
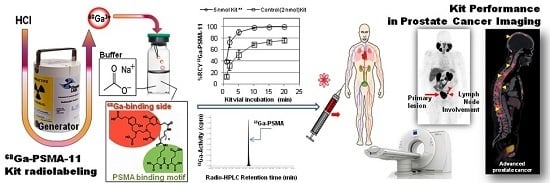
Development of a Single Vial Kit Solution for Radiolabeling of 68Ga-DKFZ-PSMA-11 and Its Performance in Prostate Cancer Patients

 ,
, 
Abstract
:
1. Introduction
2. Results and Discussion
2.1. 68Ge/68Ga Generator
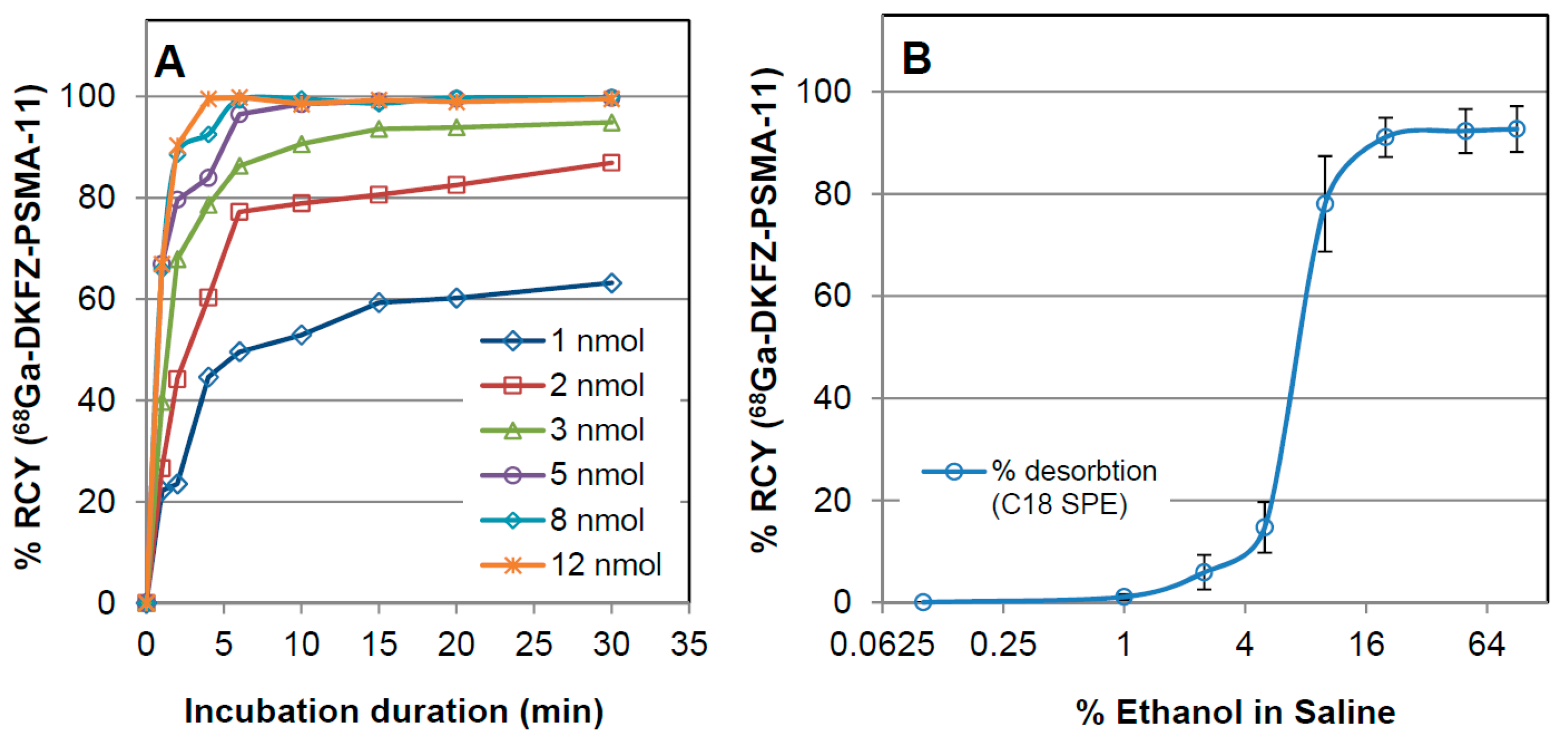
2.2. Preliminary Assessment of the Radiolabeling Parameters

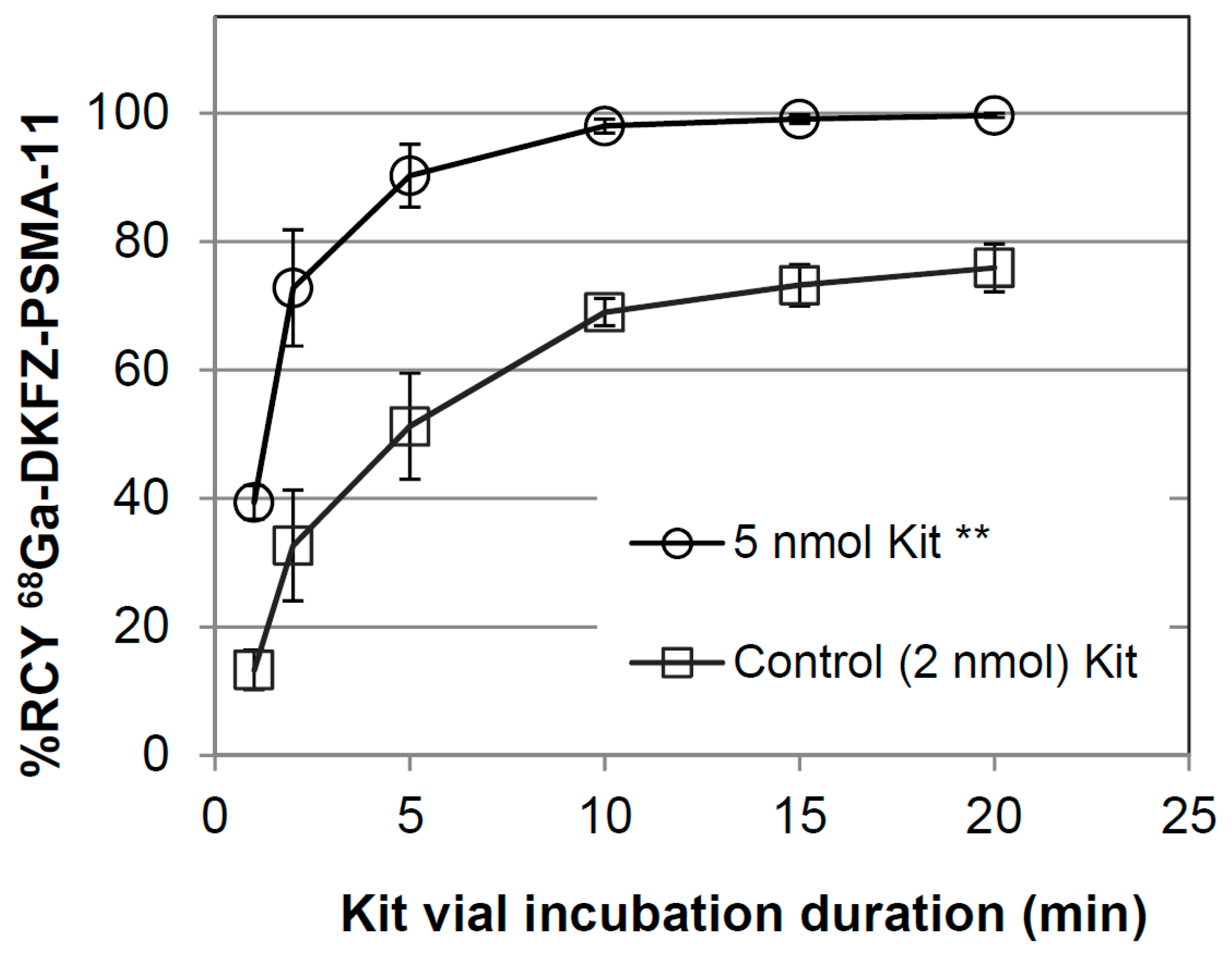
2.3. In-House Kit Vial Formulation of DKFZ-PSMA-11

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Quality Control Test | Specification | Test Results |
|---|---|---|
| Eluate fraction yield (MBq) | ≥300 MBq/1 mL | 332–1039 |
| 68Ge breakthrough (total eluate batch 10 mL) | ≤0.001% over 9 months | max: 0.00074% mean: 0.0003% ± 0.0001% |
| Cationic impurities (Zn, Fe, Cu, Sn, Al) | ≤50 ppm/1 mL | pass |
| Product yield (MBq) | ≥200 MBq/1 mL | 310 ± 52 |
| Visual inspection | Clear colourless, particle-free | pass |
| Radiochemical identity ITLC | Rf 68Ga-DKFZ-PSMA-11 = 0.75 ± 0.2 | 0.73–0.77 |
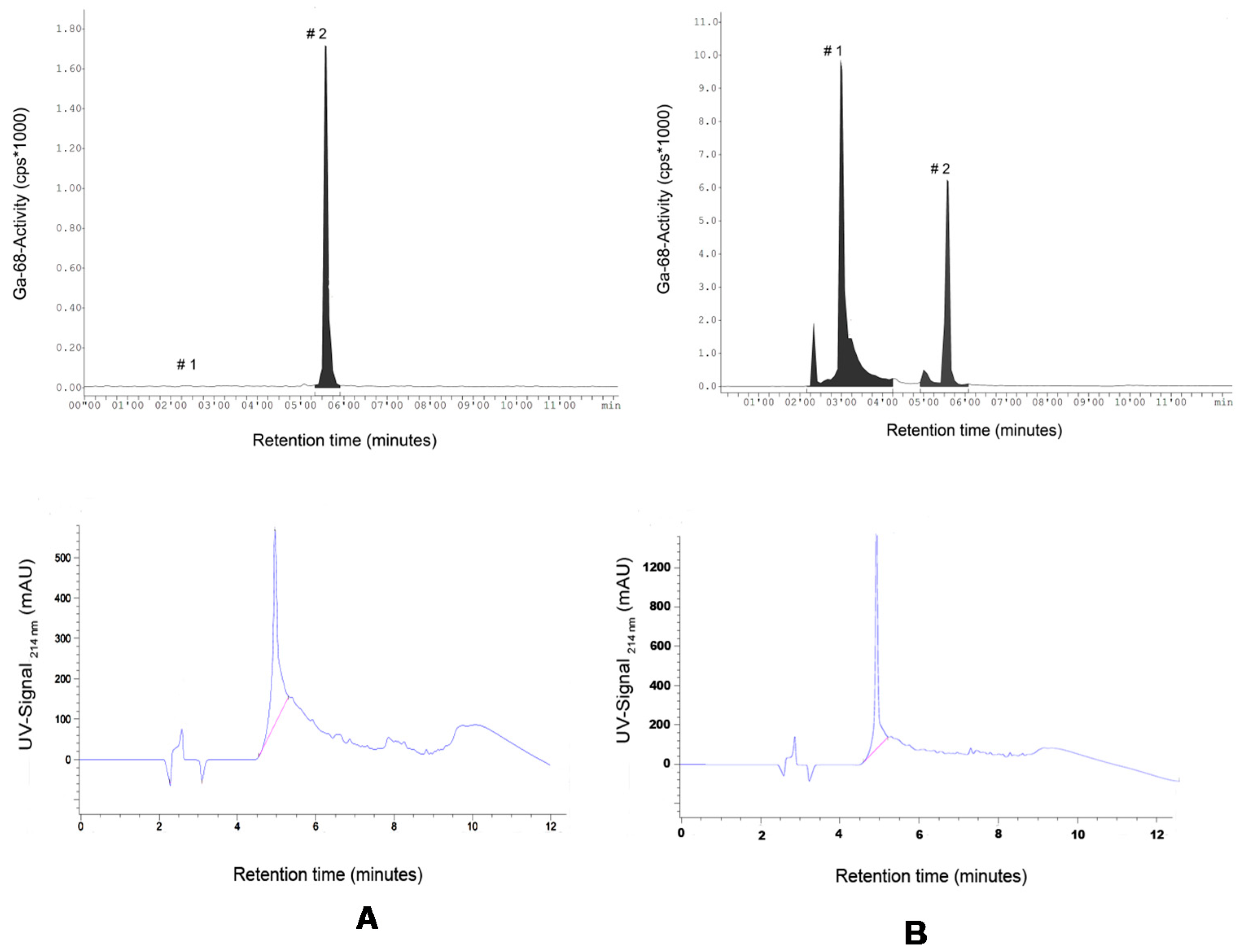
| Radiochemical identity HPLC | Retention time = 5.3 ± 0.5 min | 5.18–5.58 |
| Chemical identity HPLC(UV214nm) | Retention time = 4.9 ± 0.5 min | 4.83–5.08 |
| Radiochemical purity | ≥95% | 99.6 |
| pH for injection | physiological (6.0–7.6) | 6.5–7.0 |
| Sterile filter integrity | ≥3.5 bar | 5.9 ± 0.9 (n = 7) |
| Radionuclide identity | 67.7 ± 5 min | 65.1–69.8 (n = 6) |
| Residual 68Germanium (2–5 mL) | ≤0.001% | 0.000057 ± 0.000015 |
| Sterility | Sterile (fungal/anaerobe/aerobe) | pass |
| Total product endotoxins | max: 20 EU | pass |

2.4. Quality Assessment of the 68Ga-DKFZ-PSMA-11 Kit
2.4.1. Appearance and Sterility

2.4.2. Radionuclidic Identity and pH Value
2.4.3. Radiochemical Stability
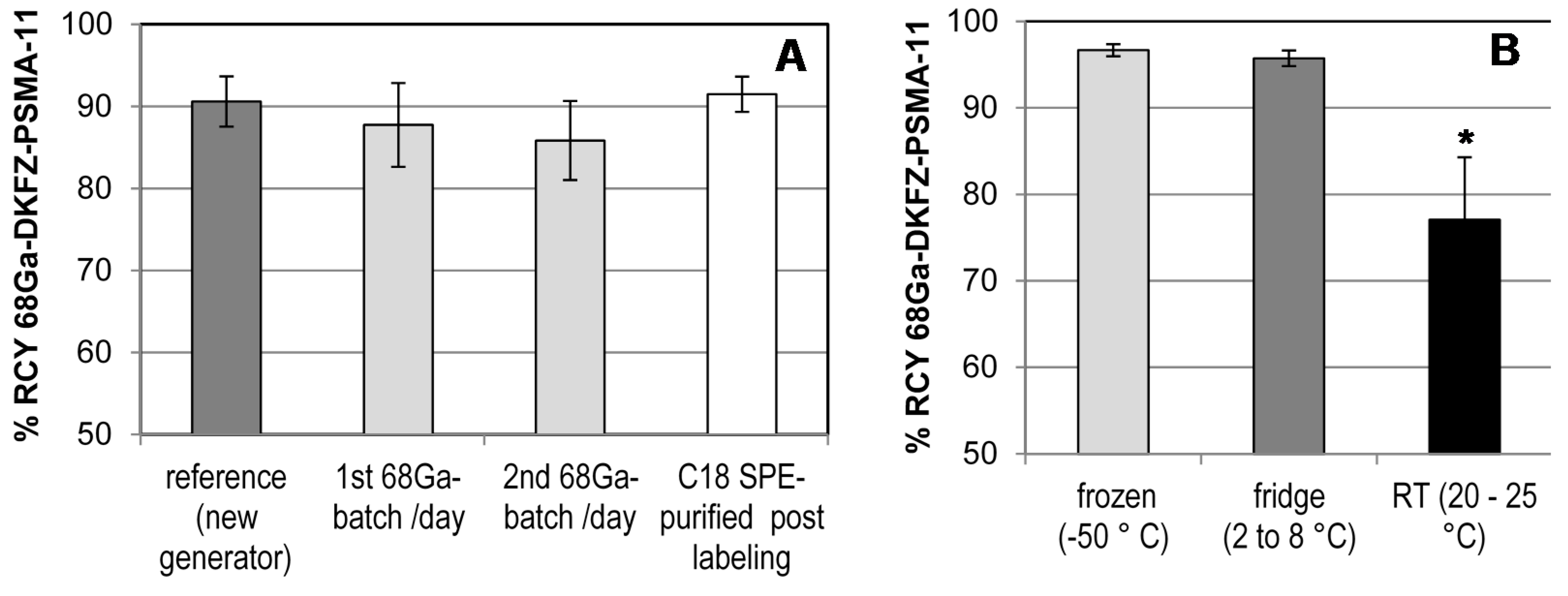
2.4.4. Long-Term Storage and Radiolabeling Reproducibility

