Same Abbreviated Injury Scale Values May Be Associated with Different Risks to Mortality in Trauma Patients: A Cross-Sectional Retrospective Study Based on the Trauma Registry System in a Level I Trauma Center


 ,
, 
Abstract
:1. Background
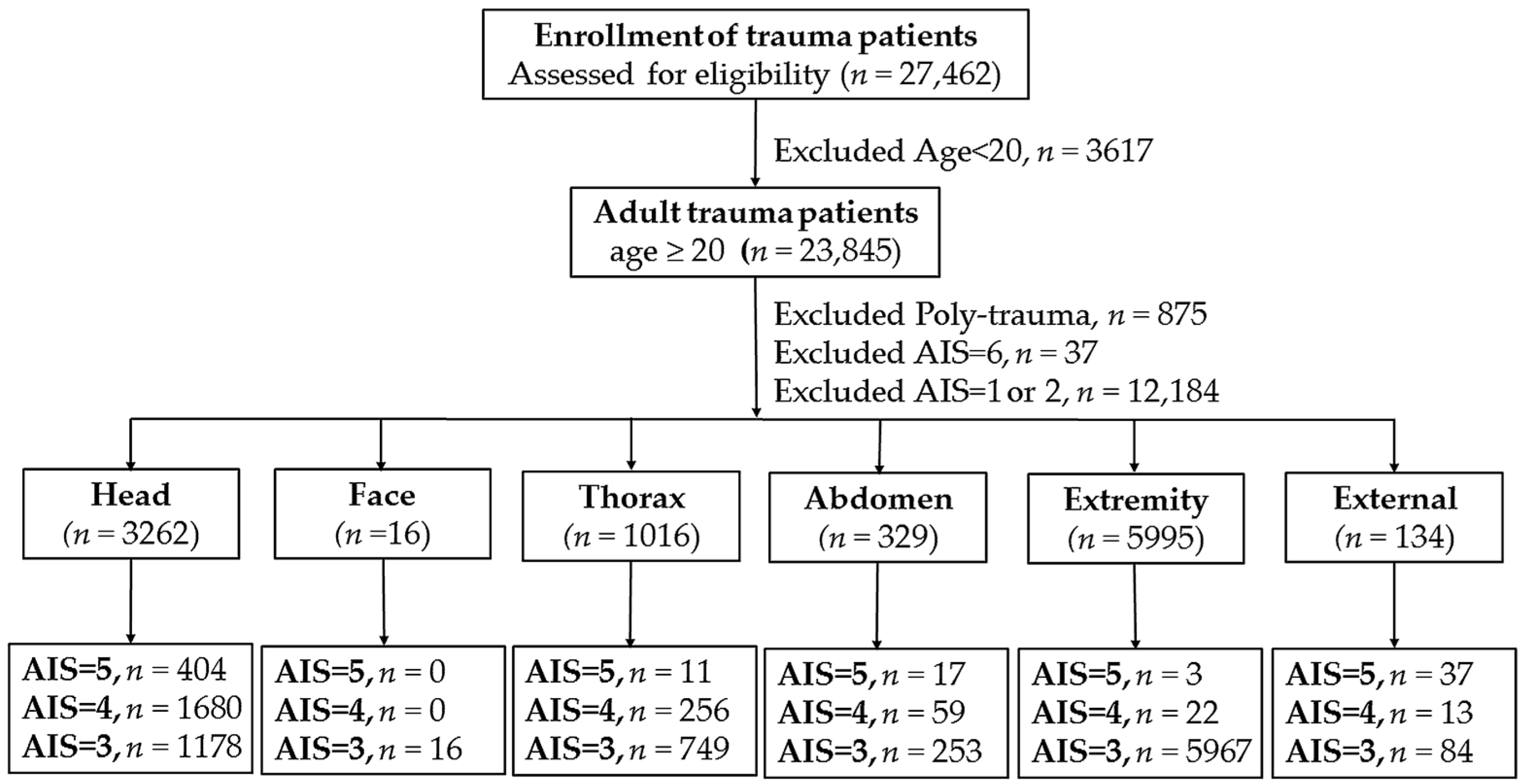
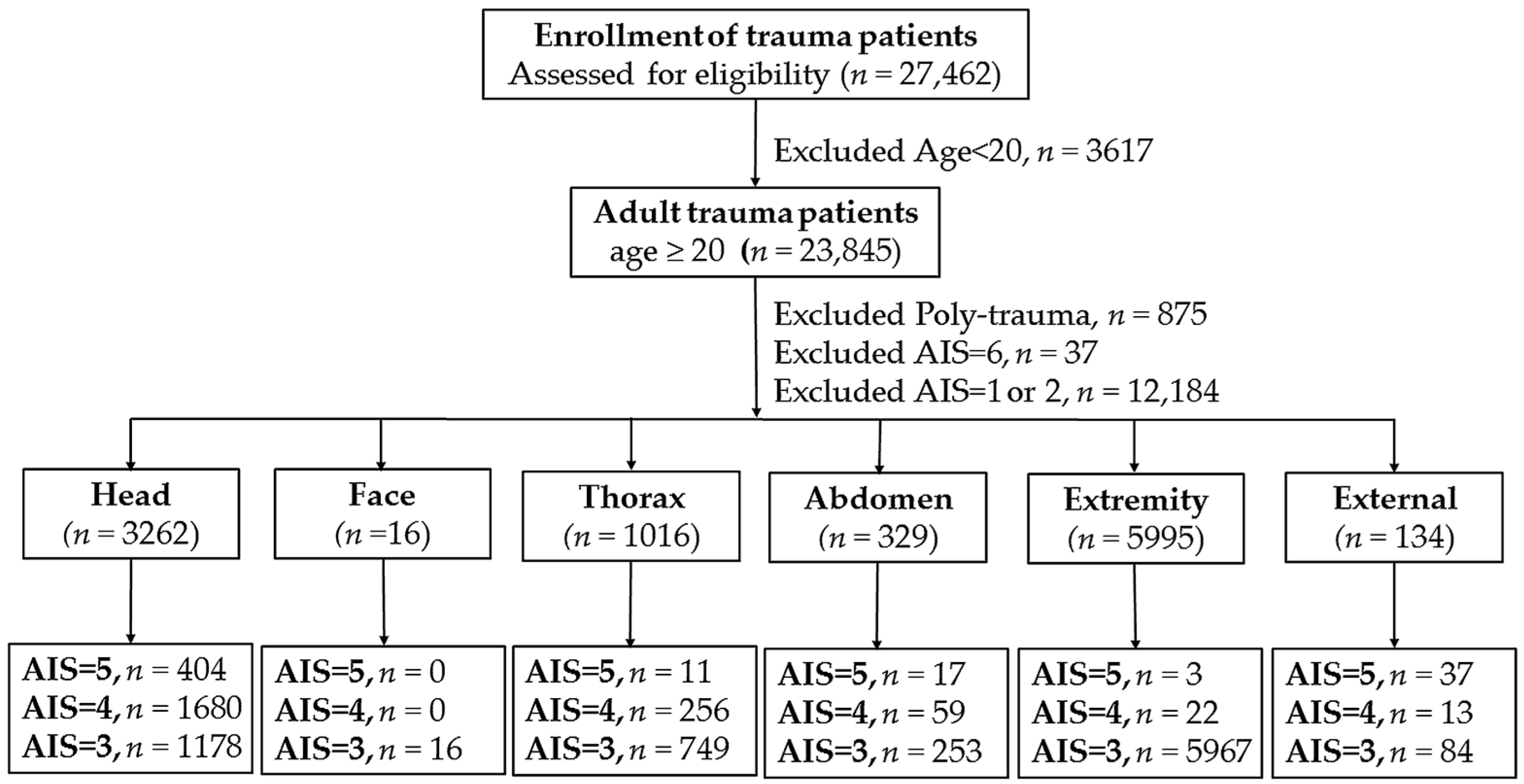
2. Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Injury Characteristics and Outcomes of Patients with AIS of 5
3.2. Injury Characteristics and Outcomes of Patients with AIS of 4
3.3. Injury Characteristics and Outcomes of Patients with AIS of 3
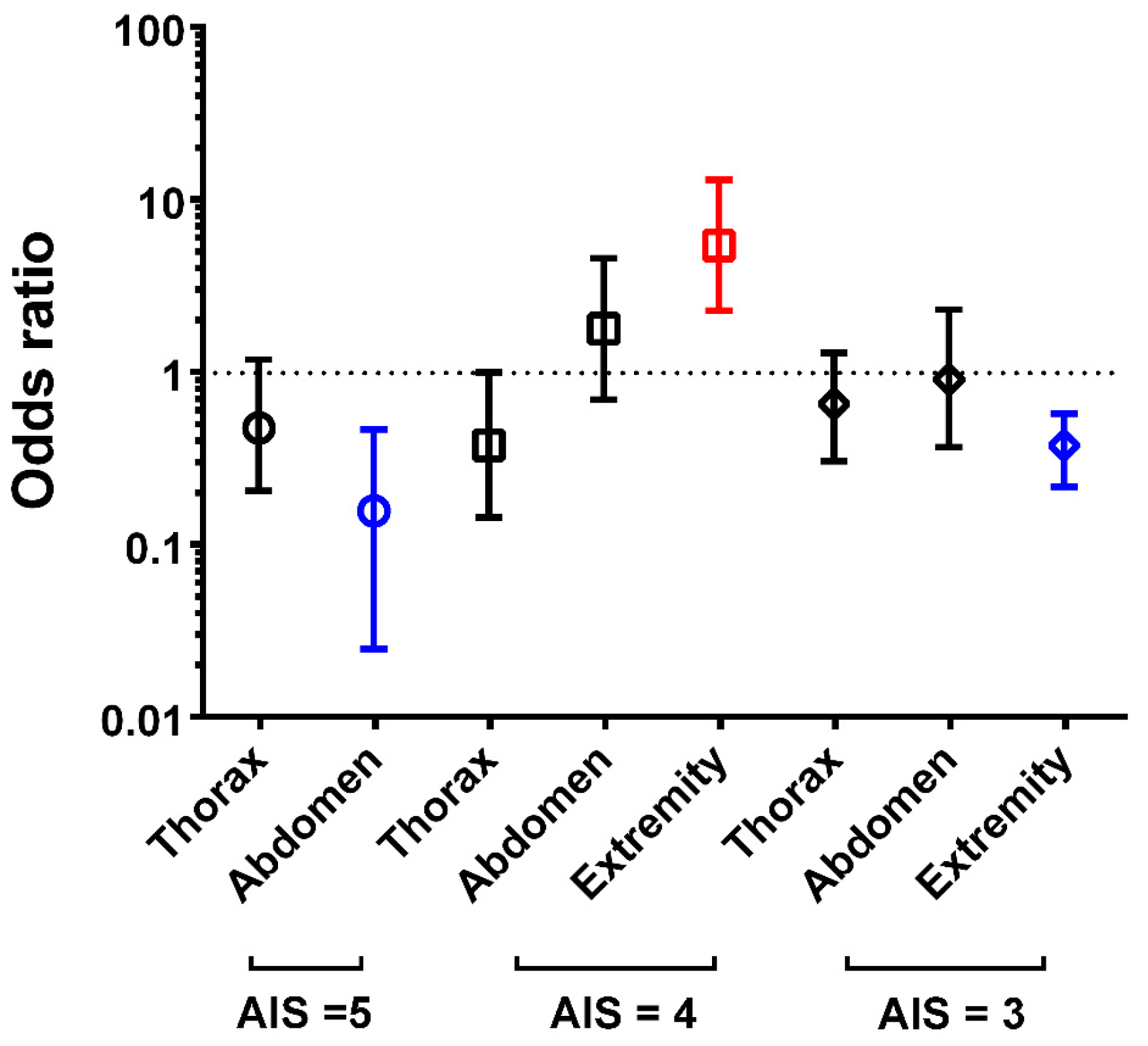
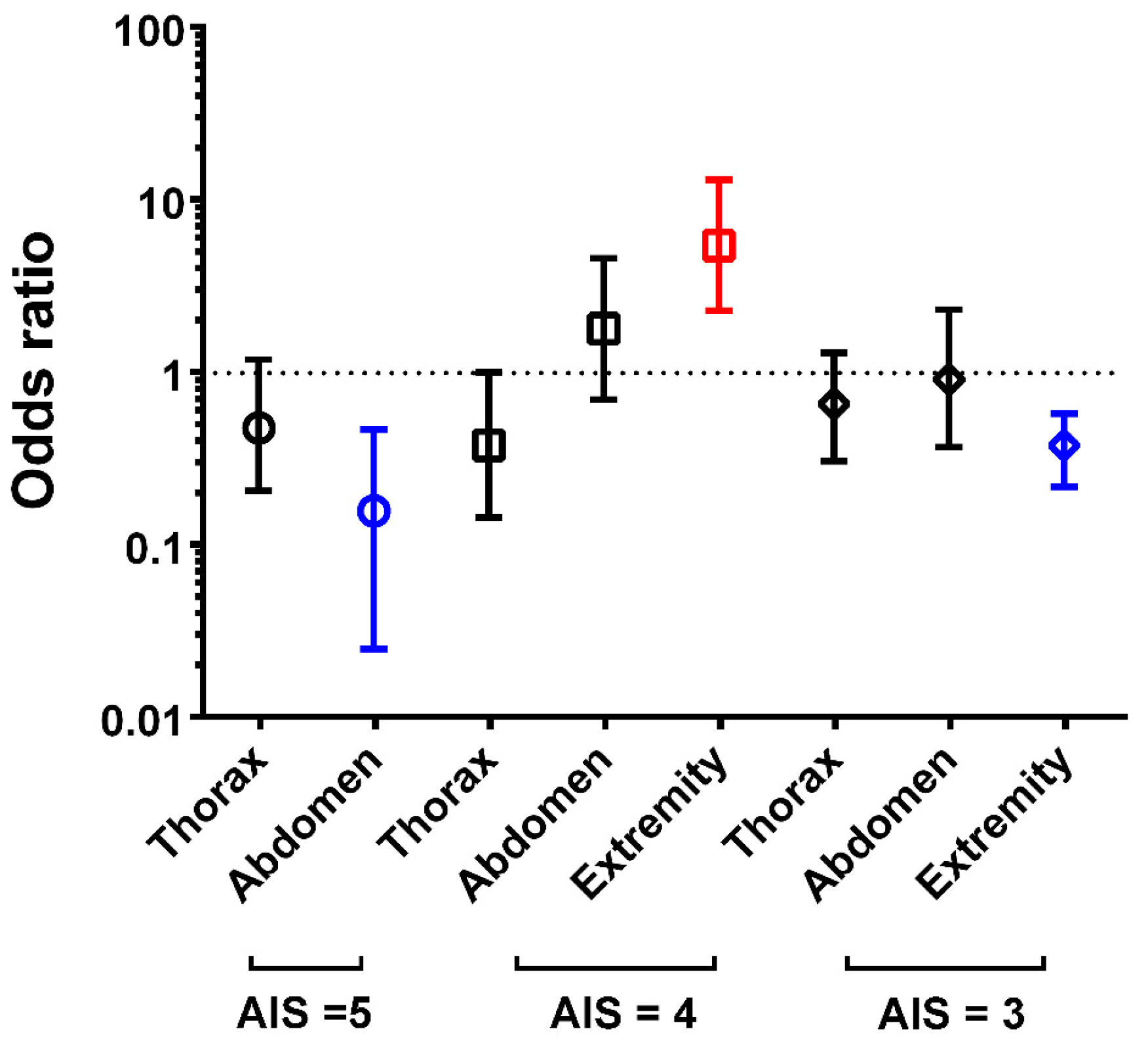
3.4. Summary of the Odds of Adjusted Mortality in the Patients
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rating the severity of tissue damage. I. The abbreviated scale. JAMA 1971, 215, 277–280.
- Baker, S.P.; O’Neill, B.; Haddon, W., Jr.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma Acute Care Surg. 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Osler, T.; Baker, S.P.; Long, W. A modification of the injury severity score that both improves accuracy and simplifies scoring. J. Trauma Acute Care Surg. 1997, 43, 922–925, discussion 925–926. [Google Scholar] [CrossRef]
- Wang, M.D.; Fan, W.H.; Qiu, W.S.; Zhang, Z.L.; Mo, Y.N.; Qiu, F. The exponential function transforms the Abbreviated Injury Scale, which both improves accuracy and simplifies scoring. Eur. J. Trauma Emerg. Surg. 2014, 40, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.C.H.; Kuo, P.J.; Chen, Y.C.; Chien, P.C.; Hsieh, H.Y.; Hsieh, C.H. Comparison of the new Exponential Injury Severity Score with the Injury Severity Score and the New Injury Severity Score in trauma patients: A cross-sectional study. PLoS ONE 2017, 12, e0187871. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Butcher, N.; Balogh, Z.J. AIS > 2 in at least two body regions: A potential new anatomical definition of polytrauma. Injury 2012, 43, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Beverland, D.E.; Rutherford, W.H. An assessment of the validity of the injury severity score when applied to gunshot wounds. Injury 1983, 15, 19–22. [Google Scholar] [CrossRef]
- Copes, W.S.; Champion, H.R.; Sacco, W.J.; Lawnick, M.M.; Keast, S.L.; Bain, L.W. The Injury Severity Score revisited. J. Trauma Acute Care Surg. 1988, 28, 69–77. [Google Scholar] [CrossRef]
- Van Belleghem, G.; Devos, S.; De Wit, L.; Hubloue, I.; Lauwaert, D.; Pien, K.; Putman, K. Predicting in-hospital mortality of traffic victims: A comparison between AIS-and ICD-9-CM-related injury severity scales when only ICD-9-CM is reported. Injury 2016, 47, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Weaver, A.A.; Barnard, R.T.; Kilgo, P.D.; Martin, R.S.; Stitzel, J.D. Mortality-based Quantification of Injury Severity for Frequently Occurring Motor Vehicle Crash Injuries. Ann. Adv. Automot. Med. 2013, 57, 235–246. [Google Scholar] [PubMed]
