The Cutting Movement Assessment Score (CMAS) Qualitative Screening Tool: Application to Mitigate Anterior Cruciate Ligament Injury Risk during Cutting

 , , and
, , and 
Abstract
:1. Introduction
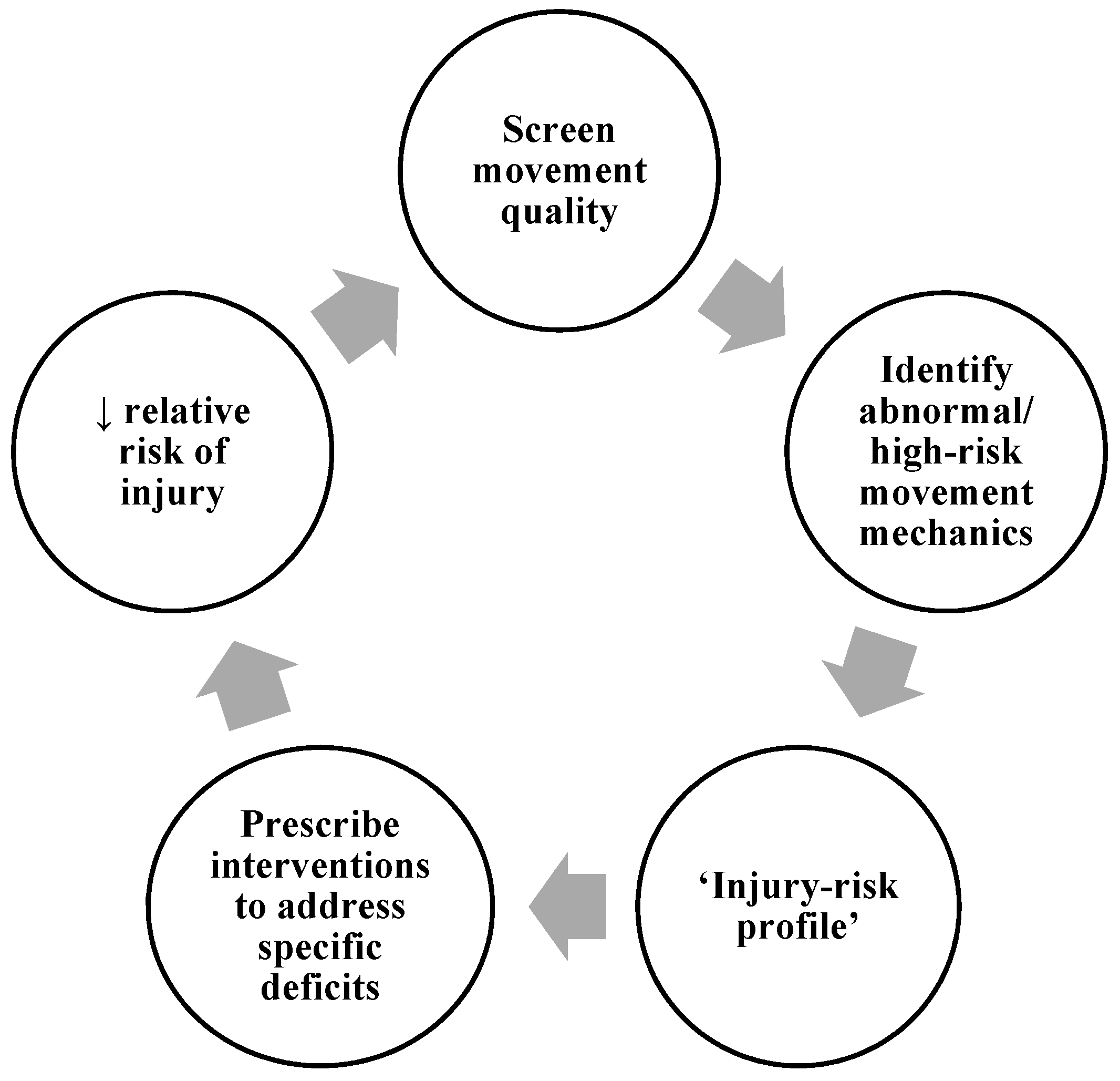
2. Qualitative Screening: Why Assess Cutting Movement Quality?
3. Introducing the Cutting Movement Assessment Score (CMAS)
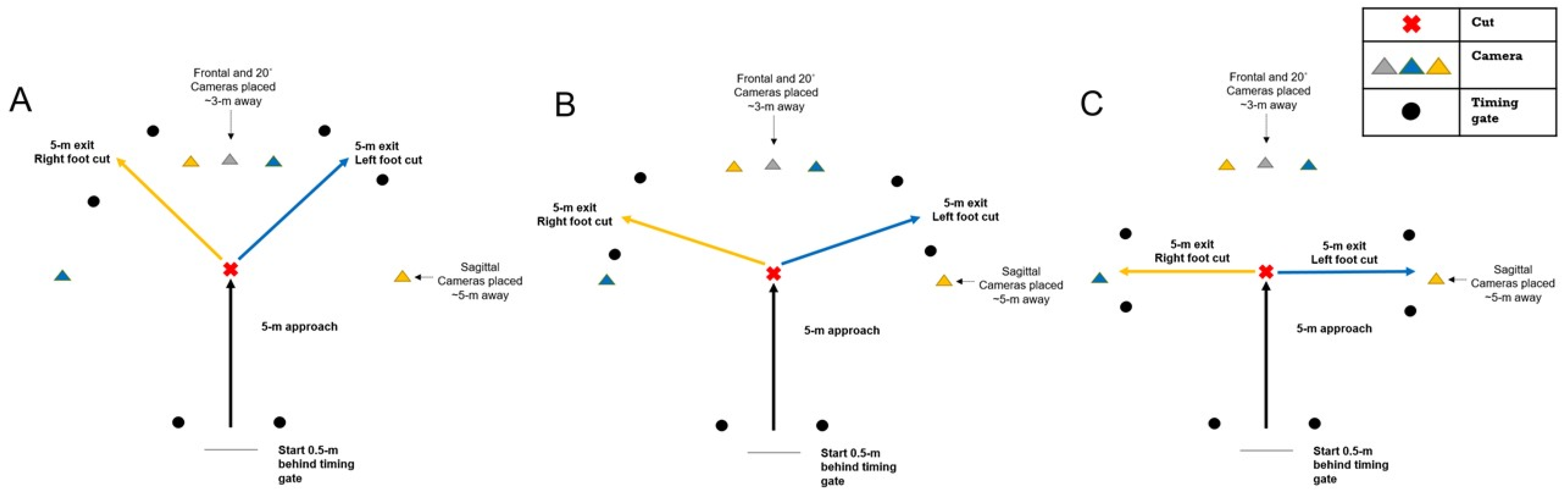
4. CMAS Methodological Procedures
5. CMAS Criteria Rationale and Operational Definitions
5.1. Item (1) Clear PFC Braking Strategy
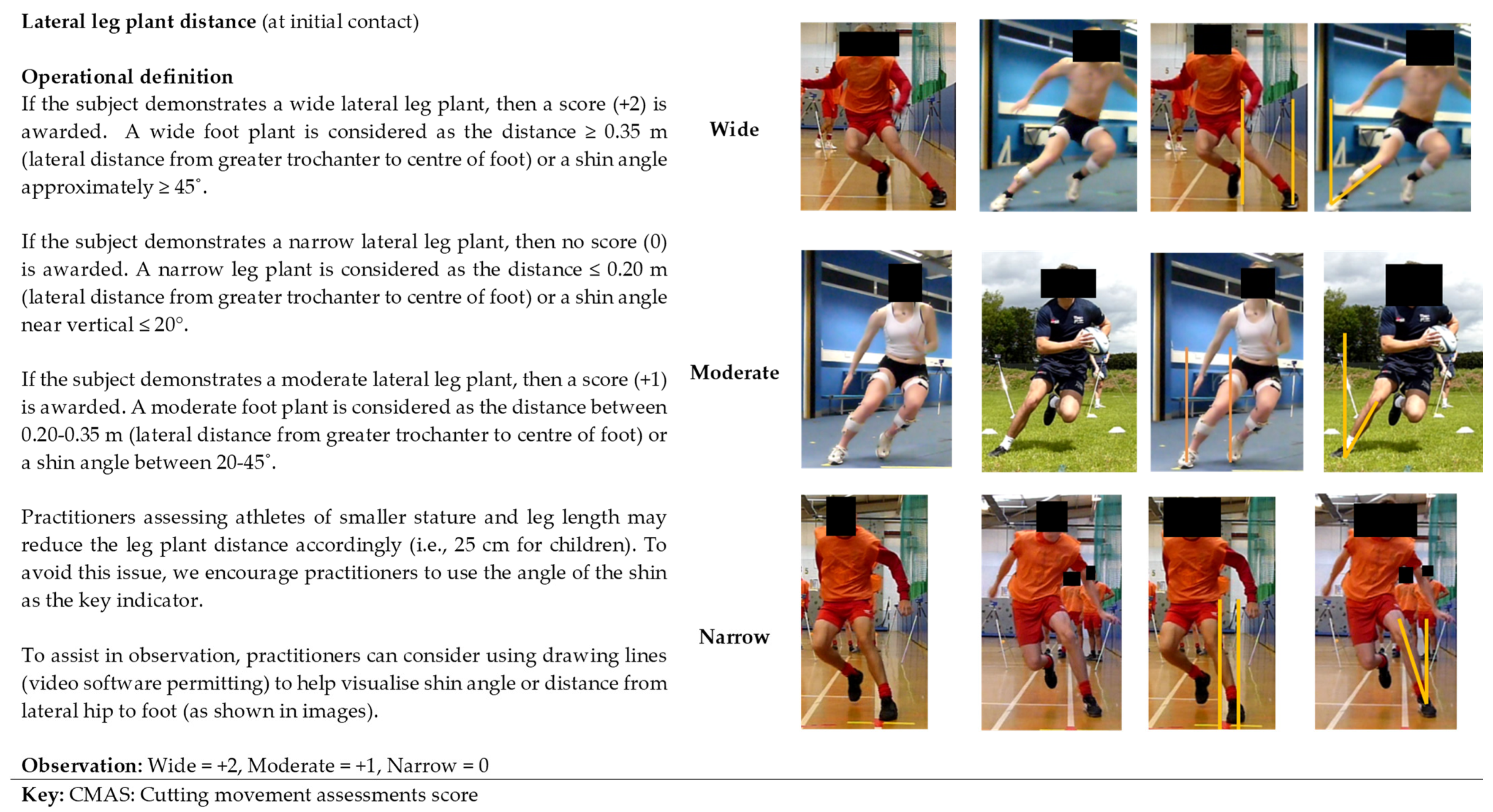
5.2. Item (2) Lateral Leg Plant Distance
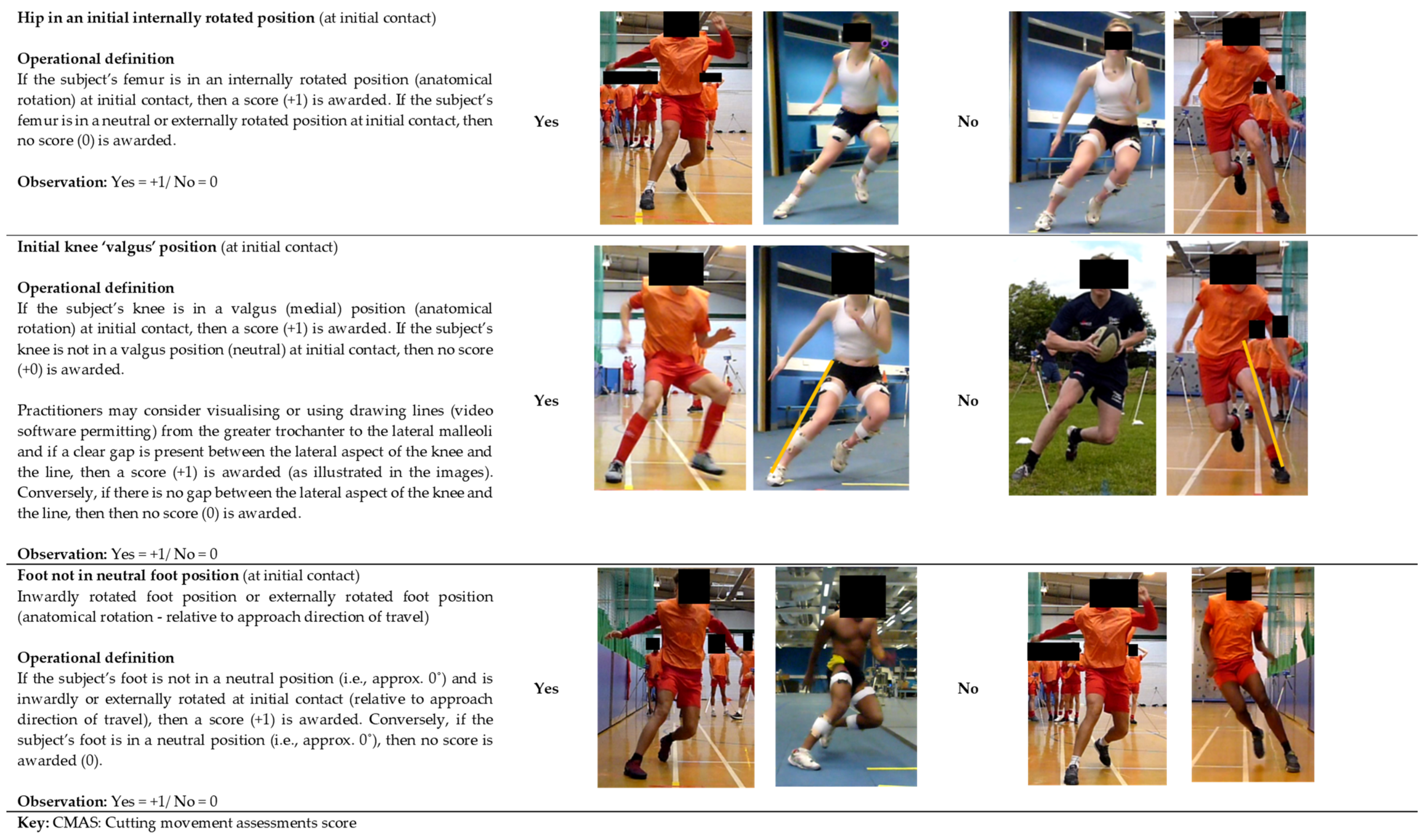
5.3. Item (3) Hip in an Initially Rotated Position
5.4. Item (4) Initial Knee ‘Valgus’ Position
5.5. Item (5) Foot Not in Neutral Foot Position
5.6. Item (6) Frontal/Transverse Plane Trunk Position
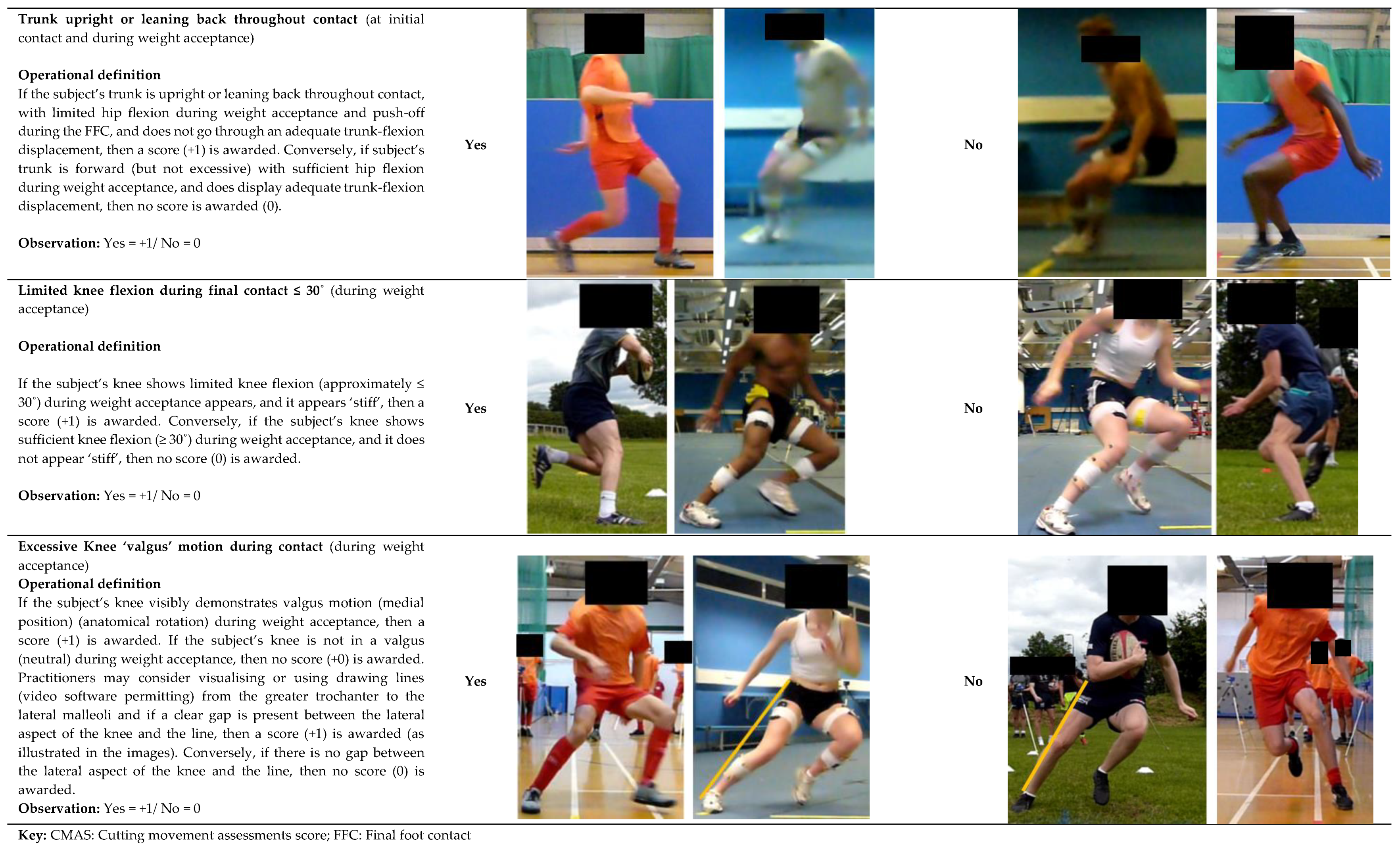
5.7. Item (7) Trunk Upright or Leaning Back Throughout Contact
5.8. Item (8) Limited Knee Flexion
5.9. Item (9) Excessive Knee ‘Valgus’ Motion during Weight Acceptance
5.10. CMAS Criteria: Considerations for Rearfoot, Midfoot, Forefoot Contact?
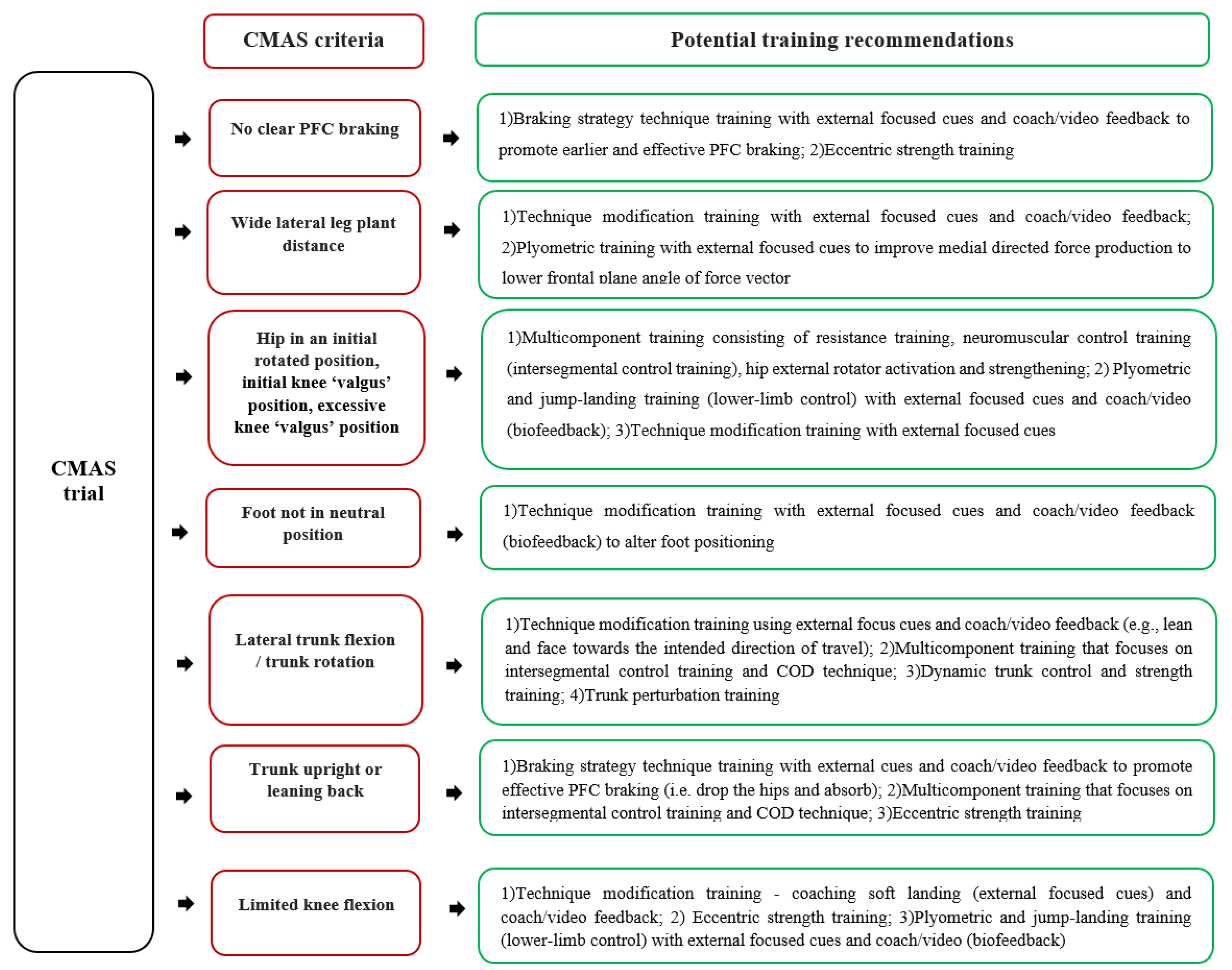
6. Practical Applications: Interpreting CMAS Score and the CMAS Training Recommendations Decision Tree
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hewett, T. Preventive biomechanics: A paradigm shift with a translational approach to biomechanics. Am. J. Sports Med. 2017, 45, 2654–2664. [Google Scholar] [CrossRef]
- Cumps, E.; Verhagen, E.; Annemans, L.; Meeusen, R. Injury rate and socioeconomic costs resulting from sports injuries in Flanders: Data derived from sports insurance statistics 2003. Br. J. Sports Med. 2008, 42, 767–772. [Google Scholar] [CrossRef]
- Quatman, C.E.; Hewett, T.E. The anterior cruciate ligament injury controversy: Is “valgus collapse” a sex-specific mechanism? Br. J. Sports Med. 2009, 43, 328–335. [Google Scholar] [CrossRef]
- Langford, J.L.; Webster, K.E.; Feller, J.A. A prospective longitudinal study to assess psychological changes following anterior cruciate ligament reconstruction surgery. Br. J. Sports Med. 2009, 43, 377–378. [Google Scholar] [CrossRef]
- Lohmander, L.S.; Englund, P.M.; Dahl, L.L.; Roos, E.M. The long-term consequence of anterior cruciate ligament and meniscus injuries. Am. J. Sports Med. 2007, 35, 1756–1769. [Google Scholar] [CrossRef] [Green Version]
- Quatman, C.E.; Quatman-Yates, C.C.; Hewett, T.E. A ‘Plane’Explanation of Anterior Cruciate Ligament Injury Mechanisms. Sports Med. 2010, 40, 729–746. [Google Scholar] [CrossRef]
- Meeuwisse, W.H.; Tyreman, H.; Hagel, B.; Emery, C. A dynamic model of etiology in sport injury: The recursive nature of risk and causation. Clin. J. Sport Med. 2007, 17, 215–219. [Google Scholar] [CrossRef]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition-narrative review and new concept. Br. J. Sports Med. 2016, 50, 1309–1314. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, D.G. Rationale for training programs to reduce anterior cruciate ligament injuries in Australian football. J. Orthop. Sport Phys. 2001, 31, 645–654. [Google Scholar] [CrossRef] [Green Version]
- Lipps, D.B.; Wojtys, E.M.; Ashton-Miller, J.A. Anterior cruciate ligament fatigue failures in knees subjected to repeated simulated pivot landings. Am. J. Sports Med. 2013, 41, 1058–1066. [Google Scholar] [CrossRef]
- Wojtys, E.M.; Beaulieu, M.L.; Ashton-Miller, J.A. New perspectives on ACL injury: On the role of repetitive sub-maximal knee loading in causing ACL fatigue failure. J. Orthop. Res. 2016, 34, 2059–2068. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, S.; Schall, M.C., Jr. Musculoskeletal disorders as a fatigue failure process: Evidence, implications and research needs. Ergonomics 2017, 60, 255–269. [Google Scholar] [CrossRef]
- Beaulieu, M.L.; Wojtys, E.M.; Ashton-Miller, J.A. Risk of anterior cruciate ligament fatigue failure is increased by limited internal femoral rotation during in vitro repeated pivot landings. Am. J. Sports Med. 2015, 43, 2233–2241. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Kim, J.; Shao, W.; Schlecht, S.H.; Baek, S.Y.; Jones, A.K.; Ahn, T.; Ashton-Miller, J.A.; Banaszak Holl, M.M.; Wojtys, E.M. An Anterior Cruciate Ligament Failure Mechanism. Am. J. Sports Med. 2019, 47, 2067–2076. [Google Scholar] [CrossRef]
- Bahr, R.; Krosshaug, T. Understanding injury mechanisms: A key component of preventing injuries in sport. Br. J. Sports Med. 2005, 39, 324–329. [Google Scholar] [CrossRef]
