1. Introduction
Cholestasis, a hallmark feature of hepatobiliary disease, is characterized by impairment of bile and bilirubin secretion [
1,
2,
3] and alterations in the expression levels of hepatic membrane transporters and bile acid metabolic enzymes [
2,
4]. Cholestasis is often divided into two categories based on etiology, namely, intrahepatic and extrahepatic. Surgical removal of primary foci remains the main treatment for extrahepatic cholestasis, whereas the therapeutic options for intrahepatic cholestasis are limited because liver transplantation is only appropriate for certain patients. Thus, a better understanding of the molecular mechanisms underlying intrahepatic cholestasis is required to identify novel drug targets and improve current therapies.
Rosmarinic acid (RA) (
Figure 1) is one of the most important and well-known polyphenolic antioxidants that is abundant in various medicinal plants of the Lamiaceae family and have historically been used in Traditional Chinese Medicine, which include
Rabdosia rubescens (Hemsl.) H. Hara.,
R. amethystoides (Benth.) Hara.,
Rosmarinus officinalis L.,
Perilla frutescens (L.) Britton, and
Salvia miltiorrhiza Bunge [
5,
6,
7].
R. lophanthoides is one of the major subspecies of
R. amethystoides (Benth.) Hara., commonly known as
Xihuangcao in China. It is a folk remedy that is commonly used for the prevention and treatment of hepatobiliary diseases in Southern China. Several studies have reported the role of RA and its pharmaceutical and biotechnological effects; for example, anti-colitic, antioxidant, anti-inflammatory, anti-leukemic, and anti-hepatic ischemia activities, as well as neuroprotective effects [
8,
9,
10,
11,
12,
13,
14]. Its curative effects have been proven by both clinical applications and experimental research [
7,
15].
However, the pharmacokinetic (PK) and pharmacodynamic (PD) data about RA is limited and its anti-liver injury activity remains unclear. Upon oral administration, RA is rapidly absorbed (plasma values ca. 5 μmol/L) and metabolized into conjugated and/or methylated forms, which are mostly degraded and metabolized as conjugated forms of caffeic, ferulic, and
m-coumaric acids [
16].
To determine the pharmacological properties of RA, a more specific and specialized PK-PD model is essential. PK/PD integration, dose titration study, and PK-PD modeling are major methods that are employed to describe the dose-effect relationship of a drug by establishing the correlation between its PK and PD data. PK-PD modeling is a more effective approach to studies on PK/PD integration and dose adjustment. It has been widely used in pre-clinical and clinical studies and contribute to expressing drug efficacy over time and plasma concentration, thereby providing valuable references for optimizing the clinical dosage, improving the therapeutic efficacy, and reducing the toxic and side effects [
17,
18,
19,
20,
21]. For example, PK/PD modeling was successfully applied for the selective dopamine D2 antagonist remoxipride, both in humans [
22] and rats [
23] to predict the pharmacological response beyond the tested conditions. Lv J reported that rhubarb is effective for the treatment of jaundice using the PK/PD model [
24]. To date, no PK/PD model of RA in ANIT-induced cholestasis has been established to date. In our previous studies, we showed that RA is the predominant active component in a water extract of
R. serra. Furthermore, we reported that
R. serra imparts distinct hepatoprotective effects [
25]. The present study assessed the pharmacodynamic and pharmacokinetic properties of RA in a cholestasis rat model induced by ANIT.
3. Discussion
RA is a natural water-soluble polyphenol that is often stored at low temperatures and in the dark. Previous studies have shown that RA and methylated RA can be detected in the plasma after administration. The absorption, distribution, metabolism, and excretion of RA in the body takes 8–18 h. This indicates that RA can be partially absorbed, metabolized, or biotransformed into other substances in rats.
In this study, we investigated the changes in RA in healthy and cholestasis model rats after a single oral administration. The study also assessed various extraction methods for plasma protein using ethyl acetate and methanol-water, methanol-phosphoric acid and methanol-acetic acid water on the peak of RA was studied. The results indicated that methanol-acetic acid water is the optimal mobile phase.
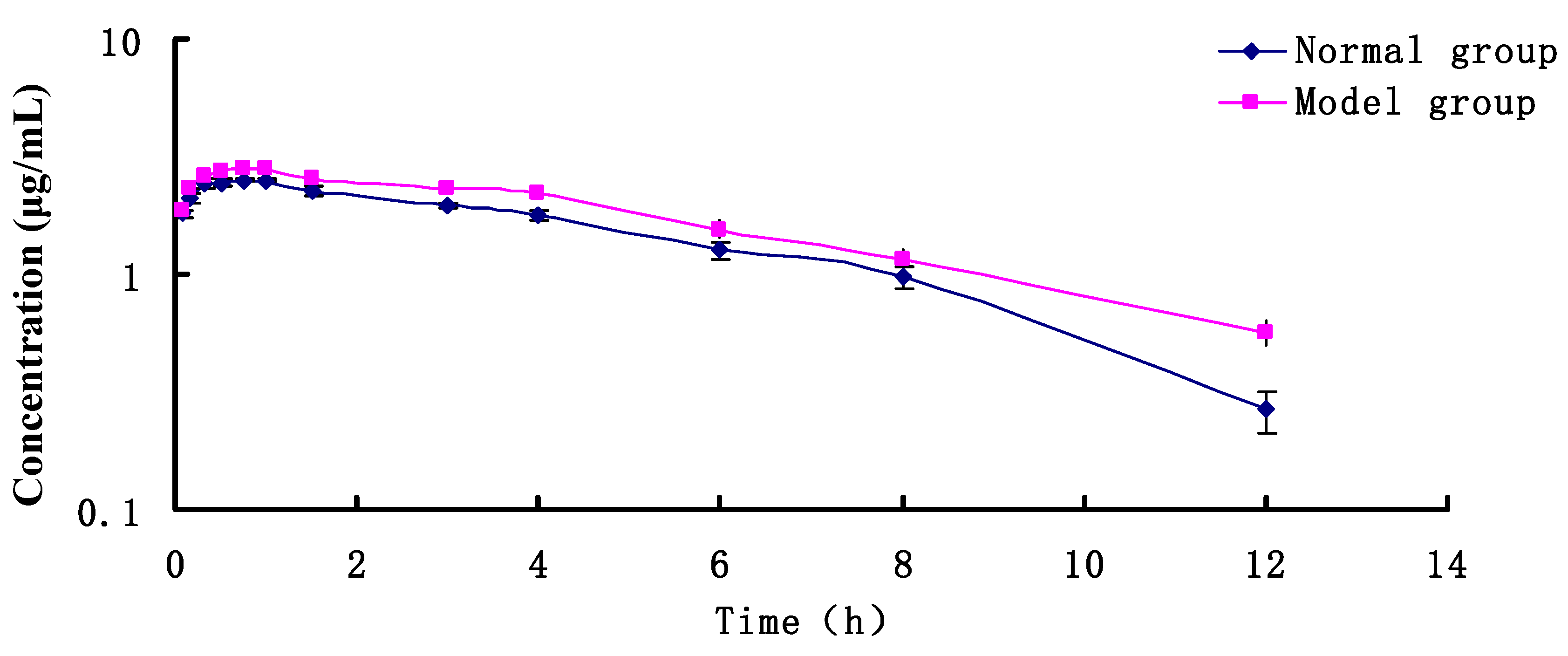
RA parameters were calculated using a PK software. The AUC(0-∞) of RA (100 mg/kg) in normal control group was 17.29 mg·h/mL. The AUC(0-∞) of RA in rats was increased by 23.11 mg·h/mL after ANIT-induced cholestasis, which may be due to liver injury and a significant decrease in bile secretion during cholestasis, thereby leading to drug accumulation and ultimately liver toxicity.
