
Histopathological and Quantitative Lesions of the Cardiac Conduction System and Its Vascularization Related to Chronic Cocaine Abusers and Sudden Unexpected Death

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cases
2.2. Histological Examination of the Cardiac Conduction System and Its Vascularization
2.3. Morphometry and Image Analysis
2.4. Data Analysis
3. Results
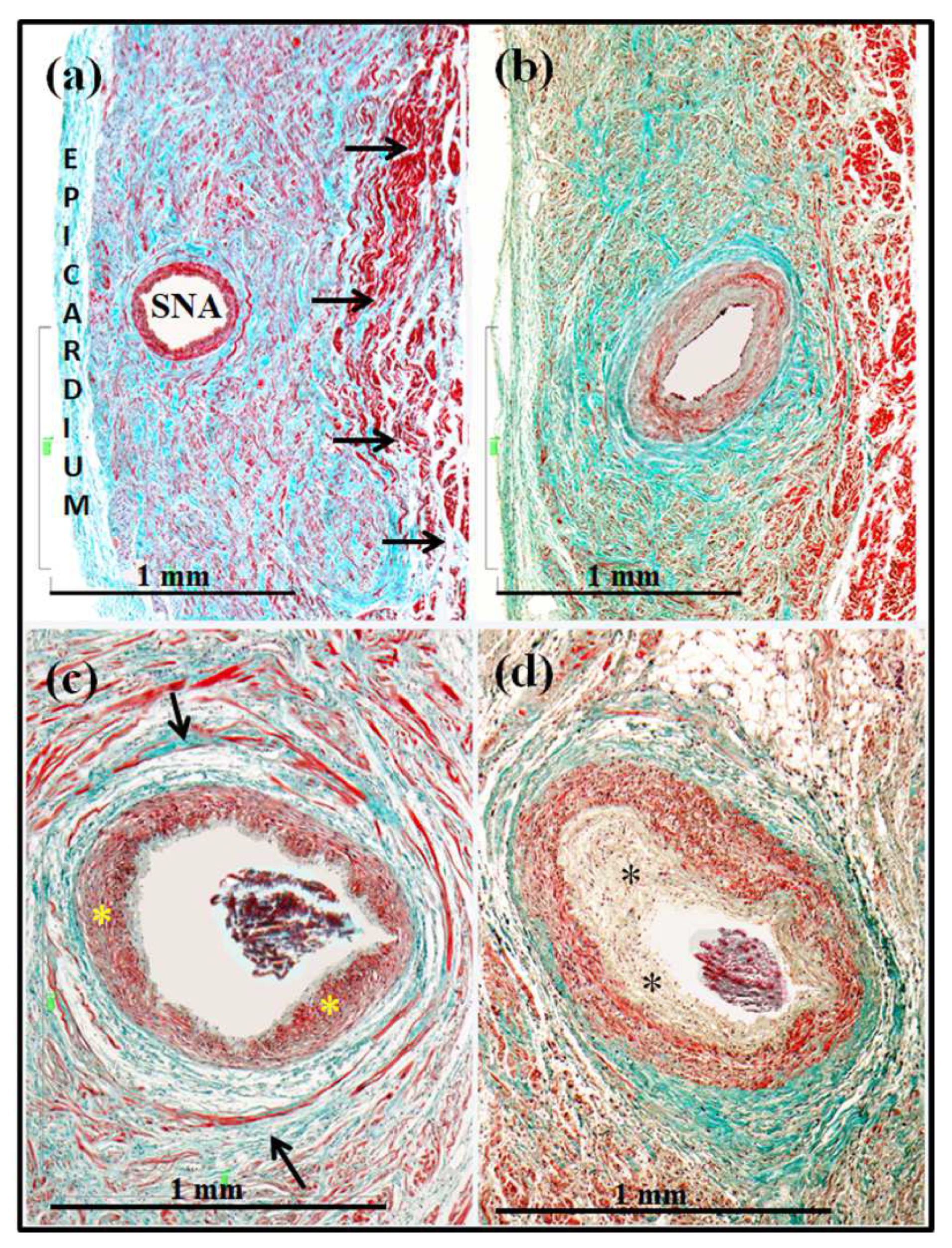
3.1. Sinus Node and Artery
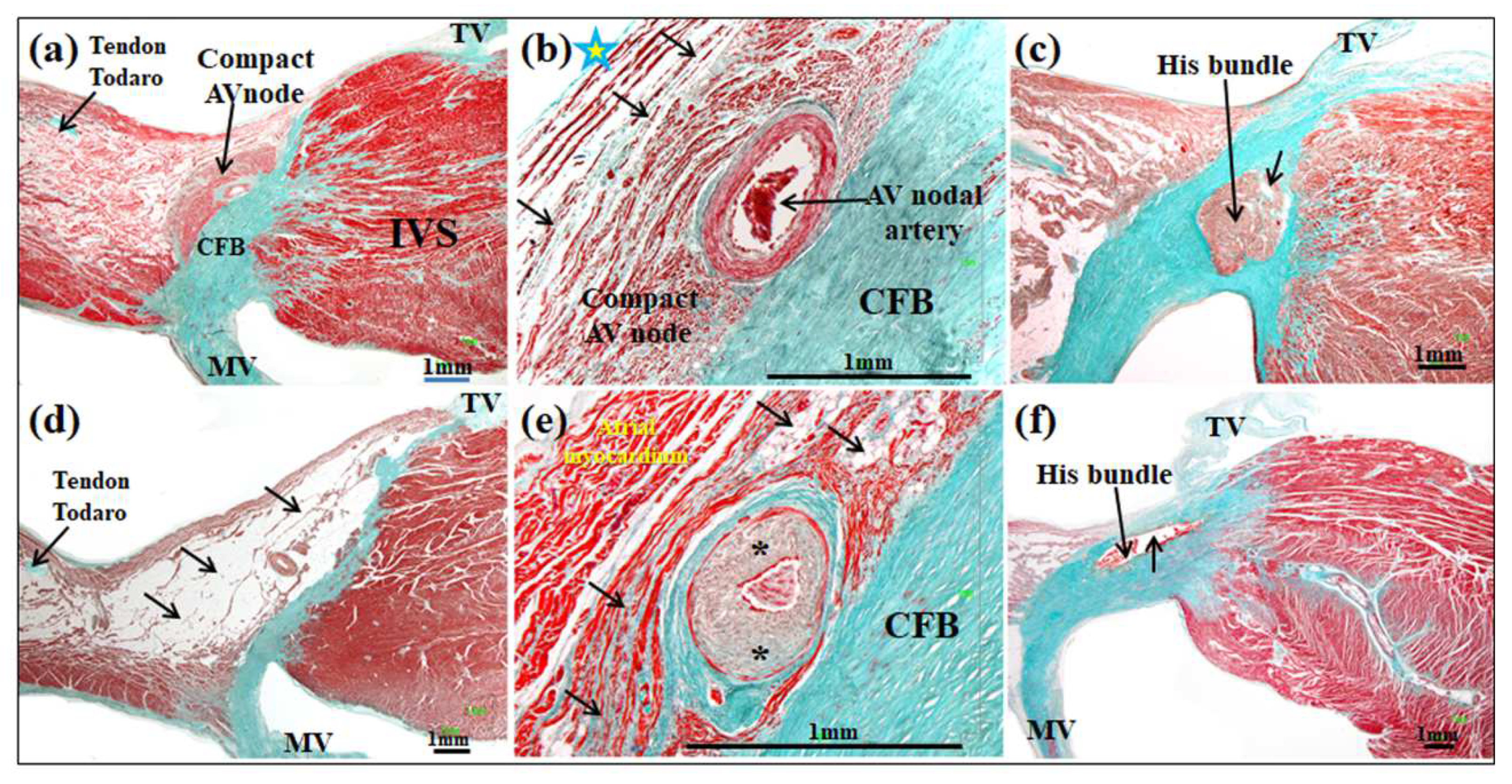
3.2. Atrioventricular Conduction System and Vascularization
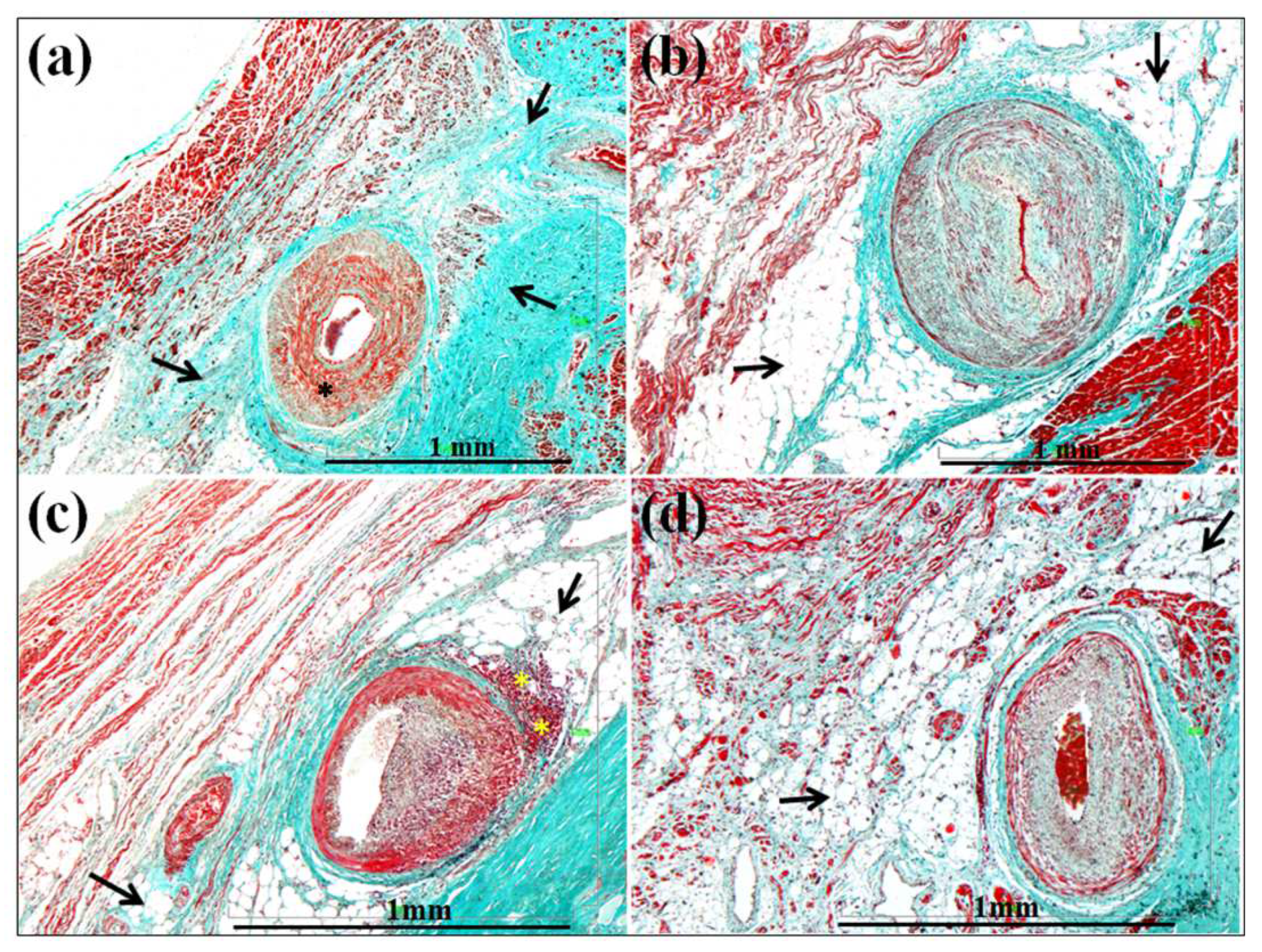
3.3. Affectation of the Walls and Lumen of the Small Intramyocardial Vessels
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- UNODC. World Drug Report. 2018. Available online: https://www.unodc.org/wdr2018/prelaunch/WDR18_Booklet_1_EXSUM.pdf (accessed on 9 October 2019).