- Edwards, W.B. Modeling overuse injuries in sport as a mechanical fatigue phenomenon. Exerc. Sport Sci. Rev. 2018, 46, 224–231. [Google Scholar] [CrossRef]
- Walden, M.; Krosshaug, T.; Bjorneboe, J.; Andersen, T.E.; Faul, O.; Hagglund, M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: A systematic video analysis of 39 cases. Br. J. Sports Med. 2015, 49, 1452–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, C.; Blackburn, J.; Withers, D.; Tierney, G.; Moran, C.; Simms, C. Mechanisms of ACL injury in professional rugby union: A systematic video analysis of 36 cases. Br. J. Sports Med. 2018, 52, 944–1001. [Google Scholar] [CrossRef]
- Olsen, O.-E.; Myklebust, G.; Engebretsen, L.; Bahr, R. Injury mechanisms for anterior cruciate ligament injuries in team handball a systematic video analysis. Am. J. Sports Med. 2004, 32, 1002–1012. [Google Scholar] [CrossRef]
- Brophy, R.H.; Stepan, J.G.; Silvers, H.J.; Mandelbaum, B.R. Defending puts the anterior cruciate ligament at risk during soccer: A gender-based analysis. Sports Health 2015, 7, 244–249. [Google Scholar] [CrossRef]
- Cochrane, J.L.; Lloyd, D.G.; Buttfield, A.; Seward, H.; McGivern, J. Characteristics of anterior cruciate ligament injuries in Australian football. J. Sci. Med. Sport 2007, 10, 96–104. [Google Scholar] [CrossRef]
- Faude, O.; Junge, A.; Kindermann, W.; Dvorak, J. Injuries in female soccer players a prospective study in the german national league. Am. J. Sports Med. 2005, 33, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Boden, B.P.; Dean, G.S.; Feagin, J.A.; Garrett, W.E. Mechanisms of anterior cruciate ligament injury. Orthopedics 2000, 23, 573–578. [Google Scholar] [CrossRef]
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebretsen, L.; Bahr, R.; Krosshaug, T. Mechanisms for noncontact anterior cruciate ligament injuries knee joint kinematics in 10 injury situations from female team handball and basketball. Am. J. Sports Med. 2010, 38, 2218–2225. [Google Scholar] [CrossRef]
- Kimura, Y.; Ishibashi, Y.; Tsuda, E.; Yamamoto, Y.; Tsukada, H.; Toh, S. Mechanisms for anterior cruciate ligament injuries in badminton. Br. J. Sports Med. 2010, 44, 1124–1127. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.T.; Mandelbaum, B.R.; Schub, D.; Rodeo, S.A.; Matava, M.J.; Silvers, H.J.; Cole, B.J.; ElAttrache, N.S.; McAdams, T.R.; Brophy, R.H. Video analysis of anterior cruciate ligament tears in professional American football athletes. Am. J. Sports Med. 2018, 46, 862–868. [Google Scholar] [CrossRef]
- Stuelcken, M.C.; Mellifont, D.B.; Gorman, A.D.; Sayers, M.G. Mechanisms of anterior cruciate ligament injuries in elite women’s netball: A systematic video analysis. J. Sports Sci. 2016, 34, 1516–1522. [Google Scholar] [CrossRef]
- Boden, B.P.; Torg, J.S.; Knowles, S.B.; Hewett, T.E. Video analysis of anterior cruciate ligament injury abnormalities in hip and ankle kinematics. Am. J. Sports Med. 2009, 37, 252–259. [Google Scholar] [CrossRef]
- Besier, T.F.; Lloyd, D.G.; Cochrane, J.L.; Ackland, T.R. External loading of the knee joint during running and cutting maneuvers. Med. Sci. Sports Exerc. 2001, 33, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.A.; Herrington, L.; Graham-Smith, P. Braking characteristics during cutting and pivoting in female soccer players. J. Electromyogr. Kinesiol. 2016, 30, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, A.R.; Lloyd, D.G.; Elliott, B.C.; Steele, J.R.; Munro, B.J.; Russo, K.A. The effect of technique change on knee loads during sidestep cutting. Med. Sci. Sports Exerc. 2007, 39, 1765–1773. [Google Scholar] [CrossRef] [Green Version]
- Dempsey, A.R.; Lloyd, D.G.; Elliott, B.C.; Steele, J.R.; Munro, B.J. Changing sidestep cutting technique reduces knee valgus loading. Am. J. Sports Med. 2009, 37, 2194–2200. [Google Scholar] [CrossRef] [Green Version]
- Kristianslund, E.; Faul, O.; Bahr, R.; Myklebust, G.; Krosshaug, T. Sidestep cutting technique and knee abduction loading: Implications for ACL prevention exercises. Br. J. Sports Med. 2014, 48, 779–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, C.S.; Chaudhari, A.M.; Andriacchi, T.P. Valgus plus internal rotation moments increase anterior cruciate ligament strain more than either alone. Med. Sci. Sports Exerc. 2011, 43, 1484–1491. [Google Scholar] [CrossRef]
