
User-Informed Adaptation in IoT Home Healthcare: Grounding Development in Empirical Evidence



Abstract
:1. Introduction
2. Related Work and Research Procedure
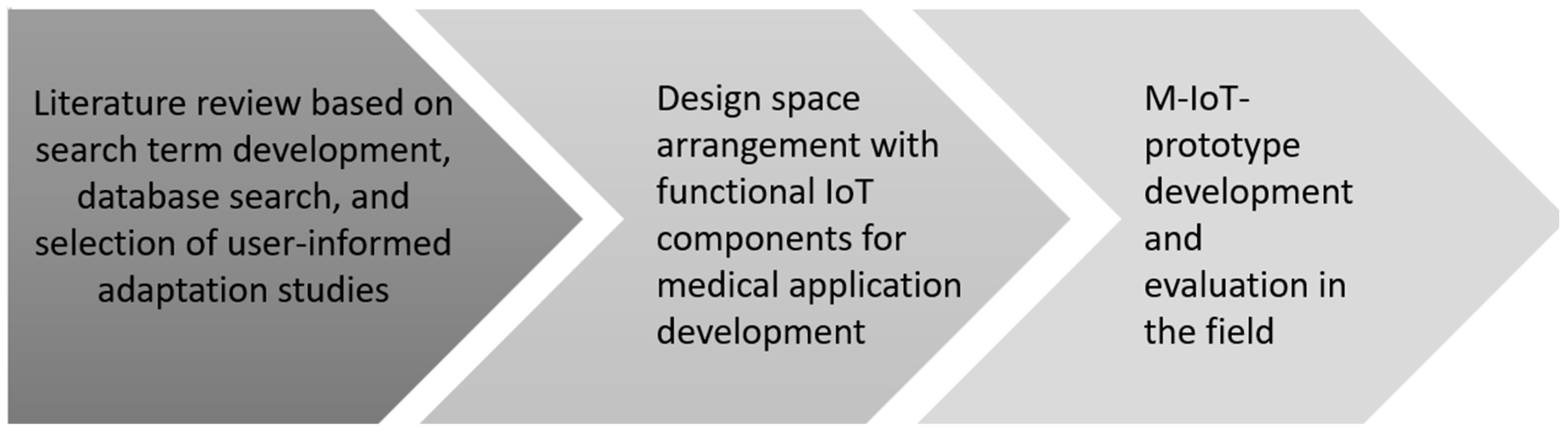
2.1. Methodology
2.1.1. Literature Review
Step 1: Search for Technological and Empirical Evidence
Step 2: Selection of Papers for Analysis
Step 3: Structured Analysis
2.1.2. Result Generation
Step 4: Development of Adaptation Concept and Hardware for the Prototype
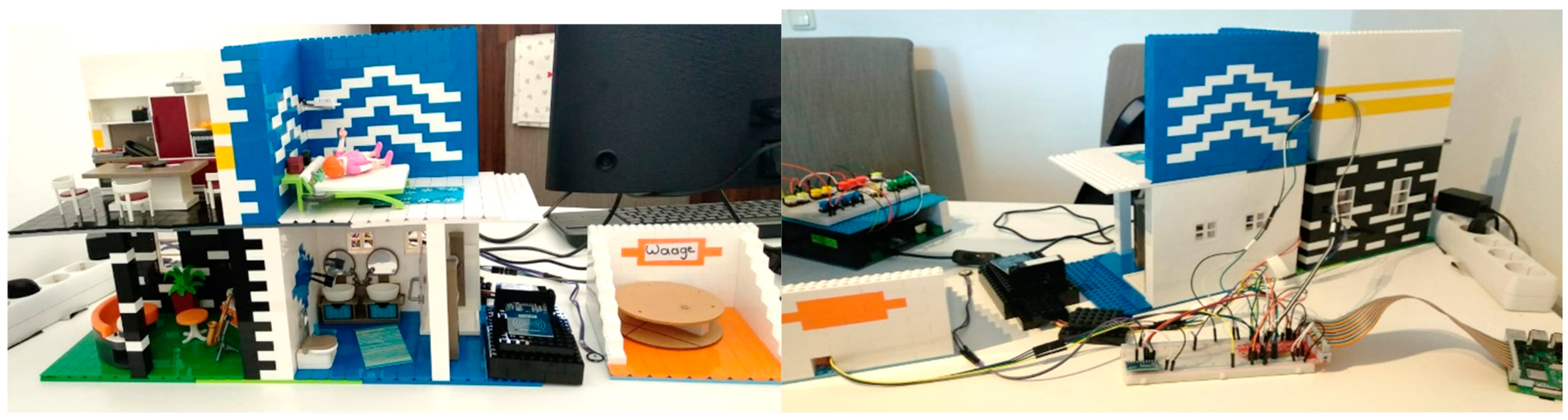
Step 5: Development of T-Care Prototype
Step 6: User Tests
2.2. Literature Analysis
2.3. Structuring the Design Space
2.3.1. Sensors and Actuators
- Physiological sensors: Heart rate, ECG, EEG, skin temperature, respiration rate (interval), blood pressure gauge
- Environmental sensors: Air temperature, smoke sensor, gas sensor, air humidity, air pressure, UV, NO2, noise sensor
- Sensors for data exchange: RFID, NFC
- Force transducer sensors: Weight sensor, load cells pressure cushion
- Movement detection: Ultrasonic sensor, proximity sensor, IR sensor, accelerator, intertial sensor
- Image Processing: Camera