- Rowell, S.E.; Barbosa, R.R.; Diggs, B.S.; Schreiber, M.A.; Holcomb, J.B.; Wade, C.E.; Brasel, K.J.; Vercruysse, G.; MacLeod, J.; Dutton, R.P.; et al. Specific abbreviated injury scale values are responsible for the underestimation of mortality in penetrating trauma patients by the injury severity score. J. Trauma Acute Care Surg. 2011, 71, S384–S388. [Google Scholar] [CrossRef] [PubMed]
- Aharonson-Daniel, L.; Giveon, A.; Stein, M.; Peleg, K. Different AIS triplets: Different mortality predictions in identical ISS and NISS. J. Trauma Acute Care Surg. 2006, 61, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.; Halcomb, E.; Caldwell, E.; Sugrue, M. Differences in mortality predictions between Injury Severity Score triplets: A significant flaw. J. Trauma Acute Care Surg. 2004, 56, 1321–1324. [Google Scholar] [CrossRef]
- Kilgo, P.D.; Meredith, J.W.; Hensberry, R.; Osler, T.M. A note on the disjointed nature of the injury severity score. J. Trauma Acute Care Surg. 2004, 57, 479–485, discussion 486–487. [Google Scholar] [CrossRef]
- Stancin, T.; Kaugars, A.S.; Thompson, G.H.; Taylor, H.G.; Yeates, K.O.; Wade, S.L.; Drotar, D. Child and family functioning 6 and 12 months after a serious pediatric fracture. J. Trauma Acute Care Surg. 2001, 51, 69–76. [Google Scholar] [CrossRef]
- Michaels, A.J.; Madey, S.M.; Krieg, J.C.; Long, W.B. Traditional injury scoring underestimates the relative consequences of orthopedic injury. J. Trauma Acute Care Surg. 2001, 50, 389–395, discussion 396. [Google Scholar] [CrossRef]
- Beale, E.W.; Janis, J.E.; Minei, J.P.; Elliott, A.C.; Phelan, H.A. Predictors of failed primary abdominal closure in the trauma patient with an open abdomen. South. Med. J. 2013, 106, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Loh, S.A.; Rockman, C.B.; Chung, C.; Maldonado, T.S.; Adelman, M.A.; Cayne, N.S.; Pachter, H.L.; Mussa, F.F. Existing trauma and critical care scoring systems underestimate mortality among vascular trauma patients. J. Vasc. Surg. 2011, 53, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Rau, C.S.; Wu, S.C.; Chien, P.C.; Kuo, P.J.; Chen, Y.C.; Hsieh, H.Y.; Hsieh, C.H. Prediction of Mortality in Patients with Isolated Traumatic Subarachnoid Hemorrhage Using a Decision Tree Classifier: A Retrospective Analysis Based on a Trauma Registry System. Int. J. Environ. Res. Public Health 2017, 14, 1420. [Google Scholar] [CrossRef] [PubMed]