- Markolf, K.L.; Burchfield, D.M.; Shapiro, M.M.; Shepard, M.F.; Finerman, G.A.M.; Slauterbeck, J.L. Combined knee loading states that generate high anterior cruciate ligament forces. J. Orthop. Res. 1995, 13, 930–935. [Google Scholar] [CrossRef]
- Kiapour, A.M.; Demetropoulos, C.K.; Kiapour, A.; Quatman, C.E.; Wordeman, S.C.; Goel, V.K.; Hewett, T.E. Strain response of the anterior cruciate ligament to uniplanar and multiplanar loads during simulated landings: Implications for injury mechanism. Am. J. Sports Med. 2016, 44, 2087–2096. [Google Scholar] [CrossRef]
- Oh, Y.K.; Lipps, D.B.; Ashton-Miller, J.A.; Wojtys, E.M. What strains the anterior cruciate ligament during a pivot landing? Am. J. Sports Med. 2012, 40, 574–583. [Google Scholar] [CrossRef] [Green Version]
- Bates, N.A.; Myer, G.D.; Shearn, J.T.; Hewett, T.E. Anterior cruciate ligament biomechanics during robotic and mechanical simulations of physiologic and clinical motion tasks: A systematic review and meta-analysis. Clin. Biomech. 2015, 30, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Hewett, T.; Myer, G.D.; Ford, K.R.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Van den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes a prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLean, S.G.; Huang, X.; van den Bogert, A.J. Association between lower extremity posture at contact and peak knee valgus moment during sidestepping: Implications for ACL injury. Clin. Biomech. 2005, 20, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Havens, K.L.; Sigward, S.M. Cutting mechanics: Relation to performance and anterior cruciate ligament injury risk. Med. Sci. Sports Exerc. 2015, 47, 818–824. [Google Scholar] [CrossRef]
- Jones, P.A.; Herrington, L.; Graham-Smith, P. Technique determinants of knee joint loads during cutting in female soccer players. Hum. Mov. Sci. 2015, 42, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.S. Change-of-Direction Biomechanics: Is What’s Best for Anterior Cruciate Ligament Injury Prevention Also Best for Performance? Sports Med. 2018, 48, 1799–1807. [Google Scholar] [CrossRef] [PubMed]
- Pappas, E.; Nightingale, E.J.; Simic, M.; Ford, K.R.; Hewett, T.E.; Myer, G.D. Do exercises used in injury prevention programmes modify cutting task biomechanics? A systematic review with meta-analysis. Br. J. Sports Med. 2015, 49, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Padua, D.A.; DiStefano, L.J.; Hewett, T.E.; Garrett, W.E.; Marshall, S.W.; Golden, G.M.; Shultz, S.J.; Sigward, S.M. National Athletic Trainers’ Association Position Statement: Prevention of Anterior Cruciate Ligament Injury. J. Athl. Train. 2018, 53, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Dos’Santos, T.; Thomas, C.; Comfort, P.; Jones, P.A. The Effect of Training Interventions on Change of Direction Biomechanics Associated with Increased Anterior Cruciate Ligament Loading: A Scoping Review. Sports Med. 2019, 49, 1837–1859. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, D.G.; Buchanan, T.S. Strategies of muscular support of varus and valgus isometric loads at the human knee. J. Biomech. 2001, 34, 1257–1267. [Google Scholar] [CrossRef]
- Donnelly, C.; Elliott, B.C.; Ackland, T.R.; Doyle, T.L.; Beiser, T.F.; Finch, C.F.; Cochrane, J.; Dempsey, A.R.; Lloyd, D. An anterior cruciate ligament injury prevention framework: Incorporating the recent evidence. Res. Sports Med. 2012, 20, 239–262. [Google Scholar] [CrossRef]
- Fox, A.S.; Bonacci, J.; McLean, S.G.; Saunders, N. Efficacy of ACL injury risk screening methods in identifying high-risk landing patterns during a sport-specific task. Scand. J. Med. Sci. Sports 2017, 27, 525–534. [Google Scholar] [CrossRef]
- Zahidi, N.N.M.; Ismail, S.I. Notational analysis of evasive agility skills executed by attacking ball carriers among elite rugby players of the 2015 Rugby World Cup. J. Movement Health Exerc. 2018, 7, 99–113. [Google Scholar]
- Wheeler, K.W.; Askew, C.D.; Sayers, M.G. Effective attacking strategies in rugby union. Eur. J. Sports Sci. 2010, 10, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Karcher, C.; Buchheit, M. On-court demands of elite handball, with special reference to playing positions. Sports Med. 2014, 44, 797–814. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.B.; Wright, A.A.; Dischiavi, S.L.; Townsend, M.A.; Marmon, A.R. Activity Demands During Multi-Directional Team Sports: A Systematic Review. Sports Med. 2017, 47, 2533–2551. [Google Scholar] [CrossRef] [PubMed]