A PK model was established using WinNonlin 6.4 software. The PK-PD binding model was fitted with the PK-PD Link program module in WinNonlin 6.4. The PK model was determined using various model fitting methods. The experimental data were expressed as x ± s. The PK and PD parameters were compared between the two groups using the t-test, and differences with a p < 0.05 were considered statistically significant.
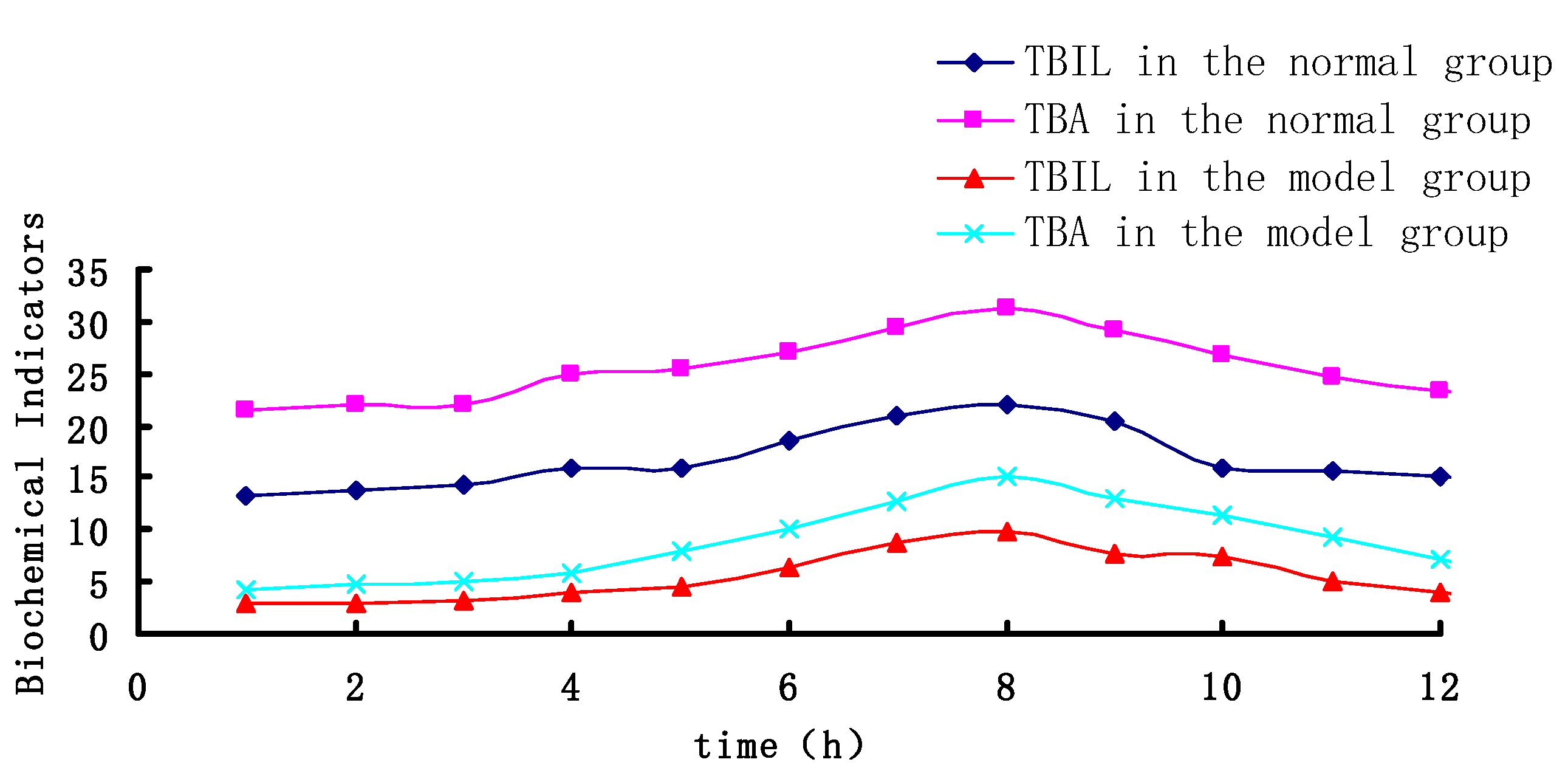
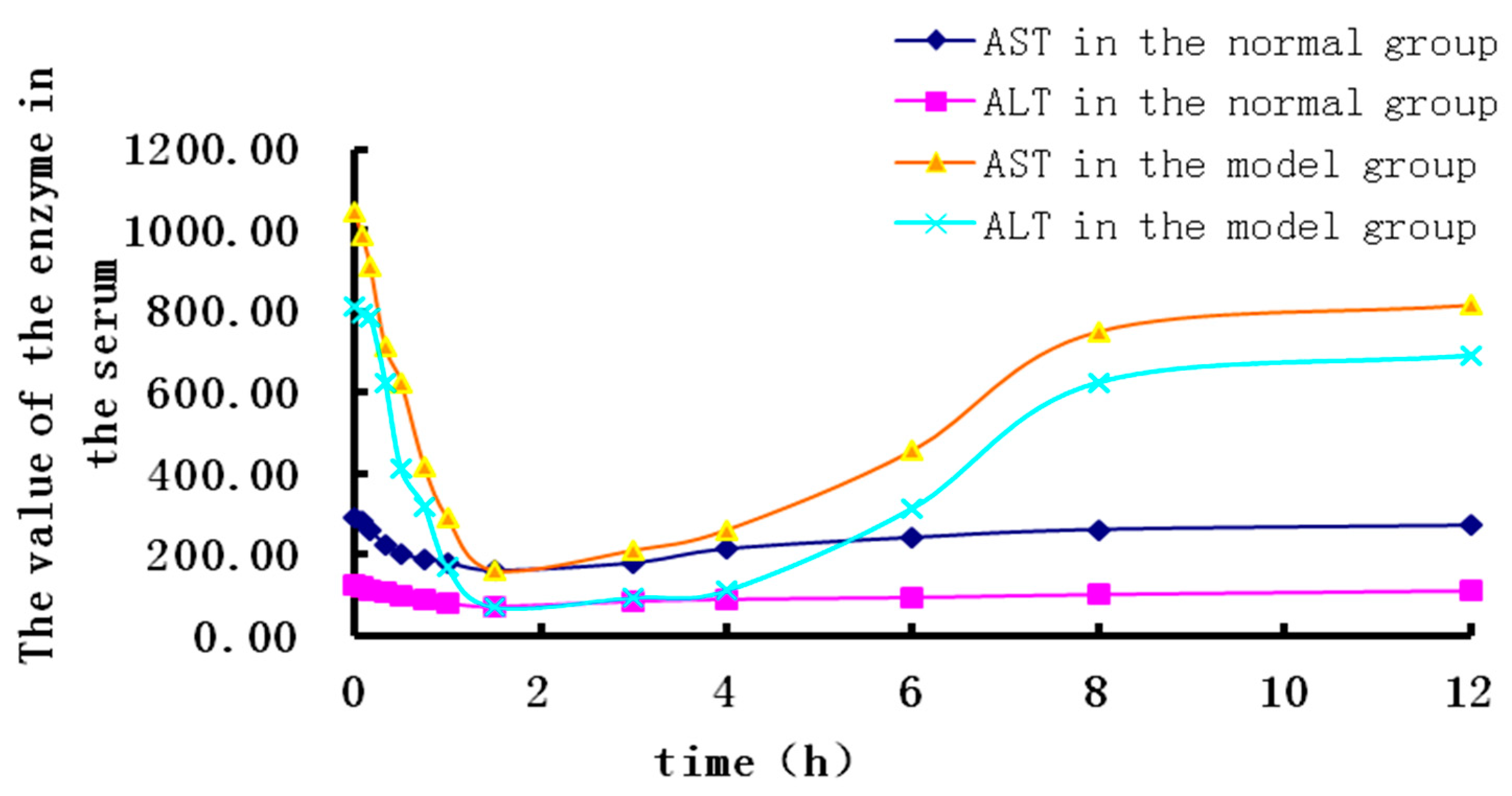
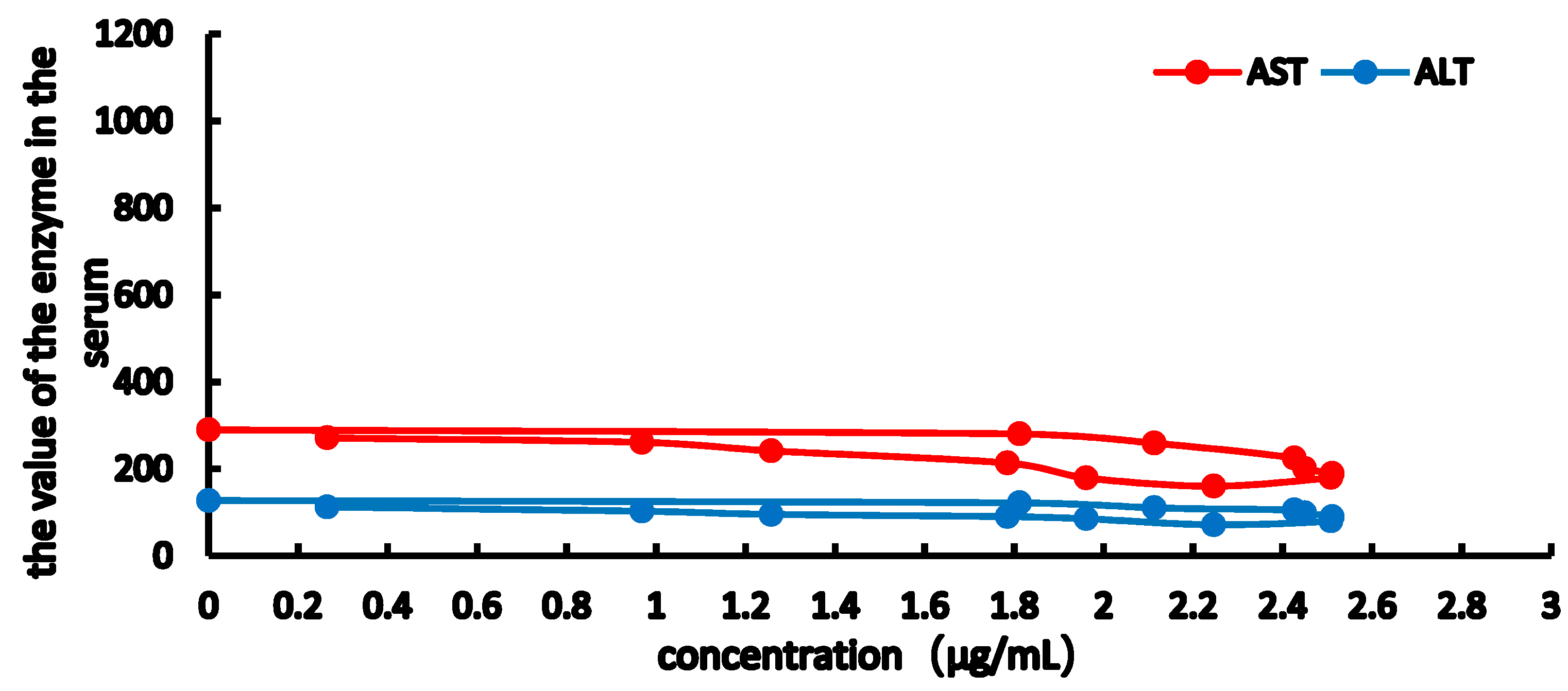
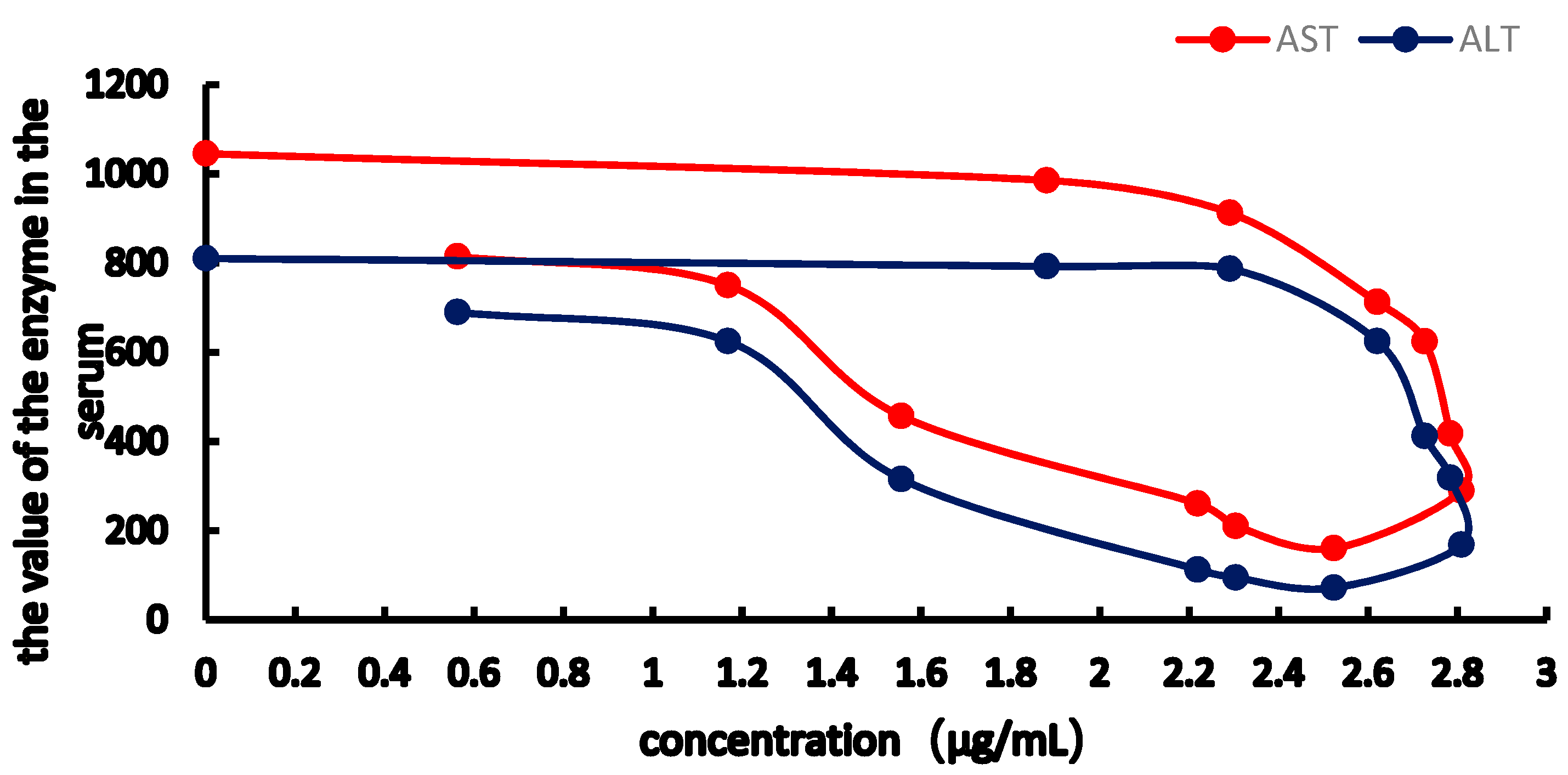
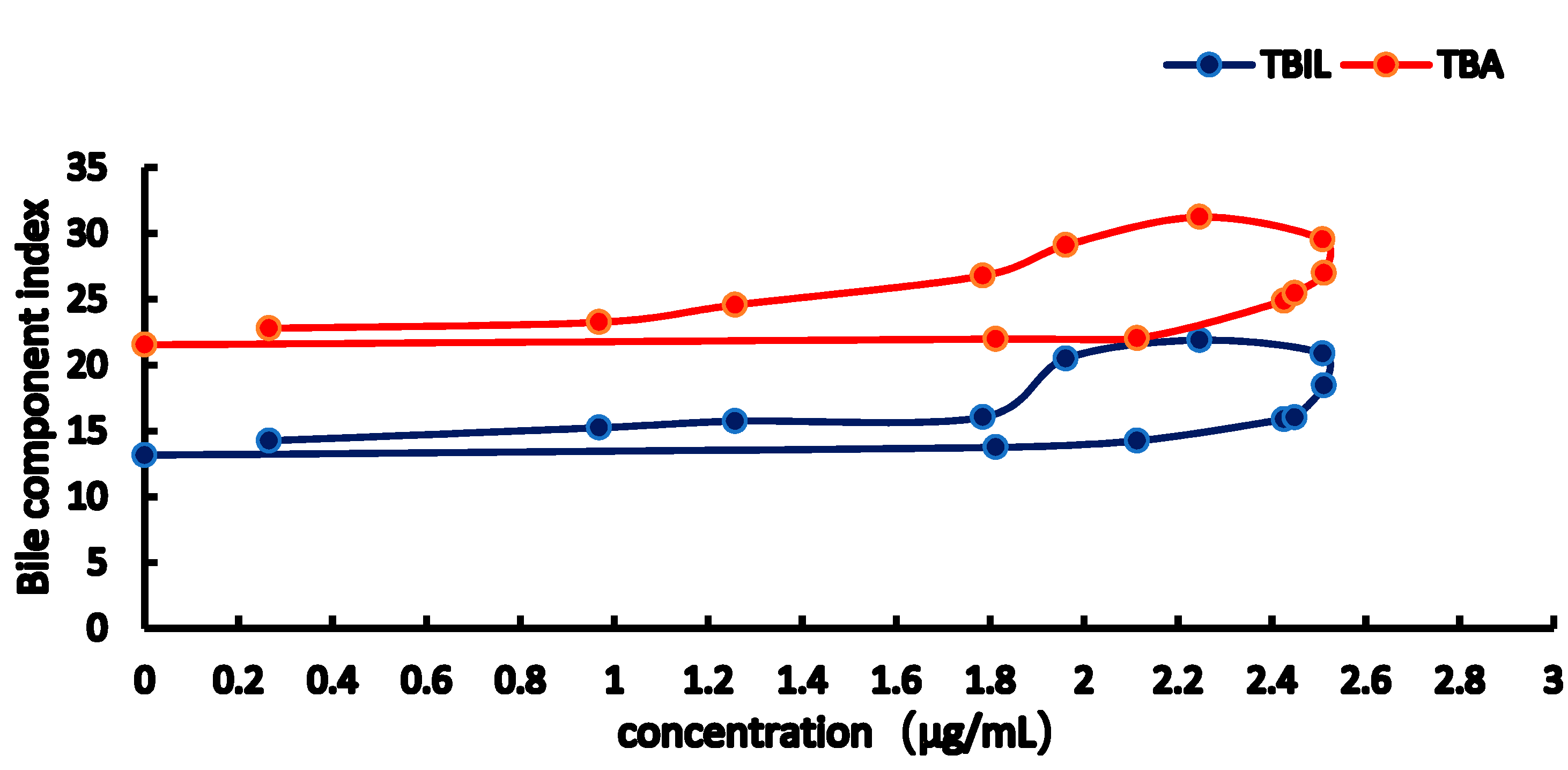
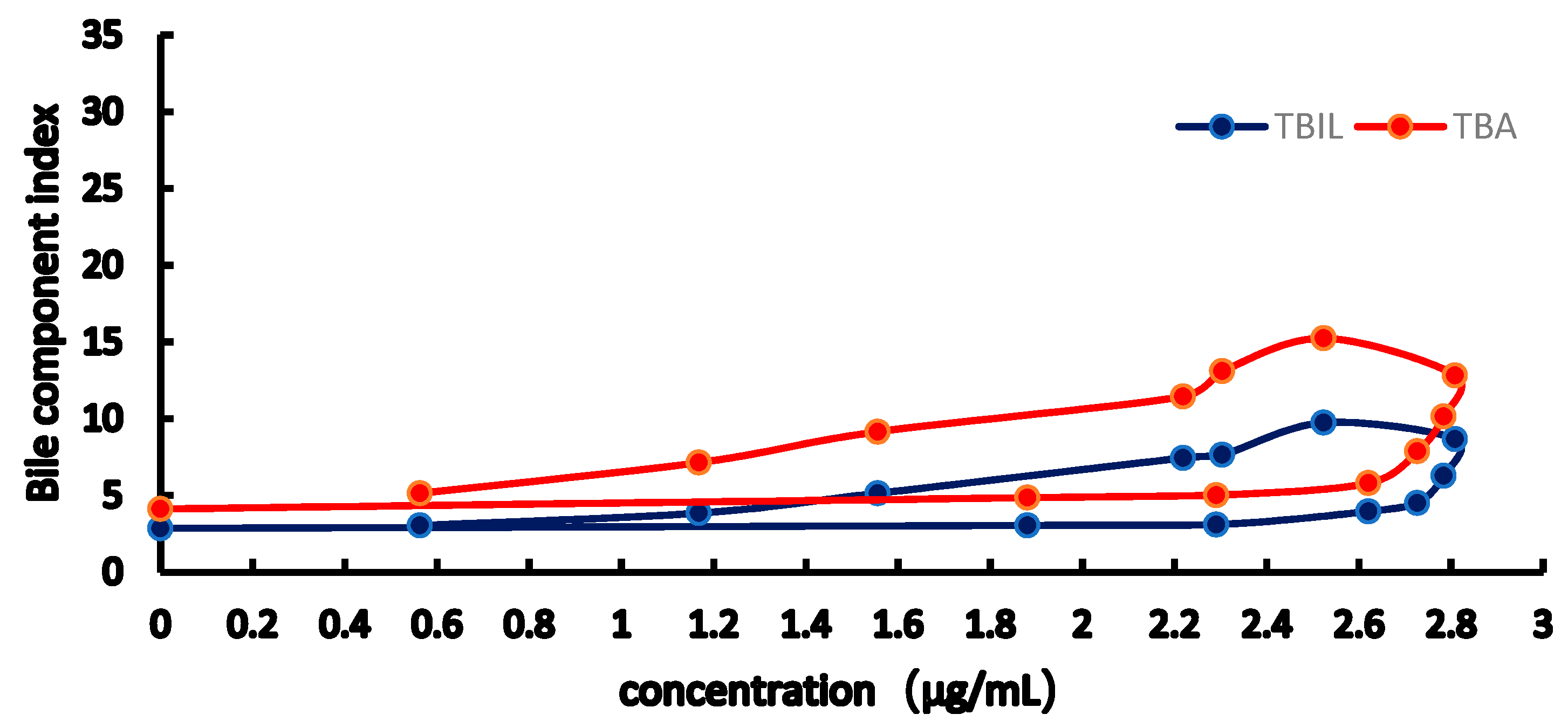
The TBIL, TBA of the E-C curve shows a counterclockwise ring, indicating that TBIL and TBA in bile significantly lagged behind the plasma concentration. The AST, ALT E-C curve showed a clockwise ring, showing that RA has maximum pharmacological activity, inhibiting the increase in AST, ALT levels, and at the same time, thereby delaying the pharmacological effects of RA. The levels of TBIL and TBA in bile and AST, ALT in serum were measured, and a significant improvement was observed 90 min after RA administration. In addition, the AUC of RA in the cholestasis rat model was higher than that in normal rats, which may be caused by bile acid excretion, thereby reducing RA elimination and half-life and increasing the maximum RA concentrations.