- Close Distance: Vibrating motor, display
- Wide Distance: Light, beeper, speaker
2.3.2. Adaptation Concepts
3. Results
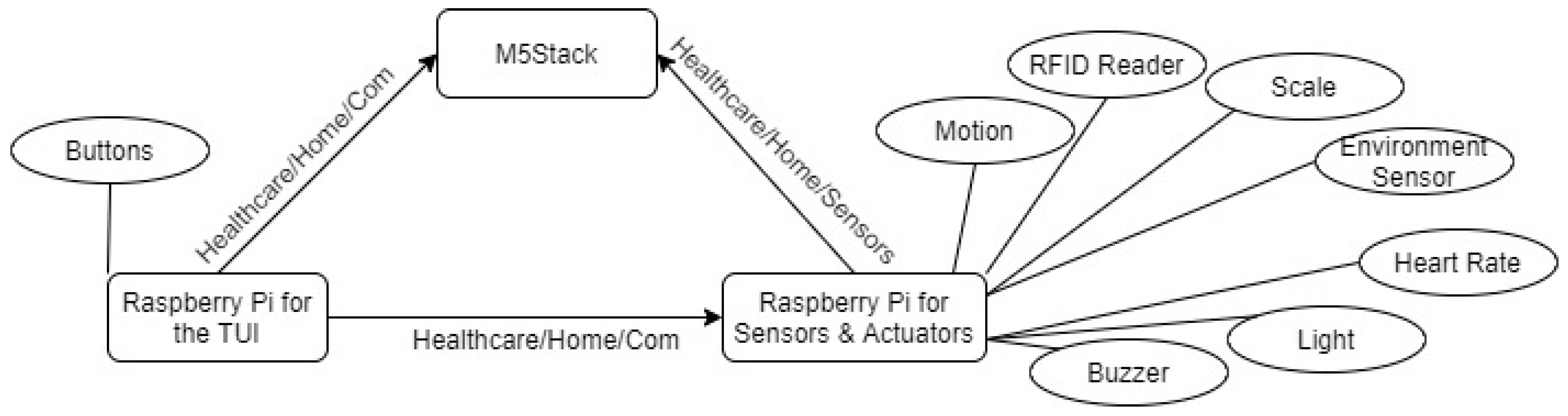
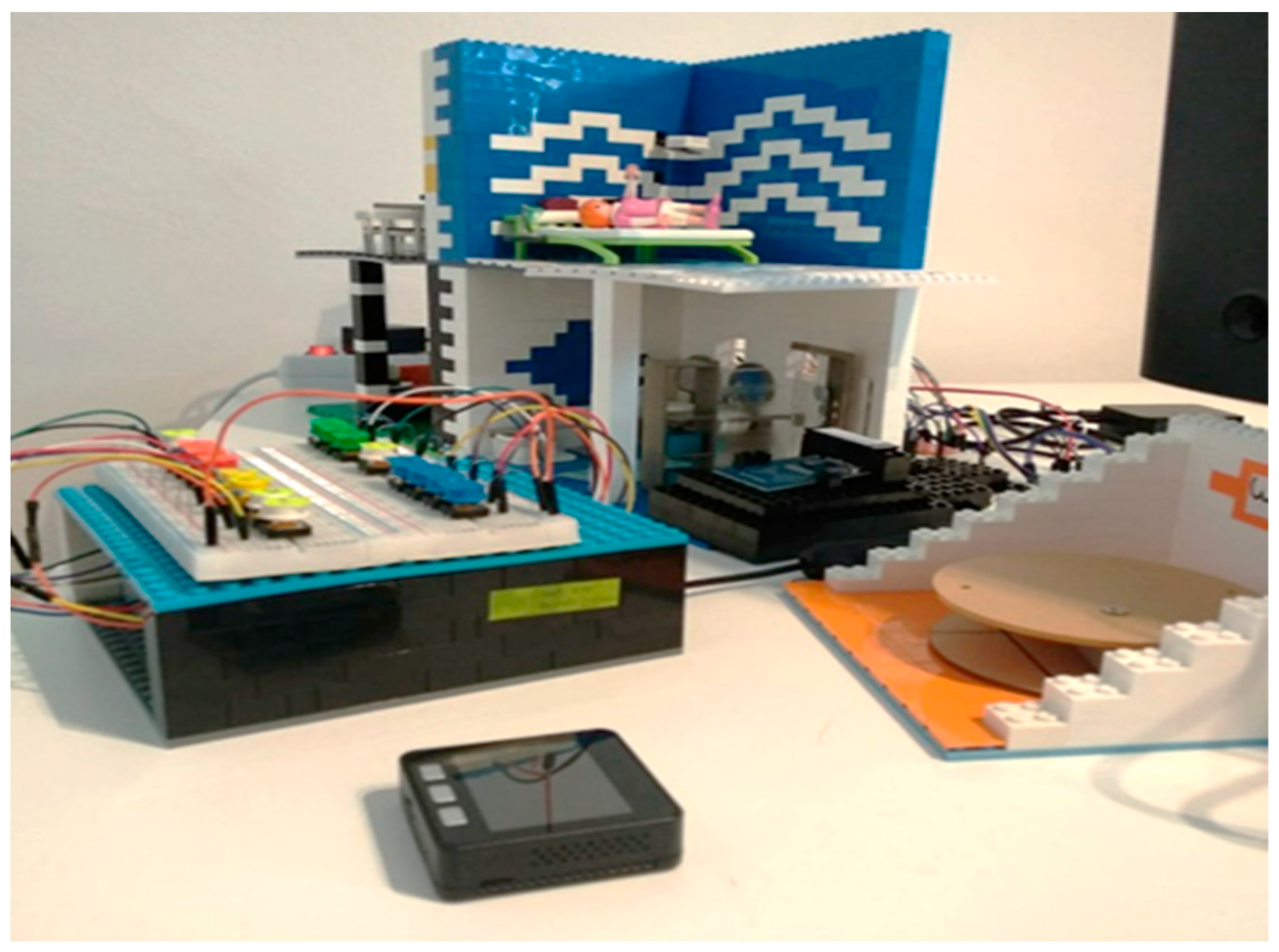
3.1. T-Care: M-IoT Prototype for User-Informed Home Healthcare
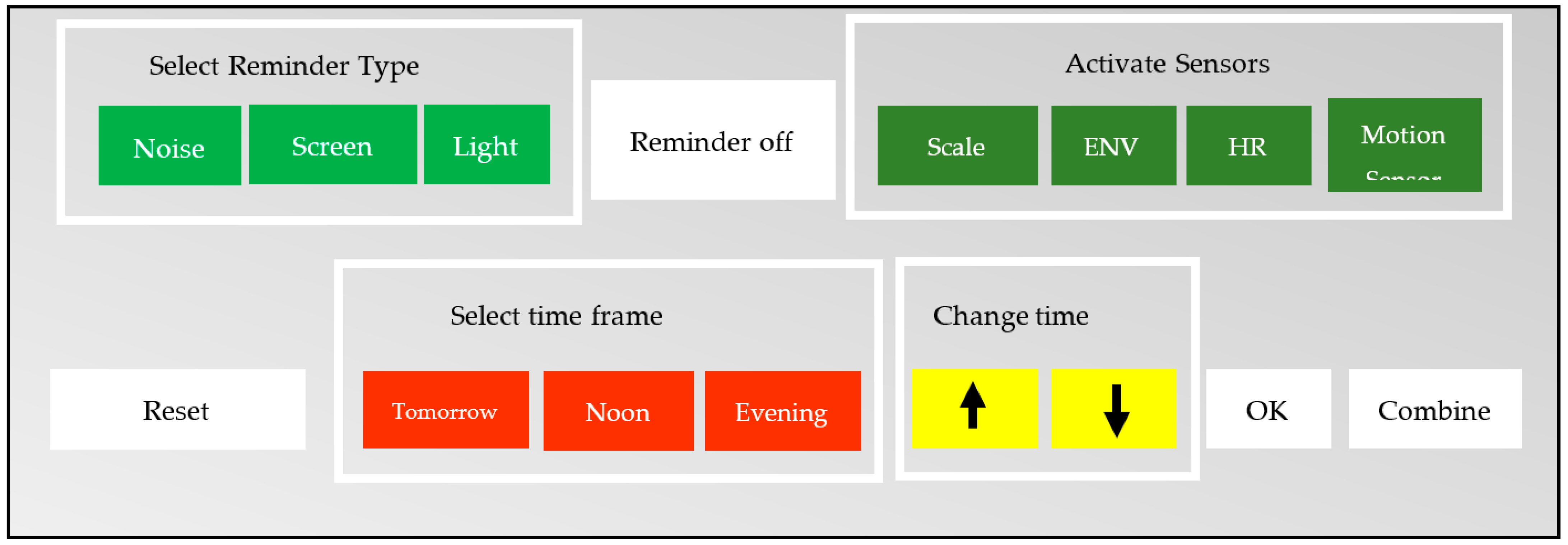
3.1.1. User Interface
3.1.2. Functionality
- Activate/deactivate different sensors for monitoring and control: Scale, Environment sensor, Heart rate sensor, Motion sensor;
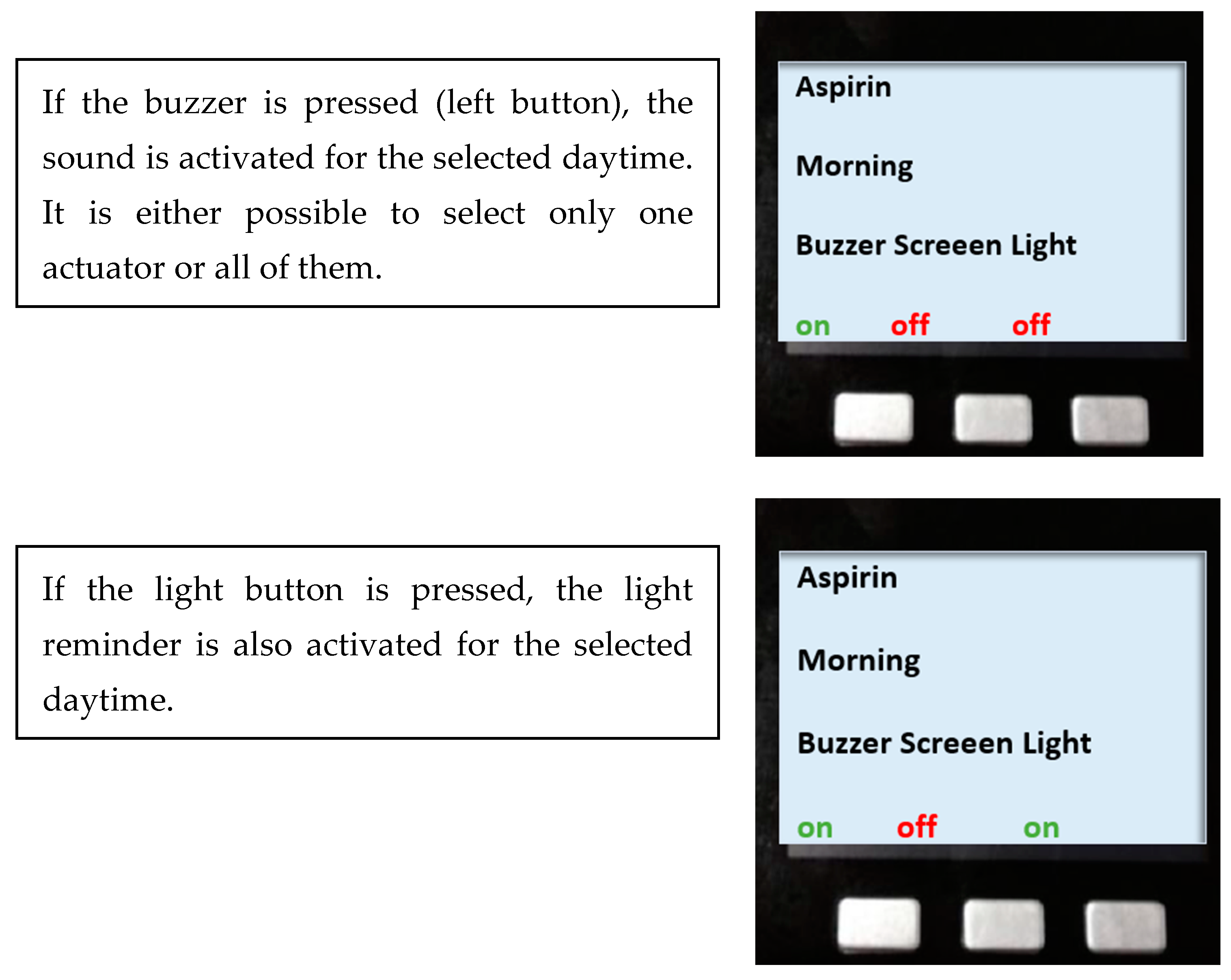
- Change medication reminder settings: Change kind of reminder (buzzer, screen, light), Change time of reminder;
- Turn off the reminder;
- Reset reminder settings to the default settings.
- Scale: If the scale is active, the medication can be placed on the scale sensor. The scale then measures the weight of the medication and senses whether the patient is taking his/her medication accordingly. It measures the weight difference before and after the pills are taken. Both values are stored in a database.
