1. Introduction
Ginkgolides (GG) are the major bioactive components found in the
Ginkgo biloba leaf (
G. biloba), mainly consisting of ginkgolide A (GA), ginkgolide B (GB), ginkgolide C (GC), etc. These compounds have been recognized as antagonists of platelet activating factor (PAF) receptor, and GB is considered to be the most powerful PAF antagonist among them [
1,
2,
3]. GG possesses many pharmacological activities, including improving cerebral circulation, expanding coronary vessels, cardioprotective, inhibiting platelet aggregation, reducing vascular permeability and preventing atherosclerosis, and thus has been widely used in the treatment of neurological and cardiovascular diseases [
4,
5].
Ginkgolides (C
20 compounds), belonging to the diterpene lactones, have a cage-like molecular structure (
Figure 1a) with three lactone rings and one spirononane ring [
1]. The structural differences between GA, GB and GC only depend on the number of hydroxy groups and their position. However, all of them share poor oral bioavailability related to their low solubility. After going through the systemic circulation, the lactone ring of ginkgolides is easily hydrolyzed, which remarkably reduces the bioavailability of ginkgolides. Because of their poor solubility and low bioavailability, the therapeutic effects of ginkgolides are greatly reduced [
6,
7]. During the last decades, pharmaceutical technologies such as microemulsions and solid dispersions have been tested and proved to improve the absorption of
G. biloba flavonoids in studies of the oral absorption mechanism, pharmacokinetics and pharmacodynamics of
G. biloba extract. However, few studies focusing on
G. biloba lactones were reported, and the existing pharmaceutical technologies could hardly solve the fundamental problems associated with the poor oral bioavailability of
G. biloba lactones. In recent years,
G. biloba lactone injection has been widely used clinically in China. However, as expected, the amount of ginkgolides in the brain tissue was only 0.02% of the dosage at 10 min after injection, accompanied by uneven distribution of the ginkgolides in the brain. Because of the easily hydrolyzed lactone ring and rapid distribution to the stomach, duodenum, liver and other parts, few ginkgolides can be detected 30 min after injection. Therefore, the concentration of ginkgolides transported into the brain is the limiting step of
G. biloba lactone against cerebral ischemia injury [
8].
The blood-brain barrier (BBB) is an anatomical defense barrier between the brain and blood. Because of its extensive tight junctions and energy-dependent efflux transporters, BBB controls substance transport from the blood to the barrier, and plays an important role in protecting the central nervous system from toxic substances and serving to maintain brain homeostasis. The BBB protects the brain from unwanted substances, while, at the same time, limits the transport of many drugs into the brain. To date, the curative effect of drugs for the central nervous system is still greatly hampered by the existence of the BBB [
9,
10]. Recent pharmacological studies have shown that aromatic refreshing traditional Chinese medicines (TCMs), such as borneol, musk, styrax, benzoinum and Tatarinow Sweetflag Rhizome, can induce resuscitation and modify the permeability of BBB, promoting the entry of other drugs into the brain with brain protective effects. As a representative, borneol (
Figure 1b) is a naturally occurring monoterpenoid compound in a class of ‘orifice-opening’ agents often used for resuscitative purposes in TCM. Borneol is divided into natural borneol (NB) and synthetic borneol (SB). SB consists of D-borneol and isoborneol, while NB contains only D-borneol [
11,
12,
13,
14,
15]. A growing body of evidence confirms that borneol is able to loosen intercellular tight junctions, and thus open the BBB and enhance the distribution of drugs in the brain [
16,
17,
18]. Therefore, borneol is believed to be an effective and promising adjuvant that can improve drug delivery to the brain.
Herein, we chose NB to modify
G. biloba lactone liposomes. Moreover, we hypothesized that it may improve the BBB permeability of ginkgolides. Liposomes are synthetic membranes and vesicles that consist of various phospholipids and cholesterol, and have good affinity for cell membranes. Liposomes possess a phospholipid bilayer structure, and contribute to improving BBB permeability and increasing the stability of encapsulated drugs [
19,
20,
21]. Due to their biocompatibility, biodegradability, low toxicity, hydrophobicity, hydrophilicity, and flexible structure, liposomes are known for their potential and actual uses in targeted drug delivery. However, ordinary liposomes are easily taken up by phagocytic cells and accumulate in the reticuloendothelial system (RES), which results in short residence times in the body [
22,
23]. Although some liposomes possess active targeting effects by attaching specific ligands (e.g., antibodies, peptides, nucleic acids, folic acid, sugars) [
24,
25,
26,
27], a saturation phenomenon may occur between specific ligands and target molecules [
28].