Emax represents the largest drug effect, reflecting the intrinsic activity of RA, wherein the greater the value, te greater the intrinsic activity. EC50 is the concentration of drug in response to 50% of the maximal effect, which reflects the affinity of a drug to acceptor. The smaller the EC50, the greater the affinity of a drug to its receptor. γ reflects the size of the slope of the central section of the curve, which reflects the selectivity and sensitivity of a drug.
Based on the TBIL and TBA levels, the Emax model group was 24% and 48% of that of the control group, indicating that RA has a certain recovery TBIL, TBA function. EC50 analysis showed that RA has a higher affinity for TBIL. The AST and ALT levels show that Imax is the greatest benefit of inhibition, wherein the greater the value, the greater the intrinsic activity of a drug, indicating that RA-induced inhibition of AST, ALT increases is better. The γ values indicate that the RA concentration-effect curve is steeply S-shaped, suggesting that there is a need to further investigate the safety of using RA as a drug. After this relationship has been established, this model could provide useful information or explanation of the therapeutic action of RA in ANIT-induced acute cholestasis.
Bile is a unique and vital aqueous secretion of the liver that is formed by hepatocytes and is modified downstream by absorptive and secretory properties of the bile duct epithelium. Cholestasis is defined as the impairment of normal bile flow resulting either from a functional defect at the level of the hepatocytes or from obstruction at the bile duct level and might result from infection, drugs, and autoimmune, metabolic, or genetic disorders [
26,
27,
28,
29]. Bile is an alkaline body liquid produced by the liver cells of most vertebrates. After secretion, bile enters the gallbladder where it is concentrated or directly delivered to the intestinal lumen. Bile consists of ~95% water that contain various endogenous solid constituents such as bile salts, bilirubin phospholipids, cholesterol, amino acids, and steroids. Meanwhile, exogenous drugs, xenobiotics, and environmental toxins are also secreted through bile [
30].
Interruption of bile flow leads to the accumulation of bile acids and other bile components in the liver and, ultimately, hepatobiliary toxicity. Liver injury is characterized by elevated serum bile acids and bilirubin, the increased aspartate aminotransferase activity, and histopathological lesions. TBA and TBIL increased when the secretion of bile is obstructed in cholestasis. A significant increase in ALT and AST levels are hallmarks of liver injury. Bsep and Mrp2 are critically involved in this process, and many kinds of bile acid transporters have been demonstrated to play vital roles in maintaining hepatic bile acid homeostasis in absorption and excretion [
31,
32].
ANIT is a hepatotoxicant that was used to simulate human intrahepatic cholestasis in rats. The liver intrahepatic cholestasis injury caused by ANIT is thought to reflect the potential toxicity of this chemical in hepatocytes and biliary cells [
26,
33]. ANIT damages bile duct epithelia, thereby inducing cholestasis. The ANIT-induced pathological changes in the liver tissues include hyperplasia of the bile duct epithelial cells, necrosis of liver cells, inflammatory cell infiltration, and hyperplasia of collagen fibers.
In our previous studies, three doses of ANIT (60 mg/kg, 65 mg/kg, and 100 mg/kg, respectively) were intragastric administered to rats, and bile flow rate and pathological changes were observed, indicating liver cholestasis injury, including edema, bile duct obstruction, serious interlobular duct epithelial apoptosis, or necrosis [
25]. Based on liver pathologic grades, 65 mg/kg was determined to be suitable for our experiment. The ANIT dose 48 h before the last administration of RA was also determined.
5. Materials and Methods
5.1. Drugs and Reagents
RA (Chengdu Must Biological Technology Co., Ltd., Chengdu, China, batch number 1411507, purity 99.4%); ferulic acid (Chengdu Must Biological Technology Co., Ltd; batch number: 150305, purity ≥ 98%); bilirubin direct (DBIL), total bile acid (TBA), and total bilirubin (TBIL) reagent (BioSino Biological Technology Co., Ltd., Beijing, China; batch numbers 140621, 140721, and 140531, respectively); aspartate transaminase (AST) and alanine aminotransferase (ALT) (Shanghai Kehua Bio-Engineering Co., Ltd., Shanghai, China; batch numbers 20140214 and 20140521, respectively); ANIT (Sigma, San Jose, CA, USA; batch number STBC5577V); and ultrapure water, prepared by our laboratory, was used throughout of this research. All other chemicals were of analytical grade. The extraction procedure was as follows: approximately 2 kg of dried R. lophanthoides were crushed into small pieces and filtered through a 40-mesh (0.45-mm) sieve, then the pieces were soaked in 40 L of ethanol at room temperature for 1 h. RA was extracted from ethanol using the heating circumfluence method at 80 °C twice, each for 2 h. A macroporous resin X-5 was employed absorb the extract at a rate of 2 BV/h, which was then washed with 80% ethanol, and the eluent was concentrated by reducing pressure followed by drying by vacuum, yielding 39.32 g of RA.
5.2. Animals
SPF-grade male Sprague-Dawley rats, weighing 200 g–220 g, were purchased from the Medical Experimental Animal Center of Guangdong Province (Guangdong, China). The animals were housed under controlled standard conditions (25 ± 2 °C), relative humidity (60 ± 10%) with the natural light–dark cycle, and free access to standard rat food (laboratory rodent chow) and water for one week prior to the experiment. The animals were fasted overnight with free access to water prior to drug administration. All animal experiments were performed in accordance with the Guidelines for the Care and use of Laboratory Animals of Guangzhou University of Chinese Medicine.
5.3. Instruments
Clinical chemistry analysis of serum samples was conducted with an Automatic Biochemistry Analyzer (ECHO, Milan, Italy). Chromatographic analysis was performed using an Agilent 1100 series HPLC system (Agilent Technologies Inc., Santa Clara, CA, USA) consisting of a quaternary pump, a diode array detector (DAD), an autosampler, a vacuum degasser, and a column oven. Data analysis and model establishing were conducted using Winnolin 6.4 (Pharsight Corporation, Mountain View, USA).
