1. Introduction
The complex regressions and transformations that take place within the circulatory system of the developing embryo can result in numerous venous variations that persist into adulthood. While anomalies of the inferior vena cava (IVC) are rare, they have become more frequently encountered due to the increased use of computed tomography and other imaging modalities [
1,
2]. The major congenital venous anomalies reported in the literature include left-sided IVC, duplicated IVC (DIVC), retroaortic left renal vein (RV), circumaortic left RV, accessory left RV, and azygos or hemiazygos continuation of IVC [
1,
2]. DIVCs were first identified in 1916 via gross dissection [
3]. Subsequent case reports and imaging studies have established an incidence rate among the population from 0.2% to 3.0% [
1,
3,
4]. Itoh et al. proposed a classification of venous draining in the case of DIVC. In females, Type II drainage (left gonadal vein (LGV) draining to left IVC (LIVC) at the level of the left renal vein) was recorded as the most common variation, followed by Type III (LGV drainage to the left renal vein proximal to the preaortic trunk which connects the left and right IVCs). Type I drainage (LGV draining to the LIVC distal to the left renal vein draining to the LIVC) is recorded less frequently, with Type IV (either LGV drainage to the preaortic trunk or to a common drainage point with the suprarenal vein) not being recorded in the study [
1]. While most DIVCs are clinically silent and found incidentally via imaging studies, they do carry important clinical relevance during retroperitoneal surgeries [
3,
4]. DIVCs also impact clinical decision making in the treatment of thrombotic disease states as the presence of a DIVC itself confers an increased risk for deep venous thrombosis [
3,
4]. DIVCs have the potential to influence circulatory hemodynamics by altering the normal anatomical course of the gonadal veins (testicular vein in males, ovarian vein in females).
Vascular abnormalities of the RVs are not uncommon and may carry an increased surgical risk. Especially in instances of renal vessel repair via a laparoscopic approach which is already more difficult compared to open surgery and often results in various complications [
5]. Thus, understanding the morphology and prevalence of RV anomalies is of great importance during surgical repair. Furthermore, RV anomalies have been associated with varicocele, nutcracker syndrome, pelvic congestion syndrome, hematuria, low-back pain, and renal ectopia [
5]. The presence of multiple renal veins has been reported in the literature with highly variable prevalence ranges (2–40% [
5]).
The celiac trunk (CT), superior mesenteric artery (SMA), and inferior mesenteric artery (IMA) comprise the three major unpaired visceral branches of the abdominal aorta which supply arterial blood to the abdominal gastrointestinal tract. Most reference texts highlight that the SMA gives rise to the middle colic artery (MCA), right colic artery (RCA), and ileocolic artery (ICA), as well as many jejunal and ileal branches, while the hindgut receives its supply from the inferior mesenteric artery (IMA) [
6]. However, reports have cited variations in the origin and course of these abdominal vessels, particularly the CT and SMA [
7]. Variations of the CT and SMA are the most well documented of the anomalies within the literature. As is the case for DIVC, arterial anomalies of the gut are believed to be the result of changes occurring during the development of these vessels. The most noteworthy variation pertains to aberrancies specific to the origin of the left colic artery (LCA), as these tend to occur less frequently [
8].
The aim of this study is to provide a cadaveric case report of an individual with a duplicated IVC accompanied by multiple left accessory RVs and an SMA-derived left colic artery for the purpose of highlighting a unique collection of anatomical variations. To the best of the authors’ knowledge, this constellation of relatively rare anatomical anomalies has not yet been reported in the literature.