- Dos’Santos, T.; McBurnie, A.; Thomas, C.; Comfort, P.; Jones, P.A. Biomechanical Comparison of Cutting Techniques: A Review and Practical Applications. Strength Cond. J. 2019, 41, 40–54. [Google Scholar] [CrossRef]
- Dos’Santos, T.; McBurnie, A.; Donelon, T.; Thomas, C.; Comfort, P.; Jones, P.A. A qualitative screening tool to identify athletes with “high-risk” movement mechanics during cutting: The cutting movement assessment score (CMAS). Phys. Ther. Sport 2019, 38, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R. Why screening tests to predict injury do not work and probably never will: A critical review. Br. J. Sports Med. 2016, 50, 776–780. [Google Scholar] [CrossRef] [Green Version]
- Fox, A.S.; Bonacci, J.; McLean, S.G.; Spittle, M.; Saunders, N. A systematic evaluation of field-based screening methods for the assessment of anterior cruciate ligament (ACL) injury risk. Sports Med. 2016, 46, 715–735. [Google Scholar] [CrossRef]
- McCunn, R.; Aus der Fünten, K.; Fullagar, H.H.K.; McKeown, I.; Meyer, T. Reliability and association with injury of movement screens: A critical review. Sports Med. 2015, 46, 763–781. [Google Scholar] [CrossRef]
- Herrington, L.C.; Munro, A.G.; Jones, P.A. Assessment of factors associated with injury risk. In Performance Assessment in Strength and Conditioning; Comfort, P., McMahon, J.J., Jones, P.A., Eds.; Routledge: Abingdon, UK, 2018; pp. 53–95. [Google Scholar]
- Mok, K.-M.; Leow, R.-S. Measurement of movement patterns to enhance ACL injury prevention-A dead end? J. Sports Med. Arthrosc. Rehabil. Technol. 2016, 5, 13–16. [Google Scholar] [CrossRef] [Green Version]
- McCunn, R.; Meyer, T. Screening for risk factors: If you liked it then you should have put a number on it. Br. J. Sports Med. 2016, 50, 1354. [Google Scholar] [CrossRef]
- Jones, P.A.; Herrington, L.; Graham-Smith, P. Technique determinants of knee abduction moments during pivoting in female soccer players. Clin. Biomech. 2016, 31, 107–112. [Google Scholar] [CrossRef]
- Sigward, S.M.; Cesar, G.M.; Havens, K.L. Predictors of frontal plane knee moments during side-step cutting to 45 and 110 degrees in men and women: Implications for anterior cruciate ligament injury. Clin. J. Sport Med. 2015, 25, 529–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamison, S.T.; Pan, X.; Chaudhari, A.M.W. Knee moments during run-to-cut maneuvers are associated with lateral trunk positioning. J. Biomech. 2012, 45, 1881–1885. [Google Scholar] [CrossRef] [PubMed]
- Frank, B.; Bell, D.R.; Norcross, M.F.; Blackburn, J.T.; Goerger, B.M.; Padua, D.A. Trunk and hip biomechanics influence anterior cruciate loading mechanisms in physically active participants. Am. J. Sports Med. 2013, 41, 2676–2683. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, C.J.; Lloyd, D.G.; Elliott, B.C.; Reinbolt, J.A. Optimizing whole-body kinematics to minimize valgus knee loading during sidestepping: Implications for ACL injury risk. J. Biomech. 2012, 45, 1491–1497. [Google Scholar] [CrossRef]
- Dai, B.; William, E.G.; Michael, T.G.; Darin, A.P.; Robin, M.Q.; Bing, Y. The Effects of 2 Landing Techniques on Knee Kinematics, Kinetics, and Performance During Stop-Jump and Side-Cutting Tasks. Am. J. Sports Med. 2014, 43, 466–474. [Google Scholar] [CrossRef]
- Weir, G.; Alderson, J.; Smailes, N.; Elliott, B.; Donnelly, C. A Reliable Video-based ACL Injury Screening Tool for Female Team Sport Athletes. Int. J. Sports Med. 2019, 40, 191–199. [Google Scholar] [CrossRef]
- Sigward, S.M.; Powers, C.M. Loading characteristics of females exhibiting excessive valgus moments during cutting. Clin. Biomech. 2007, 22, 827–833. [Google Scholar] [CrossRef]
- Dos’Santos, T.; Thomas, C.; Comfort, P.; Jones, P.A. The effect of angle and velocity on change of direction biomechanics: An angle-velocity trade-off. Sports Med. 2018, 48, 2235–2253. [Google Scholar] [CrossRef] [Green Version]
- McBurnie, A.; Dos’ Santos, T.; Jones, P.A. Biomechanical Associates of Performance and Knee Joint Loads During an 70–90° Cutting Maneuver in Sub-Elite Soccer Players. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kristianslund, E.; Krosshaug, T. Comparison of drop jumps and sport-specific sidestep cutting: Implications for anterior cruciate ligament injury risk screening. Am. J. Sports Med. 2013, 41, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Chinnasee, C.; Weir, G.; Sasimontonkul, S.; Alderson, J.; Donnelly, C. A Biomechanical Comparison of Single-Leg Landing and Unplanned Sidestepping. Int. J. Sports Med. 2018, 39, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Padua, D.A.; Marshall, S.W.; Boling, M.C.; Thigpen, C.A.; Garrett, W.E.; Beutler, A.I. The landing error scoring system (LESS) is a valid and reliable clinical assessment tool of jump-landing biomechanics the JUMP-ACL study. Am. J. Sports Med. 2009, 37, 1996–2002. [Google Scholar] [CrossRef] [PubMed]