5.4. Liquid Chromatography
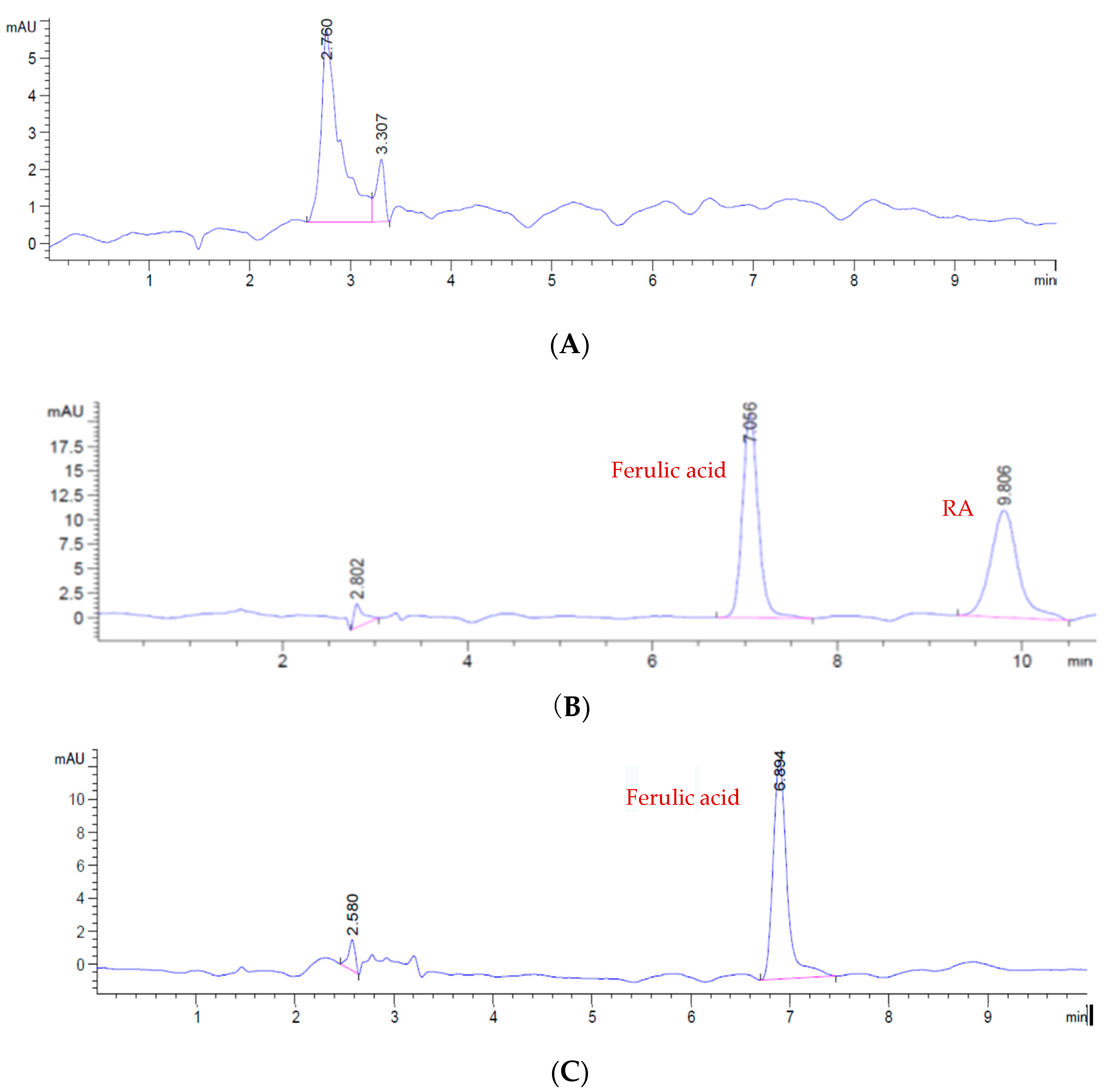
RA was separated using a Luna C18 column (250 mm × 4.6 mm, Phenomenex, Torrance, CA, USA), and separation was performed on an Agilent 1100 series HPLC equipment. The mobile phase composition included methanol (A) and 1% acetic acid (B) (A:B = 45:55, v/v). The detection wavelength was 330 nm. Isocratic elution was performed at a flow rate of 1 mL/min for a total run time of 12 min and an injection volume of 10 μL. Column temperature was maintained at 30 °C.
5.5. Standard Solution and Sample Preparation
Stock solutions of RA (2 mg/mL) and ferulic acid [internal standard (IS), 1 mg/mL] in methanol were prepared. Working solutions of these analytes were freshly prepared by diluting the standard solutions in methanol to concentrations of 1500, 1000, 500, 300, 100, 90, 50, 25, 10 and 5 μg/mL. In addition, a working IS solution at a concentration of 140 μg/mL was prepared.