2. Case Report
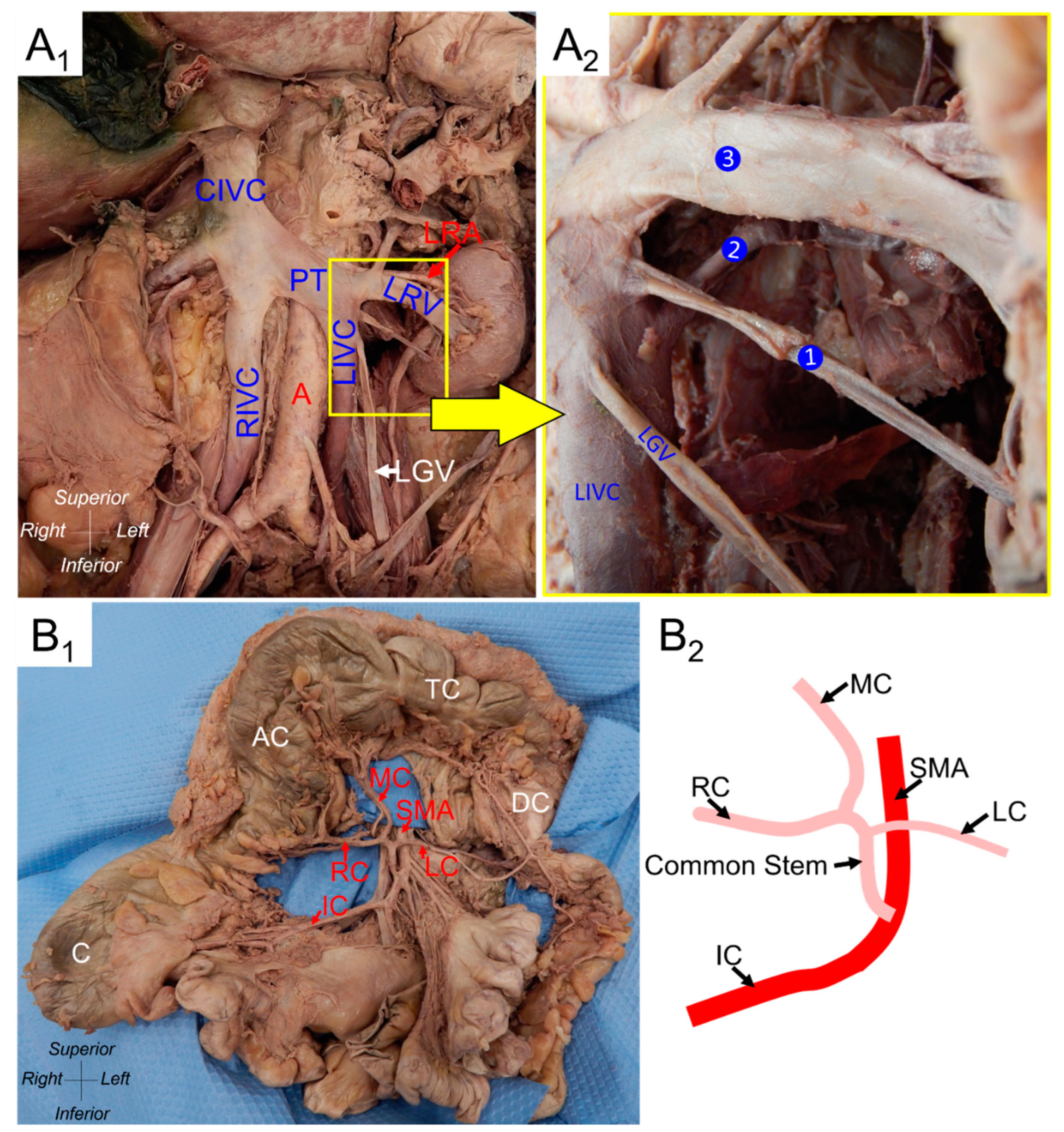
The DIVC, multiple left accessory renal veins, and an SMA-derived left colic artery reported here were found in a 74-year-old female cadaver during routine dissection in a medical gross anatomy course. In addition to the expected IVC on the right side of the donor, an additional vessel was identified coursing on the left side of the abdominal aorta parallel to the IVC (
Figure 1(A
1)). This structure was identified as a left IVC (LIVC). The LIVC received the left RV as well as multiple smaller accessory RVs (
Figure 1(A
2)). To better understand the relationships within the abdomen, measurements of key structures were taken using ImageJ Software (version 1.53j) [
9]. The most caudal accessory RV measured 2.26 mm in diameter and exited the kidney 19.41 mm inferiorly to the hilum and 29.14 mm superior to the inferior pole. The right IVC (RIVC) measured 14.59 mm in diameter, while the LIVC measured 9.97 mm in diameter distally and 20.60 mm caudally near the renal vein entrances. The LIVC coursed obliquely superiorly across the abdominal aorta to join the right IVC, forming a common IVC (CIVC), 27.15 mm in diameter. The confluence of the RIVC and LIVC, known as the preaortic trunk (PT), measured 22.08 mm in diameter. The CIVC continued in a textbook fashion along a retrohepatic route before passing through the diaphragm and into the right atrium. Rather than draining in the common route into the left renal vein, the left gonadal vein (GV) drained directly into the LIVC 4.84 mm inferior to the drainage point of the left renal vein. This is categorized by Itoh et al. as a Type I drainage pattern [
1] (
Figure 1(A
1,A
2)). The left GV measured 4.84 mm in diameter (
Table 1).
Examination of the SMA revealed a branch which functioned as a common stem for the RCA, MCA, and LCA (
Figure 1(B
1,B
2)). This common stem branched off of the SMA 59.93 mm from the aorta. The LCA branched off this stem after 21.70 mm. The stem then continued for 5.97 mm before splitting into an RCA and MCA. The SMA measured 7.23 mm in diameter. The LCA, RCA, and MCA had diameters of 2.99 mm, 3.76 mm, and 3.45 mm, respectively (
Table 1). No LCA was detected off of the IMA.
