
| NL | Dutch |
| NO | Norwegian |
| OS | Operating System |
| PL | Polish |
| PT | Portuguese |
| PWE | People with Epilepsy |
| RO | Romanian |
| RU | Russian |
| SD | Seizure Detection |
| SL | Seizure Log |
| SM | Seizure Management |
| SP | Sara Parreira |
| SR | Serbian |
| SUDEP | Sudden Unexpected Death in Epilepsy |
| SV | Swedish |
| TH | Thai |
| TPC | Third-party Communication |
| TR | Turkish |
| WHO | World Health Organisation |
| ZH | Chinese |
Appendix A. Overall App Description

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| App Name | Platform | Languages | Purpose | SL | TPC | Access | |
|---|---|---|---|---|---|---|---|
| • | +Control Diario Epilepsia (Fundacion Carlos Slim) | Android and iOS | ES | SM | ✓ | ✓ | Free |
| Alert for Embrace Watch & Mate for Embrace Watch (Empatica) | Android and iOS | EN | SD | ✓ | ✓ | Premium and Needs equipment | |
| Anfallskalender (FLYT IT AS) | iOS | NB | SM | ✓ | - | Free | |
| • | Appilepsy (Appilepsy LLC) | iOS | EN | SM | ✓ | ✓ | Free |
| • | Aura Seizure Helper (Stevhen) | iOS | EN, ID | SM | ✓ | ✓ | Free |
| • | Birdhouse for Epilepsy (Birdhouse LLC) | Android and iOS | EN | SM | ✓ | ✓ | Free and Premium |
| Bleuberi (H2L2 Technology Ltd) | iOS | EN | SM | ✓ | - | 2-week trial | |
| Brain4U (MedToPublic) | Android and iOS | KO | SM | ✓ | ✓ | Free | |
| Brio - Heart Rate Monitor (Candlhat Studios) | Android and iOS | EN | SD | ✓ | - | Needs equipment | |
| • | E-Epilepsy Inclusion (The Hong Kong Society of Rehabilitation) | Android and iOS | ZH, EN | SM | ✓ | ✓ | Free |
| ELFy (ELFy Apps Limited) | Android and iOS | EN | SM | - | ✓ | Free | |
| • | EpApp (Sidney Children’s Hospitals Network) | Android and iOS | EN | SM | ✓ | ✓ | Free |
| • | Epi & Me (HandMe) | iOS | EN, FR | SM | ✓ | ✓ | Free |
| EpiAnfald (Filadelfia DK) | iOS | DA, EN | SM | ✓ | - | Closed | |
| EPIC (Epilepsy Care) | Android | EN | SD | ✓ | ✓ | Failed to access | |
| • | EpiCalendar (MedyCal) | Android | PT | SM | ✓ | ✓ | Free & Premium |
| • | EpiDiary (Irody Inc.) | Android and iOS | EN | SM | ✓ | ✓ | Free |
| Epihunter Companion and Epihunter Core (Epihunter nv) | Android and iOS | EN, NL | SD | ✓ | ✓ | Premium and Needs equipment | |
| • | Epilepsia (Maleny Abrego) | Android | ES | SM | ✓ | ✓ | Free |
| Epilepsia Mexico (Ivan Gonzalez Cortes) | iOS | ES | SM | ✓ | ✓ | Closed | |
| • | Epilepsy Seizures Diary (MedTests) | Android | EN | SM | ✓ | ✓ | Free |
| Epilepsy (Tan Hui Jan) | iOS | EN | SM | ✓ | - | Free | |
| • | Epilepsy Connect (Epilepsy France) | iOS | FR | SM | ✓ | ✓ | Free |
| Epilepsy Diary 3 (Crystal Software Group: CSG mobile team) | Android | TH | SM | ✓ | ✓ | Free | |
| Epilepsy Diary 5 (Crystal Software Group: CSG mobile team) | Android | TH | SM | ✓ | ✓ | Free | |
| Epilepsy Foundation (Chowgule Mediconsult Private LTD) | Android and iOS | EN, HI, MR | SD | ✓ | ✓ | Failed to access | |