- ENV: The environment sensor measures the temperature and humidity of the environment. It measures these values, at the time of activation and, once set active, every hour, and saves them in the database.
- HR: The heart rate sensor measures the heart rate of the patient when he/she places a finger on the sensor, and saves the values in the database.
- Motion: The motion sensor can recognize whether a person is located in a room and moving around. If this sensor is active and the light reminder for medication intake starts, the buzzer will also start, even though it was not activated manually by the user. However, if the patient is not in the room and not next to the system, he/she will not recognize the reminder. Therefore, if the patient is in another room and the motion sensor realizes that, it will activate the buzzer as a reminder.
- Reminder off: When a reminder is active, it can be turned off by pushing the “reminder off” button.
- Combine: The “combine” button is used to change the medication time or kind of reminder. Once the time is selected, the kind of reminder can be set by pushing the buttons for the buzzer, screen, or light. It is possible to select one, two, or all three options. Additionally, it is possible to select one of the arrows on the TUI to change the time.
- OK: The “OK” button (as mentioned above) is pressed after setting the time or changing the kind of reminder. Once the “OK” button is pressed, the new settings are saved in the database.
- Reset: If it is required to return the settings for a medication reminder to the default settings, the “reset” button needs to be pressed.
3.2. Field Study
3.2.1. Pre-Test
- Medication: Antiepileptics twice a day (08:00 and 20:00 h).
- Vital parameter: Monitoring device with Sao2 and pulse. During a seizure, a drop-in saturation can be detected and O2 can be administered if necessary.
- Methods/tools: Mobile phone app on which the time can be quickly stopped with one click during a cramp event and in which a history is then created. Furthermore, the strength and various cramp symptoms can also be entered. A pulse oximeter provides an alert in the case of a drop-in saturation.
3.2.2. User Tests
- Medication: take medication (depot neuroleptics) at both 08:00 and 19:00 h every 2 to 4 weeks.
- Vital parameter: measure body temperature.