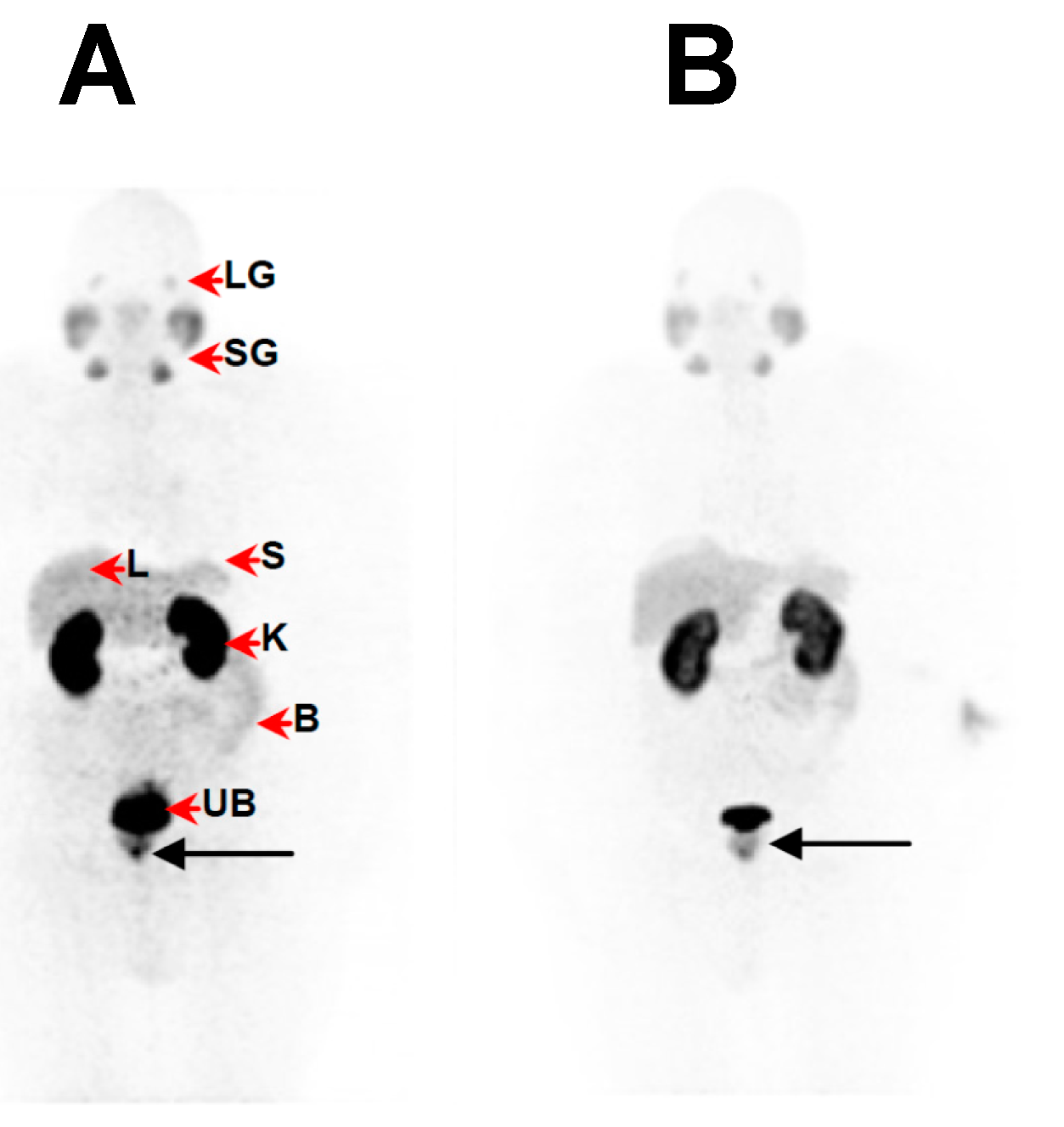
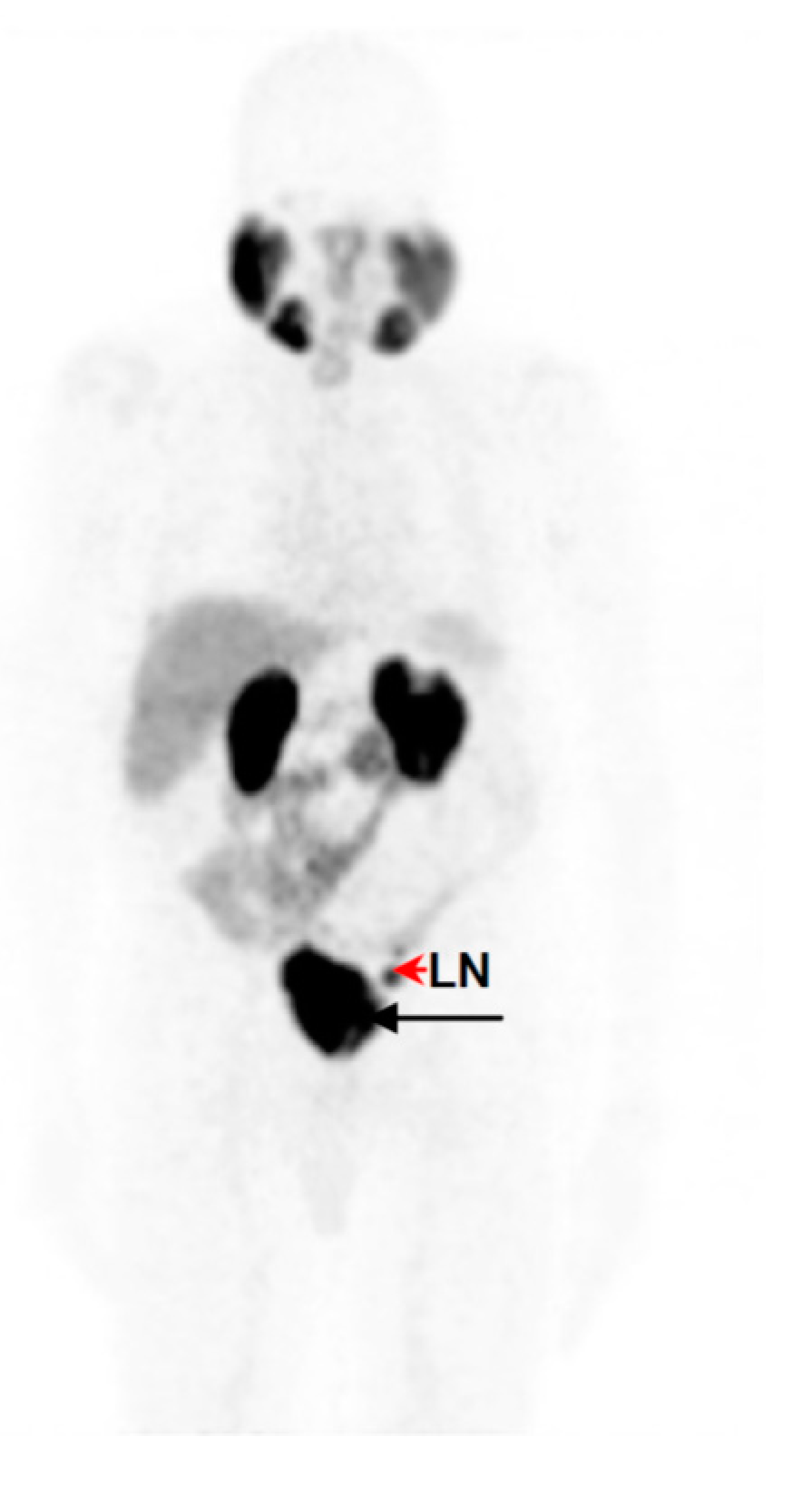
2.5. Clinical PET/CT—68Ga-DKFZ-PSMA-11 Kit Performance in Prostate Cancer Patients



2.6. Discussion
3. Material and Methods
3.1. Chemicals and Materials
3.2. 68Ge/68Ga Generator
3.3. Preliminary Assessment of Radiolabeling Parameters
3.4. In-House Kit Vial Formulation of DKFZ-PSMA-11
3.5. 68Ga Radiolabeling of DKFZ-PSMA-11 Kits
3.6. Quality Assessment of the 68Ga-DKFZ-PSMA-11 Kit
3.6.1. Appearance and Sterility
3.6.2. Radionuclidic Identity and pH Value
3.6.3. Radiochemical Stability
3.6.4. Long-Term Storage and Radiolabeling Reproducibility
3.7. Clinical PET/CT—68Ga-DKFZ-PSMA-11 Kit Performance in Prostate Cancer Patients
Image Acquisition, Reconstruction and Analysis
3.8. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Center, M.M.; Jemal, A.; Lortet-Tieulent, J.; Ward, E.; Ferlay, J.; Brawley, O.; Bray, F. International variation in prostate cancer incidence and mortality rates. Eur. Urol. 2012, 61, 1079–1092. [Google Scholar] [CrossRef] [PubMed]
- Kravchick, S.; Cytron, S.; Peled, R.; Altshuler, A.; Ben-Dor, D. Using gray-scale and two different techniques of color Doppler sonography to detect prostate cancer. Urology 2003, 61, 977–981. [Google Scholar] [CrossRef]
- Hricak, H.; Dooms, G.C.; Jeffrey, R.B.; Avallone, A.; Jacobs, D.; Benton, W.K.; Narayan, P.; Tanagho, E.A. Prostatic carcinoma: Staging by clinical assessment, CT, and MR imaging. Radiology 1987, 162, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Gronberg, H. Prostate cancer epidemiology. Lancet 2003, 361, 859–864. [Google Scholar] [CrossRef]
- Jadvar, H. Imaging evaluation of prostate cancer with 18F-fluorodeoxyglucose PET/CT: Utility and limitations. Eur. J. Nucl. Med. Mol. Imaging 2013, 40 (Suppl. 1), 5–10. [Google Scholar] [CrossRef] [PubMed]