| • | Epilepsy Ireland (Epilepsy Ireland) | Android and iOS | EN | SM | ✓ | ✓ | Free |
| • | Epilepsy Journal (Olly Tree Applications) | Android and iOS | PT, DE, ZH, HR, ES, FR, KA, EL, HI, NL, EN, IT, JA, NB, PL, RO, RU, SV, SR | SM | ✓ | ✓ | Free |
| Epistemic App (Epistemic) | Android | EN, PT | SM | ✓ | ✓ | Failed to access | |
| • | GSK MI Epilepsia (Pharmaconsult, SA) | iOS | ES | SM | ✓ | ✓ | Free |
| Heart Buddy (Sean Pedley) | iOS | EN | SD | - | ✓ | Needs equipment | |
| • | Helpilepsy (Epione BVBA) | Android and iOS | FR, DE, NL, EN, DA, ES, CANE, CANF, HU, IT | SM | ✓ | ✓ | Free |
| Inspyre App (Smart Monitor) | Android | EN | SD | ✓ | ✓ | Premium and Needs equipment | |
| • | Kairy Epilepsy (Kairy Limited) | iOS | EN | SM | ✓ | ✓ | Free and Premium |
| My Epilepsy (Catalyst Hub Apps) | Android | AR, EN | SM | ✓ | - | Free | |
| My Epilepsy Record (ESH Solutions Limited) | Android and iOS | EN | SM | ✓ | ✓ | Closed | |
| My Epistatus (Veriton Pharma) | Android | EN | SM | ✓ | ✓ | Closed | |
| • | My Seizure Diary (Epilepsy Foundation) | Android and iOS | EN | SM | ✓ | ✓ | Free |
| • | myChildren’s (Nationwide Children’s Hospital) | Android | EN | SM | ✓ | ✓ | Free |
| OpenSeizureDetector and Garmin Connect App (OpenSeizureDetector) | Android | EN, FR, IT | SD | ✓ | ✓ | Needs equipment | |
| • | PurpleCare (DHYGEE SA) | Android and iOS | EN, IT, FR | SM | ✓ | ✓ | Free |
| Sami3 Sleep Activity Monitor (HiPass Design LLC) | iOS | EN | SD | ✓ | ✓ | Needs equipment | |
| Seer (Seer Medical) | Android and iOS | EN, DE | SM | ✓ | - | Free | |
| • | SeizAlarm (SeizAlarm LLC) | iOS | EN | SD | ✓ | ✓ | 2-week trial |
| • | Seizario (Epipal) (HealthAppy Tech) | Android | EN | SD | ✓ | ✓ | Free |
| Seizure Alert (My Medic Watch) | Android | EN, FR | SD | ✓ | ✓ | 30-day trial and Needs equipment | |
| Seizure Counter (SJAPPER AS) | iOS | EN | SD | ✓ | - | Free | |
| Seizure Cycle (Sheikh Zayed Institute) | Android and iOS | EN ? | SM | ✓ | ✓ | Closed | |
| • | Seizure Tracker/ Seizure Log (Seizure Tracker LLC) | Android & iOS | EN | SM | ✓ | ✓ | Free |
| SeizureSync Epilepsy Log (doc.ai) | iOS | EN | SD | ✓ | ✓ | Failed to access | |
| • | Simple Seizure Diary (Luke Berry) | Android | EN | SM | ✓ | ✓ | Free |
| • | Social-SERAS Epilepsy (mjn-neuro) | Android | CA, EN, ES | SM | ✓ | ✓ | Free |
| • | SOENIA Medical Diary (BrainCare Oy) | Android and iOS | DE, EN, FI, SV | SM | ✓ | ✓ | Free |
| Yeditepe EpilepsiSiz (G Boson) | Android and iOS | TR | SM | ✓ | ✓ | Free |
Appendix B. In-Depth Features
| Name | Seizure Cycle (SL) | Resolution (SL) | Other Logs (SL) | Type and Dosage (Med) | Schedule (Med) | History (Med) | Side Effects (Med) |
|---|---|---|---|---|---|---|---|
| +Control Diario Epilepsia (Fundacion Carlos Slim) | - | Monthly | Emotion log | ✓ | ✓ | - | - |
