
Technology Readiness Level of Robotic Technology and Artificial Intelligence in Dentistry: A Comprehensive Review

 ,
, 
 and
and 
Abstract
:1. Introduction
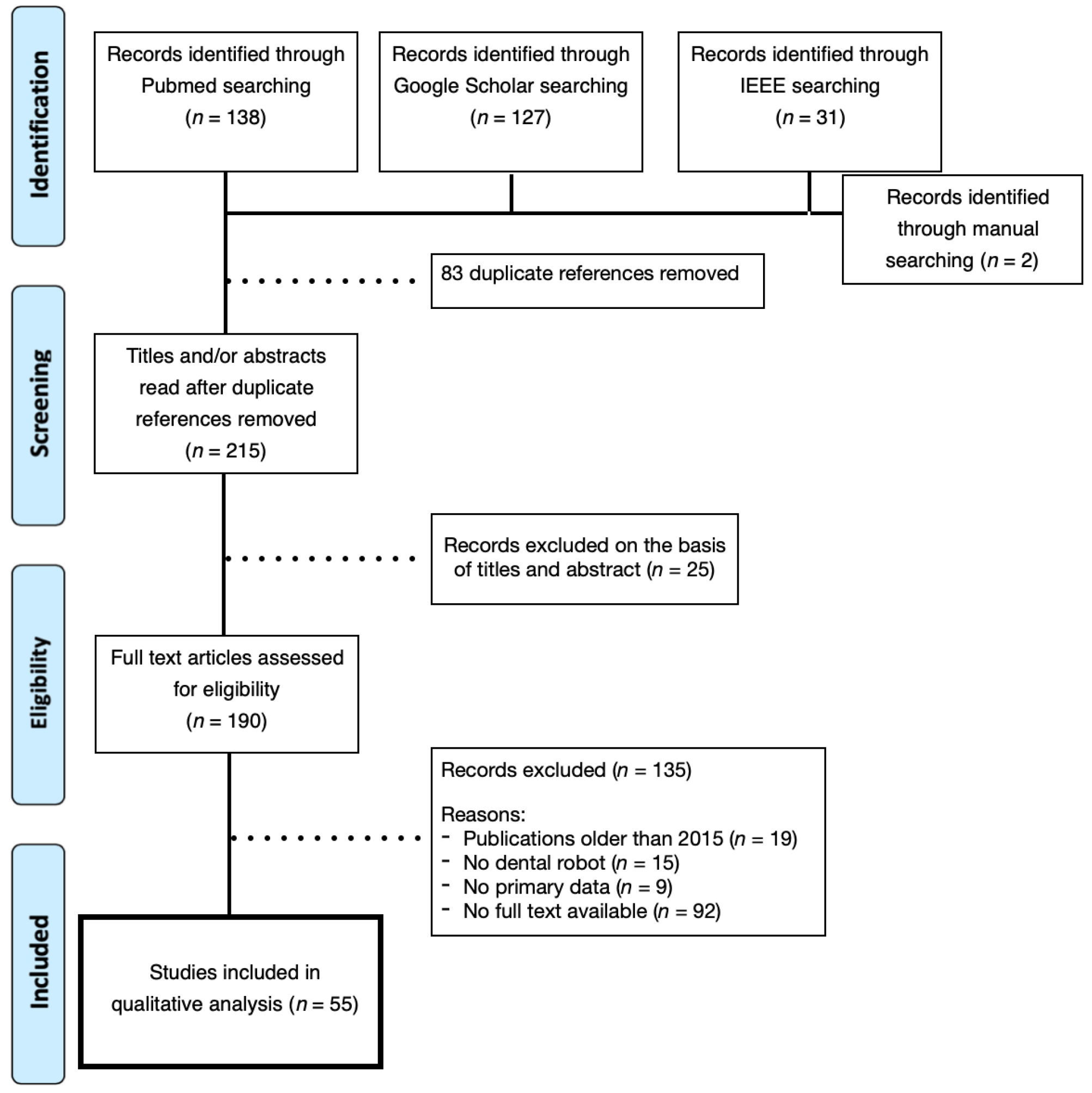
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Selection of Articles and Information Extraction
3. Results
3.1. Study Selection
3.2. Study Demography
3.3. Robotics Results per Field of Dentistry
3.3.1. Orthodontics
3.3.2. Implantology and Surgery
3.4. AI Results per Fields of Dentistry
3.4.1. AI in Orthodontics
3.4.2. AI in Dental Radiology
3.4.3. AI in Dental Implantology
3.4.4. Technology Readiness Level
4. Discussion
4.1. Summary of Results
4.2. Pediatric Dentistry
4.3. Collaborations
4.4. Dental Education
4.5. Limitations
4.6. Risks
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Almurib, H.A.; Al-Qrimli, H.F.; Kumar, N. A review of application industrial robotic design. In Proceedings of the 2011 Ninth International Conference on ICT and Knowledge Engineering, Bangkok, Thailand, 12–13 January 2012; pp. 105–112. [Google Scholar]
- Liu, L.; Watanabe, M.; Ichikawa, T. Robotics in Dentistry: A Narrative Review. Dent. J. 2023, 11, 62. [Google Scholar] [CrossRef] [PubMed]
- Kwoh, Y.S.; Hou, J.; Jonckheere, E.A.; Hayati, S. A robot with improved absolute positioning accuracy for CT guided sterotactic brain surgery. IEEE Trans. Biomed. Eng. 1988, 35, 153–160. [Google Scholar] [CrossRef]
- Yuan, F.; Lyu, P. A preliminary study on a tooth preparation robot. Adv. Appl. Ceram. 2019, 119, 332–337. [Google Scholar] [CrossRef]
- Abe, S.; Noguchi, N.; Matsuka, Y.; Shinohara, C.; Kimura, T.; Oka, K.; Okura, K.; Rodis, O.M.M.; Kawano, F. Educational effects using a robot patient simulation system for development of clinical attitude. Eur. J. Dent. Educ. 2018, 22, e327–e336. [Google Scholar] [CrossRef] [PubMed]
- van Riet, T.C.; Sem, K.T.C.J.; Ho, J.P.T.; Spijker, R.; Kober, J.; de Lange, J. Robot technology in dentistry, part one of a systematic review: Literature characteristics. Dent. Mater. 2021, 37, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Grischke, J.; Johannsmeier, L.; Eich, L.; Griga, L.; Haddadin, S. Dentronics: Towards robotics and artificial intelligence in dentistry. Dent. Mater. 2020, 36, 765–778. [Google Scholar] [CrossRef] [PubMed]
- Pereira, K.R.; Sinha, R. Welcome the “new kid on the block” into the family: Artificial intelligence in oral and maxillofacial surgery. Br. J. Oral Maxillofac. Surg. 2020, 58, 83–84. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, F.; Fan, S.; Chow, J.K. Robotics in dental implantology. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 513–518. [Google Scholar] [CrossRef]
- Amm, E.W. Clinical outcomes for patients finished with the SureSmileTM method compared with conventional fixed orthodontic therapy. Angle Orthod. 2011, 81, 926. [Google Scholar]