- Apolo, A.B.; Pandit-Taskar, N.; Morris, M.J. Novel tracers and their development for the imaging of metastatic prostate cancer. J. Nucl. Med. 2008, 49, 2031–2041. [Google Scholar] [CrossRef] [PubMed]
- Jadvar, H. Molecular imaging of prostate cancer: PET radiotracers. Am. J. Roentgenol. 2012, 199, 278–291. [Google Scholar] [CrossRef] [PubMed]
- Castellucci, P.; Jadvar, H. PET/CT in prostate cancer: Non-choline radiopharmaceuticals. Q. J. Nucl. Med. Mol. Imaging 2012, 56, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Jadvar, H. Can choline PET tackle the challenge of imaging prostate cancer? Theranostics 2012, 2, 331–332. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Zechmann, C.M.; Malcher, A.; Eder, M.; Eisenhut, M.; Linhart, H.G.; Holland-Letz, T.; Hadaschik, B.A.; Giesel, F.L.; Debus, J.; et al. Comparison of PET imaging with a 68Ga-labeled PSMA ligand and 18F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Vorster, M.; Modiselle, M.; Ebenhan, T.; Wagener, C.; Sello, T.; Zeevaart, J.R.; Moshokwa, E.; Sathekge, M.M. Fluorine-18-fluoroethylcholine PET/CT in the detection of prostate cancer: A South African experience. Hell. J. Nucl. Med. 2015, 18, 53–59. [Google Scholar] [PubMed]
- Demirkol, M.O.; Acar, O.; Ucar, B.; Ramazanoglu, S.R.; Saglican, Y.; Esen, T. Prostate-specific membrane antigen-based imaging in prostate cancer: Impact on clinical decision making process. Prostate 2015, 75, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Osborne, J.R.; Akhtar, N.H.; Vallabhajosula, S.; Anand, A.; Deh, K.; Tagawa, S.T. Prostate-specific membrane antigen-based imaging. Urol. Oncol. 2013, 31, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Malcher, A.; Eder, M.; Eisenhut, M.; Linhart, H.G.; Hadaschik, B.A.; Holland-Letz, T.; Giesel, F.L.; Kratochwil, C.; Haufe, S.; et al. PET imaging with a [68Ga]gallium-labeled PSMA ligand for the diagnosis of prostate cancer: Biodistribution in humans and first evaluation of tumour lesions. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Buhler, P.; Wolf, P.; Elsasser-Beile, U. Targeting the prostate-specific membrane antigen for prostate cancer therapy. Immunotherapy 2009, 1, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Foss, C.A.; Byun, Y.; Nimmagadda, S.; Pullambhatla, M.; Fox, J.J.; Castanares, M.; Lupold, S.E.; Babich, J.W.; Mease, R.C.; et al. Radiohalogenated prostate-specific membrane antigen (PSMA)-based ureas as imaging agents for prostate cancer. J. Med. Chem. 2008, 51, 7933–7943. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.R.; Foss, C.A.; Castanares, M.; Mease, R.C.; Byun, Y.; Fox, J.J.; Hilton, J.; Lupold, S.E.; Kozikowski, A.P.; Pomper, M.G. Synthesis and evaluation of technetium-99m- and rhenium-labeled inhibitors of the prostate-specific membrane antigen (PSMA). J. Med. Chem. 2008, 51, 4504–4517. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.R.; Pullambhatla, M.; Byun, Y.; Nimmagadda, S.; Green, G.; Fox, J.J.; Horti, A.; Mease, R.C.; Pomper, M.G. 68Ga-labeled inhibitors of prostate-specific membrane antigen (PSMA) for imaging prostate cancer. J. Med. Chem. 2010, 53, 5333–5341. [Google Scholar] [CrossRef] [PubMed]
- Eder, M.; Schafer, M.; Bauder-Wust, U.; Hull, W.E.; Wangler, C.; Mier, W.; Haberkorn, U.; Eisenhut, M. 68Ga-complex lipophilicity and the targeting property of a urea-based PSMA inhibitor for PET imaging. Bioconjugate Chem. 2012, 23, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Haberkorn, U.; Eder, M.; Eisenhut, M.; Zechmann, C.M. [68Ga]Gallium-labeled PSMA ligand as superior PET tracer for the diagnosis of prostate cancer: Comparison with 18F-FECH. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1085–1086. [Google Scholar] [CrossRef] [PubMed]