- Karch, S.B. Cocaine and the heart: Clinical and pathological correlations. Adv. Biosci. 1991, 80, 211–218. [Google Scholar]
- Qureshi, A.I.; Suri, M.F.; Guterman, L.R.; Hopkins, L.N. Cocaine use and the likelihood of nonfatal myocardial infarction and stroke: Data from the third national health and nutrition examinations survey. Circulation 2001, 103, 502–506. [Google Scholar] [CrossRef] [Green Version]
- Egred, M.; Davis, G.K. Cocaine and the heart. Postgrad. Med. J. 2005, 81, 568–571. [Google Scholar] [CrossRef]
- Liaudet, L.; Calderari, B.; Pacher, P. Pathophysiological mechanisms of catecholamine and cocaine-mediated cardiotoxicity. Heart Fail. Rev. 2014, 19, 815–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.N.; Chang, H.D.; Sung, R.J. Cocaine-induced inhibition of ATP-sensitive K+ channels in rat ventricular myocytes and in heart-derived H9c2 cells. Basic Clin. Pharmacol. Toxicol. 2006, 98, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Reyes, S.; Kane, G.C.; Zingman, L.V.; Yamada, S.; Terzic, A. Targeted disruption of K(ATP) channels aggravates cardiac toxicity in cocaine abuse. Clin. Transl. Sci. 2009, 2, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Crumb, W.J., Jr.; Clarkson, C.W. Characterization of cocaine-induced block of cardiac sodium channels. Biophys. J. 1990, 57, 589–599. [Google Scholar] [CrossRef] [Green Version]
- Renard, D.C.; Delaville, F.J.; Thomas, A.P. Inhibitory effects of cocaine on Ca2+ transients and contraction in single cardiomyocytes. Am. J. Physiol. 1994, 266 Pt 2, H555–H567. [Google Scholar] [CrossRef] [PubMed]
- Sharma, J.; Rathnayaka, N.; Green, C.; Moeller, F.G.; Schmitz, J.M.; Shoham, D.; Dougherty, A.H. Bradycardia as a marker of chronic cocaine use: A novel cardiovascular finding. Behav. Med. 2016, 42, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackman, W.M.; Friday, K.J.; Anderson, J.L.; Aliot, E.M.; Clark, M.; Lazzara, R. The long QT syndromes: A critical review, new clinical observations and a unifying hypothesis. Prog. Cardiovasc. Dis. 1988, 31, 115–172. [Google Scholar] [CrossRef]
- Gupta, A.; Lawrence, A.T.; Krishnan, K.; Kavinsky, C.J.; Trohman, R.G. Current concepts in the mechanisms and management of drug-induced QT prolongation and torsade de pointes. Am. Heart J. 2007, 153, 891–899. [Google Scholar] [CrossRef]
- Atkinson, T.S.; Sanders, N.; Mancino, M.; Oliveto, A. Effects of disulfiram on QTc interval in non-opioid-dependent and methadone-treated cocainedependent patients. J. Addict. Med. 2013, 7, 243–248. [Google Scholar] [CrossRef]
- Virmani, R.; Robinowitz, M.; Smialek, J.E.; Smyth, D.F. Cardiovascular effects of cocaine: An autopsy study of 40 patients. Am. Heart J. 1988, 115, 1068–1076. [Google Scholar] [CrossRef]
- Winek, C.L.; Wahba, W.W.; Winek, C.L., Jr.; Balzer, T.W. Drug and chemical blood-level data 2001. Forensic Sci. Int. 2001, 122, 107–123. [Google Scholar] [CrossRef]
- Bauman, J.L.; Grawe, J.J.; Winecoff, A.P.; Hariman, R.J. Cocaine-related sudden cardiac death: A hypothesis correlating basic science and clinical observations. J. Clin. Pharmacol. 1994, 34, 902–911. [Google Scholar] [CrossRef]
- Michaud, K.; Augsburger, M.; Sporkert, F.; Bollmann, M.; Krompecher, T.; Mangin, P. Interpretation of lesions of the cardiac conduction system in cocaine-related fatalities. J. Forensic Leg. Med. 2007, 14, 416–422. [Google Scholar] [CrossRef]