- Methods/tools: Reminder for the medication intake, reminder for the appointment with the doctor regarding depot syringe.
- Medication: Antiepileptics to be taken twice a day (08:00 and 20:00 h).
- Vital parameter: Monitoring device with Sao2 and pulse. During a seizure, a drop-in saturation can be detected and O2 can be administered if necessary.
- Methods/tools: Mobile phone app on which the time can be quickly stopped with one click during a cramp event and in which a history is then created. Furthermore, the strength and various cramp symptoms can also be entered. A pulse oximeter provides an alert in the case of a drop-in saturation.
- Medication: take medication (depot neuroleptics) at both 08:00 and 19:00 h, every 2 to 4 weeks.
- Vital parameter: measure body temperature.
- Methods/tools: Reminder for the medication intake, reminder for the appointment with the doctor regarding depot syringe.
3.2.3. Test Results
3.3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Terms of the Literature Search
Appendix B. Questionnaire for Scenario Identification
- Which field(s) did you study for your current job in the health sector?
- What is your current job title?
- In which area are you currently working? Name the ward where you work or important characteristics of your field of activity.
- How long have you been working in this profession? It is sufficient to state the period of employment in half-year increments, e.g., 1.5 years.
- Have you had other professional experience in the health sector before? In the case of multiple work experiences, please answer the following questions about your work experience and clearly mark which profession is meant by your answers. If yes, please answer the following questions. If not, you can continue with the details on the use cases.
- In which area(s) did you work?
- How long were you employed in the activity or activities mentioned? It is sufficient to state the activity in half-year increments, e.g., 1.5 years.
- What was/were your exact job title/s?
- Do you have previous experience with adaptivity or IoT elements (e.g., Raspberry Pi)?
Details for Your Use Cases
Appendix C. PSSUQ
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | n/a | Comments | |
| Overall, I am satisfied with how easy it is to use this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| It was simple to use this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| I could effectively complete the tasks and scenarios using this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| I was able to complete the tasks and scenarios quickly using this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| I was able to efficiently complete the tasks and scenarios using this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| I felt comfortable using this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| It was easy to learn to use this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| I believe I could become productive quickly using this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| The system gave error messages that clearly told me how to fix problems. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| Whenever I made a mistake using the system, I could recover easily and quickly. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| The information (such as on-screen messages and other documentation) provided with this system was clear. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| It was easy to find the information I needed. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| The information provided for the system was easy to understand. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| The information was effective in helping me complete the tasks and scenarios. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| The organization of information on the system screens was clear. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| The interface of this system was pleasant. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| I liked using the interface of this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| This system has all the functions and capabilities I expect it to have. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| Overall, I am satisfied with this system. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
References
- Banafa, A. Secure and Smart Internet of Things (IoT); River Publishers: Delft, The Netherlands, 2018; ISBN 9788770220309. [Google Scholar]
- Borelli, E.; Paolini, G.; Antoniazzi, F.; Barbiroli, M.; Benassi, F.; Chesani, F.; Chiari, L.; Fantini, M.; Fuschini, F.; Galassi, A.; et al. HABITAT: An IoT solution for independent elderly. Sensors 2019, 19, 1258. [Google Scholar] [CrossRef]
- Fattah, S.; Sung, N.-M.; Ahn, I.-Y.; Ryu, M.; Yun, J. Building IoT services for aging in place using standard-based IoT platforms and heterogeneous IoT products. Sensors 2017, 17, 2311. [Google Scholar] [CrossRef]