- Herrington, L.; Munro, A. A preliminary investigation to establish the criterion validity of a qualitative scoring system of limb alignment during single-leg squat and landing. J. Exerc. Sports Orthop. 2014, 1, 1–6. [Google Scholar]
- Jones, P.A.; Donelon, T.; Dos’ Santos, T. A preliminary investigation into a qualitative assessment tool to identify athletes with high knee abduction moments during cutting: Cutting Movement Assessment Score (CMAS). Prof. Strength Cond. 2017, 47, 37–42. [Google Scholar]
- Nilstad, A.; Andersen, T.E.; Kristianslund, E.; Bahr, R.; Myklebust, G.; Steffen, K.; Krosshaug, T. Physiotherapists can identify female football players with high knee valgus angles during vertical drop jumps using real-time observational screening. J. Orthop. Sport Phys. 2014, 44, 358–365. [Google Scholar] [CrossRef] [Green Version]
- Smith, H.C.; Johnson, R.J.; Shultz, S.J.; Tourville, T.; Holterman, L.A.; Slauterbeck, J.; Vacek, P.M.; Beynnon, B.D. A prospective evaluation of the Landing Error Scoring System (LESS) as a screening tool for anterior cruciate ligament injury risk. Am. J. Sports Med. 2012, 40, 521–526. [Google Scholar] [CrossRef]
- Ekegren, C.L.; Miller, W.C.; Celebrini, R.G.; Eng, J.J.; Macintyre, D.L. Reliability and validity of observational risk screening in evaluating dynamic knee valgus. J. Orthop. Sport Phys. 2009, 39, 665–674. [Google Scholar] [CrossRef] [Green Version]
- Padua, D.A.; Boling, M.C.; DiStefano, L.J.; Onate, J.A.; Beutler, A.I.; Marshall, S.W. Reliability of the landing error scoring system-real time, a clinical assessment tool of jump-landing biomechanics. J. Sport Rehabil. 2011, 20, 145–156. [Google Scholar] [CrossRef] [Green Version]
- Myer, G.D.; Brent, J.L.; Ford, K.R.; Hewett, T.E. Real-time assessment and neuromuscular training feedback techniques to prevent ACL injury in female athletes. Strength Cond. J. 2011, 33, 21–35. [Google Scholar] [CrossRef] [Green Version]
- Myer, G.D.; Ford, K.R.; Hewett, T.E. Tuck jump assessment for reducing anterior cruciate ligament injury risk. Athl. Ther. Today J. Sports Health Care Prof. 2008, 13, 39–44. [Google Scholar]
- Herrington, L.; Myer, G.D.; Munro, A. Intra and inter-tester reliability of the tuck jump assessment. Phys. Ther. Sport 2013, 14, 152–155. [Google Scholar] [CrossRef]
- Almangoush, A.; Herrington, L.; Jones, R. A preliminary reliability study of a qualitative scoring system of limb alignment during single leg squat. Phys. Ther. Rehabil. 2014, 1, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Herrington, L.; Myer, G.; Horsley, I. Task based rehabilitation protocol for elite athletes following anterior cruciate ligament reconstruction: A clinical commentary. Phys. Ther. Sport 2013, 14, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Krosshaug, T.; Nakamae, A.; Boden, B.P.; Engebretsen, L.; Smith, G.; Slauterbeck, J.R.; Hewett, T.E.; Bahr, R. Mechanisms of anterior cruciate ligament injury in basketball video analysis of 39 cases. Am. J. Sports Med. 2007, 35, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Torg, J.S.; Boden, B.P. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: Lateral trunk and knee abduction motion are combined components of the injury mechanism. Br. J. Sports Med. 2009, 43, 417–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alenezi, F.; Herrington, L.; Jones, P.; Jones, R. Relationships between lower limb biomechanics during single leg squat with running and cutting tasks: A preliminary investigation. Br. J. Sports Med. 2014, 48, 560–561. [Google Scholar] [CrossRef] [Green Version]
- Tanikawa, H.; Matsumoto, H.; Komiyama, I.; Kiriyama, Y.; Toyama, Y.; Nagura, T. Comparison of knee mechanics among risky athletic motions for noncontact anterior cruciate ligament injury. J. Appl. Biomech. 2013, 29, 749–755. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, K.M.; Monteiro, S.K.; Hoelker, I.A. Comparison of selected lateral cutting activities used to assess ACL injury risk. J. Appl. Biomech. 2009, 25, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.A.; Herrington, L.C.; Munro, A.G.; Graham-Smith, P. Is there a relationship between landing, cutting, and pivoting tasks in terms of the characteristics of dynamic valgus? Am. J. Sports Med. 2014, 42, 2095–2102. [Google Scholar] [CrossRef] [Green Version]