- Sachdeva, R.C.; Aranha, S.L.; Egan, M.E.; Gross, H.T.; Sachdeva, N.S.; Currier, G.F.; Kadioglu, O. Treatment time: SureSmile vs. conventional. Orthodontics 2012, 13, 72–85. [Google Scholar]
- Saxe, A.K.; Louie, L.J.; Mah, J. Efficiency and effectiveness of SureSmile. World J. Orthod. 2010, 11, 16–22. [Google Scholar] [PubMed]
- Xia, Z.; Deng, H.; Weng, S.; Gan, Y.; Xiong, J.; Wang, H. Development of a robotic system for orthodontic archwire bending. In Proceedings of the 2016 IEEE International Conference on Robotics and Automation (ICRA), Stockholm, Sweden, 16–21 May 2016; pp. 730–735. [Google Scholar]
- Larson, B.E.; Vaubel, C.J.; Grünheid, T. Effectiveness of computer-assisted orthodontic treatment technology to achieve predicted outcomes. Angle Orthod. 2013, 83, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.L.; Kusnoto, B.; Galang-Boquiren, M.T.; BeGole, E.; Obrez, A. Mesiodistal tip and faciolingual torque outcomes in computer-driven orthodontic appliances. J. World Fed. Orthod. 2015, 4, 63–70. [Google Scholar] [CrossRef]
- Muller-Hartwich, R.; Jost-Brinkmann, P.G.; Schubert, K. Precision of implementing virtual setups for orthodontic treatment using CAD/CAM-fabricated custom archwires. J. Orofac. Orthop. 2016, 77, 1. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.; Xia, Z.; Weng, S.; Gan, Y.; Xiong, J.; Ou, Y.; Zhang, J. Motion planning and control of a robotic system for orthodontic archwire bending. In Proceedings of the 2015 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Hamburg, Germany, 28 September–2 October 2015. [Google Scholar]
- Abutayyem, H.; Alsalam, A.A.A.; Iqbal, R.M.; Alkhabuli, J.; El-Din Mohamed, S.K. Robotic use in orthodontics: Literature review. Oral Health Dent. Sci. 2019, 3, 1–5. [Google Scholar] [CrossRef]
- Vaishnavi, D.; Sheethal, J.; Kishore, K. Robotic wire bending in orthodontics. Dentistry 2021, 11, 584. [Google Scholar]
- Kumar, P.; Dixit, P.; Kalaivani, V.; Rajapandian, K. Future advances in robotic dentistry. J. Dent. Health Oral. Disord. Ther. 2017, 7, 00241. [Google Scholar] [CrossRef]
- Mozer, P.S. Accuracy and deviation analysis of static and robotic guided implant surgery: A case study. Int. J. Oral. Maxillofac. Implant. 2020, 35, e86–e90. [Google Scholar] [CrossRef] [PubMed]
- Yeotikar, S.; Parimi, A.M.; Daseswar Rao, Y.V. Automation of end effector guidance of robotic arm for dental implantation using computer vision. In Proceedings of the 2016 IEEE Distributed Computing, VLSI, Electrical Circuits and Robotics (DISCOVER), Mangalore, India, 13–14 August 2016; pp. 84–89. [Google Scholar]