3. Discussion
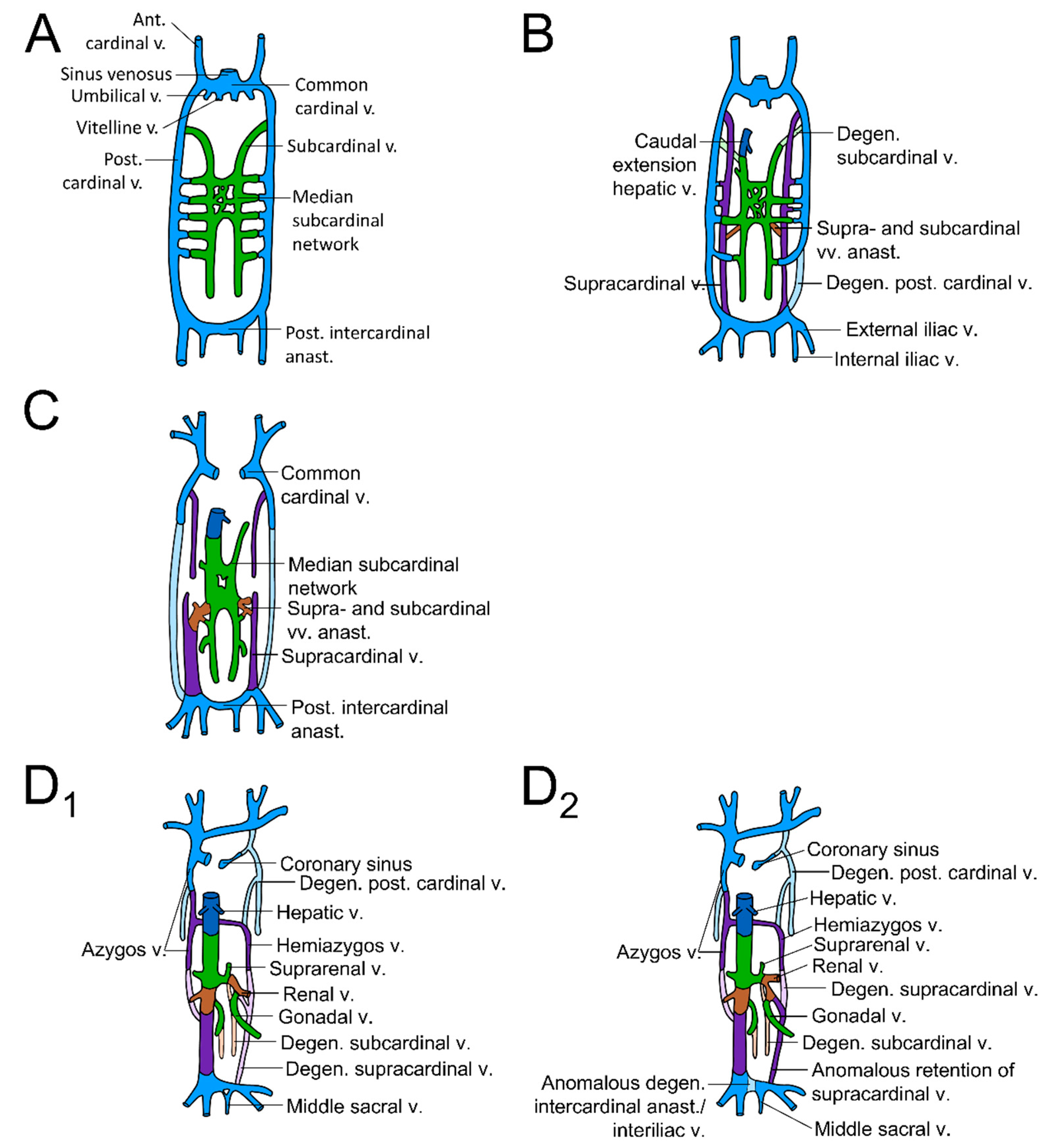
Embryogenesis of the infrahepatic IVC begins in the sixth week and is completed by the eighth week [
2]. Formation of this retroperitoneal venous structure is a complex process derived from three paired fetal venous systems which emerge in the following order: the posterior cardinal, the subcardinal, and the supracardinal veins [
4]. These structures, although initially bilateral, develop into a composite unilateral right-sided intrahepatic IVC. Specifically, the right and left posterior cardinal veins develop first and regress with only their distal elements remaining to form the root of the azygos vein and the common iliac veins (
Figure 2A) [
3,
10,
11]. The right and left subcardinal veins develop next, anteriorly and medially to the posterior cardinal veins, and these veins form the left and right suprarenal veins, the left and right gonadal veins, and additionally a portion of the left RV (specifically the stem of the left RV;
Figure 2A) [
3,
10,
11]. Only the right subcardinal vein persists and forms the suprarenal IVC, while the remainder of the left subcardinal vein ultimately regresses (
Figure 2B) [
3,
11]. A paired set of supracardinal veins develop which follow a similar fate as the subcardinal veins. The left and right supracardinal veins form the azygos and hemiazygos venous system, typically the right supracardinal vein, persists to form the infrarenal IVC while the left supracardinal vein regresses (
Figure 2C) [
3,
10,
11]. Near the kidneys, the supracardinal veins degenerate and the renal segment of the IVC is formed by an anastomosis between the supra- and subcardinal veins [
4].