In the present study, we prepared ginkgolide liposomes modified with borneol, and hypothesized that it might improve the BBB permeability of ginkgolides. The effective factors in the preparation of borneol-modified liposome (GGB-LP) were optimized by Response Surface methodology (RSM), and the blood-brain barrier permeability was compared between GGB-LP and ginkgolides liposomes without borneol (GG-LP). This work will provide a theoretical basis for further in vivo experiments to study whether GGB-LPs could promote the neuroprotective activity of G. biloba lactones against cerebral ischemia injury.
3. Materials and Methods
3.1. Materials
Natural borneol (99.2% purity) was purchased from Shanghai Yuanye Biotechnologies Co., Ltd. (Shanghai, China). Ginkgolides (50.69% GB, 47.56% GA, 0.92% GC) was purchased from Nanjing Zixi Biological Products Co., Ltd. (Nanjing, China). Soya lecithin was bought from Shanghai Advanced Viecle Technology Co., Ltd. (Shanghai, China). Cholesterol was purchased from Sinopharm Chemical Reagent Co., Ltd. (Shanghai, China). Reference GA was obtained from the Jiangsu Institute for Food and Drug Control (Nanjing, China). Reference GB was obtained from the National Institute for Food and Drug Control (Beijing, China). Standard ketoprofen was obtained from the National Institute for the Control of Pharmaceutical and Biological Products (Beijing, China). Ginkgolides Injection was manufactured by Jiangsu Kanion Pharmaceutical Co., Ltd. (Lianyungang, China). Other chemicals and reagents used were chromatographic or analytical grade.
3.2. Preparation of Ginkgolides Liposomes Modified by Borneol (GGB-LP)
Liposomes were prepared by the thin film ultrasonic dispersion method [
31]. Briefly, 25 mg of ginkgolides, 15 mg of borneol, and appropriate amounts of soya lecithin and cholesterol were placed in 250 mL pear-shaped flask. Absolute ethanol (50 mL) was then added and the mixture was dissolved completely with the aid of ultrasound. The organic solvent was evaporated under a reduced pressure at 40 °C and 60 g by a rotary evaporator. The thin film was hydrated with PBS (pH 7.4) by rotary evaporation under reduced pressure. Then liposomes were formed by ultrasonication for 15 min and the filtration with 0.22 μm microporous membrane.
3.3. Characterization of GGB-LP
The particle size of distributions, mean diameter and polydispersity Index (PDI) of GGB-LP were measured by a nanoparticle size measuring instrument (Malvern Instruments Ltd., Malvern, UK). The encapsulation efficiency (EE) of GB was determined using Sephadex G-50 gel filtration chromatography and high performance liquid chromatography-evaporative light scattering detector (HPLC-ELSD) analysis. The operation procedure was that 0.5 mL of GGB-LP was eluted by addition of 15 mL PBS (pH 7.4) at the flow rate of 1 mL/min. The eluent solution was placed into the tube and 1% Triton and 0.1 mol/L hydrochloric acid were added for demulsification. After adequate mixing, the resulting solution was centrifuged at 6000× g for 10 min, and then analyzed using HPLC-ELSD method. GB was quantified based on a standard curve constructed right after the sample analysis. The total amount of GB in the suspension was determined by dissolving the sample in 1% Triton and 0.1 mol/L hydrochloric acid, followed by centrifugation in the same condition and HPLC-ELSD analysis. The EE of borneol was also determined. Briefly, GGB-LP (5 mL) was centrifuged at 6000× g for 30 min, and the suspension was then analyzed by gas chromatography (GC) for the content of free borneol. For determination of the total amount of borneol, liposome solution was dissolved in 1% Triton and 0.1 mol/L hydrochloric acid, centrifuged (6000× g, 10 min) and analyzed using GC.
The equation for EE of GB or borneol in GGB-LP is as follows:
where
Win is the amount of GB or borneol entrapped, and
Wtotal is the total amount of GB or borneol used in the preparation [
32].