- Sánchez-Quintana, D.; Cabrera, J.A.; Farré, J.; Climent, V.; Anderson, R.H.; Ho, S.Y. Sinus node revisited in the era of electroanatomical mapping and catheter ablation. Heart 2005, 91, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.H.; Sánchez-Quintana, D.; Mori, S.; Cabrera, J.A.; Sternick, B.E. Re-evaluation of the structure of the atrioventricular node and its connections with the atrium. Europace 2020, 22, 821–830. [Google Scholar] [CrossRef]
- Climent, V.; Hurlé, A.; Ho, S.Y.; Sáenz-Santamaría, J.; Nogales, A.G.; Sánchez-Quintana, D. Early morphologic changes following microwave endocardial ablation for treatment of chronic atrial fibrillation during mitral valve surgery. J. Cardiovasc. Electrophysiol. 2004, 15, 1277–1283. [Google Scholar] [CrossRef]
- Amorós-Figueras, G.; Roselló-Diez, E.; Sánchez-Quintana, D.; Casabella-Ramón, S.; Jorge, E.; Nevado-Medina, J.; Arzamendi, D.; Millán, X.; Alonso-Martin, C.; Guerra, J.M.; et al. Changes in local atrial electrograms and surface ECG induced by acute atrial myocardial infarction. Front. Physiol. 2020, 11, 264–273. [Google Scholar] [CrossRef]
- Sánchez-Quintana, D.; Ho, S.Y.; Cabrera, J.A.; Farré, J.; Anderson, R.H. Topographic anatomy of the inferior pyramidal space: Relevance to radiofrequency catheter ablation. J. Cardiovasc. Electrophysiol. 2001, 12, 210–217. [Google Scholar] [CrossRef]
- Sánchez-Quintana, D.; Anderson, R.H.; Tretter, J.T.; Cabrera, J.A.; Sternick, E.B.; Farré, J. Anatomy of the conduction tissues 100 years on: What have we learned? Heart 2021, 2021, 320304. [Google Scholar] [CrossRef]
- Cabrera, J.A.; Anderson, R.H.; Porta-Sánchez, A.; Macías, Y.; Cano, O.; Spicer, D.E.; Sánchez-Quintana, D. The Atrioventricular Conduction Axis and its Implications for Permanent Pacing. Arrhythm. Electrophysiol. Rev. 2021, 10, 181–189. [Google Scholar] [CrossRef]
- Dominic, P.; Ahmad, J.; Awwab, H.; Bhuiyan, M.S.; Kevil, C.G.; Goeders, N.E.; Murnane, K.S.; Patterson, J.C.; Sandau, K.E.; Gopinathannair, R.; et al. Stimulant drugs of abuse and cardiac arrhythmias. Circ. Arrhythm. Electrophysiol. 2022, 15, 71–83. [Google Scholar] [CrossRef]
- Schwartz, B.G.; Rezkalla, S.; Kloner, R.A. Cardiovascular effects of cocaine. Circulation 2010, 122, 2558–2569. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.; Lin, P.H.; Bush, R.L.; Nguyen, L.; Lumsdem, A.B. Acute arterial thrombosis associated with cocaine abuse. J. Vasc. Surg. 2004, 40, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Lucena, J.; Blanco, M.; Jurado, C.; Rico, A.; Salguero, M.; Vazquez, R.; Thiene, G.; Basso, C. Cocaine-related sudden death: A prospective investigation in south-west Spain. Eur. Heart J. 2010, 31, 318–329. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, A.J.; Levine, B.; Titus, J.; Smialek, J.E. The interpretation of cocaine and benzoilecgonine concentrations in postmortem cases. Forensic Sci. Int. 1999, 101, 17–25. [Google Scholar] [CrossRef]
- Blaho, K.; Logan, B.; Winbery, S.; Park, L.; Schwilke, E. Blood cocaine and metabolite concentrations, clinical findings, and outcome of patients presenting to an ED. Am. J. Emerg. Med. 2000, 18, 593–598. [Google Scholar] [CrossRef]
- Karch, S.B. Interpretation of blood cocaine and metabolite concentrations. Am. J. Emerg. Med. 2000, 18, 635–636. [Google Scholar] [CrossRef]