| Appilepsy (Appilepsy LLC) | ✓ | Yearly | Trigger log on seizure log | ✓ | ✓ | - | - |
| Aura Seizure Helper (Stevhen) | - | Monthly | Post-seizure questionnaire | - | - | - | - |
| Birdhouse for Epilepsy (Birdhouse LLC) | Premium | Monthly | Triggers, sleep and food | ✓ | Premium | ✓ | ✓ |
| E-Epilepsy Inclusion (The Hong Kong Society of Rehabilitation) | ✓ | Weekly, Monthly | - | ✓ | ✓ | ✓ | ✓ |
| EpApp (Sidney Children’s Hospitals Network) | ✓ | Daily | Trigger log on seizure log | ✓ | ✓ | ✓ | - |
| Epi & Me (HandMe) | ✓ | List view | Humour and energy | ✓ | ✓ | ✓ | ✓ |
| EpiCalendar (MedyCal) | - | Daily | Menstrual log | Premium | - | - | - |
| EpiDiary (Irody Inc.) | Only on Website | Weekly | Sleep and menstrual log | ✓ | ✓ | Only on website | ✓ |
| Epilepsia (Maleny Abrego) | - | Daily | Open-box on seizure log | ✓ | ✓ | - | - |
| Epilepsy Seizures Diary (MedTests) | - | Daily | Post-seizure questionnaire and symptom log | ✓ | - | - | - |
| Epilepsy Connect (Epilepsy France) | - | Monthly | Post-seizure questionnaire | ✓ | - | ✓ | - |
| Epilepsy Ireland (Epilepsy Ireland) | ✓ | Monthly, Daily | Post-seizure questionnaire | ✓ | ✓ | - | - |
| Epilepsy Journal (Olly Tree Applications) | ✓ | Monthly, Daily | Trigger log on seizure log | ✓ | ✓ | ✓ | - |
| GSK MI Epilepsia (Pharmaconsult, SA) | - | Monthly | Post-seizure questionnaire | ✓ | ✓ | - | - |
| Helpilepsy (Epione BVBA) | - | Yearly, Monthly, Weekly, Daily | Post-seizure questionnaire & sleep & mood log | ✓ | ✓ | - | ✓ |
| Kairy Epilepsy (Kairy Limited) | Premium | Weekly | Logs for several features a | ✓ | ✓ | ✓ | ✓ |
| My Seizure Diary (Epilepsy Foundation) | ✓ | Weekly, Daily | Trigger log, mood and menstrual log | ✓ | ✓ | - | ✓ |
| myChildren’s (Nationwide Children’s Hospital) | - | Daily | Open-box on seizure log | ✓ | ✓ | - | - |
| PurpleCare (DHYGEE SA) | - | Monthly, Weekly | Trigger log on seizure log | ✓ | ✓ | - | ✓ |
| SeizAlarm (SeizAlarm LLC) | ✓ | Yearly, Monthly, Weekly | Post-seizure questionnaire | - | - | - | - |
| Seizario/ Epipal (HealthAppy Tech) | - | Post-seizure questionnaire, mood log | ✓ | - | - | - | |
| Seizure Tracker/ Seizure Log (Seizure Tracker LLC) | ✓ | Daily | Trigger log on seizure log | Only on website | Only on website | - | Only on website |
| Simple Seizure Diary (Luke Berry) | ✓ | Daily | Trigger log on seizure log | - | - | - | - |
| Social-SERAS Epilepsy (mjn-neuro) | - | Daily | Other logs b | - | - | - | - |
| SOENIA Medical Diary (BrainCare Oy) | - | Daily | Trigger log on seizure log | - | - | - | - |
| Name | Report Export (TPC) | Channel (TPC) | Alarm Button (DS) | Seizure Procedures (DS) | GPS Tracking (DS) | Video and Audio (DS) | Personalisable Content |
|---|---|---|---|---|---|---|---|
| +Control Diario Epilepsia (Fundacion Carlos Slim) | - | Phone | - | ✓ | - | Video rec. | ✓ |