- Akhtar, N.; Rahman, S.; Sadia, H.; Perwej, Y. A holistic analysis of Medical Internet of Things (MIoT). J. Inf. Comput. Sci. 2021, 11, 209–222. [Google Scholar] [CrossRef]
- Ugon, A.; Séroussi, B.; Lovis, C. (Eds.) Transforming Healthcare with the Internet of Things. In Proceedings of the EFMI Special Topic Conference 2016, Paris, France, 17–19 April 2016; IOS Press: Amsterdam, The Netherlands, 2016; Volume 221. ISSN 0926-9630. [Google Scholar]
- Yang, L.; Ge, Y.; Li, W.; Rao, W.; Shen, W. A home mobile healthcare system for wheelchair users. In Proceedings of the 2014 IEEE 18th International Conference on Computer Supported Cooperative Work in Design (CSCWD), Hsinchu, Taiwan, 21–23 May 2014; pp. 609–614. [Google Scholar] [CrossRef]
- Bong, W.K.; Chen, W.; Bergland, A. Tangible user interface for social interactions for the elderly: A Review of literature. Adv. Hum. Comput. Interact. 2018, 2018, 7249378. [Google Scholar] [CrossRef]
- Adil, M.; Alshahrani, H.; Rajab, A.; Shaikh, A.; Song, H.; Farouk, A. QoS review: Smart sensing in wake of COVID-19, current trends and specifications with future research directions. IEEE Sens. J. 2022, 23, 865–876. [Google Scholar] [CrossRef] [PubMed]
- Ajagbe, S.A.; Awotunde, J.B.; Adesina, A.O.; Achimugu, P.; Kumar, T.A. Internet of medical things (IoMT): Applications, challenges, and prospects in a data-driven technology. Intell. Healthc. Infrastruct. Algorithms Manag. 2022, 299–319. [Google Scholar] [CrossRef]
- Cherifi, A.; Khanouche, M.E.; Amirat, Y.; Farah, Z. A parallel approach for user-centered QoS-aware services composition in the Internet of Things. Eng. Appl. Artif. Intell. 2023, 123, 106277. [Google Scholar] [CrossRef]
- Shneiderman, B. Human-centered artificial intelligence: Three fresh ideas. AIS Trans. Hum. Comput. Interact. 2020, 12, 109–124. [Google Scholar] [CrossRef]
- Yarosh, S.; Zave, P. Locked or not? Mental models of IoT feature interaction. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; pp. 2993–2997. [Google Scholar] [CrossRef]
- Pape-Haugaard, L.B.; Lovis, C.; Cort Madsen, I.; Weber, P.; Hostrup Nielsen, P.; Scott, P. Digital Personalized Health and Medicine. In Proceedings of the MIE 2020, Geneva, Switzerland, 28 April–1 May 2020; IOS Press: Amsterdam, The Netherlands, 2020; Volume 270, ISBN 978-1-64368-083-5. [Google Scholar]
- Kabir, K.S.; Kenfield, S.A.; Van Blarigan, E.L.; Chan, J.M.; Wiese, J. Ask the Users: A Case Study of Leveraging User-Centered Design for Designing Just-in-Time Adaptive Interventions (JITAIs). Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2022, 6, 1–21. [Google Scholar] [CrossRef]
- Beaudry, A.; Pinsonneault, A. Understanding user responses to information technology: A coping model of user adaptation. MIS Quarterly 2005, 29, 493. [Google Scholar] [CrossRef]
- Orlikowski, W.J. Improvising organizational transformation over time: A situated change perspective. Inf. Syst. Res. 1996, 7, 63–92. [Google Scholar] [CrossRef]
- Chatterjee, A.; Prinz, A.; Gerdes, M.; Martinez, S.; Pahari, N.; Meena, Y.K. ProHealth eCoach: User-centered design and development of an eCoach app to promote healthy lifestyle with personalized activity recommendations. BMC Health Serv. Res. 2022, 22, 1120. [Google Scholar] [CrossRef]
- Jordan, P.W. Designing Pleasurable Products: An Introduction to the New Human Factors; CRC Press: Boca Raton, FL, USA, 2002. [Google Scholar] [CrossRef]
- Silverstone, R.; Haddon, L. Design the domestication of information communication technologies: Technical change everyday life. In Communication by Design: The Politics of Information and Communication Technologies; Mansell, R., Silverstone, R., Eds.; Oxford University: Oxford, UK, 1996; pp. 44–74. ISBN 9780198289418. [Google Scholar]
- Spreicer, W. Tangible interfaces as a chance for higher technology acceptance by the elderly. In Proceedings of the 12th International Conference on Computer Systems and Technologies—CompSysTech ’11, Vienna, Austria, 16–17 June 2011; pp. 311–316. [Google Scholar] [CrossRef]
- Qi, J.; Yang, P.; Min, G.; Amft, O.; Dong, F.; Xu, L. Advanced internet of things for personalised healthcare systems: A survey. Pervasive Mob. Comput. 2017, 41, 132–149. [Google Scholar] [CrossRef]
- Christensen, D.J.; Fogh, R.; Lund, H.H. Playte, a tangible interface for engaging human-robot interaction. In Proceedings of the The 23rd IEEE International Symposium on Robot and Human Interactive Communication, Edinburgh, UK, 25–29 August 2014. [Google Scholar] [CrossRef]
- Lewis, J.R. IBM computer usability satisfaction questionnaires: Psychometric evaluation and instructions for use. Int. J. Hum. Comput. Interact. 1995, 7, 57–78. [Google Scholar] [CrossRef]
- Haghi, M.; Neubert, S.; Geissler, A.; Fleischer, H.; Stoll, N.; Stoll, R.; Thurow, K. A Flexible and pervasive IoT-based healthcare platform for physiological and environmental parameters monitoring. IEEE Internet Things J. 2020, 7, 5628–5647. [Google Scholar] [CrossRef]