- Munro, A.G.; Herrington, L.; Comfort, P. The Relationship Between 2-Dimensional Knee-Valgus Angles During Single-Leg Squat, Single-Leg-Land, and Drop-Jump Screening Tests. J. Sports Rehabil. 2017, 26, 72–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos’ Santos, T. Biomechanical Determinants of Injury Risk and Performance during Change of Direction: Implications for Screening and Intervention. Doctoral Dissertation, University of Salford, Salford, UK, 2020. [Google Scholar]
- Dos’Santos, T.; McBurnie, A.; Comfort, P.; Jones, P.A. The Effects of Six-Weeks Change of Direction Speed and Technique Modification Training on Cutting Performance and Movement Quality in Male Youth Soccer Players. Sports 2019, 7, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowling, A.V.; Corazza, S.; Chaudhari, A.M.; Andriacchi, T.P. Shoe-surface friction influences movement strategies during a sidestep cutting task: Implications for anterior cruciate ligament injury risk. Am. J. Sports Med. 2010, 38, 478–485. [Google Scholar] [CrossRef]
- Dowling, A.V.; Andriacchi, T.P. Role of Shoe–Surface Interaction and Noncontact ACL Injuries. In ACL Injuries in the Female Athlete; Springer: Berlin/Heidelberg, Germany, 2012; pp. 85–108. [Google Scholar]
- Pedroza, A.; Fernandez, S.; Heidt, J.R.; Kaeding, C. Evaluation of the shoe-surface interaction using an agility maneuver. Med. Sci. Sports Exerc. 2010, 42, 1754–1759. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.R.; McLeod, W.D.; Ward, T.; Howard, K. The cutting mechanism. Am. J. Sports Med. 1977, 5, 111–121. [Google Scholar] [CrossRef]
- Dos’ Santos, T.; Thomas, C.; Comfort, P.; Jones, P.A. The Role of the Penultimate Foot Contact During Change of Direction: Implications on Performance and Risk of Injury. Strength Cond. J. 2019, 41, 87–104. [Google Scholar] [CrossRef]
- Graham-Smith, P.; Rumpf, M.; Jones, P.A. Assessment of Deceleration Ability and Relationship to Approach Speed and Eccentric Strength. ISBS Proc. Arch. 2018, 36, 8. [Google Scholar]
- Grassi, A.; Smiley, S.P.; Roberti di Sarsina, T.; Signorelli, C.; Marcheggiani Muccioli, G.M.; Bondi, A.; Romagnoli, M.; Agostini, A.; Zaffagnini, S. Mechanisms and situations of anterior cruciate ligament injuries in professional male soccer players: A YouTube-based video analysis. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 697–981. [Google Scholar] [CrossRef]
- Havens, K.L.; Sigward, S.M. Whole body mechanics differ among running and cutting maneuvers in skilled athletes. Gait Posture 2014, 42, 240–245. [Google Scholar] [CrossRef]
- Inaba, Y.; Yoshioka, S.; Iida, Y.; Hay, D.C.; Fukashiro, S. A biomechanical study of side steps at different distances. J. Appl. Biomech. 2013, 29, 336–345. [Google Scholar] [CrossRef] [Green Version]
- Golden, G.M.; Pavol, M.J.; Hoffman, M.A. Knee joint kinematics and kinetics during a lateral false-step maneuver. J. Athl. Train. 2009, 44, 503–510. [Google Scholar] [CrossRef]
- McLean, S.G.; Lipfert, S.W.; Van den Bogert, A.J. Effect of gender and defensive opponent on the biomechanics of sidestep cutting. Med. Sci. Sports Exerc. 2004, 36, 1008–1016. [Google Scholar] [CrossRef] [Green Version]
- Nyland, J.; Caborn, D.N.M.; Shapiro, R.; Johnson, D.L.; Fang, H. Hamstring extensibility and transverse plane knee control relationship in athletic women. Knee Surg. Sports Traumatol. Arthrosc. 1999, 7, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Loudon, J.K.; Jenkins, W.; Loudon, K.L. The relationship between static posture and ACL injury in female athletes. J. Orthop. Sport Phys. 1996, 24, 91–97. [Google Scholar] [CrossRef] [Green Version]
- Ford, K.R.; Myer, G.D.; Toms, H.E.; Hewett, T.E. Gender differences in the kinematics of unanticipated cutting in young athletes. Med. Sci. Sports Exerc. 2005, 37, 124–129. [Google Scholar] [CrossRef] [Green Version]
- Dempster, W.T. Space Requirements of the Seated Operator: Geometrical, Kinematic, and Mechanical Aspects of the Body, with Special Reference to the Limbs. Michigan State Univ East Lansing. 1955. Available online: https://apps.dtic.mil/sti/pdfs/AD0087892.pdf (accessed on 6 April 2021).