- Eder, M.; Neels, O.; Muller, M.; Bauder-Wust, U.; Remde, Y.; Schafer, M.; Hennrich, U.; Eisenhut, M.; Afshar-Oromieh, A.; Haberkorn, U.; et al. Novel preclinical and radiopharmaceutical aspects of [68Ga]Ga-PSMA-HBED-CC: A new PET tracer for imaging of prostate cancer. Pharmaceuticals (Basel) 2014, 7, 779–796. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Avtzi, E.; Giesel, F.L.; Holland-Letz, T.; Linhart, H.G.; Eder, M.; Eisenhut, M.; Boxler, S.; Hadaschik, B.A.; Kratochwil, C.; et al. The diagnostic value of PET/CT imaging with the 68Ga-labeled PSMA ligand HBED-CC in the diagnosis of recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Al-Nahhas, A.; Win, Z.; Szyszko, T.; Singh, A.; Khan, S.; Rubello, D. What can gallium-68 PET add to receptor and molecular imaging? Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 1897–1901. [Google Scholar] [CrossRef] [PubMed]
- Velikyan, I. Prospective of 68Ga-radiopharmaceutical development. Theranostics 2013, 4, 47–80. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.; Pandey, U.; Chakravarty, R.; Sarma, H.D.; Dash, A. Development of single vial kits for preparation of 68Ga-labeled peptides for PET imaging of neuroendocrine tumours. Mol. Imaging Biol. 2014, 16, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Wangler, C.; Wangler, B.; Lehner, S.; Elsner, A.; Todica, A.; Bartenstein, P.; Hacker, M.; Schirrmacher, R. A universally applicable 68Ga-labeling technique for proteins. J. Nucl. Med. 2011, 52, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Vorster, M.; Mokaleng, B.; Sathekge, M.M.; Ebenhan, T. A modified technique for efficient radiolabeling of 68Ga-citrate from a SnO2-based 68Ge/68Ga generator for better infection imaging. Hell. J. Nucl. Med. 2013, 16, 193–198. [Google Scholar] [PubMed]