- Yu, K.; Uozumi, S.; Ohnishi, K.; Usuda, S.; Kawana, H.; Nakagawa, T. Stereo vision based robot navigation system using modulated potential field for implant surgery. In Proceedings of the 2015 IEEE International Conference on Industrial Technology (ICIT), Seville, Spain, 17–19 March 2015; pp. 493–498. [Google Scholar]
- Yu, K.; Ohnishi, K.; Kawana, H.; Usuda, S. Modulated potential Field using 5 DoF implant assist robot for position and angle adjustment. In Proceedings of the IECON 2015—41st Annual Conference of the IEEE Industrial Electronics Society, Yokohama, Japan, 9–12 November 2015; pp. 002166–002171. [Google Scholar]
- Yuan, F.S.; Zheng, J.Q.; Zhang, Y.P.; Wang, Y.; Sun, Y.C.; Lyu, P.J. Preliminary study on the automatic preparation of dental implant socket controlled by micro-robot. Chin. J. Dent. Res. 2018, 53, 524–528. [Google Scholar]
- Meleshnikov, A.M.; Vorotnikov, A.A.; Klimov, D.D.; Poduraev, Y.V. Prototype probe determining waveguide–Gum contact for a robot surgical system. Russ. Eng. Res. 2020, 40, 86–88. [Google Scholar] [CrossRef]
- van Riet, T.C.; Sem, K.T.C.J.; Ho, J.P.T.; Spijker, R.; Kober, J.; de Lange, J. Robot technology in dentistry, part two of a systematic review: An overview of initiatives. Dent. Mater. 2021, 37, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; McKenzie, F.D.; Bawab, S.; Li, J.; Yoon, Y.; Huang, J.-K. Automated dental implantation using image-guided robotics: Registration results. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Shen, Z.; Xu, W.Y.T.; Lam, W.Y.H.; Hsung, R.T.C.; Pow, E.H.N.; Kosuge, K.; Wang, Z. A compact dental robotic system using soft bracing technique. IEEE Robot. Autom. Lett. 2019, 4, 1271–1278. [Google Scholar] [CrossRef]
- Bolding, S.L.; Reebye, U.N. Accuracy of haptic robotic guidance of dental implant surgery for completely edentulous arches. J. Prosthet. Dent. 2021, 128, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.; Zhang, W.; Cai, L.; Zheng, L.; Bao, K.; Rao, Y.; Yang, L.; Ye, W.; Guan, P.; Yang, W.; et al. Optics-guided Robotic System for Dental Implant Surgery. Chin. J. Mech. Eng. 2022, 35, 55. [Google Scholar] [CrossRef]
- Rao, Y.V.D.; Parimi, A.M.; Rahul, D.S.P.; Patel, D.; Nitin Mythreya, Y.V. Robotics in dental implantation. Mater. Today Proc. 2017, 4, 9327–9332. [Google Scholar] [CrossRef]
- Thanathornwong, B. Bayesian-Based Decision Support System for Assessing the Needs for Orthodontic Treatment. Healthc. Inform. Res. 2018, 24, 22–28. [Google Scholar] [CrossRef]
- Kim, H.; Shim, E.; Park, J.; Kim, Y.J.; Lee, U.; Kim, Y. Web-based fully automated cephalometric analysis by deep learning. Comput. Methods Programs Biomed. 2020, 194, e105513. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Liu, Y.; Oh, S.H.; Ahn, H.W.; Kim, S.H.; Nelson, G. Evaluation of a multi-stage convolutional neural network-based fully automated landmark identification system using cone-beam computed tomography synthesized posteroanterior cephalometric images. Korean J. Orthod. 2021, 51, 77–85. [Google Scholar] [CrossRef]