- Mendiguchia, J.; Ford, K.R.; Quatman, C.E.; Alentorn-Geli, E.; Hewett, T.E. Sex differences in proximal control of the knee joint. Sports Med. 2011, 41, 541–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewett, T.E.; Myer, G.D. The mechanistic connection between the trunk, knee, and anterior cruciate ligament injury. Exerc. Sport Sci. Rev. 2011, 39, 161. [Google Scholar] [CrossRef] [Green Version]
- Zazulak, B.T.; Hewett, T.E.; Reeves, N.P.; Goldberg, B.; Cholewicki, J. The effects of core proprioception on knee injury: A prospective biomechanical-epidemiological study. Am. J. Sports Med. 2007, 35, 368–373. [Google Scholar] [CrossRef]
- Zazulak, B.T.; Hewett, T.E.; Reeves, N.P.; Goldberg, B.; Cholewicki, J. Deficits in Neuromuscular Control of the Trunk Predict Knee Injury Risk: Prospective Biomechanical-Epidemiologic Study. Am. J. Sports Med. 2007, 35, 1123–1130. [Google Scholar] [CrossRef]
- Marshall, B.M.; Franklyn-Miller, A.D.; King, E.A.; Moran, K.A.; Strike, S.; Falvey, A. Biomechanical factors associated with time to complete a change of direction cutting maneuver. J. Strength Cond. Res. 2014, 28, 2845–2851. [Google Scholar] [CrossRef]
- David, S.; Mundt, M.; Komnik, I.; Potthast, W. Understanding cutting maneuvers–The mechanical consequence of preparatory strategies and foot strike pattern. Hum. Mov. Sci. 2018, 62, 202–210. [Google Scholar] [CrossRef]
- Sheehan, F.T.; Sipprell Iii, W.H.; Boden, B.P. Dynamic sagittal plane trunk control during anterior cruciate ligament injury. Am. J. Sports Med. 2012, 40, 1068–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimokochi, Y.; Ambegaonkar, J.P.; Meyer, E.G.; Lee, S.Y.; Shultz, S.J. Changing sagittal plane body position during single-leg landings influences the risk of non-contact anterior cruciate ligament injury. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 888–897. [Google Scholar] [CrossRef] [Green Version]
- Yu, B.; Lin, C.-F.; Garrett, W.E. Lower extremity biomechanics during the landing of a stop-jump task. Clin. Biomech. 2006, 21, 297–305. [Google Scholar] [CrossRef]
- Sigward, S.M.; Pollard, C.D. Proximal Risk Factors for ACL Injury: Role of the Hip Joint and Musculature. In ACL Injuries in the Female Athlete; Springer: Berlin/Heidelberg, Germany, 2018; pp. 207–223. [Google Scholar]
- Pollard, C.D.; Sigward, S.M.; Powers, C.M. Limited hip and knee flexion during landing is associated with increased frontal plane knee motion and moments. Clin. Biomech. 2010, 25, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Yeow, C.H.; Lee, P.V.S.; Goh, J.C.H. Non-linear flexion relationships of the knee with the hip and ankle, and their relative postures during landing. Knee 2011, 18, 323–328. [Google Scholar] [CrossRef]
- Nguyen, A.-D.; Taylor, J.B.; Wimbish, T.G.; Keith, J.L.; Ford, K.R. Preferred Hip Strategy During Landing Reduces Knee Abduction Moment in Collegiate Female Soccer Players. J. Sport Rehabil. 2018, 27, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Powers, C.M. The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J. Orthop. Sport Phys. 2010, 40, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markolf, K.L.; Gorek, J.F.; Kabo, J.M.; Shapiro, M.S. Direct measurement of resultant forces in the anterior cruciate ligament. An in vitro study performed with a new experimental technique. J. Bone Jt. Surg. Am. 1990, 72, 557–567. [Google Scholar] [CrossRef]
- Withrow, T.J.; Huston, L.J.; Wojtys, E.M.; Ashton-Miller, J.A. The relationship between quadriceps muscle force, knee flexion, and anterior cruciate ligament strain in an in vitro simulated jump landing. Am. J. Sports Med. 2006, 34, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Beynnon, B.D.; Fleming, B.C.; Johnson, R.J.; Nichols, C.E.; Renström, P.A.; Pope, M.H. Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am. J. Sports Med. 1995, 23, 24–34. [Google Scholar] [CrossRef]
- Beynnon, B.; Howe, J.; Pope, M.H.; Johnson, R.J.; Fleming, B. The measurement of anterior cruciate ligament strain in vivo. Int. Orthop. 1992, 16, 1–12. [Google Scholar] [CrossRef]
- Leppänen, M.; Pasanen, K.; Kujala, U.M.; Vasankari, T.; Kannus, P.; Äyrämö, S.; Krosshaug, T.; Bahr, R.; Avela, J.; Perttunen, J. Stiff landings are associated with increased ACL injury risk in young female basketball and floorball players. Am. J. Sports Med. 2017, 45, 386–393. [Google Scholar] [CrossRef]
- Devita, P.; Skelly, W.A. Effect of landing stiffness on joint kinetics and energetics in the lower extremity. Med. Sci. Sports Exerc. 1992, 24, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.-N.; Bates, B.T.; Dufek, J.S. Contributions of lower extremity joints to energy dissipation during landings. Med. Sci. Sports Exerc. 2000, 32, 812–819. [Google Scholar] [CrossRef]