- Hain, S.F.; Maisey, M.N. Positron emission tomography for urological tumours. BJU Int. 2003, 92, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Goodman, O.B., Jr.; Barwe, S.P.; Ritter, B.; McPherson, P.S.; Vasko, A.J.; Keen, J.H.; Nanus, D.M.; Bander, N.H.; Rajasekaran, A.K. Interaction of prostate specific membrane antigen with clathrin and the adaptor protein complex-2. Int. J. Oncol. 2007, 31, 1199–1203. [Google Scholar] [PubMed]
- Hillier, S.M.; Maresca, K.P.; Femia, F.J.; Marquis, J.C.; Foss, C.A.; Nguyen, N.; Zimmerman, C.N.; Barrett, J.A.; Eckelman, W.C.; Pomper, M.G.; et al. Preclinical evaluation of novel glutamate-urea-lysine analogues that target prostate-specific membrane antigen as molecular imaging pharmaceuticals for prostate cancer. Cancer Res. 2009, 69, 6932–6940. [Google Scholar] [CrossRef] [PubMed]
- Maresca, K.P.; Hillier, S.M.; Femia, F.J.; Keith, D.; Barone, C.; Joyal, J.L.; Zimmerman, C.N.; Kozikowski, A.P.; Barrett, J.A.; Eckelman, W.C.; et al. A series of halogenated heterodimeric inhibitors of prostate specific membrane antigen (PSMA) as radiolabeled probes for targeting prostate cancer. J. Med. Chem. 2009, 52, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Schafer, M.; Bauder-Wust, U.; Leotta, K.; Zoller, F.; Mier, W.; Haberkorn, U.; Eisenhut, M.; Eder, M. A dimerized urea-based inhibitor of the prostate-specific membrane antigen for 68Ga-PET imaging of prostate cancer. EJNMMI Res. 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, E. Clinical PET: Its time has come? J. Nucl. Med. 1993, 34, 1132–1133. [Google Scholar] [PubMed]
- Amor-Coarasa, A.; Milera, A.; Carvajal, D.; Gulec, S.; McGoron, A.J. Lyophilized kit for the preparation of the PET perfusion agent [68Ga]-MAA. Int. J. Mol. Imaging 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Vorster, M.; Maes, A.; van de Wiele, C.; Sathekge, M.M. 68Ga-citrate PET/CT in Tuberculosis: A pilot study. Q. J. Nucl. Med. Mol. Imaging 2014. [Google Scholar]