- Jung, S.K.; Kim, T.W. New approach for the diagnosis of extractions with neural network machine learning. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 127–133. [Google Scholar] [CrossRef]
- Tanikawa, C.; Yamashiro, T. Development of novel artificial intelligence systems to predict facial morphology after orthognathic surgery and orthodontic treatment in Japanese patients. Sci. Rep. 2021, 11, 15853. [Google Scholar] [CrossRef] [PubMed]
- Park, W.J.; Park, J.B. History and application of artificial neural networks in dentistry. Eur. J. Dent. 2018, 12, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Ezhov, M.; Gusarev, M.; Golitsyna, M.; Yates, J.M.; Kushnerev, E.; Tamimi, D.; Aksoy, S.; Shumilov, E.; Sanders, A.; Orhan, K. Clinically applicable artificial intelligence system for dental diagnosis with CBCT. Sci. Rep. 2021, 11, 15006, Erratum in Sci. Rep. 2021, 11, 22217. [Google Scholar] [CrossRef] [PubMed]
- Hiraiwa, T.; Ariji, Y.; Fukuda, M.; Kise, Y.; Nakata, K.; Katsumata, A.; Fujita, H.; Ariji, E. A deep-learning artificial intelligence system for assessment of root morphology of the mandibular first molar on panoramic radiography. Dentomaxillofacial Radiol. 2019, 48, 20180218. [Google Scholar] [CrossRef] [PubMed]
- Setzer, F.C.; Shi, K.J.; Zhang, Z.; Yan, H.; Yoon, H.; Mupparapu, M.; Li, J. Artificial intelligence for the computer-aided detection of periapical lesions in cone-beam computed tomographic images. J. Endod. 2020, 46, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Johari, M.; Esmaeili, F.; Andalib, A.; Garjani, S.; Saberkari, H. Detection of vertical root fractures in intact and endodontically treated premolar teeth by designing a probabilistic neural network: An ex vivo study. Dentomaxillofacial Radiol. 2017, 46, 20160107. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.-J.; Yun, J.-P.; Yeom, H.-G.; Shin, W.-S.; Lee, J.-H.; Jeong, S.-H.; Seo, M.-S. Deep-learning for predicting C-shaped canals in mandibular second molars on panoramic radiographs. Dentomaxillofacial Radiol. 2021, 50, 20200513. [Google Scholar] [CrossRef]
- Qiao, X.; Zhang, Z.; Chen, X. Multifrequency impedance method based on neural network for root canal length measurement. Appl. Sci. 2020, 10, 7430. [Google Scholar] [CrossRef]
- Lee, J.H.; Jeong, S.N. Efficacy of deep convolutional neural network algorithm for the identification and classification of dental implant systems, using panoramic and periapical radiographs: A pilot study. Medicine 2020, 99, e20787. [Google Scholar] [CrossRef]
- Elgarba, B.M.; Van Aelst, S.; Swaity, A.; Morgan, N.; Shujaat, S.; Jacobs, R. Deep learning-based segmentation of dental implants on cone-beam computed tomography images: A validation study. J. Dent. 2023, 137, 104639. [Google Scholar] [CrossRef]