| Appilepsy (Appilepsy LLC) | ✓ | - | - | - | - | ✓ | |
| Aura Seizure Helper (Stevhen) | - | Phone | ✓ | ✓ | ✓ | - | - |
| Birdhouse for Epilepsy (Birdhouse LLC) | - | Web Platform | - | - | - | Premium | ✓ |
| E-Epilepsy Inclusion (The Hong Kong Society of Rehabilitation) | - | App2App | - | - | - | Video rec. | - |
| EpApp (Sidney Children’s Hospitals Network) | ✓ | Email, instant msg. | - | - | - | - | ✓ |
| Epi & Me (HandMe) | ✓ | - | - | - | - | ✓ | |
| EpiCalendar (MedyCal) | ✓ | - | - | - | - | - | - |
| EpiDiary (Irody Inc.) | ✓ | Web platform | ✓ | - | - | - | ✓ |
| Epilepsia (Maleny Abrego) | - | Phone | ✓ | - | ✓ | - | - |
| Epilepsy Seizures Diary (MedTests) | ✓ | Email, instant msg. | - | - | - | - | - |
| Epilepsy Connect (Epilepsy France) | ✓ | - | - | - | - | - | - |
| Epilepsy Ireland (Epilepsy Ireland) | ✓ | - | - | - | Video rec. | ✓ | |
| Epilepsy Journal (Olly Tree Applications) | ✓ | Email, instant msg. | ✓ | - | Add location manually | - | - |
| GSK MI Epilepsia (Pharmaconsult, SA) | ✓ | Email, instant msg. | - | - | - | - | - |
| Helpilepsy (Epione BVBA) | - | - | - | - | Video rec. | - | |
| Kairy Epilepsy (Kairy Limited) | Premium | Premium | - | - | - | - | - |
| My Seizure Diary (Epilepsy Foundation) | - | App2App | - | - | - | - | ✓ |
| myChildren’s (Nationwide Children’s Hospital) | ✓ | Email, instant msg. | - | ✓ | - | - | - |
| PurpleCare (DHYGEE SA) | ✓ | Web platform | - | - | - | Video rec. | - |
| SeizAlarm (SeizAlarm LLC) | ✓ | Email, phone | ✓ | - | ✓ | - | - |
| Seizario/ Epipal (HealthAppy Tech) | - | Phone | ✓ | - | - | - | - |
| Seizure Tracker/ Seizure Log (Seizure Tracker LLC) | Only on Website | Web platform | ✓ | - | - | Video and audio rec. | - |
| Simple Seizure Diary (Luke Berry) | ✓ | Email, instant msg. | ✓ | - | - | - | ✓ |
| Social-SERAS Epilepsy (mjn-neuro) | ✓ | - | - | - | - | - | ✓ |
| SOENIA Medical Diary (BrainCare Oy) | - | Web platform | - | - | Add location manually | - | ✓ |
Appendix C. MARS Evaluation
| Name | N Raters | Engagement | Functionality | Aesthetics | Information | Overall |
|---|---|---|---|---|---|---|
| +Control Diario Epilepsia (Fundacion Carlos Slim) | 5 | 3.7 | 4.2 | 3.7 | 4.0 | 3.8 |
| Appilepsy (Appilepsy LLC) | 3 | 4.1 | 4.4 | 4.3 | 4.1 | 4.2 |
| Aura Seizure Helper (Stevhen) | 3 | 3.5 | 4.4 | 3.9 | 4.7 | 4.2 |
| Birdhouse for Epilepsy (Birdhouse LLC) | 6 | 3.0 | 2.9 | 3.2 | 2.7 | 3.0 |
| E-Epilepsy Inclusion (The Hong Kong Society of Rehabilitation) | 3 | 3.7 | 4.1 | 3.4 | 3.5 | 3.6 |
| EpApp (Sidney Children’s Hospitals Network) | 1 | 4.4 | 3.2 | 4.0 | 4.5 | 4.2 |
| Epi & Me (HandMe) | 3 | 3.3 | 4.0 | 3.9 | 3.8 | 3.8 |
| EpiCalendar (MedyCal) | 3 | 2.3 | 3.9 | 2.6 | 2.5 | 2.6 |
| EpiDiary (Irody Inc.) | 2 | 3.5 | 3.4 | 3.0 | 3.4 | 3.4 |
| Epilepsia (Maleny Abrego) | 3 | 3.0 | 3.2 | 2.7 | 2.3 | 2.8 |
| Epilepsy Seizures Diary (MedTests) | 2 | 1.3 | 3.4 | 3.2 | 2.8 | 3.2 |