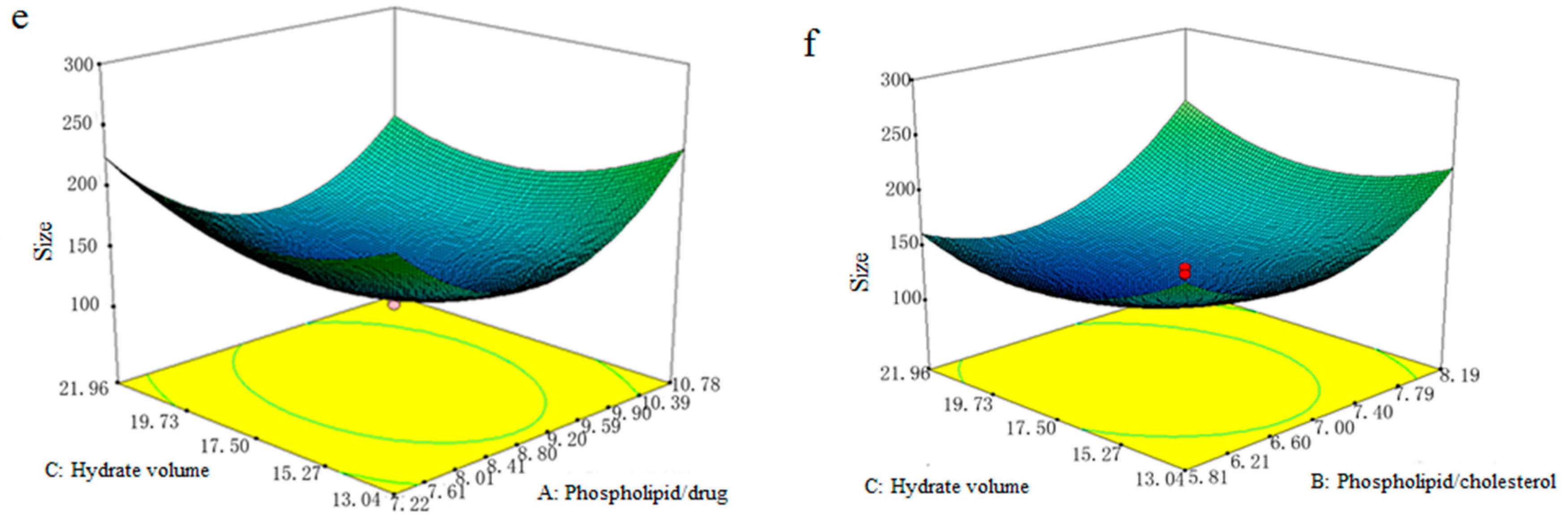
3.4. Optimization of GGB-LP Preparation by Response Surface-Central Composite Design
The preparation conditions of GGB-LP were optimized by response surface-central composite design in this study. Based on the single factor tests, the weight ratio of phospholipid and drug (
X1), the weight ratio of phospholipid/cholesterol (
X2) and the volume of PBS (pH 7.4) used for hydration (
X3, mL), were identified as key factors responsible for EE and size, and thus selected to optimize the preparation conditions of GGB-LP. The selected factors were subjected to response surface methodology (RSM) with central composite design. The ranges of independent variables are as follows: the range of
X1 is 6 to 12; the range of
X2 is 5 to 9; the range of
X3 is 10 to 25. The range and central point values of the three independent variables investigated are summarized in
Table 6. The dependent variables Y
1 and Y
2 were EE and particle size respectively. Three independent variables at five levels (3
5) were adopted for response surface-central composite design by using Design-Expert software (Version 8.05, Stat-Ease Inc., Minneapolis, MN, USA). The coefficient of correlation (
R2) and analysis of variance (ANOVA) were applied to evaluate suitability of the model. The fitted polynomial equations were expressed in 3D response surfaces [
33].
3.5. Blood-Brain Barrier Permeability of GGB-LP
3.5.1. In Vitro Cell Uptake Study for Evaluation of BBB Penetration Potential
bEnd.3 cells, the immortalized mouse brain endothelial cell line, were cultured in 90% Dulbecco’s modified Eagle’s medium supplemented with 4 mM L-glutamine, 1.5 g/L sodium bicarbonate, 4.5 g/L glucose and 10% fetal bovine serum, at 37 °C in a humidified environment with 5% CO2. In in vitro cell uptake studies, bEnd.3 cells were seeded at 107 cells/100 μL in an Eppendorf tube and incubated at 37 °C with GGB-LP, GG-LP, and GG-inj, respectively for 0.5, 1 and 2 h. At each incubation time points, cells were separated by centrifugation (1500× g, 10 min), washed with PBS followed by the addition of ultrapure water to prepare the total cell lysate. An aliquot of 100 μL of the supernatant was transferred to another Eppendorf tube. Then both of the tubes with the respective GB contents were measured by UPLC-MS (supposed to be A and B, respectively). The cell uptake index was calculated from the formula .
3.5.2. Animals and Administration of GG Formulations
Kunming strain mice (SPF level, male, weighing within 20 ± 2 g) used for this study were obtained from Qinglongshan Animal Breeding Farms (Nanjing, China). Before the experiment, the mice were fasted for 12 h but allowed free access to water. All animal experiments were conducted in full compliance with the guide for the care and use of laboratory animals and approved by the animal and ethics review committee of Nanjing University of Chinese Medicine, China. Mice were randomly and equally assigned to three different groups of GG formulations (n = 35 for each group) including ginkgolides injection (GG-inj) group, ginkgolide liposomes without borneol (GG-LP) group and GGB-LP group. Animals were given the GG formulations by intravenous injection via the tail vein, at a single dose of 6.5 mg/kg GB in the formulations. At the indicated times (5, 15, 30, 60, 120 and 240 min) after administration, blood was collected from the retrobulbar venous plexus. Blood samples were centrifuged at 3000× g for 6 min. Plasma was separated and stored at −20 °C until use. In addition to blood, tissue samples, including heart, liver, spleen, lung, kidney, and brain, were also collected after cervical dislocation. The tissues ware washed with physiological saline, dried with filter paper, weighed and stored at −20 °C until further experiment.