- Roy, S.; Dey, S.; Khutia, N.; Roy Chowdhury, A.; Datta, S. Design of patient specific dental implant using FE analysis and computational intelligence techniques. Appl. Soft Comput. 2018, 65, 272–279. [Google Scholar] [CrossRef]
- Li, H.; Shi, M.; Liu, X.; Shi, Y. Uncertainty optimization of dental implant based on finite element method, global sensitivity analysis and support vector regression. Proc. Inst. Mech. Eng. Part H 2019, 233, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Lin, C.H.; Hu, Y.H.; You, Z.H. Predicting the failure of dental implants using supervised learning techniques. Appl. Sci. 2018, 8, 698. [Google Scholar] [CrossRef]
- Jiang, J.; Chen, H.; Ma, X.; Zhang, Y.; Liu, Y. Forming planning method and experimentation of personalized orthodontic archwires. Zhongguo Jixie Gongcheng/China Mech. Eng. 2020, 11, 1323–1330, 1336. [Google Scholar]
- Zhang, Y.; Jia, X.; Jiang, J.; Liu, Y.; Wang, Y. Simulation and analysis of orthodontic archwire bending robot. Int. J. Smart Home 2016, 10, 263–270. [Google Scholar] [CrossRef]
- Jiang, J.G.; Bo, P.; Yong De, Z.; Xiao Yang, Y.; Yi, L.; Bei Xin, S. Control system of orthodontic archwire bending robot based on LabVIEW and ATmega2560. Int. J. Control. Autom. 2016, 9, 189–198. [Google Scholar] [CrossRef]
- Jiang, J.G.; Han, Y.S.; Zhang, Y.D.; Liu, Y.J.; Wang, Z.; Liu, Y. Springback mechanism analysis and experiments on robotic bending of rectangular orthodontic archwire. Chin. J. Mech. Eng. 2017, 30, 1406–1415. [Google Scholar] [CrossRef]
- Jiang, J.; Ma, X.; Zhang, Y.; Huo, B.; Liu, Y. Study on three-dimensional digital expression and robot bending method of orthodontic archwire. Appl. Bionics Biomech. 2018, 2018, 2176478. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Yang, J.; Tan, Y.; Hu, J.; Liu, D.; Zhu, J. An intelligent dental robot. Adv. Robot. 2018, 32, 659–669. [Google Scholar] [CrossRef]
- Otani, T.; Raigrodski, A.J.; Mancl, L.; Kanuma, I.; Rosen, J. In vitro evaluation of accuracy and precision of automated robotic tooth preparation system for porcelain laminate veneers. J. Prosthet. Dent. 2015, 114, 229–235. [Google Scholar] [CrossRef]
- Yuan, F.; Zheng, J.; Sun, Y.; Wang, Y.; Lyu, P. Regulation and measurement of the heat generated by automatic tooth preparation in a confined space. Photomed. Laser Surg. 2017, 35, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Yuan, F.; Wang, Y.; Zhang, Y.; Sun, Y.; Wang, D.; Lyu, P. An automatic tooth preparation technique: A preliminary study. Sci. Rep. 2016, 6, 25281. [Google Scholar] [CrossRef] [PubMed]
- Araie, T.; Ikeda, T.; Nishizawa, U.; Kakimoto, A.; Toyama, S.; Ragulskis, M. Study of the chewing assistance mechanism in powered robotic dentures. Vibroengineering Procedia 2018, 19, 163–168. [Google Scholar] [CrossRef]