| Epilepsy Connect (Epilepsy France) | 3 | 3.9 | 4.0 | 4.1 | 3.8 | 4.0 |
| Epilepsy Ireland (Epilepsy Ireland) | 3 | 3.2 | 3.7 | 3.0 | 3.2 | 3.2 |
| Epilepsy Journal (Olly Tree Applications) | 6 | 4.3 | 4.4 | 4.1 | 4.0 | 4.2 |
| GSK MI Epilepsia (Pharmaconsult, SA) | 3 | 3.8 | 4.3 | 4.0 | 4.1 | 4.0 |
| Helpilepsy (Epione BVBA) | 6 | 4.2 | 4.5 | 4.7 | 3.9 | 4.4 |
| Kairy Epilepsy (Kairy Limited) | 3 | 3.2 | 4.1 | 3.7 | 3.8 | 3.8 |
| My Epilepsy ( Foundation) | 2 | 2.2 | 3.6 | 2.2 | 2.8 | 2.5 |
| My Seizure Diary (Epilepsy Foundation) | 2 | 3.8 | 2.6 | 3.2 | 2.8 | 3.0 |
| myChildren’s (Nationwide Children’s Hospital) | 3 | 3.6 | 3.5 | 3.1 | 3.8 | 3.6 |
| PurpleCare (DHYGEE SA) | 6 | 4.1 | 4.4 | 4.4 | 4.0 | 4.2 |
| SeizAlarm (SeizAlarm LLC) | 2 | 3.5 | 4.2 | 3.7 | 4.0 | 3.8 |
| Epipal (Seizario) (HealthAppy Tech) | 2 | 2.8 | 3.4 | 3.0 | 2.1 | 2.9 |
| Seizure Tracker/ Seizure Log (Seizure Tracker LLC) | 6 | 2.7 | 3.8 | 3.3 | 3.6 | 3.4 |
| Simple Seizure Diary (Luke Berry) | 2 | 4.1 | 4.2 | 3.5 | 3.1 | 3.8 |
| Social-SERAS Epilepsy (mjn-neuro) | 3 | 3.2 | 3.7 | 3.6 | 2.9 | 3.4 |
| SOENIA Medical Diary (BrainCare Oy) | 3 | 3.1 | 4.1 | 3.1 | 3.3 | 3.2 |
References
- World Health Organization, Global Campaign against Epilepsy, Programme for Neurological Diseases, Neuroscience (World Health Organization), International Bureau for Epilepsy, World Health Organization; Department of Mental Health, Substance Abuse, International Bureau of Epilepsy and International League against Epilepsy. Atlas: Epilepsy Care in the World; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- French, J.A. Refractory epilepsy: Clinical overview. Epilepsia 2007, 48, 3–7. [Google Scholar] [CrossRef]
- Beghi, E. Addressing the burden of epilepsy: Many unmet needs. Pharmacol. Res. 2016, 107, 79–84. [Google Scholar] [CrossRef]
- Assenza, G.; Lanzone, J.; Brigo, F.; Coppola, A.; Di Gennaro, G.; Di Lazzaro, V.; Ricci, L.; Romigi, A.; Tombini, M.; Mecarelli, O. Epilepsy care in the time of COVID-19 pandemic in Italy: Risk factors for seizure worsening. Front. Neurol. 2020, 11, 737. [Google Scholar] [CrossRef]
- Moalong, K.M.C.; Espiritu, A.I.; Fernandez, M.L.L.; Jamora, R.D.G. Treatment gaps and challenges in epilepsy care in the Philippines. Epilepsy Behav. 2021, 115, 107491. [Google Scholar] [CrossRef] [PubMed]
- Mahendran, M.; Speechley, K.N.; Widjaja, E. Systematic review of unmet healthcare needs in patients with epilepsy. Epilepsy Behav. 2017, 75, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Fesler, J.R.; Stanton, S.; Merner, K.; Ross, L.; McGinley, M.P.; Bena, J.; Rasmussen, P.; Najm, I.; Punia, V. Bridging the gap in epilepsy care: A single-center experience of 3700 outpatient tele-epilepsy visits. Epilepsia 2020, 61, e95–e100. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.S.; Blum, D.E.; DiVentura, B.; Vannest, J.; Hixson, J.D.; Moss, R.; Herman, S.T.; Fureman, B.E.; French, J.A. Seizure diaries for clinical research and practice: Limitations and future prospects. Epilepsy Behav. 2012, 24, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191. [Google Scholar] [CrossRef]