- Rau, C.S.; Wu, S.C.; Chen, Y.C.; Chien, P.C.; Hsieh, H.Y.; Kuo, P.J.; Hsieh, C.H. Effect of Age on Glasgow Coma Scale in Patients with Moderate and Severe Traumatic Brain Injury: An Approach with Propensity Score-Matched Population. Int. J. Environ. Res. Public Health 2017, 14, 1378. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.M.; Aquilino, A.; Cortese, F.; Scicchitano, P.; Sassara, M.; Mola, E.; Rollo, R.; Caldarola, P.; Giorgino, F.; Pomo, V.; et al. Feasibility and effectiveness of a disease and care management model in theprimary health care system for patients with heart failure and diabetes (Project Leonardo). Vasc. Health Risk Manag. 2010, 6, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C. Major trauma and the injury severity score—Where should we set the bar? Annu. Proc. Assoc. Adv. Automot. Med. 2007, 51, 13–29. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
| Variables | Head/Neck n = 404 | Thorax n = 11 | Abdomen n = 17 | |||
|---|---|---|---|---|---|---|
| Sex | ||||||
| Male, n (%) | 265 | (65.6) | 8 | (72.7) | 12 | (70.6) |
| Female, n (%) | 139 | (34.4) | 3 | (27.3) | 5 | (29.4) |
| Age (years) | 57.1 | ±19.3 | 49.8 | ±18.4 | 37.4 | ±15.5 |
| Co-morbidities | ||||||
| DM, n (%) | 63 | (15.6) | 1 | (9.1) | 1 | (5.9) |
| HTN, n (%) | 131 | (32.4) | 1 | (9.1) | 1 | (5.9) |
| CAD, n (%) | 22 | (5.4) | 0 | (0.0) | 0 | (0.0) |
| CHF, n (%) | 4 | (1.0) | 0 | (0.0) | 0 | (0.0) |
| CVA, n (%) | 22 | (5.4) | 0 | (0.0) | 0 | (0.0) |
| ESRD, n (%) | 17 | (4.2) | 0 | (0.0) | 0 | (0.0) |
| Mechanisms | ||||||
| Driver (motor vehicle), n (%) | 4 | (1.0) | 0 | (0.0) | 3 | (17.6) |
| Passenger (motor vehicle), n (%) | 4 | (1.0) | 1 | (9.1) | 1 | (5.9) |
| Driver (motorcycle), n (%) | 165 | (40.8) | 3 | (27.3) | 10 | (58.8) |
| Pillion (motorcycle), n (%) | 10 | (2.5) | 1 | (9.1) | 1 | (5.9) |
| Bicyclist, n (%) | 27 | (6.7) | 0 | (0.0) | 0 | (0.0) |
| Pedestrian, n (%) | 17 | (4.2) | 0 | (0.0) | 1 | (5.9) |
| Fall, n (%) | 163 | (40.3) | 6 | (54.5) | 1 | (5.9) |
| Struck by/against, n (%) | 14 | (3.5) | 0 | (0.0) | 0 | (0.0) |
| ISS | 26.3 | ±2.2 | 26.4 | ±2.0 | 27.3 | ±2.3 |
| Mortality, n (%) | 179 | (44.3) | 1 | (9.1) | 1 | (5.9) |
| Variables | Head/Neck n = 1680 | Thorax n = 256 | Abdomen n = 59 | Extremity n = 22 | ||||
|---|---|---|---|---|---|---|---|---|
| Sex | ||||||||
| Male, n (%) | 339 | (67.4) | 15 | (78.9) | 19 | (65.5) | 2 | (33.3) |
| Female, n (%) | 164 | (32.6) | 4 | (21.1) | 10 | (34.5) | 4 | (66.7) |
| Age (years) | 55.5 | ±19.2 | 46.7 | ±19.5 | 39.1 | ±16.0 | 44.2 | ±12.8 |
| Co-morbidities | ||||||||
| DM, n (%) | 78 | (15.5) | 1 | (5.3) | 1 | (3.4) | 0 | (0.0) |
| HTN, n (%) | 154 | (30.6) | 1 | (5.3) | 1 | (3.4) | 1 | (16.7) |