- Kizghin, D.A.; Nelson, C.A. Optimal design of a parallel robot for dental articulation. In Proceedings of the 2019 Design of Medical Devices Conference, Minneapolis, MN, USA, 15–18 April 2019. [Google Scholar]
- Carossa, M.; Cavagnetto, D.; Ceruti, P.; Mussano, F.; Carossa, S. Individual mandibular movement registration and reproduction using an optoeletronic jaw movement analyzer and a dedicated robot: A dental technique. BMC Oral Health 2020, 20, 271. [Google Scholar] [CrossRef] [PubMed]
- Bula, I.; Hajrizi, E. Cost oriented autonomous mobile service robot. IFAC PapersOnLine 2019, 52, 91–94. [Google Scholar] [CrossRef]
- Li, J.; Lam, W.Y.H.; Chiu Hsung, R.T.; Pow, E.H.N.; Wang, Z. A customizable, compact robotic manipulator for assisting multiple dental procedures. In Proceedings of the 2018 3rd International Conference on Advanced Robotics and Mechatronics (ICARM), Singapore, 18–20 July 2018; pp. 720–725. [Google Scholar]
- Li, J.; Lam, W.Y.H.; Hsung, R.T.C.; Pow, E.H.N.; Wu, C.; Wang, Z. Control and motion scaling of a compact cable-driven dental robotic manipulator. In Proceedings of the 2019 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM), Hong Kong, China, 8–12 July 2019; pp. 1002–1007. [Google Scholar]
- Iijima, T.; Matsunaga, T.; Shimono, T.; Ohnishi, K.; Usuda, S.; Kawana, H. Development of a multi DOF haptic robot for dentistry and Oral surgery. In Proceedings of the 2020 IEEE/SICE International Symposium on System Integration (SII), Honolulu, HI, USA, 12–15 January 2020; pp. 52–57. [Google Scholar]
- Li, J.; Lam, J.; Liu, M.; Wang, Z. Compliant control and compensation for a compact cable-driven robotic manipulator. IEEE Robot. Autom. Lett. 2020, 5, 5417–5424. [Google Scholar] [CrossRef]
- Tao, Y.; Zhang, T.; Xu, W.; Tsang, H.Y.; Li, J.; Wang, Z. A compact asymmetrical manipulator for robotic dentistry. In Proceedings of the 9th IEEE International Conference on CYBER Technology in Automation, Control and Intelligent Systems, Suzhou, China, 29 July–2 August 2019; pp. 164–168. [Google Scholar]
- Yu, K.; Matsunaga, T.; Kawana, H.; Usuda, S.; Ohnishi, K. Frequency-based analysis of the relationship between cutting force and CT number for an implant-surgery-teaching robot. IEEJ J. Ind. Appl. 2017, 6, 66–72. [Google Scholar] [CrossRef]
- Kasimoglu, Y.; Kocaaydin, S.; Karsli, E.; Esen, M.; Bektas, I.; Ince, G.; Tuna, E.B. Robotic approach to the reduction of dental anxiety in children. Acta Odontol. Scand. 2020, 78, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Yasemin, M.; Kasımoğlu, Y.; Kocaaydin, S.; Karsli, E.; Ince, E.B.T.; Ince, G. Management of dental anxiety in children using robots. In Proceedings of the 2016 24th Signal Processing and Communication Application Conference (SIU), Zonguldak, Turkey, 16–19 May 2016; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2016. [Google Scholar]