The final portion of the IVC is the hepatic portion which forms from the right hepatic vein [
4]. Thus, the singular structure known as the IVC exists as composite of four distinct components: (1) the hepatic IVC originating from the hepatic vein, (2) the suprarenal vein originating from the right subcardinal vein, (3) the renal segment arising from the right supracardinal anastomosis, and 4) the infrarenal segment, arising from the right supracardinal anastomosis (
Figure 2(D
1)) [
11]. From this developmental perspective, it is possible to appreciate that persistence of the left supracardinal vein is the primary cause of a duplicated IVC, such as the one found in this donor (
Figure 2(D
2)) [
11]. It should be noted that IVC anomalies occur twice as often in men than in women and thus this finding of such an anomaly in a female cadaver is especially unlikely [
3].
Renal vessels can have anatomical variations in terms of their number, sites of origin, diameter, and relationships amongst each other. Anomalies of the renal veins include retroaortic or circumaortic courses [
12]. However, over the years, anatomical differences within the renal venous system have been far less extensively evaluated compared to the renal arterial system. When these variations do exist, renal venous anatomical variations are relatively less robust compared to the variations found in the renal arteries. Because of these reasons, renal vein variations may be entirely missed or overlooked during imaging [
13].
In utero, the arteries supplying the human gut are distributed segmentally as primitive vitelline arteries that are branches of the aorta. The origins of these vessels either fuse together or obliterate entirely due to the rotation and lengthening of the gut tube as development progresses [
6]. The final result is a reduction in the number of vitelline arteries to three major vessels most commonly seen in reference texts—the CT, SMA, and IMA. Due to this developmentally active period where fusion and obliteration are ongoing, persistent interconnections and variations tend to be relatively common and account for the territorial overlap between these three vessels [
6]. In this case report, the presence of an SMA-derived LCA is interesting as this particular finding accounts for one of the more rarely encountered vascular variants. The incidence of this anomaly alone has been cited at a very low frequency of just 1% [
7]. In addition to this study, only a few other cadaveric case reports [
14,
15] and one clinical case report [
8] are known to have identified aberrancies in the LCA.
The unique cadaveric specimen in this case report possesses several rare accessory renal veins including one relatively close to the inferior pole of the kidney, making this a unique finding during dissection. This finding adds to the pool of the literature pertaining to renal venous anatomical variations which, as described above, is a poorly studied topic with limited information.
4. Conclusions
The DIVC can result in complications during retroperitoneal surgeries and also in interventional radiology procedures and, therefore, identification of this vascular anomaly prior to intervention is critical to minimize patient injury [
2,
3]. Moreover, although DIVC is often asymptomatic, it can be mistaken for lymphadenopathy on radiology, particularly when patients are being examined for a renal malignancy [
2]. Lastly, it has been suggested that presence of a DIVC itself places patients at higher risk for thrombosis and thromboembolic events and that recurrent pulmonary embolisms (despite IVC filter placement) should be cause for consideration of DIVC as evidenced by multiple case reports [
2,
3,
4]. Therefore, understanding the embryologic origin of such anomalies and promoting familiarity with these anatomical anomalies among surgeons and radiologists is vital to minimizing intraoperative complications and misdiagnosis. Variations of the left renal vein are known to heavily influence intraoperative decisions, particularly during renal transplantation, retroperitoneal surgery, and vascular procedures [
12].
Differences among the colic blood supply, as found in this study, are significant as they can influence surgical procedures such as esophageal replacement, colonic conduit surgery, and oncological colon resections [
8]. Furthermore, these aberrations may also play a role in the pathogenesis of pseudoaneurysms involving the colic artery, which themselves are a rare entity [
8]. The possibility of variants in colic blood supply warrants pre-operative 3D reconstruction imaging of these arteries to aid in surgical planning, avoid dilemmas during surgery, and shorten total time spent in the operating room. Additionally, pre-operative imaging prevents accidental ligation of aberrant arteries which would otherwise render the corresponding colic segments ischemic. These highly variable vascular patterns highlight the need for physicians to understand and anticipate anomalies in vascular anatomy which may cause complications during surgical and diagnostic procedures [
8,
14,
15,
16].






{kind=link}
{kind=link}