| CAD, n (%) | 24 | (5.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| CHF, n (%) | 4 | (0.8) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| CVA, n (%) | 23 | (4.6) | 1 | (5.3) | 0 | (0.0) | 0 | (0.0) |
| ESRD, n (%) | 17 | (3.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Mechanisms | ||||||||
| Driver (motor vehicle), n (%) | 11 | (2.2) | 1 | (5.3) | 6 | (20.7) | 0 | (0.0) |
| Passenger (motor vehicle), n (%) | 6 | (1.2) | 2 | (10.5) | 1 | (3.4) | 0 | (0.0) |
| Driver (motorcycle), n (%) | 226 | (44.9) | 9 | (47.4) | 16 | (55.2) | 2 | (33.3) |
| Pillion (motorcycle), n (%) | 12 | (2.4) | 1 | (5.3) | 1 | (3.4) | 2 | (33.3) |
| Bicyclist, n (%) | 31 | (6.2) | 0 | (0.0) | 0 | (0.0) | 1 | (16.7) |
| Pedestrian, n (%) | 24 | (4.8) | 0 | (0.0) | 1 | (3.4) | 0 | (0.0) |
| Fall, n (%) | 177 | (35.2) | 6 | (31.6) | 3 | (10.3) | 1 | (16.7) |
| Struck by/against, n (%) | 16 | (3.2) | 0 | (0.0) | 1 | (3.4) | 0 | (0.0) |
| ISS | 29.1 | ±6.8 | 33.5 | ±10.5 | 33.4 | ±8.2 | 36.3 | ±12.7 |
| Temperature (°C) | 36.4 | ±1.8 | 36.3 | ±0.7 | 36.3 | ±0.4 | 36.2 | ±0.2 |
| Heart rate (beats/min) | 91.6 | ±26.7 | 99.5 | ±21.1 | 100.3 | ±20.0 | 98.3 | ±24.4 |
| Respiratory rate (times/min) | 19.0 | ±4.8 | 22.7 | ±9.2 | 21.3 | ±4.5 | 23.0 | ±8.5 |
| Systolic blood pressure (mmHg) | 155.9 | ±48.9 | 122.8 | ±30.5 | 103.4 | ±27.6 | 105.7 | ±36.9 |
| AIS ≥ 3 in other region (s) | 99 | (19.7) | 8 | (42.1) | 12 | (41.4) | 3 | (50.0) |
| Mortality, n (%) | 229 | (45.5) | 5 | (26.3) | 1 | (3.4) | 3 | (50.0) |
| Thorax vs. Head/Neck | Abdomen vs. Head/Neck | |||||
|---|---|---|---|---|---|---|
| Variables | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | ||
| Sex | ||||||
| Male, n (%) | 1.8 | (0.59–5.55) | 0.331 | 0.9 | (0.42–2.02) | 0.840 |
| Female, n (%) | 0.6 | (0.18–1.69) | 0.331 | 1.1 | (0.50–2.39) | 0.840 |
| Age (years) | - | 0.050 | - | <0.001 | ||
| Co-morbidities | ||||||
| DM, n (%) | 0.3 | (0.04–2.30) | 0.334 | 0.2 | (0.03–1.45) | 0.103 |
| HTN, n (%) | 0.1 | (0.02–0.95) | 0.019 | 0.1 | (0.01–0.60) | 0.003 |
| CAD, n (%) | - | 0.615 | - | 0.388 | ||
| CHF, n (%) | - | 1.000 | - | 1.000 | ||
| CVA, n (%) | 1.2 | (0.15–9.07) | 1.000 | - | 0.391 | |
| ESRD, n (%) | - | 0.650 | - | 0.615 | ||
| Mechanisms | ||||||
| Driver (motor vehicle), n (%) | 2.5 | (0.30–20.30) | 0.362 | 11.7 | (3.97–34.33) | <0.001 |
| Passenger (motor vehicle), n (%) | 9.7 | (1.83–51.86) | 0.031 | 3.0 | (0.34–25.42) | 0.326 |
| Driver (motorcycle), n (%) | 1.1 | (0.44–2.76) | 1.000 | 1.5 | (0.71–3.20) | 0.339 |
| Pillion (motorcycle), n (%) | 2.3 | (0.28–18.44) | 0.386 | 1.5 | (0.18–11.64) | 1.000 |
| Bicyclist, n (%) | - | 0.402 | - | 0.247 | ||
| Pedestrian, n (%) | - | 0.618 | 0.7 | (0.09–5.46) | 1.000 | |
| Fall, n (%) | 0.9 | (0.32–2.28) | 0.812 | 0.2 | (0.06–0.71) | 0.007 |