- Breeman, W.A.; de Blois, E.; Sze Chan, H.; Konijnenberg, M.; Kwekkeboom, D.J.; Krenning, E.P. 68Ga-labeled DOTA-peptides and 68Ga-labeled radiopharmaceuticals for positron emission tomography: Current status of research, clinical applications, and future perspectives. Semin. Nucl. Med. 2011, 41, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Kabasakal, L.; Demirci, E.; Ocak, M.; Akyel, R.; Nematyazar, J.; Aygun, A.; Halac, M.; Talat, Z.; Araman, A. Evaluation of PSMA PET/CT imaging using a 68Ga-HBED-CC ligand in patients with prostate cancer and the value of early pelvic imaging. Nucl. Med. Commun. 2015, 36, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, K.; Bluemel, C.; Weineisen, M.; Schottelius, M.; Wester, H.J.; Czernin, J.; Eberlein, U.; Beykan, S.; Lapa, C.; Riedmiller, H.; et al. Biodistribution and radiation dosimetry for a novel probe targeting prostate specific membrane antigen for imaging and therapy (68Ga-PSMA I & T). J. Nucl. Med. 2015, 56, 855–861. [Google Scholar] [PubMed]
- Sathekge, M.; Modiselle, M.; Vorster, M.; Mokgoro, N.; Nyakale, N.; Mokaleng, B.; Ebenhan, T. 68Ga-PSMA imaging of metastatic breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1482–1483. [Google Scholar] [CrossRef] [PubMed]
- Demirci, E.; Ocak, M.; Kabasakal, L.; Decristoforo, C.; Talat, Z.; Halac, M.; Kanmaz, B. 68Ga-PSMA PET/CT imaging of metastatic clear cell renal cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1461–1462. [Google Scholar] [CrossRef] [PubMed]