- Bertol, E.; Trignano, C.; Di Milia, M.G.; Di Padua, M.; Mari, F. Cocaine-related deaths: An enigma still under investigation. Forensic Sci. Int. 2008, 176, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Karch, S.B.; Stephens, B.S. When is cocaine the cause of death? Am. J. Forensic Med. Pathol. 1991, 12, 1–2. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, M.E. Inhibition of HERG potassium channels by cocaethylene: A metabolite of cocaine and ethanol. Cardiovasc. Res. 2002, 53, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Harris, D.; Everhart, E.T.; Mendelson, J.; Jones, R.T. The pharmacology of cocaethylene in humans following cocaine and ethanol administration. Drug Alcohol Depend. 2003, 72, 169–182. [Google Scholar] [CrossRef]
- Wilson, L.D.; Henning, R.J.; Suttheiner, C.; Lavins, E.; Balraj, E.; Earl, S. Cocaethylene causes dose-dependent reductions in cardiac functions in anesthetized dogs. J. Cardiovasc. Pharmacol. 1995, 26, 965–973. [Google Scholar] [CrossRef]
- Clark, J.C.; Milroy, C.M.; Forrest, A.R.W. Deaths from methadone use. J. Clin. Forensic Med. 1995, 2, 143–144. [Google Scholar] [CrossRef]
- Krantz, M.J.; Lowery, C.M.; Martell, B.A.; Gourevitch, M.N.; Arnsten, J.H. Effects of methadone on QT-interval dispersion. Pharmacotherapy 2005, 25, 1523–1529. [Google Scholar] [CrossRef]
- Argo, A.; Spatola, G.F.; Zerbo, S.; Sortino, C.; Lanzarone, A.; Uzzo, M.L.; Pitruzzella, A.; Farè, F.; Roda, G.; Gambaro, V.; et al. A possible biomarker for methadone related deaths. J. Forensic Leg. Med. 2017, 49, 8–14. [Google Scholar] [CrossRef]
- Franklin, S.M.; Thihalolipavan, S.; Fontaine, J.M. Sinus bradycardia in habitual cocaine users. Am. J. Cardiol. 2017, 119, 1611–1615. [Google Scholar] [CrossRef]
- Iacobellis, G.; Kemp, W. Cardiomyocyte apoptosis in cocaine-induced myocarditis with involvement of bundle of His and left bundle branch. Int. J. Cardiol. 2006, 112, 116–118. [Google Scholar] [CrossRef]
- Gilloteaux, J.; Ekwedike, N.N. Cocaine causes atrial Purkinje fiber damage. Ultrastruct. Pathol. 2010, 34, 90–98. [Google Scholar] [CrossRef]
- Darke, S.; Kaye, S.; Duflou, J. Comparative cardiac pathology among deaths due to cocaine toxicity, opioid toxicity and non-drug-related causes. Addiction 2006, 101, 1771–1777. [Google Scholar] [CrossRef]
- Bebarta, V.S.; Summers, S. Brugada electrocardiographic pattern induced by cocaine toxicity. Ann. Emerg. Med. 2007, 49, 827–829. [Google Scholar] [CrossRef]
- Ortega-Carnicer, J.; Bertos-Polo, J.; Gutierrez-Tirado, C. Aborted sudden death, transient Brugada pattern, and wide QRS dysrrhythmias after massive cocaine ingestion. J. Electrocardiol. 2001, 34, 345–349. [Google Scholar] [CrossRef]
- Mahoney, J.J., 3rd; Haile, C.N.; De La Garza, R., 2nd; Thakkar, H.; Newton, T.F. Electrocardiographic characteristics in individuals with cocaine use disorder. Am. J. Addict. 2017, 26, 221–227. [Google Scholar] [CrossRef]
- Nerantzis, C.E.; Koulouris, S.N.; Marianou, S.K.; Pastromas, S.C.; Koutsaftis, P.N.; Agapitos, E.B. Histologic findings of the sinus node and the perinodal area in street heroin addicts, victims of sudden unexpected death. J. Forensic. Sci. 2011, 56, 645–648. [Google Scholar] [CrossRef]