| Struck by/against, n (%) | - | 0.659 | 1.1 | (0.14–8.49) | 1.000 | |
| ISS | - | 0.090 | - | 0.009 | ||
| Temperature (°C) | - | 0.696 | - | 0.678 | ||
| Heart rate (beats/min) | - | 0.204 | - | 0.085 | ||
| Respiratory rate (times/min) | - | 0.100 | - | 0.013 | ||
| Systolic blood pressure (mmHg) | - | 0.004 | - | <0.001 | ||
| AIS ≥ 3 in other region (s) | 3.0 | (1.16–7.57) | 0.024 | 2.8 | (1.33–6.23) | 0.009 |
| Mortality, n (%) | 0.4 | (0.15–1.20) | 0.107 | 0.04 | (0.01–0.32) | <0.001 |
| Adjusted mortality | 0.4 | (0.14–1.25) | 0.118 | 0.1 | (0.01–0.39) | 0.004 |
| Log-Rank test | - | 0.219 | - | <0.001 | ||
| Variables | Head/Neck n = 1680 | Thorax n = 256 | Abdomen n = 59 | Extremity n = 22 | ||||
|---|---|---|---|---|---|---|---|---|
| Sex | ||||||||
| Male, n (%) | 1077 | (64.1) | 191 | (74.6) | 37 | (62.7) | 12 | (54.5) |
| Female, n (%) | 603 | (35.9) | 65 | (25.4) | 22 | (37.3) | 10 | (45.5) |
| Age (years) | 58.0 | ±19.4 | 52.1 | ±15.2 | 40.9 | ±16.8 | 56.0 | ±19.3 |
| Co-morbidities | ||||||||
| DM, n (%) | 324 | (19.3) | 37 | (14.5) | 2 | (3.4) | 1 | (4.5) |
| HTN, n (%) | 591 | (35.2) | 60 | (23.4) | 5 | (8.5) | 2 | (9.1) |
| CAD, n (%) | 89 | (5.3) | 8 | (3.1) | 0 | (0.0) | 0 | (0.0) |
| CHF, n (%) | 14 | (0.8) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| CVA, n (%) | 114 | (6.8) | 8 | (3.1) | 0 | (0.0) | 0 | (0.0) |
| ESRD, n (%) | 54 | (3.2) | 1 | (0.4) | 1 | (1.7) | 0 | (0.0) |
| Mechanisms | ||||||||
| Driver (motor vehicle), n (%) | 13 | (0.8) | 16 | (6.2 | 11 | (18.6) | 0 | (0.0) |
| Passenger (motor vehicle), n (%) | 9 | (0.5) | 6 | (2.3) | 2 | (3.4) | 1 | (4.5) |
| Driver (motorcycle), n (%) | 749 | (44.6) | 157 | (61.3) | 31 | (52.5) | 9 | (40.9) |
| Pillion (motorcycle), n (%) | 28 | (1.7) | 3 | (1.2) | 0 | (0.0) | 0 | (0.0) |
| Bicyclist, n (%) | 90 | (5.4) | 3 | (1.2) | 2 | (3.4) | 3 | (13.6) |
| Pedestrian, n (%) | 67 | (4.0) | 9 | (3.5) | 1 | (1.7) | 0 | (0.0) |
| Fall, n (%) | 663 | (39.5) | 46 | (18.0) | 6 | (10.2) | 5 | (22.7) |
| Struck by/against, n (%) | 61 | (3.6) | 16 | (6.2) | 6 | (10.2) | 4 | (18.2) |
| ISS | 17.7 | ±2.5 | 19.0 | ±2.7 | 18.0 | ±2.4 | 17.7 | ±2.1 |
| Temperature (°C) | 36.5 | ±1.1 | 36.5 | ±0.7 | 36.4 | ±0.8 | 36.4 | ±1.1 |
| Heart rate (beats/min) | 86.2 | ±18.5 | 93.6 | ±18.8 | 89.9 | ±19.3 | 103.9 | ±25.2 |
| Respiratory rate (times/min) | 18.7 | ±2.6 | 19.2 | ±2.7 | 19.2 | ±2.6 | 20.8 | ±4.8 |
| Systolic blood pressure (mmHg) | 156.6 | ±35.3 | 141.9 | ±33.4 | 118.6 | ±31.6 | 101.8 | ±42.7 |
| Mortality, n (%) | 80 | (4.8) | 3 | (1.2) | 4 | (6.8) | 5 | (22.7) |
| Thorax vs. Head/Neck | Abdomen vs. Head/Neck | Extremity vs. Head/Neck | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |||