- Razavi, M.; Talebi, H.A.; Zareinejad, M.; Dehghan, M.R. A GPU-implemented physics-based haptic simulator of tooth drilling. Int. J. Med. Robot. Comput. Assist. Surg. 2015, 11, 476–485. [Google Scholar] [CrossRef]
- van der Meer, W.J.; Vissink, A.; Ng, Y.L.; Gulabivala, K. 3D Computer aided treatment planning in endodontics. J. Dent. 2016, 45, 67–72. [Google Scholar] [CrossRef]
- De Ceulaer, J.; De Clercq, C.; Swennen, G.R. Robotic surgery in oral and maxillofacial, craniofacial and head and neck surgery: A systematic review of the literature. Int. J. Oral. Maxillofac. Surg. 2012, 41, 1311–1324. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, K.; Kunte, S.; Patil, K.; Shah, P.P.; Shah, R.V.; Jajoo, S.S. Artificial Intelligence in Pediatric Dentistry—A Systematic Review. J. Dent. Res. Rev. 2023, 10, 7–12. [Google Scholar] [CrossRef]
- Vishwanathaiah, S.; Fageeh, H.; Khanagar, S.; Maganur, P.C. Artificial Intelligence Its Uses and Application in Pediatric Dentistry: A Review. Biomedicines 2023, 11, 788. [Google Scholar] [CrossRef] [PubMed]
- Kolibree. Brushing Gets Better When You Hum. Available online: https://www.kolibree.com/en (accessed on 17 March 2024).
- Dave, M.; Patel, N. Artificial intelligence in healthcare and education. Br. Dent. J. 2023, 234, 761–764. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Strunga, M.; Urban, R.; Surovková, J.; Afrashtehfar, K.I. Impact of Artificial Intelligence on Dental Education: A Review and Guide for Curriculum Update. Educ. Sci. 2023, 13, 150. [Google Scholar] [CrossRef]
- Schwendicke, F.; Chaurasia, A.; Wiegand, T.; Uribe, S.E.; Fontana, M.; Akota, I.; Tryfonos, O.; Krois, J. Artificial intelligence for oral and dental healthcare: Core education curriculum. J. Dent. 2023, 128, 104363. [Google Scholar] [CrossRef] [PubMed]
- Harvard School of Dental Medicine. Exploring How AI Can Enhance Dental Education. 12 March 2024. Available online: https://hsdm.harvard.edu/news/exploring-how-ai-can-enhance-dental-education (accessed on 15 March 2024).
- Saghiri, M.A.; Vakhnovetsky, J.; Nadershahi, N. Scoping review of artificial intelligence and immersive digital tools in dental education. J. Dent. Educ. 2022, 86, 736–750. [Google Scholar] [CrossRef]
- Kavadella, A.; da Silva, M.A.D.; Kaklamanos, E.G.; Stamatopoulos, V.; Giannakopoulos, K. Evaluation of ChatGPT’s Real-Life Implementation in Undergraduate Dental Education: Mixed Methods Study. JMIR Med. Educ. 2024, 10, e51344. [Google Scholar] [CrossRef]
- What Is Explainable AI? Available online: https://www.ibm.com/topics/explainable-ai (accessed on 18 February 2024).