- Dilorio, C.; Henry, M. Self-management in persons with epilepsy. J. Neurosci. Nurs. J. Am. Assoc. Neurosci. Nurses 1995, 27, 338–343. [Google Scholar] [CrossRef]
- Fraser, R.T.; Johnson, E.K.; Lashley, S.; Barber, J.; Chaytor, N.; Miller, J.W.; Ciechanowski, P.; Temkin, N.; Caylor, L. PACES in epilepsy: Results of a self-management randomized controlled trial. Epilepsia 2015, 56, 1264–1274. [Google Scholar] [CrossRef] [Green Version]
- Blachut, B.; Hoppe, C.; Surges, R.; Elger, C.; Helmstaedter, C. Subjective seizure counts by epilepsy clinical drug trial participants are not reliable. Epilepsy Behav. 2017, 67, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.; Feng, W.; Chen, K.; French, J.A.; Rushton, M.; Hubbard, S.; Ren, Z.; Potero, E.; Parkerson, K.A. Use of an electronic seizure diary in a randomized, controlled trial of natalizumab in adult participants with drug-resistant focal epilepsy. Epilepsy Behav. 2021, 118, 107925. [Google Scholar] [CrossRef] [PubMed]
- Conde-Blanco, E.; Centeno, M.; Tio, E.; Muriana, D.; García-Peñas, J.J.; Serrano, P.; Nagel, A.G.; Serratosa, J.; Jiménez, Á.P.; Toledo, M.; et al. Emergency implementation of telemedicine for epilepsy in Spain: Results of a survey during SARS-CoV-2 pandemic. Epilepsy Behav. 2020, 111, 107211. [Google Scholar] [CrossRef] [PubMed]
- Escoffery, C.; McGee, R.; Bidwell, J.; Sims, C.; Thropp, E.K.; Frazier, C.; Mynatt, E.D. A review of mobile apps for epilepsy self-management. Epilepsy Behav. 2018, 81, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, J.P.; Wolking, S.; Weber, Y.; Rosenow, F. Decision-support-Systeme, Assistenzsysteme und Telemedizin in der Epileptologie. Der Nervenarzt 2021, 92, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Mohammadzadeh, N.; Khenarinezhad, S.; Ghazanfarisavadkoohi, E.; Safari, M.S.; Pahlevanynejad, S. Evaluation of M-Health Applications Use in Epilepsy: A Systematic Review. Iran. J. Public Health 2021, 50, 459–469. [Google Scholar] [CrossRef]
- Phongtraychack, A.; Dolgaya, D. Evolution of Mobile Applications. MATEC Web Conf. 2018, 155, 01027. [Google Scholar] [CrossRef] [Green Version]
- Statista Research Department. Average Number of New Android App Releases via Google Play per Month from March 2019 to November 2021. 2021. Available online: https://www.statista.com/statistics/1020956/android-app-releases-worldwide/ (accessed on 1 January 2022).
- 42Matters. iOS Apple App Store Statistics and Trends 2021. 2021. Available online: https://42matters.com/ios-apple-app-store-statistics-and-trends (accessed on 1 January 2022).