| Sex | |||||||||
| Male, n (%) | 1.6 | (1.22–2.22) | 0.001 | 0.9 | (0.55–1.61) | 0.890 | 0.7 | (0.29–1.56) | 0.376 |
| Female, n (%) | 0.6 | (0.45–0.82) | 0.001 | 1.1 | (0.62–1.82) | 0.890 | 1.5 | (0.64–3.47) | 0.376 |
| Age (years) | - | <0.001 | - | <0.001 | - | 0.622 | |||
| Co-morbidities | |||||||||
| DM, n (%) | 0.7 | (0.49–1.02) | 0.070 | 0.1 | (0.04–0.61) | 0.002 | 0.2 | (0.03–1.49) | 0.100 |
| HTN, n (%) | 0.6 | (0.42–0.77) | <0.001 | 0.2 | (0.07–0.43) | <0.001 | 0.2 | (0.04–0.79) | 0.011 |
| CAD, n (%) | 0.6 | (0.28–1.20) | 0.166 | - | 0.071 | - | 0.408 | ||
| CHF, n (%) | - | 0.238 | - | 1.000 | - | 1.000 | |||
| CVA, n (%) | 0.4 | (0.21–0.92) | 0.026 | - | 0.052 | - | 0.394 | ||
| ESRD, n (%) | 0.1 | (0.02–0.86) | 0.013 | 0.5 | (0.07–3.82) | 0.721 | - | 0.642 | |
| Mechanisms | |||||||||
| Driver (motor vehicle), n (%) | 8.5 | (4.06–17.99) | <0.001 | 29.4 | (12.53–68.94) | <0.001 | - | 1.000 | |
| Passenger (motor vehicle), n (%) | 4.5 | (1.57–12.63) | 0.009 | 6.5 | (1.38–30.84) | 0.051 | 8.8 | (1.07–72.95) | 0.122 |
| Driver (motorcycle), n (%) | 2.0 | (1.51–2.58) | <0.001 | 1.4 | (0.82–2.32) | 0.234 | 0.9 | (0.37–2.02) | 0.831 |
| Pillion (motorcycle), n (%) | 0.7 | (0.21–2.32) | 0.616 | - | 0.623 | - | 1.000 | ||
| Bicyclist, n (%) | 0.2 | (0.07–0.67) | 0.004 | 0.6 | (0.15–2.58) | 0.584 | 2.8 | (0.81–9.60) | 0.115 |
| Pedestrian, n (%) | 0.9 | (0.43–1.78) | 0.738 | 0.4 | (0.06–3.04) | 0.515 | - | 0.625 | |
| Fall, n (%) | 0.3 | (0.24–0.47) | <0.001 | 0.2 | (0.07–0.41) | <0.001 | 0.5 | (0.17–1.23) | 0.127 |
| Struck by/against, n (%) | 1.8 | (1.00–3.12) | 0.057 | 3.0 | (1.24–7.26) | 0.024 | 5.9 | (1.94–17.95) | 0.008 |
| ISS | - | <0.001 | - | 0.451 | - | 0.991 | |||
| Temperature (°C) | - | 0.306 | - | 0.728 | - | 0.839 | |||
| Heart rate (beats/min) | - | <0.001 | - | 0.131 | - | 0.004 | |||
| Respiratory rate (times/min) | - | 0.004 | - | 0.158 | - | 0.053 | |||
| Systolic blood pressure (mmHg) | - | <0.001 | - | <0.001 | - | <0.001 | |||
| Mortality, n (%) | 0.2 | (0.07–0.76) | 0.012 | 1.5 | (0.51–4.11) | 0.528 | 5.9 | (2.12–16.35) | 0.004 |
| Adjusted mortality | 0.3 | (0.09–1.01) | 0.051 | 2.1 | (0.64–6.80) | 0.220 | 8.4 | (2.84–25.07) | <0.001 |
| Log-Rank test | - | 0.003 | - | 0.713 | - | 0.028 | |||
| Variables | Head/Neck n = 1178 | Thorax n = 749 | Abdomen n = 253 | Extremity n = 5967 | ||||
|---|---|---|---|---|---|---|---|---|
| Sex | ||||||||
| Male, n (%) | 686 | (58.2) | 517 | (69.0) | 151 | (59.7) | 2599 | (43.6) |
| Female, n (%) | 492 | (41.8) | 232 | (31.0) | 102 | (40.3) | 3368 | (56.4) |
| Age (years) | 54.2 | ±18.7 | 54.6 | ±16.1 | 48.5 | ±18.0 | 62.2 | ±19.9 |
| Co-morbidities | ||||||||