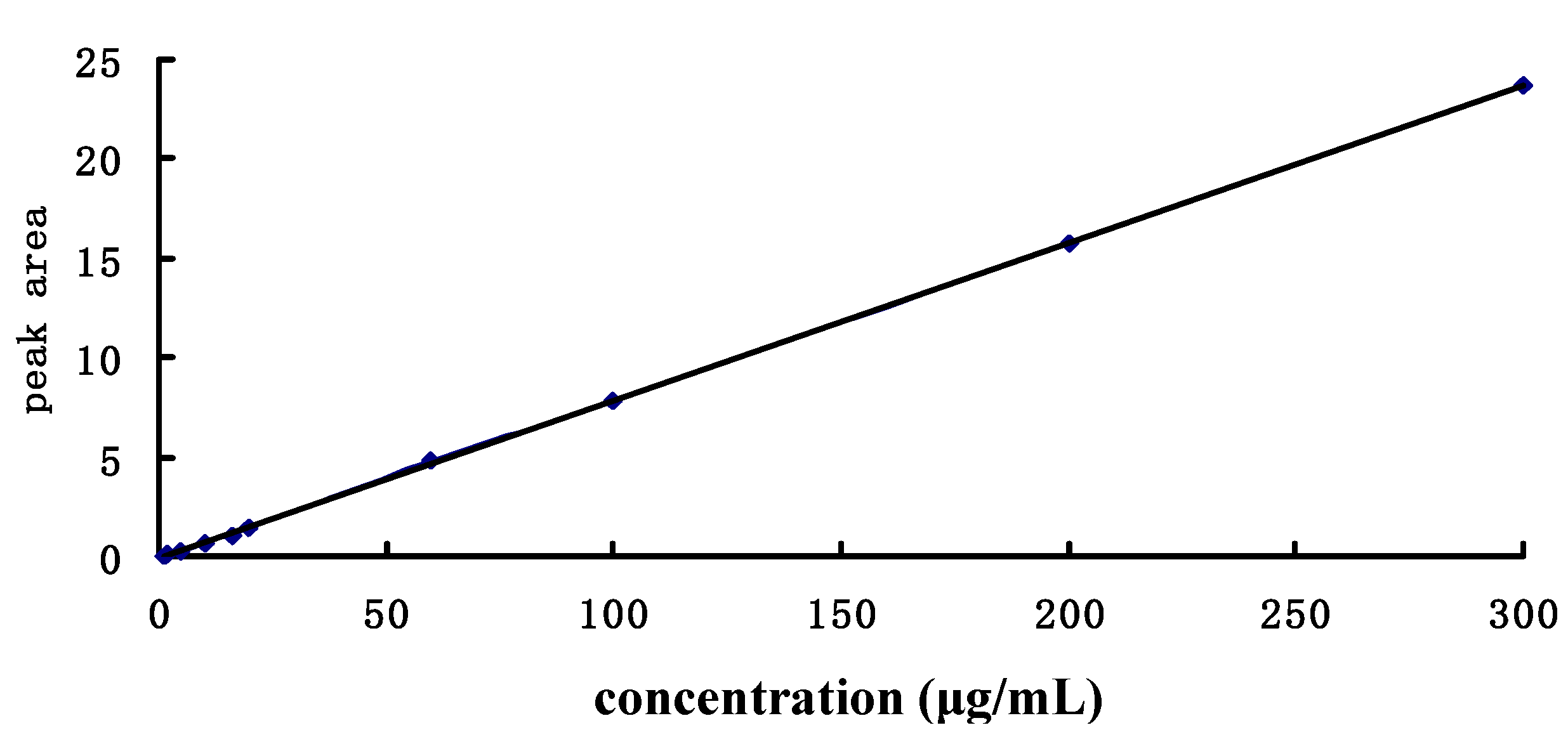
Corresponding standard (10 μL) and ethyl acetate (300 μL) was added into 100 μL blank serum, mixed together for 10 min then 10 μL of the internal standard (ferulic acid) and 10%HCL (10 μL) was put into the mixture in turn, mixed again for 5mins, and centrifuged (12,000 r/min) for 15 min. The substratum (aqueous layer) was extracted with ethyl acetate and merged with organic layer, and flushing with nitrogen, redissolved with methanol (50 μL) and injected with 10 μL. The standard curve concentration was: 300, 200, 100, 60, 20, 16, 10, 5, 2 and 1 μg/mL. All solutions that contained the IS were stored at 4 °C and were prepared for PK studies.
Each sample was mixed for 1 min and centrifuged at 12,000 rpm for 15 min at 4 °C. After stratification, the aqueous layer was separated and extracted twice with ethyl acetate. The ethyl acetate solution were dried under nitrogen and then dissolved in 100 μL methanol, mixed for 30 s, centrifuged (12,000 rpm) for 15 min, and then 10 μL was injected into the HPLC for analysis.
To validate our method, three concentrations of the standard solution containing RA (35 μg/mL, 48 μg/mL, 70 μg/mL) and IS were used for preparing QC plasma samples.
5.6. PK and PD Research
Sixteen Sprague-Dawley rats were randomly divided into two experimental groups: control group and model group. Animal models of intrahepatic cholestasis were established (80 mg·kg−1) 48 h treatment with ANIT, and RA (100 mg/kg) was orally administered before time zero. Blood samples were collected at 0.083, 0.17, 0.33, 0.5, 0.75, 1, 1.5, 3, 4, 6, 8, 12 and 20 h after oral administration. Orbital venous blood samples were collected into heparinized Eppendorf tubes and left to stand for 1 h. Then, the blood samples were then centrifuged at 3800 rpm for 10 min at 4 °C to isolate the serum, which were transferred into clean tubes and stored at −80 °C until analysis.
Before the operation, all rats were fasted and supplied with water for 8 h. Approximately 48 h after administration of ANIT, the rats were anesthetized and operated by bile duct cannulation on the 3rd day. The right side common carotid artery was separated for intubation. Then, RA (100 mg/kg) was given to the animals, and 0.1 mL blood samples and 0.25 mL bile were in turn collected at 0, 0.083, 0.167, 0.33, 0.5, 0.75, 1, 1.5, 3, 4, 6, 8 and 12 h, respectively. Bile from each rat was collected for 5 min, followed by isolation of the liver. The blood samples were allowed to coagulate for 10 min to obtain serum, followed by centrifugation at 3000 rpm for 10 min. All blood and bile samples were stored at 4 °C until analysis.
5.7. Blood Biochemical Determinations
After bile collection, the animals were sacrificed. Blood samples were stored in Eppendoff tubes and used in chemical analysis, including ALT and AST. TBIL and TBA in bile were also assayed using kits. Analysis was conducted using an automatic biochemical analyzer (Italy Echo instruments, Milan, Italy).
5.8. Analysis
The PK data were analyzed using the WinNonlin 6.4 software which was provided by Dr. Zipeng Gong. Oral administration of RA was performed to determine blood PK parameters, including elimination half-life (t1/2), mean retention time of drug (MRT), area under the concentration-time curve (AUC(0-t) and AUC(0-∞)), clearance (CL), and the apparent volume of distribution (Vd).
Analysis was performed using the t-test and one-way ANOVA with test using SPSS 21.0 (IBM company, Chicago, IL, USA, and differences with a p < 0.05 were considered statistically significant and those with a p < 0.01 were regarded as highly significant.

 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}