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Grady, P.A.; Gough, L.L. Self-management: A comprehensive approach to management of chronic conditions. Am. J. Public Health 2014, 104, e25–e31. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile App Rating Scale: A New Tool for Assessing the Quality of Health Mobile Apps. JMIR mHealth uHealth 2015, 3, e27. [Google Scholar] [CrossRef] [Green Version]
- Knitza, J.; Tascilar, K.; Messner, E.M.; Meyer, M.; Vossen, D.; Pulla, A.; Bosch, P.; Kittler, J.; Kleyer, A.; Sewerin, P.; et al. German mobile apps in rheumatology: Review and analysis using the Mobile Application Rating Scale (MARS). JMIR mHealth uHealth 2019, 7, e14991. [Google Scholar] [CrossRef] [PubMed]
- Goldenholz, D.M.; Moss, R.; Scott, J.; Auh, S.; Theodore, W.H. Confusing placebo effect with natural history in epilepsy: A big data approach. Ann. Neurol. 2015, 78, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Chiang, S.; Moss, R.; Patel, A.D.; Rao, V.R. Seizure detection devices and health-related quality of life: A patient-and caregiver-centered evaluation. Epilepsy Behav. 2020, 105, 106963. [Google Scholar] [CrossRef] [PubMed]
- Chiang, S.; Goldenholz, D.M.; Moss, R.; Rao, V.R.; Haneef, Z.; Theodore, W.H.; Kleen, J.K.; Gavvala, J.; Vannucci, M.; Stern, J.M. Prospective validation study of an epilepsy seizure risk system for outpatient evaluation. Epilepsia 2020, 61, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Helmy, A.; Helmy, A. Seizario: Novel Mobile Algorithms for Seizure and Fall Detection. In Proceedings of the 2015 IEEE Globecom Workshops (GC Wkshps), San Diego, CA, USA, 6–10 December 2015; pp. 1–6. [Google Scholar]
- Helmy, A.; Helmy, A. Detecting epileptic seizures with a smartphone using frequency analysis. In Proceedings of the IEEE INFOCOM 2018-IEEE Conference on Computer Communications Workshops (INFOCOM WKSHPS), Honolulu, HI, USA, 15–19 April 2018; pp. 1–2. [Google Scholar]
- SOENIA. Clinical Evidence-SOENIA. Available online: https://gettingbetter.fi/testi/wordpress/clinical-evidence/ (accessed on 23 September 2021).
- Dhygee. Dhygee—The Patient Dedicated Digital Healthcare Start-Up. Available online: https://dhygee.com/#our-awards (accessed on 23 September 2021).
- Brigo, F.; Bonavita, S.; Leocani, L.; Tedeschi, G.; Lavorgna, L. Telemedicine and the challenge of epilepsy management at the time of COVID-19 pandemic. Epilepsy Behav. 2020, 110, 107164. [Google Scholar] [CrossRef] [PubMed]
- Helpilepsy. Patient—Helpilepsy. Available online: https://helpilepsy.com/patient/ (accessed on 23 September 2021).
- Foundation, D.S. MemberMonday Spotlight. Available online: https://www.dravetfoundation.org/member-monday-david-and-natasha/?eType=EmailBlastContent&eId=56ace3cb-995e-4ef3-a3d8-43c787b78fda (accessed on 23 September 2021).