- Yang, G.; Xie, L.; Mantysalo, M.; Zhou, X.; Pang, Z.; Xu, L.D.; Kao-Walter, S.; Chen, Q.; Zheng, L.-R. A health-IoT platform based on the integration of intelligent packaging, unobtrusive bio-sensor, and intelligent medicine box. IEEE Trans. Ind. Inform. 2014, 10, 2180–2191. [Google Scholar] [CrossRef]
- Moustafa, H.; Schooler, E.M.; Shen, G.; Kamath, S. Remote monitoring and medical devices control in eHealth. In Proceedings of the 2016 IEEE 12th International Conference on Wireless and Mobile Computing, Networking and Communications (WiMob), New York, NY, USA, 17–19 October 2016; pp. 1–8. [Google Scholar] [CrossRef]
- Kao, H.-Y.; Wei, C.-W.; Yu, M.-C.; Liang, T.-Y.; Wu, W.-H.; Wu, Y.J. Integrating a mobile health applications for self-management to enhance Telecare system. Telemat. Inform. 2018, 35, 815–825. [Google Scholar] [CrossRef]
- Rozsa, V.; Denisczwicz, M.; Dutra, M.L.; Ghodous, P.; Ferreira da Silva, C.F.; Moayeri, N.; Biennier Figay, N. An Application Domain-Based Taxonomy for IoT Sensors. In Proceedings of the 23rd ISPE International Conference on Transdisciplinary Engineering: Crossing Boundaries, Curitiba, Brazil, 3–7 October 2016; pp. 249–258. [Google Scholar] [CrossRef]
- Rayes, A.; Salam, S. (Eds.) The Things in IoT: Sensors Actuators. In Internet of Things from Hype to Reality; Springer International Publishing: Berlin/Heidelberg, Germany, 2017; pp. 57–77. [Google Scholar] [CrossRef]
- De Raffaele, C.; Buhagiar, G.; Smith, S.; Gemikonakli, O. Designing a table-top tangible user interface system for higher education. In Proceedings of the 2017 International Conference on Smart Systems and Technologies (SST), Osijek, Croatia, 18–20 October 2017; pp. 285–291. [Google Scholar] [CrossRef]
- Nathoo, A.; Bekaroo, G.; Gangabissoon, T.; Santokhee, A. Using tangible user interfaces for teaching concepts of internet of things: Usability and learning effectiveness. Interact. Technol. Smart Educ. 2020, 17, 133–158. [Google Scholar] [CrossRef]
- Verhaegh, J.; Fontijn, W.; Jacobs, A. On the Benefits of Tangible Interfaces for Educational Games. In Proceedings of the 2008 Second IEEE International Conference on Digital Game and Intelligent Toy Enhanced Learning, Banff, AL, Canada, 17–19 November 2008; pp. 141–145. [Google Scholar] [CrossRef]
- Schneider, B.; Jermann, P.; Zufferey, G.; Dillenbourg, P. Benefits of a Tangible Interface for Collaborative Learning and Interaction. IEEE Trans. Learn. Technol. 2011, 4, 222–232. [Google Scholar] [CrossRef]
- Zuckerman, O.; Gal-Oz, A. To TUI or not to TUI: Evaluating performance and preference in tangible vs. graphical user interfaces. Int. J. Hum. Comput. Stud. 2013, 71, 803–820. [Google Scholar] [CrossRef]
- Krestanova, A.; Cerny, M.; Augustynek, M. Development and technical design of tangible user interfaces in wide-field areas of application. Sensors 2021, 21, 4258. [Google Scholar] [CrossRef]
- Santos, J.; Vairinhos, M.; Rodriguez, J.; Jesus, L.M. Home-Based Activities for Children with Speech Sound Disorders: Requirements for a Tangible User Interface for Internet of Things Artefacts. Appl. Sci. 2022, 12, 8971. [Google Scholar] [CrossRef]
- Wolf, J.A.; Niederhauser, V.; Marshburn, D.; LaVela, S.L. Reexamining “Defining Patient Experience”: The human experience in healthcare. Patient Exp. J. 2021, 8, 16–29. [Google Scholar] [CrossRef]
- Chang, D.; Gu, Z.; Li, F.; Jiang, R. A user-centric smart product-service system development approach: A case study on medication management for the elderly. Adv. Eng. Inform. 2019, 42, 100979. [Google Scholar] [CrossRef]
- Sadoughi, F.; Behmanesh, A.; Sayfouri, N. Internet of things in medicine: A systematic mapping study. J. Biomed. Inform. 2020, 103, 103383. [Google Scholar] [CrossRef] [PubMed]
- Bhuiyan, M.N.; Rahman, M.M.; Billah, M.M.; Saha, D. Internet of things (IoT): A review of its enabling technologies in healthcare applications, standards protocols, security, and market opportunities. IEEE Internet Things J. 2021, 8, 10474–10498. [Google Scholar] [CrossRef]
- Stary, C. The Internet-of-Behavior as Organizational Transformation Space with Choreographic Intelligence. In Proceedings of the S-BPM-One 2020, Bremen, Germany, 2–3 December 2020; Freitag, M., Kinra, A., Kotzab, H., Kreowski, H.-J., Thoben, K.-D., Eds.; Springer: Cham, Switzerland, 2020; Volume 1278, pp. 113–132. [Google Scholar] [CrossRef]
- Stary, C.; Kaar, C.; Jahn, M. Featuring dual learning experiences in tangible CPS education: A synchronized internet-of-things–digital-twin system. In Proceedings of the SIGCHI Symposium on Engineering Interactive Computing Systems, Eindhoven, The Netherlands, 8–11 June 2021; pp. 56–62. [Google Scholar] [CrossRef]
- Stary, C.; Elstermann, M.; Fleischmann, A.; Schmidt, W. Behavior-centered digital-twin design for dynamic cyber-physical system development. Complex Syst. Inform. Model. Q. CSIMQ 2022, 30, 31–52. [Google Scholar] [CrossRef]
- Lee, C.W. Application of metaverse service to healthcare industry: A strategic perspective. Int. J. Environ. Res. Public Health 2022, 19, 13038. [Google Scholar] [CrossRef]