| DM, n (%) | 177 | (15.0) | 119 | (15.9) | 34 | (13.4) | 1373 | (23.0) |
| HTN, n (%) | 371 | (31.5) | 211 | (28.2) | 55 | (21.7) | 2519 | (42.4) |
| CAD, n (%) | 36 | (3.1) | 20 | (2.7) | 6 | (2.4) | 379 | (6.4) |
| CHF, n (%) | 12 | (1.0) | 4 | (0.5) | 2 | (0.8) | 100 | (1.7) |
| CVA, n (%) | 59 | (5.0) | 17 | (2.3) | 6 | (2.4) | 490 | (8.2) |
| ESRD, n (%) | 20 | (1.7) | 10 | (1.3) | 1 | (0.4) | 191 | (3.2) |
| Mechanisms | ||||||||
| Driver (motor vehicle), n (%) | 21 | (1.8) | 31 | (4.1) | 18 | (7.1) | 56 | (0.9) |
| Passenger (motor vehicle), n (%) | 14 | (1.2) | 12 | (1.6) | 6 | (2.4) | 28 | (0.5) |
| Driver (motorcycle), n (%) | 650 | (55.2) | 432 | (57.7) | 99 | (39.1) | 1848 | (31.0) |
| Pillion (motorcycle), n (%) | 31 | (2.6) | 13 | (1.7) | 4 | (1.6) | 125 | (2.1) |
| Bicyclist, n (%) | 63 | (5.3) | 23 | (3.1) | 3 | (1.2) | 232 | (3.9) |
| Pedestrian, n (%) | 37 | (3.1) | 12 | (1.6) | 4 | (1.6) | 115 | (1.9) |
| Fall, n (%) | 310 | (26.3) | 173 | (23.1) | 92 | (36.4) | 3317 | (55.6) |
| Struck by/against, n (%) | 52 | (4.4) | 53 | (7.1) | 27 | (10.7) | 246 | (4.1) |
| ISS | 11.0 | ±2.4 | 11.7 | ±2.5 | 10.4 | ±2.0 | 9.3 | ±1.1 |
| Temperature (°C) | 36.5 | ±1.1 | 36.5 | ±0.7 | 36.4 | ±0.8 | 36.4 | ±1.1 |
| Heart rate (beats/min) | 86.2 | ±18.5 | 93.6 | ±18.8 | 89.9 | ±19.3 | 103.9 | ±25.2 |
| Respiratory rate (times/min) | 18.7 | ±2.6 | 19.2 | ±2.7 | 19.2 | ±2.6 | 20.8 | ±4.8 |
| Systolic blood pressure (mmHg) | 156.6 | ±35.3 | 141.9 | ±33.4 | 118.6 | ±31.6 | 101.8 | ±42.7 |
| Mortality, n (%) | 19 | (1.6) | 7 | (0.9) | 4 | (1.6) | 47 | (0.8) |
| Thorax vs. Head/Neck | Abdomen vs. Head/Neck | Extremity vs. Head/Neck | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |||
| Sex | |||||||||
| Male, n (%) | 1.6 | (1.32–1.94) | <0.001 | 1.1 | (0.81–1.40) | 0.674 | 0.6 | (0.49–0.63) | <0.001 |
| Female, n (%) | 0.6 | (0.52–0.76) | <0.001 | 0.9 | (0.71–1.24) | 0.674 | 1.8 | (1.59–2.05) | <0.001 |
| Age (years) | - | 0.625 | - | <0.001 | - | <0.001 | |||
| Co-morbidities | |||||||||
| DM, n (%) | 1.1 | (0.83–1.38) | 0.650 | 0.9 | (0.59–1.30) | 0.559 | 1.7 | (1.43–2.01) | <0.001 |
| HTN, n (%) | 0.9 | (0.70–1.04) | 0.127 | 0.6 | (0.44–0.84) | 0.002 | 1.6 | (1.39–1.82) | <0.001 |
| CAD, n (%) | 0.9 | (0.50–1.52) | 0.678 | 0.8 | (0.32–1.85) | 0.684 | 2.2 | (1.52–3.05) | <0.001 |
| CHF, n (%) | 0.5 | (0.17–1.62) | 0.310 | 0.8 | (0.17–3.48) | 1.000 | 1.7 | (0.91–3.02) | 0.122 |
| CVA, n (%) | 0.4 | (0.26–0.76) | 0.003 | 0.5 | (0.20–1.08) | 0.094 | 1.7 | (1.29–2.24) | <0.001 |
| ESRD, n (%) | 0.8 | (0.37–1.68) | 0.577 | 0.2 | (0.03–1.72) | 0.153 | 1.9 | (1.20–3.05) | 0.006 |
| Mechanisms | |||||||||
| Driver (motor vehicle), n (%) | 2.4 | (1.36–4.17) | 0.002 | 4.2 | (2.21–8.04) | <0.001 | 0.5 | (0.32–0.87) | 0.014 |