- Donnelly, C.J.; Chinnasee, C.; Weir, G.; Sasimontonkul, S.; Alderson, J. Joint dynamics of rear-and fore-foot unplanned sidestepping. J. Sci. Med. Sport 2017, 20, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Cortes, N.; Morrison, S.; Van Lunen, B.L.; Onate, J.A. Landing technique affects knee loading and position during athletic tasks. J. Sci. Med. Sport 2012, 15, 175–181. [Google Scholar] [CrossRef] [Green Version]
- David, S.; Komnik, I.; Peters, M.; Funken, J.; Potthast, W. Identification and risk estimation of movement strategies during cutting maneuvers. J. Sci. Med. Sport 2017, 20, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Kunugi, S.; Mashimo, S.; Okuma, Y.; Masunari, A.; Miyazaki, S.; Hisajima, T.; Miyakawa, S. Effect of forefoot strike on lower extremity muscle activity and knee joint angle during cutting in female team handball players. Sports Med. Open 2016, 2, 32. [Google Scholar] [CrossRef] [Green Version]
- Burkhart, B.; Ford, K.R.; Myer, G.D.; Heidt, R.S., Jr.; Hewett, T.E. Anterior cruciate ligament tear in an athlete: Does increased heel loading contribute to ACL rupture? N. Am. J. Sports Phys. Ther. NAJSPT 2008, 3, 141–144. [Google Scholar] [PubMed]
- Hewit, J.; Cronin, J.; Button, C.; Hume, P. Understanding deceleration in sport. Strength Cond. J. 2011, 33, 47–52. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, J.J. Can muscle co-contraction protect knee ligaments after injury or repair? J. Bone Jt. Surg. Am. 1993, 75, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, B.C.; Renstrom, P.A.; Ohlen, G.; Johnson, R.J.; Peura, G.D.; Beynnon, B.D.; Badger, G.J. The gastrocnemius muscle is an antagonist of the anterior cruciate ligament. J. Orthop. Res. 2001, 19, 1178–1184. [Google Scholar] [CrossRef]
- Adouni, M.; Shirazi-Adl, A.; Marouane, H. Role of gastrocnemius activation in knee joint biomechanics: Gastrocnemius acts as an ACL antagonist. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E. Response to: ‘Why screening tests to predict injury do not work -and probably never will…: A critical review’. Br. J. Sports Med. 2016, 50, 1353. [Google Scholar] [CrossRef]
- Benjaminse, A.; Gokeler, A.; Dowling, A.V.; Faigenbaum, A.; Ford, K.R.; Hewett, T.E.; Onate, J.A.; Otten, B.; Myer, G.D. Optimization of the anterior cruciate ligament injury prevention paradigm: Novel feedback techniques to enhance motor learning and reduce injury risk. J. Orthop. Sport Phys. 2015, 45, 170–182. [Google Scholar] [CrossRef]
- Herrington, L.C.; Comfort, P. Training for prevention of ACL injury: Incorporation of progressive landing skill challenges into a program. Strength Cond. J. 2013, 35, 59–65. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recommended Camera | Variable | Observation | Score | ||
|---|---|---|---|---|---|
| Penultimate contact | |||||
| Side/20–45° |
| Y/N | Y = 0/N = 1 | ||
| Final Contact | |||||
| Front/20–45° |
| Wide, Moderate, Narrow | Wide = 2, Moderate = 1, Narrow = 0 | ||
| Front/20–45° |
| Y/N | Y = 1/N = 0 | ||
| Front/20–45° |
| Y/N | Y = 1/N = 0 | ||
| All 3 |
| Y/N | Y = 1/N = 0 | ||
| Front/20–45° |
| L/TR, U, M | L/TR = 2, U = 1, M = 0 | ||
| Side/20–45° |
| Y/N | Y = 1/N = 0 | ||
| Side/20–45° |
| Y/N | Y = 1/N = 0 | ||
| Front/20–45° |
| Y/N | Y = 1/N = 0 | ||
| Low CMAS ≤ 3 | Moderate CMAS 4–6 | High CMAS ≥ 7 | Score | /11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dos’Santos, T.; Thomas, C.; McBurnie, A.; Donelon, T.; Herrington, L.; Jones, P.A. The Cutting Movement Assessment Score (CMAS) Qualitative Screening Tool: Application to Mitigate Anterior Cruciate Ligament Injury Risk during Cutting. Biomechanics 2021, 1, 83-101. https://doi.org/10.3390/biomechanics1010007
Dos’Santos T, Thomas C, McBurnie A, Donelon T, Herrington L, Jones PA. The Cutting Movement Assessment Score (CMAS) Qualitative Screening Tool: Application to Mitigate Anterior Cruciate Ligament Injury Risk during Cutting. Biomechanics. 2021; 1(1):83-101. https://doi.org/10.3390/biomechanics1010007
Chicago/Turabian StyleDos’Santos, Thomas, Christopher Thomas, Alistair McBurnie, Thomas Donelon, Lee Herrington, and Paul A. Jones. 2021. "The Cutting Movement Assessment Score (CMAS) Qualitative Screening Tool: Application to Mitigate Anterior Cruciate Ligament Injury Risk during Cutting" Biomechanics 1, no. 1: 83-101. https://doi.org/10.3390/biomechanics1010007