3.5.3. UPLC-MS Analysis of GB in Plasma and Tissues
Thawed plasma samples (100 μL), 10 μL of internal standard (ketoprofen, 0.1 μg/mL) and 20 μL hydrochloric acid (1 mol/L) were placed into a centrifuge tube, adequately mixed by vortexing for 1 min and 1 mL of ethyl acetate was added. Subsequently, the mixture was vortex-mixed for 5 min and centrifuged at 3600× g for 6 min. 900 μL of supernatant was concentrated under reduced pressure, and the residue is redissolved in 100 μL of the mobile phase, vortexed for 5 min, and centrifuged (8400× g, 10 min). The resultant supernatant (80 μL) was analyzed by UPLC-MS. For analysis of GB tissues, samples of heart, liver, spleen, lung, kidney, and brain were respectively homogenized with 3 mL of normal saline in a tissue homogenizer, mixed with 20 μL internal standard (ketoprofen, 0.1 μg/mL ),vortex-mixed for 3 min and centrifuged at 3600× g for 10 min. After centrifugation, the upper organic layer was transferred into a tube and evaporated to dryness in a stream of nitrogen. Mobile phase (100 μL) was added into the tube for redissolution. Then the samples were vortex-mixed for 3 min and centrifuged at 7200× g for 5 min. The resultant supernatant was analyzed by UPLC-MS.
The levels of GB in plasma and tissues were assayed by UPLC-MS (Xevo TQD, Waters, Waters Corporation, Milford, MA, USA). The chromatographic conditions were as follows: Acquity UPL HSS T3 column (100 mm × 2.1 mm, 1.8 μm); column temperature, 40 °C; mobile phase was composed of 0.4% formic acid and methanol (30:70, v/v); flow rate, 0.25 mL/min; injection volume, 5 μL. The mass spectrometer was equipped with electro spray ionization (ESI) source, and the UPLC-MS analysis was operated in the positive ionization mode. Quantification was carried out using the multiple reaction monitoring (MRM) mode. Other MS parameters were set as following: the ion source temperature, 150 °C; desolvation temperature, 400 °C; flow rate of desolvation gas, 1000 L/h.
3.6. Data Analysis
Non-compartmental analysis of the pharmacokinetic data was performed by the statistical moment method using the DAS 2.0 pharmacokinetic program (Chinese Pharmacological Society, China). The key parameters of pharmacokinetics (such as AUC0→∞, MRT, Tmax, Cmax and CL) were achieved from DAS 2.0 pharmacokinetic program. The tissue targeting efficiency was evaluated using the relative uptake rate (re) and the drug targeting index (DTI). The re is calculated as follows: (“AUCx’’ is the AUC of tissue x, and ‘‘lp’’ is the GG-LP or GGB-LP). re > 1 represents that the test group has certain tissue targeting compared with the control group, and the higher Re indicates the better tissue targeting; re < 1 indicates no targeting. DTI was obtained by the following equation: (“AUCp’’ is the AUC of plasma), and the value of DTI > 1 was considered as the targeting distribution. Statistical comparisons were performed by one-way ANOVA for multiple groups, and p < 0.05 was considered statistically significant.
4. Conclusions
In this study, GGB-LPs were prepared, and the preparation conditions were optimized by RSM. The optimal preparation conditions for GGB-LP was as follows: ratio of phospholipid to drug (w/w) 9:1, ratio of phospholipid to cholesterol (w/w) 7:1, and volume of PBS for hydration 17.5 mL. The RSM result was reliable and the EE of GGB-LP was 87.56%. Besides, the average particle size of GGB-LP was 129 nm, suggesting that liposomes were well-distributed. In addition, the blood-brain barrier permeability study showed GGB-LPs had better permeability and delivered a higher concentration of GB in the brain, compared with GG-inj and GG-LP. Moreover, GGB-LP produced low level of ginkgolides accumulated in non-pathological organs, and the elimination of drug in these organs was fast. This study demonstrates that borneol can promote the transport of ginkgolide across the BBB, which may be attributed to the enhancement of blood-brain barrier permeability by borneol. With the aid of borneol, the clinical efficacy of ginkgolides against ischemic stroke would be enhanced, which will play an important role in the treatment of central nervous system.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}