| Passenger (motor vehicle), n (%) | 1.4 | (0.62–2.94) | 0.544 | 2.0 | (0.77–5.31) | 0.232 | 0.4 | (0.21–0.75) | 0.006 |
| Driver (motorcycle), n (%) | 1.1 | (0.92–1.33) | 0.300 | 0.5 | (0.40–0.69) | <0.001 | 0.4 | (0.32–0.41) | <0.001 |
| Pillion (motorcycle), n (%) | 0.7 | (0.34–1.26) | 0.215 | 0.6 | (0.21–1.70) | 0.381 | 0.8 | (0.53–1.18) | 0.274 |
| Bicyclist, n (%) | 0.6 | (0.35–0.91) | 0.023 | 0.2 | (0.07–0.68) | 0.004 | 0.7 | (0.54–0.95) | 0.025 |
| Pedestrian, n (%) | 0.5 | (0.26–0.97) | 0.038 | 0.5 | (0.18–1.40) | 0.216 | 0.6 | (0.42–0.88) | 0.011 |
| Fall, n (%) | 0.8 | (0.68–1.04) | 0.118 | 1.6 | (1.20–2.13) | 0.002 | 3.5 | (3.05–4.03) | <0.001 |
| Struck by/against, n (%) | 1.6 | (1.11–2.45) | 0.013 | 2.6 | (1.59–4.21) | <0.001 | 0.9 | (0.69–1.26) | 0.690 |
| ISS | - | <0.001 | - | <0.001 | - | <0.001 | |||
| Temperature (°C) | - | 0.710 | - | 0.918 | - | 0.103 | |||
| Heart rate (beats/min) | - | 0.377 | - | 0.055 | - | 0.573 | |||
| Respiratory rate (times/min) | - | 0.699 | - | 0.330 | - | 0.074 | |||
| Systolic blood pressure (mmHg) | - | 0.038 | - | <0.001 | - | 0.499 | |||
| Mortality, n (%) | 0.6 | (0.24–1.38) | 0.231 | 1.0 | (0.33–2.91) | 1.000 | 0.5 | (0.28–0.83) | 0.009 |
| Adjusted mortality | 0.6 | (0.23–1.40) | 0.218 | 0.9 | (0.29–2.89) | 0.875 | 0.3 | (0.15–0.51) | <0.001 |
| Log-Rank test | - | 0.100 | - | 0.719 | - | 0.001 | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rau, C.-S.; Wu, S.-C.; Kuo, P.-J.; Chen, Y.-C.; Chien, P.-C.; Hsieh, H.-Y.; Hsieh, C.-H. Same Abbreviated Injury Scale Values May Be Associated with Different Risks to Mortality in Trauma Patients: A Cross-Sectional Retrospective Study Based on the Trauma Registry System in a Level I Trauma Center. Int. J. Environ. Res. Public Health 2017, 14, 1552. https://doi.org/10.3390/ijerph14121552
Rau C-S, Wu S-C, Kuo P-J, Chen Y-C, Chien P-C, Hsieh H-Y, Hsieh C-H. Same Abbreviated Injury Scale Values May Be Associated with Different Risks to Mortality in Trauma Patients: A Cross-Sectional Retrospective Study Based on the Trauma Registry System in a Level I Trauma Center. International Journal of Environmental Research and Public Health. 2017; 14(12):1552. https://doi.org/10.3390/ijerph14121552
Chicago/Turabian StyleRau, Cheng-Shyuan, Shao-Chun Wu, Pao-Jen Kuo, Yi-Chun Chen, Peng-Chen Chien, Hsiao-Yun Hsieh, and Ching-Hua Hsieh. 2017. "Same Abbreviated Injury Scale Values May Be Associated with Different Risks to Mortality in Trauma Patients: A Cross-Sectional Retrospective Study Based on the Trauma Registry System in a Level I Trauma Center" International Journal of Environmental Research and Public Health 14, no. 12: 1552. https://doi.org/10.3390/ijerph14121552