- Ebenhan, T.; Chadwick, N.; Sathekge, M.M.; Govender, P.; Govender, T.; Kruger, H.G.; Marjanovic-Painter, B.; Zeevaart, J.R. Peptide synthesis, characterization and 68Ga-radiolabeling of NOTA-conjugated ubiquicidin fragments for prospective infection imaging with PET/CT. Nucl. Med. Biol. 2014, 41, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, D.D.; Breeman, W.A. Scaled-up radiolabeling of DOTATATE with 68Ga eluted from a SnO2-based 68Ge/68Ga generator. Appl. Radiat. Isot. 2012, 70, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Baur, B.; Solbach, C.; Andreolli, E.; Winter, G.; Machulla, H.J.; Reske, S.N. Synthesis, radiolabeling and in vitro characterisation of the Gallium-68-, Yttrium-90- and Lutetium-177-labeled PSMA ligand, CHX-A′′-DTPA-DUPA-Pep. Pharmaceuticals (Basel) 2014, 7, 517–529. [Google Scholar] [CrossRef] [PubMed]
- Sample Availability: DKFZ-PSMA-11 kit vials are available from the authors.
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ebenhan, T.; Vorster, M.; Marjanovic-Painter, B.; Wagener, J.; Suthiram, J.; Modiselle, M.; Mokaleng, B.; Zeevaart, J.R.; Sathekge, M. Development of a Single Vial Kit Solution for Radiolabeling of 68Ga-DKFZ-PSMA-11 and Its Performance in Prostate Cancer Patients. Molecules 2015, 20, 14860-14878. https://doi.org/10.3390/molecules200814860
Ebenhan T, Vorster M, Marjanovic-Painter B, Wagener J, Suthiram J, Modiselle M, Mokaleng B, Zeevaart JR, Sathekge M. Development of a Single Vial Kit Solution for Radiolabeling of 68Ga-DKFZ-PSMA-11 and Its Performance in Prostate Cancer Patients. Molecules. 2015; 20(8):14860-14878. https://doi.org/10.3390/molecules200814860
Chicago/Turabian StyleEbenhan, Thomas, Mariza Vorster, Biljana Marjanovic-Painter, Judith Wagener, Janine Suthiram, Moshe Modiselle, Brenda Mokaleng, Jan Rijn Zeevaart, and Mike Sathekge. 2015. "Development of a Single Vial Kit Solution for Radiolabeling of 68Ga-DKFZ-PSMA-11 and Its Performance in Prostate Cancer Patients" Molecules 20, no. 8: 14860-14878. https://doi.org/10.3390/molecules200814860