- Nerantzis, C.E.; Couvaris, C.M.; Pastromas, S.C.; Marianou, S.K.; Boghiokas, I.D.; Koutsaftis, P.N. Histological findings of the atrioventricular conductive system in street heroin addicts, victims of sudden unexpected death. J. Forensic. Sci. 2013, 58 (Suppl. 1), S99–S104. [Google Scholar] [CrossRef]
- Mosseri, M.; Yarom, R.; Gostman, M.S.; Hasin, Y. Histologic evidence for small-vessel coronary artery disease in patients with angina pectoris and patent large coronary arteries. Circulation 1986, 74, 964–972. [Google Scholar] [CrossRef] [Green Version]
- Rajab, R.; Stearns, E.; Baithun, S. Autopsy pathology of cocaine users from the Eastern district of London: A retrospective cohort study. J. Clin. Pathol. 2008, 61, 848–850. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Gabutti, A.; Meini, M.; Prontera, C.; Pasanisi, E.; Passino, C.; Emdin, M.; Lombardi, M. Silent myocardial damage in cocaine addicts. Heart 2011, 97, 2056–2062. [Google Scholar] [CrossRef]
- De Jong, S.; van Veen, T.A.; van Rijen, H.V.; de Bakker, J.M. Fibrosis and cardiac arrhythmias. J. Cardiovasc. Pharmacol. 2011, 57, 630–638. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Cases | Gender | Age/Years | Heart Weight | Arrhythmic History |
|---|---|---|---|---|
| 20 specimens chronic cocaine abusers | 17 male/3 female | 25.3 ± 5 | 286 ± 30 g | Unknown |
| 20 specimens that did not have a history of drug addiction | 14 male/6 female | 27.5 ± 4 | 300 ± 25 g | Unknown |
| Cocaine Abusers Group Control Group | ||||||
|---|---|---|---|---|---|---|
| Samples | Findings | Heart Cases | % | Heart Cases | % | p |
| Sinus node structure | Increase adipose/ fibrous tissue | 7 | 35 | 1 | 5 | p < 0.001 |
| Sinus node artery | Lumen stenosis | 15 | 75 | 5 | 25 | p < 0.001 |
| AV node structure | Increase adipose/ fibrous tissue | 15 | 75 | 6.5 | 32 | p < 0.001 |
| AV node artery | Lumen stenosis | 20 | 100 | 6.5 | 32 | p < 0.001 |
| His bundle structure | Increase adipose/ fibrous tissue | 11 | 55 | 3.5 | 17 | p < 0.001 |
| Left-branch structure | Increase adipose/ fibrous tissue | 19 | 95 | 4 | 19 | p < 0.001 |
| Right-branch structure | Increase adipose/ fibrous tissue | 11.6 | 58 | 3.5 | 17 | p < 0.001 |
| Small vessels atherosclerotic lesion | Lumen stenosis | 12 | 60 | 7 | 35 | p < 0.001 |
| Inflammatory infiltration | Surrounding area | 8 | 40 | 0 | 0 | p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Quintana, D.; Alama, S.; Macías, Y.; Cabrera, J.-Á.; Santos, M.; Salguero, M. Histopathological and Quantitative Lesions of the Cardiac Conduction System and Its Vascularization Related to Chronic Cocaine Abusers and Sudden Unexpected Death. Forensic Sci. 2022, 2, 423-437. https://doi.org/10.3390/forensicsci2020032
Sánchez-Quintana D, Alama S, Macías Y, Cabrera J-Á, Santos M, Salguero M. Histopathological and Quantitative Lesions of the Cardiac Conduction System and Its Vascularization Related to Chronic Cocaine Abusers and Sudden Unexpected Death. Forensic Sciences. 2022; 2(2):423-437. https://doi.org/10.3390/forensicsci2020032
Chicago/Turabian StyleSánchez-Quintana, Damián, Sergio Alama, Yolanda Macías, José-Ángel Cabrera, María Santos, and Manuel Salguero. 2022. "Histopathological and Quantitative Lesions of the Cardiac Conduction System and Its Vascularization Related to Chronic Cocaine Abusers and Sudden Unexpected Death" Forensic Sciences 2, no. 2: 423-437. https://doi.org/10.3390/forensicsci2020032