- Le Marne, F.A.; Butler, S.; Beavis, E.; Gill, D.; Bye, A.M. EpApp: Development and evaluation of a smartphone/tablet app for adolescents with epilepsy. J. Clin. Neurosci. 2018, 50, 214–220. [Google Scholar] [CrossRef]
- Yoo, S.; Lim, K.; Baek, H.; Jang, S.K.; Hwang, G.Y.; Kim, H.; Hwang, H. Developing a mobile epilepsy management application integrated with an electronic health record for effective seizure management. Int. J. Med. Inform. 2020, 134, 104051. [Google Scholar] [CrossRef]
- Choi, S.A.; Lim, K.; Baek, H.; Yoo, S.; Cho, A.; Kim, H.; Hwang, H.; Kim, K.J. Impact of mobile health application on data collection and self-management of epilepsy. Epilepsy Behav. 2021, 119, 107982. [Google Scholar] [CrossRef]
- Alzamanan, M.Z.; Lim, K.S.; Ismail, M.A.; Ghani, N.A. Self-Management Apps for People With Epilepsy: Systematic Analysis. JMIR mHealth uHealth 2021, 9, e22489. [Google Scholar] [CrossRef]
- Dozières-Puyravel, B.; Danse, M.; Goujon, E.; Höhn, S.; Auvin, S. Views of adolescents and their parents on mobile apps for epilepsy self-management. Epilepsy Behav. 2020, 106, 107039. [Google Scholar] [CrossRef]
- Thompson, M.E.; Goodwin, R.; Ojeda, A.; Morris, L.; Fairman, A.D. User preferences for the design of a mobile health system to support transition-age youth with epilepsy. J. Pediatr. Health Care 2020, 34, e28–e36. [Google Scholar] [CrossRef] [PubMed]
- Rahim, M.I.A.; Thomas, R.H. Gamification of medication adherence in epilepsy. Seizure 2017, 52, 11–14. [Google Scholar] [CrossRef] [Green Version]
- Stirling, R.E.; Cook, M.J.; Grayden, D.B.; Karoly, P.J. Seizure forecasting and cyclic control of seizures. Epilepsia 2021, 62, S2–S14. [Google Scholar] [CrossRef]
- Payne, D.E.; Dell, K.L.; Karoly, P.J.; Kremen, V.; Gerla, V.; Kuhlmann, L.; Worrell, G.A.; Cook, M.J.; Grayden, D.B.; Freestone, D.R. Identifying seizure risk factors: A comparison of sleep, weather, and temporal features using a Bayesian forecast. Epilepsia 2021, 62, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Schnall, R.; Rojas, M.; Bakken, S.; Brown, W.; Carballo-Dieguez, A.; Carry, M.; Gelaude, D.; Mosley, J.P.; Travers, J. A user-centered model for designing consumer mobile health (mHealth) applications (apps). J. Biomed. Inform. 2016, 60, 243–251. [Google Scholar] [CrossRef]
- Goldenholz, D.M.; Moss, R.; Jost, D.A.; Crone, N.E.; Krauss, G.; Picard, R.; Caborni, C.; Cavazos, J.E.; Hixson, J.; Loddenkemper, T.; et al. Common data elements for epilepsy mobile health systems. Epilepsia 2018, 59, 1020–1026. [Google Scholar] [CrossRef] [Green Version]






| Item | Engagement | Functionality | Aesthetics | Information |
|---|---|---|---|---|
| Sub-items | Entertainment | Performance | Layout | Accuracy of app description |
| Interest | Ease of use | Graphics | Goals | |
| Customisation | Navigation | Visual appeal | Quality of information | |
| Interactivity | Gestural design | Quantity of information | ||
| Target group | Credibility | |||
| Evidence base |
| ID | Age Range | OS | # Rated Apps |
|---|---|---|---|
| R1 | [18, 30] | iOS | 16 |
| R2 | iOS | 15 | |
| R3 | Android | 18 | |
| R4 | Android | 18 | |
| R5 | iOS | 13 | |
| R6 | Android | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abreu, M.; Carmo, A.S.; Franco, A.; Parreira, S.; Vidal, B.; Costa, M.; Peralta, A.R.; da Silva, H.P.; Bentes, C.; Fred, A. Mobile Applications for Epilepsy: Where Are We? Where Should We Go? A Systematic Review. Signals 2022, 3, 40-65. https://doi.org/10.3390/signals3010005
Abreu M, Carmo AS, Franco A, Parreira S, Vidal B, Costa M, Peralta AR, da Silva HP, Bentes C, Fred A. Mobile Applications for Epilepsy: Where Are We? Where Should We Go? A Systematic Review. Signals. 2022; 3(1):40-65. https://doi.org/10.3390/signals3010005
Chicago/Turabian StyleAbreu, Mariana, Ana Sofia Carmo, Ana Franco, Sara Parreira, Beatriz Vidal, Mariana Costa, Ana Rita Peralta, Hugo Plácido da Silva, Carla Bentes, and Ana Fred. 2022. "Mobile Applications for Epilepsy: Where Are We? Where Should We Go? A Systematic Review" Signals 3, no. 1: 40-65. https://doi.org/10.3390/signals3010005