{kind=link}
{kind=link}
| Author and Year | Purpose | AI Techniques | Accuracy |
|---|---|---|---|
| Thanthornwong et al., 2018 [33] | Orthodontic treatment assessment | Bayesian-based decision support system | 96% |
| Kim et al., 2021 [35] | Posteroanterior (PA) cephalometric landmark analysis | Multi-stage CNN | 88.43% (lateral cephalograms), 80.4% (CBCT) |
| Jung et al., 2016 [36] | Diagnosis of extractions | Neural network machine learning | 93% (identification of patients needing extractions), 84% (extraction plan) |
| Tanikawa et al., 2021 [37] | Prediction of facial morphology after orthognathic surgery and orthodontic treatment | Landmark-based geometric morphometric methods (GMMs), deep learning | 81% at a system error of <1 mm, 100% at a system error of <2% |
| Author and Year | Purpose | Diagnostic Techniques | AI Methods | Accuracy |
|---|---|---|---|---|
| Setzer et al., 2020 [41] | Periapical lesion diagnosis | CBCT | Deep learning algorithm | 93% |
| Johari et al., 2017 [42] | Vertical root fracture diagnosis | Periapical radiographs | PNN | 96.6% |
| Jeon et al., 2021 [43] | Root canal morphology | Panoramic radiography | CNN-based DL | 95.1% |
| Qiao et al., 2020 [44] | Root canal length measurement | Circuit system | Neural network model | 95% |
| Author and Year | Purpose | Conventional Technique | AI Methods |
|---|---|---|---|
| Elgarba et al., 2023 [46] | Segmentation of dental implants | Automated segmentation (AS) | CNN |
| Roy et al., 2018 [47] | Design of dental implants | Finite element analysis | Genetic algorithm, ANN |
| Li et al., 2019 [48] | Reduction in stress at the implant–bone interface | Finite element method | Support vector regression, k-sigma method, interval method |
| Liu et al., 2018 [49] | Prediction of dental implant failure | Statistical correlation significance analysis | Decision tree (DT), support vector machines, logistic regressions, bagging, and AdaBoost |
| Technology Readiness Level | Description |
|---|---|
| 1 | Basic Principles Observed |
| 2 | Technology Concept Formulated |
| 3 | Experimental Proof of Concept |
| 4 | Technology Validated in Laboratory Environment |
| 5 | Technology Validated in Relevant Environment |
| 6 | System Demonstrated in Relevant Environment |
| 7 | System Prototype Demonstrated in Operational Environment |
| 8 | Actual System Completed and Qualified |
| 9 | Full-Scale Deployment |
| Fields | Discovery | Development | Demonstration | Deployment | Number of Articles per Field | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| TRL | ||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | ||
| Orthodontics | [50,51,52,53,54] | [13,17] | [14,15] | 9 | ||||||
| Implantology and surgery | [26,32] | [22,23,24,25,27] | [21] | 8 | ||||||
| Prosthodontics | [55] | 1 | ||||||||
| Restorative dentistry | [4,56] | [52,57,58] | 5 | |||||||
| Gnathology | [59,60] | [61] | 3 | |||||||
| General practice | [62] | [29,63,64,65,66,67] | 7 | |||||||
| Education of students | [68] | [9] | 2 | |||||||
| Education of patients | [69] | [70] | 2 | |||||||
| Endodontics | [71] | [72] | 2 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nassani, L.M.; Javed, K.; Amer, R.S.; Pun, M.H.J.; Abdelkarim, A.Z.; Fernandes, G.V.O. Technology Readiness Level of Robotic Technology and Artificial Intelligence in Dentistry: A Comprehensive Review. Surgeries 2024, 5, 273-287. https://doi.org/10.3390/surgeries5020025
Nassani LM, Javed K, Amer RS, Pun MHJ, Abdelkarim AZ, Fernandes GVO. Technology Readiness Level of Robotic Technology and Artificial Intelligence in Dentistry: A Comprehensive Review. Surgeries. 2024; 5(2):273-287. https://doi.org/10.3390/surgeries5020025
Chicago/Turabian StyleNassani, Leonardo Mohamad, Kanza Javed, Rafat Samih Amer, Ming Hong Jim Pun, Ahmed Z. Abdelkarim, and Gustavo Vicentis Oliveira Fernandes. 2024. "Technology Readiness Level of Robotic Technology and Artificial Intelligence in Dentistry: A Comprehensive Review" Surgeries 5, no. 2: 273-287. https://doi.org/10.3390/surgeries5020025
APA StyleNassani, L. M., Javed, K., Amer, R. S., Pun, M. H. J., Abdelkarim, A. Z., & Fernandes, G. V. O. (2024). Technology Readiness Level of Robotic Technology and Artificial Intelligence in Dentistry: A Comprehensive Review. Surgeries, 5(2), 273-287. https://doi.org/10.3390/surgeries5020025