- Stary, C. Can a ‘Metaverse by Design’ benefit from Digital Process Twins? In Proceedings of the S-BPM-One 2023, Rostock, Germany, 31 May–1 June; Elstermann, M., Dittmar, A., Lederer, M., Eds.; Springer: Cham, Switzerland; Volume 1867, pp. 1–20. [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Requirements | Design Process | Runtime Characteristics | |
|---|---|---|---|
| Base Technologies | Which development board is used to connect the sensors (e.g., Raspberry Pi)? Which sensors/IoT devices are used for operations? Are further technical components required for operation? Which software is required (e.g., digital twin)? | Which architecture is used? How is it ensured from a technology perspective that (non-IT affine) individuals are able to use/adapt the system? How does the user obtain information from the system? How can the user control the system? Which design aids are used? | Does the system configure itself automatically or is support required? When will someone be notified of a person’s health problems? Who is notified about the medical problems of the patient (medical staff, relatives, patients themselves)? |
| User Needs | Which health conditions are addressed? What previous IT knowledge is required for the use/adaptation/first installation of the system? Does a technical specialist have to install the system or can patients install the system themselves? | How can the user adapt the system? How does the system communicate with the user? | How much support from other people (e.g., medical staff, relatives, friends) is necessary to run the system and implement the design? Which implementation tools are required (e.g., prototyping tool)? Which design adjustments can be implemented, supported by automation? |
| Use Cases | What domain is the target of the system used (home healthcare or something else)? Are non-technical components required to run the system (e.g., drug can)? | How is the patient’s home environment structured to use the system for the concerned use scenario? How must the sensors be set up in the patient’s private areas? | Which scenario is addressed by the system? |
| (Haghi et al., 2020) [24] | (G. Yang et al., 2014) [25] | (Borelli et al., 2019) [2] | (Fattah et al., 2017) [3] | (L. Yang et al., 2014) [6] | (Moustafa et al., 2016) [26] | (Kao et al., 2018) [27] | |||
|---|---|---|---|---|---|---|---|---|---|
| Sensors | Physiological sensors | Heart rate | X | X | |||||
| ECG | X | X | X | ||||||
| EEG | X | ||||||||
| Skin temperature | X | X | |||||||
| Respiration rate | X | ||||||||
| Respiration rate interval | X | ||||||||
| Blood pressure gauge | X | ||||||||
| Environmental sensors | Air Temperature | X | X | ||||||
| Smoke sensor | X | ||||||||
| Gas sensor | X | ||||||||
| Air humidity | X | X | |||||||
| Air pressure | X | ||||||||
| UV | X | ||||||||
| NO2 | X | ||||||||
| Noise sensor | X | ||||||||
| Data exch. | RFID | X | X | ||||||
| NFC | X | ||||||||
| Force transd. | Weight sensor | X | |||||||
| Load cells | X | ||||||||
| Pressure cushion | X | ||||||||
| Movement | Ultrasonic sensor | X | |||||||
| Proximity sensor | X | ||||||||
| IR sensor | X | ||||||||
| Accelerator | X | X | |||||||
| Inertial sensor | X | ||||||||
| Image | Camera | X | X | ||||||
| Actuators | Close distance | Vibrating motor | X | X | |||||
| Display | X | ||||||||
| Wide distance | Light | X | X | ||||||
| Beeper | X | ||||||||
| Speaker | X |
| Adaptation System Label/Denotation | (Haghi et al., 2020) [24] | (G. Yang et al., 2014) [25] | (L. Yang et al., 2014) [6] | (Moustafa et al., 2016) [26] | (Fattah et al., 2017) [3] | (Borelli et al., 2019) [2] | (Kao et al., 2018) [27] |
|---|---|---|---|---|---|---|---|
| Adaptable/flexible | X | X | X | X | X | ||
| People-centric | X | ||||||
| Individualized | X | X | X | X | X | X | |
| Expandable | X | X | X | X | X | X |
| First Test Case | Second Test Case | Third Test Case | |
|---|---|---|---|
| Overall Satisfaction Score | 1.94 | 1.53 | 1.38 |
| System Usefulness | 2.13 | 1.75 | 1.5 |
| Information Quality | 1.5 | 1 | 1 |
| Interface Quality | 2.33 | 2 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fehringer, H.; Stary, C. User-Informed Adaptation in IoT Home Healthcare: Grounding Development in Empirical Evidence. J. Theor. Appl. Electron. Commer. Res. 2023, 18, 1901-1925. https://doi.org/10.3390/jtaer18040096
Fehringer H, Stary C. User-Informed Adaptation in IoT Home Healthcare: Grounding Development in Empirical Evidence. Journal of Theoretical and Applied Electronic Commerce Research. 2023; 18(4):1901-1925. https://doi.org/10.3390/jtaer18040096
Chicago/Turabian StyleFehringer, Hannah, and Christian Stary. 2023. "User-Informed Adaptation in IoT Home Healthcare: Grounding Development in Empirical Evidence" Journal of Theoretical and Applied Electronic Commerce Research 18, no. 4: 1901-1925. https://doi.org/10.3390/jtaer18040096
APA StyleFehringer, H., & Stary, C. (2023). User-Informed Adaptation in IoT Home Healthcare: Grounding Development in Empirical Evidence. Journal of Theoretical and Applied Electronic Commerce Research, 18(4), 1901-1925. https://doi.org/10.3390/jtaer18040096